
Abstract
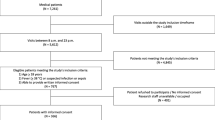
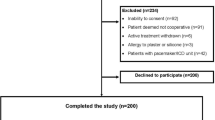
Premature discharge may result in readmission while longer hospitalization may increase risk of complications such as immobilization and reduce hospital capacity. Continuous monitoring detects more deviating vital signs than intermittent measurements and may help identify patients at risk of deterioration after discharge. We aimed to investigate the association between deviating vital signs detected by continuous monitoring prior to discharge and risk of readmission within 30 days. Patients undergoing elective major abdominal surgery or admitted with acute exacerbation of chronic obstructive pulmonary disease were included in this study. Eligible patients had vital signs monitored continuously within the last 24 h prior to discharge. The association between sustained deviated vital signs and readmission risk was analyzed by using Mann–Whitney’s U test and Chi-square test. A total of 51 out of 265 patients (19%) were readmitted within 30 days. Deviated respiratory vital signs occurred frequently in both groups: desaturation < 88% for at least ten minutes was seen in 66% of patients who were readmitted and in 62% of those who were not (p = 0.62) while desaturation < 85% for at least five minutes was seen in 58% of readmitted and 52% of non-readmitted patients (p = 0.5). At least one sustained deviated vital sign was detected in 90% and 85% of readmitted patients and non-readmitted patients, respectively (p = 0.2). Deviating vital signs prior to hospital discharge were frequent but not associated with increased risk of readmission within 30 days. Further exploration of deviating vital signs using continuous monitoring is needed.


Similar content being viewed by others

References
Klinge M, Aasbrenn M, Aasbrenn M, Öztürk B, Christiansen CF, Suetta C, Suetta C et al (2020) Readmission of older acutely admitted medical patients after short-term admissions in Denmark: a nationwide cohort study. BMC Geriatr 20:203. https://doi.org/10.1186/s12877-020-01599-4
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW (2003) The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. https://doi.org/10.7326/0003-4819-138-3-200302040-00007
Pittappilly M, Sarao MS, Bambach WL, Helmuth A, Nookala V (2019) Vital signs on hospital discharge and re admission rates. Int J Med 112:275–279. https://doi.org/10.1093/qjmed/hcz002
Siuba MT, Sadana D, Gadre S, Bruckman D, Duggal A (2022) Acute respiratory distress syndrome readmissions: a nationwide cross-sectional analysis of epidemiology and costs of care. PLoS One. https://doi.org/10.1371/JOURNAL.PONE.0263000
Rasmussen MG, Ravn P, Molsted S, Tarnow L, Rosthøj S (2017) Readmission to hospital of medical patients—a cohort study. Eur J Intern Med 46:19–24. https://doi.org/10.1016/j.ejim.2017.07.008
Shah T, Churpek MM, Perraillon MCoca, Tamara Konetzka R (2015) Understanding why patients With COPD Get Readmitted: a large national study to delineate the medicare population for the readmissions penalty expansion. Chest 147:1219–1226. https://doi.org/10.1378/CHEST.14-2181
Clausen J, Falck H, Julie H, Walbech S, Gögenur I, Hansen HF (2022) Incidence and clinical predictors of 30-day emergency readmission after colorectal cancer surgery-a nationwide cohort study. Colorectal Dis. https://doi.org/10.1111/codi.16349
Merkow RP, Ju MH, Chung JW, Hall BL, Cohen ME, Williams MV, Tsai TC, Ko CY, Bilimoria KY, Author C (2015) Underlying reasons associated with hospital readmission following surgery in the United States. JAMA 313:483–495. https://doi.org/10.1001/jama.2014.18614
Robinson R, Bhattarai M, Hudali T (2019) Vital sign abnormalities on discharge do not predict 30-day readmission. Clin Med Res 17:63–71. https://doi.org/10.3121/cmr.2019.1461
Nguyen OK, Makam AN, Clark C, Zhang S, Xie B, Velasco F, Amarasingham R, Halm EA (2017) Vital signs are still vital: instability on discharge and the risk of post-discharge adverse outcomes. J Gen Intern Med 32:42–48. https://doi.org/10.1007/s11606-016-3826-8
Halm EA, Fine MJ, Kapoor WN, Singer DE, Marrie TJ, Siu AL (2002) Instability on hospital discharge and the risk of adverse outcomes in patients with pneumonia. Arch Intern Med 162:1278–1284. https://doi.org/10.1001/archinte.162.11.1278
Elvekjaer M, Aasvang EK, Rasmus OM, Sørensen HBD, Porsbjerg CM, Jensen J-U, Haahr-Raunkjaer C, Meyhoff CS (2020) Physiological abnormalities in patients admitted with acute exacerbation of COPD: an observational study with continuous monitoring. J Clin Monit Comput 34:1051–1060. https://doi.org/10.1007/s10877-019-00415-8
Duus CL, Aasvang EK, Olsen RM, Sørensen HBD, Jørgensen LN, Achiam MP, Meyhoff CS (2018) Continuous vital sign monitoring after major abdominal surgery—quantification of micro events. Acta Anaesthesiol Scand 62:1200–1208. https://doi.org/10.1111/AAS.13173
Sun Z, Sessler DI, Dalton JE, Devereaux Pj, Shahinyan A, Naylor AJ, Hutcherson MT et al (2015) Postoperative hypoxemia is common and persistent: a prospective blinded observational study. Anesth Analg 121:709–715. https://doi.org/10.1213/ANE.0000000000000836
Taenzer AH, Pyke J, Herrick MD, Dodds TM, McGrath SP (2014) A comparison of oxygen saturation data in inpatients with low oxygen saturation using automated continuous monitoring and intermittent manual data charting. Anesth Analg 118:326–331. https://doi.org/10.1213/ANE.0000000000000049
Saab R, Wu BP, Rivas E, Chiu A, Lozovoskiy S, Ma C, Yang D, Turan A, Sessler DI (2021) Failure to detect ward hypoxaemia and hypotension: contributions of insufficient assessment frequency and patient arousal during nursing assessments. Br J Anaesth 127:760–768. https://doi.org/10.1016/j.bja.2021.06.014
Haahr-Raunkjaer C, Mølgaard J, Elvekjaer M, Rasmussen SM, Achiam MP, Jorgensen LN, Mette et al (2022) Continuous monitoring of vital sign abnormalities; association to clinical complications in 500 postoperative patients. Acta Anaesthesiol Scand 552:552–562. https://doi.org/10.1111/aas.14048
Taenzer AH, Pyke JB, McGrath SP, Blike GT (2010) Impact of pulse oximetry surveillance on rescue events and intensive care unit TransfersA Before-and-after concurrence study. Anesthesiology 112:282–287. https://doi.org/10.1097/ALN.0B013E3181CA7A9B
Jencks SF, Williams MV, Coleman EA (2009) Rehospitalizations among patients in the medicare fee-for-service program. N Engl J Med 360:1418–1428. https://doi.org/10.1056/nejmsa0803563
Hartl S, Lopez-Campos JL, Pozo-Rodriguez F, Castro-Acosta A, Studnicka M, Kaiser B, Michael Roberts C (2016) Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD Audit. Eur Respir J 47:113–121. https://doi.org/10.1183/13993003.01981-2015
Breteler MJM, KleinJan EJ, Dohmen DAJ, Leenen LPH, van Hillegersberg R, Ruurda JP, van Loon K, Blokhuis TJ, Kalkman CJ (2020) Vital signs monitoring with wearable sensors in high-risk surgical patients a clinical validation study. Anesthesiology. https://doi.org/10.1097/ALN.0000000000003029
Jencks SF, Williams MV, Coleman EA (2009) Rehospitalizations among patients in the medicare fee-for-service program. N Engl J Med 361:311–312. https://doi.org/10.1056/NEJMC090911
Funding
This work was supported by the Innovation Fund Denmark [8056-00055B], Capital Region of Denmark’s Research Foundation, Bispebjerg Hospital, Rigshospitalet, and Technical University of Denmark. No sponsor had any role in the study design, collection of data, analysis, access to the data, interpretation of data, writing, or the decision to submit the article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Christian S. Meyhoff and Eske K. Aasvang have founded a start-up company, WARD247 ApS, to pursue the WARD-projects regulatory and commercial activities. WARD247 ApS has finalized terms for license agreement for any WARD-project software and patents, of which one has been filed. WARD247 ApS has not had any influence on the study design, conduct, analysis or reporting. Christian S. Meyhoff and Eske K. Aasvang reports lecture fees from Radiometer. Nicharatch Songthawornpong, Mikkel Elvekjaer, Jesper Mølgaard, Søren M Rasmussen and Vibeke R. Eriksen declare no conflict of interest.
Human and animal rights
This analysis was based upon data from two previous observational studies (NCT03491137 and NCT03660501), both approved by the Danish Data Protection Agency.
Informed consent
Written informed consent was obtained prior to inclusion.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Songthawornpong, N., Elvekjaer, M., Mølgaard, J. et al. Deviating vital signs in continuous monitoring prior to discharge and risk of readmission: an observational study. Intern Emerg Med 18, 1453–1461 (2023). https://doi.org/10.1007/s11739-023-03318-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-023-03318-4