
Abstract
The use of virtual reality for simulations plays an important role in the initial training for robotic surgery. This randomized controlled trial aimed to investigate the impact of educational video on the performance of robotic simulation. Participants were randomized into the intervention (video) group that received an educational video and robotic simulation training or the control group that received only simulation training. The da Vinci® Skills Simulator was used for the basic course, including nine drills. The primary endpoint was the overall score of nine drills in cycles 1–10. Secondary endpoints included overall, efficiency, and penalty scores in each cycle, as well as the learning curves evaluated by the cumulative sum (CUSUM) analysis. Between September 2021 and May 2022, 20 participants were assigned to the video (n = 10) and control (n = 10) groups. The video group had significantly higher overall scores than the control group (90.8 vs. 72.4, P < 0.001). Significantly higher overall scores and lower penalty scores were confirmed, mainly in cycles 1–5. CUSUM analysis revealed a shorter learning curve in the video group. The present study demonstrated that educational video training can be effective in improving the performance of robotic simulation training and shortening the learning curve.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
An increasing number of procedures are being performed as robotic surgery in the fields of gastroenterology, urology, and gynecology [1]. Robotic surgery can provide various advantages, including high-definition 3D views, a crystal-clear surgical field view, tremor-filtration technology, and articulated instruments. Specific surgical skills and training are required to be independent robotic surgeons. Hence, the structured training program for robotic surgery has been developed with the aim of translating skill from training to clinical practice in the operating room [2, 3]. In our training model that consisted of simulation, biotissue and video training, the use of virtual reality simulation played an important initial role in educating experienced surgeons and surgical trainees. The importance of virtual reality simulator training in robotic surgery has been advocated [4,5,6,7]. However, to date, only a few studies have investigated the effects of educational videos on the performance of robotic simulation training.
This study aimed to investigate the impact of educational video on performance of robotic simulation training, called the Training program in Okayama University for minimally invasive surgery (TAKUMI-1). Furthermore, the effect of the educational video on the learning curve for robotic simulation training was evaluated using a cumulative sum (CUSUM) analysis.
Methods
Trial design
We performed a randomized controlled trial with two parallel training groups; one group received an educational video and robotic simulation training (video group), while the other received simulation training alone (control group). The study protocol was approved by the institutional ethics committee of (No: 2108–017) and was registered at the University Hospital Medical Information Network (No: UMIN000045495). The Consolidated Standards of Reporting Trials (CONSORT) guidelines were followed [8]. Written informed consent was obtained from all participants prior to enrollment and randomization.
Participants
Robotic surgery trainees in our department were recruited between September 2021 and May 2022. The participants included experienced surgeons and surgical trainees who had no experience with robotic simulation training.
Robotic simulation training
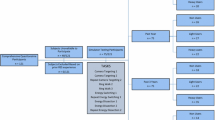
This study was performed using a da Vinci® Skills Simulator (Intuitive Surgical Inc., Sunnyvale, CA, USA). The da Vinci® Skills Simulator for the basic course, including nine drills, was used for this trial: drill 1, sea spikes 1; drill 2, sea spikes 2; drill 3, camera targeting 1; drill 4, suture sponge 1; drill 5, thread the ring; drill 6, energy switching 1; drill 7, ring and rail 1; drill 8, needle targeting; and drill 9, 30° scope swap (Supplementary Table 1). The exercise goals for each drill are listed in Supplementary Table 1.
Intervention
Educational videos on the tips and tricks of each drill were created by the principal investigator (KT) (Supplementary Table 1). The participants in both groups received robotic simulation training. However, the video group received an additional educational video training for a few hours prior to starting the robotic simulation. All participants had to perform the nine drills consecutively as one cycle, and complete 10 cycles in total.
Primary and secondary endpoints
Assessment outcomes for each drill included overall, efficiency, and penalty scores. Efficiency scores were calculated by evaluating the time to completion, economy of motion, or master workspace range. Penalty scores consisted of excessive force use, instruments out of view, drops, instrument and cone collisions, incorrect rings, missed targets, and misapplied energy time. The overall scores were calculated by subtracting the penalty from the efficiency scores.
The primary endpoint was the overall score of all drills in cycles 1–10 in both groups. The secondary endpoint included the overall, efficiency, and penalty scores in each cycle and drill, as well as the learning curves between the groups.
Sample size and randomization
The sample size was calculated based on the primary end point. Assuming a difference in the mean overall scores between the groups of 15 with a standard deviation of 10 according to our unpublished data, this study required a total sample size of 20 participants (10 participants for each group) to achieve a power of 90% and an alpha error of 5% (two-sided).
Randomization was performed by the principal investigator using a random number (Excel RAND) function. The participants were randomly divided into two groups: video and control.
Statistical analysis
Statistical analysis and sample size calculation were performed using the JMP 11.2.0 software (SAS Institute, Cary, NC, USA). First, the overall, efficiency, and penalty scores of all drills in cycles 1–10 were compared between the video and control groups. Subsequently, the overall, efficiency, and penalty scores in each cycle as well as each drill were analyzed and compared between both groups. Moreover, the detailed penalty scores for each drill were compared between the groups. Finally, a CUSUM analysis was performed to compare the learning curves between the groups. The cumulative sums of the differences in each drill from the total “time to completion” were calculated based on the cycle. A pooled mean CUSUM was plotted to summarize the results [9, 10]. Data are presented as the mean (standard deviation) for continuous variables. Differences between groups were evaluated using Student’s t test or Mann–Whitney U test for continuous variables. Statistical significance was set at P < 0.05.
Results
Participant flow
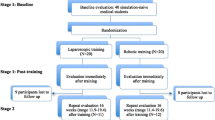
The CONSORT flow diagram is shown in Fig. 1. A total of 20 participants were assigned either to the video (n = 10) or the control (n = 10) group (Table 1). Their specialities included gastrointestinal (n = 10) or hepatopancreatobiliary surgery (n = 10). All participants completed 100% of the curriculum in both groups.

CONSORT flow diagram of the trial
Outcomes
The overall, efficiency, and penalty scores of all drills in cycles 1–10 between the video and control groups are shown in Table 2. The video group had significantly higher overall scores than the control group (90.8 vs. 72.4; P < 0.001).
The overall, efficiency and penalty scores in each cycle between the groups are shown in Fig. 2. The trend of significantly higher overall and lower penalty scores was confirmed mainly in cycles 1–5. The overall, efficiency and penalty scores for each drill between the groups are shown in Fig. 3. The overall score was significantly higher in the video group than in the control group in four out of the nine drills (drills 2, 4, 8, and 9). The video group had significantly lower penalty scores than the control in six drills (drills 2, 3, 4, 6, 8, and 9). The video group had lower penalty scores in collisions and out-of-view instruments than in the control group (Supplementary Fig. 1).

a Overall, b efficiency, and c penalty scores in each cycle for the video and control groups. *P < 0.05

a Overall, b efficiency, and c penalty scores in each drill for the video and control groups. V video group, C control group. *P < 0.05
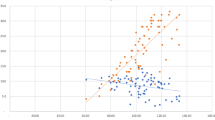
The CUSUM analysis of the total “time to completion” in each drill between the groups is depicted in Fig. 4. The video group reached a plateau within two cycles, and improved after four cycles. In contrast, the control group required 4 cycles to reach a plateau.

The cumulative sum (CUSUM) analysis of the total “time to completion” in each cycle
Discussion
This is the first randomized controlled trial to investigate the impact of educational videos on the performance of robotic simulation training. We found that educational video training improved the performance in robotic simulation. Moreover, CUSUM analysis confirmed the positive effect of the educational video on shortening the learning curve.
Educational video should be exemplary for early training in robotic surgery and have the potential to maximize trainees’ learning and skill improvement [11]. Video training could allow preparation prior to starting surgical training. Furthermore, a video-based education system can provide best practices by improving surgical quality and reducing learning curves for complex robotic procedures [12]. Accordingly, video-based education should be an effective method in surgical education [13, 14].
Regarding the evidence on robotic simulation training, several randomized controlled trials have been performed to investigate the effect of an affordable surgical robot simulator or procedural virtual reality, showing effective impact in improving robotic surgical skills [15, 16]. However, few studies have examined the effects of educational videos on the performance of robotic simulation training so far. Therefore, our study observed novel findings that demonstrated the efficiency of educational video for improving the performance in robotic simulation.
We determined that the overall scores of all drills, would be the best index for estimating the impact of educational video training. The mean overall scores in the video group were 18.4 times higher than those in the control group, probably due to educational video training.
Participants in the control group improved their overall, efficiency and penalty scores through self-learning, and eventually reached the same level as that of the video group. However, the video group had significantly higher efficiency and lower penalty scores, especially during the initial phase. We propose that participants in the video group had improved their scores through both educational video training and self-learning. The penalty scores in the video group were lower throughout the drills, especially in collisions and out-of-view instruments (Fig. 3 and Supplementary Fig. 1), than in the control group. This may be explained by the fact that educational video training can increase the ability to recognize spatial cognition.
CUSUM analysis has been used to evaluate the learning curves for surgical procedures [9, 10]. As “time to completion” is a useful predictor of efficiency scores, we believe that the total time required to complete each drill is a good indicator of the evaluation of the learning curves. Interestingly, our learning model using CUSUM analysis showed different learning curves between the two groups. The findings suggested a significant effect of educational video training on shortening learning curves.
Considering the positive effect of video training, our findings indicate that surgical video training could lead to improved robotic surgery performance in the clinical setting. Therefore, a structured training model for robotic surgery, that includes simulation, biotissue, and video training, should improve surgical skills and shorten learning curves [17, 18]. A recent meta-analysis demonstrated that surgical skills acquired through robotic simulator training can be translated to the operating room with regards to time and technical performance [4]. Moreover, it suggested potential benefits that could justify simulator training in structured robotic training programs and emphasized the role of simulation training before performance in a real operating room.
The present study had several limitations. Although this was a randomized controlled trial, the sample size was small. Further studies with larger sample sizes are required to externally validate our findings. The association between the performance of simulation training and performance in a real operating room has not yet been investigated. Therefore, future studies focusing on these are required to confirm the effect of simulation training on performance in the clinical setting. Finally, the effect of educational video on each drill was unclear. A further investigation should be helpful to understand which surgical skills can be improved through the video training.
In conclusion, this study demonstrated that educational video training can be effective in improving the performance of robotic simulation training and shortening the learning curve.
References
Intuitive Surgical. Annual Report 2021. Accessed 1 September 2022, from https://www.annualreports.com/Company/intuitive-surgical-inc.
Takagi K, Umeda Y, Yoshida R, Yagi T, Fujiwara T, Zureikat AH, Hogg ME, Koerkamp BG (2021) Surgical training model and safe implementation of robotic pancreatoduodenectomy in Japan: a technical note. World J Surg Oncol 19(1):55
Zwart MJW, Nota CLM, de Rooij T, van Hilst J, Te Riele WW, van Santvoort HC, Hagendoorn J, Rinkes I, van Dam JL, Latenstein AEJ, Takagi K, Tran TCK, Schreinemakers J, van der Schelling G, Wijsman JH, Festen S, Daams F, Luyer MD, de Hingh I, Mieog JSD, Bonsing BA, Lips DJ, Hilal MA, Busch OR, Saint-Marc O, Zeh HJ, Zureikat AH, Hogg ME, Molenaar IQ, Besselink MG, Koerkamp BG, G. Dutch Pancreatic Cancer (2022) Outcomes of a Multicenter Training Program in Robotic Pancreatoduodenectomy (LAELAPS-3). Ann Surg 276(6):e886–e895. https://doi.org/10.1097/SLA.0000000000004783
Schmidt MW, Koppinger KF, Fan C, Kowalewski KF, Schmidt LP, Vey J, Proctor T, Probst P, Bintintan VV, Muller-Stich BP, Nickel F (2021) Virtual reality simulation in robot-assisted surgery: meta-analysis of skill transfer and predictability of skill. BJS Open. https://doi.org/10.1093/bjsopen/zraa066
Costello DM, Huntington I, Burke G, Farrugia B, O’Connor AJ, Costello AJ, Thomas BC, Dundee P, Ghazi A, Corcoran N (2022) A review of simulation training and new 3D computer-generated synthetic organs for robotic surgery education. J Robot Surg 16(4):749–763
Thornblade LW, Fong Y (2021) Simulation-based training in robotic surgery: contemporary and future methods. J Laparoendosc Adv Surg Tech A 31(5):556–560
Schlegel C, Zureikat AH (2021) The role of simulation in attaining proficiency in minimally invasive hepatopancreatobiliary surgery. J Laparoendosc Adv Surg Tech A 31(5):561–564
Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, G. A. Lancaster and P. C. group (2016) CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ 355:i5239
Takagi K, Outmani L, Kimenai HJAN, Terkivatan T, Tran KTC, Ijzermans JNM, Minnee RC (2020) Learning curve of kidney transplantation in a high-volume center: Cohort study. Int J Surg 80:129–134
Takagi K, Kimenai H, Terkivatan T, Tran KTC, Ijzermans JNM, Minnee RC (2021) Learning curves of minimally invasive donor nephrectomy in a high-volume center: A cohort study of 1895 consecutive living donors. Int J Surg 86:7–12
Celentano V, Smart N, McGrath J, Cahill RA, Spinelli A, Challacombe B, Belyansky I, Hasegawa H, Munikrishnan V, Pellino G, Ahmed J, Muysoms F, Saklani A, Khan J, Popowich D, Ballecer C, Coleman MG (2021) How to report educational videos in robotic surgery: an international multidisciplinary consensus statement. Updates Surg 73(3):815–821
Hogg ME, Besselink MG, Clavien PA, Fingerhut A, Jeyarajah DR, Kooby DA, Moser AJ, Pitt HA, Varban OA, Vollmer CM, Zeh HJ, Hansen P, Committee MIPRO (2017) Training in minimally invasive pancreatic resections: a paradigm shift away from “See one, Do one, Teach one.” HPB (Oxford) 19(3):234–245
Ahmet A, Gamze K, Rustem M, Sezen KA (2018) Is video-based education an effective method in surgical education? a systematic review. J Surg Educ 75(5):1150–1158
Augestad KM, Butt K, Ignjatovic D, Keller DS, Kiran R (2020) Video-based coaching in surgical education: a systematic review and meta-analysis. Surg Endosc 34(2):521–535
Hardon SF, Kooijmans A, Horeman R, van der Elst M, Bloemendaal ALA, Horeman T (2022) Validation of the portable virtual reality training system for robotic surgery (PoLaRS): a randomized controlled trial. Surg Endosc 36(7):5282–5292
Raison N, Harrison P, Abe T, Aydin A, Ahmed K, Dasgupta P (2021) Procedural virtual reality simulation training for robotic surgery: a randomised controlled trial. Surg Endosc 35(12):6897–6902
Rice MK, Hodges JC, Bellon J, Borrebach J, Al Abbas AI, Hamad A, Knab LM, Moser AJ, Zureikat AH, Zeh HJ, Hogg ME (2020) Association of mentorship and a formal robotic proficiency skills curriculum with subsequent generations’ learning curve and safety for robotic pancreaticoduodenectomy. JAMA Surg 155(7):607–615
Al Abbas AI, Wang C, Hamad AB, Knab LM, Rice MK, Moser AJ, Zeh HJ 3rd, Zureikat AH, Hogg ME (2021) Mentorship and formal robotic proficiency skills curriculum improve subsequent generations’ learning curve for the robotic distal pancreatectomy. HPB (Oxford) 23(12):1849–1855
Funding
Open access funding provided by Okayama University. Financial support was received from Japan Society for the Promotion of Science (grant number 21K16447) and the Okayama Medical Foundation.
Author information
Authors and Affiliations
Contributions
K.T. wrote the main manuscript. K.T., N.H., and J.K. prepared figures. All authors contributed to this study, and reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Kosei Takagi, Nanako Hata, Jiro Kimura, Satoru Kikuchi, Kazuhiro Noma, Kazuya Yasui, Tomokazu Fuji, Ryuichi Yoshida, Yuzo Umeda, Takahito Yagi, and Toshiyoshi Fujiwara have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Takagi, K., Hata, N., Kimura, J. et al. Impact of educational video on performance in robotic simulation training (TAKUMI-1): a randomized controlled trial. J Robotic Surg 17, 1547–1553 (2023). https://doi.org/10.1007/s11701-023-01556-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-023-01556-4