
Abstract
Purpose
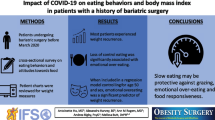
To estimate the association of emotional distress with both consumption of energy-dense micronutrient-poor foods (EDF) and body mass index (BMI) and the association between EDF consumption and change in BMI, during COVID-19 pandemic in patients with prior bariatric surgery.
Materials and Methods
This cross-sectional study applied an online structured questionnaire to 75 postoperative bariatric patients during the first Portuguese lockdown. Emotional distress was assessed trough the Hospital Anxiety and Depression Scale (HADS) and dietary intake was evaluated by Food Frequency Questionnaire (FFQ). Self-reported BMI prior to and at the end of confinement was used to compute BMI change. Pre-surgery BMI was computed from measured height and weight from clinical records.
Results
After adjustment for education, sex, time since surgery, pre-surgery BMI, and exercise practice, moderate/severe scores in HADS were significantly positively associated with consumption of EDF (ẞ = 0.799; 95% CI: 0.051, 1.546), but not with BMI. Daily EDF consumption significantly increased the odds of maintaining/increasing BMI (OR = 3.34; 95% CI: 1.18, 9.45), instead of decreasing it (reference). Sweets consumption was the only subcategory of EDF significantly positively associated with the odds of a worse outcome in BMI change (OR = 4.01; 95% CI: 1.13, 14.22).
Conclusions
Among postoperative bariatric patients, higher reported levels of emotional distress during confinement are associated with increased EDF consumption. Increased EDF consumption during confinement, particularly sweets, is associated with higher odds of bariatric patients not decreasing their BMI. Additional effort is needed to address inadequate lifestyle behaviors among these patients in the context of the COVID-19 pandemic.
Graphical abstract

Similar content being viewed by others

Introduction
With the COVID-19 pandemic, a serious disruption of health-care services ensued, with a particular impact on metabolic and bariatric surgery. In April 2020, the International Federation for the Surgery of Obesity (IFSO) issued recommendations for health-care providers, advising postponement of metabolic and bariatric surgery and remote follow-up of patients via virtual means [1]. In July 2020, the Diabetes Surgery Summit (DSS) recommendations [2] emphasized the repercussions of limited access to non-urgent care and the detrimental effect to postoperative monitoring of patients who underwent bariatric surgery, providing early guidance for postoperative surveillance.
Results from a worldwide survey to bariatric surgeons showed a strong impact on clinical practice regarding surgical and outpatient monitoring, with postponement of appointments replaced by video calls [3]. Mandatory lockdowns, physical distancing, and self-isolation practices also contributed to a shift from in-person to remote monitoring of patients that underwent metabolic and bariatric surgery [4].
In Portugal, the first cases of infection by SARS-CoV-2 were confirmed on the 2nd of March 2020 [5]. On the 18th of March 2020, with 642 infections [6], the state of emergency was declared, stating the prohibition of unjustified travel, cross-border controls and mandatory confinement [7]. During this confinement period, which lasted until the 3rd of May 2020, access to non-urgent care was halted in most Portuguese health services, and in-person appointments were cancelled with substantial impact on outpatient follow-up and on bariatric surgery.
Increased emotional distress was likely in the context of the COVID-19 pandemic, and psychological concerns in metabolic and bariatric surgery were stressed early, highlighting the propensity of a detrimental effect in adherence to treatment and patients’ outcomes [4, 8, 9]. A French bariatric multidisciplinary team conducted a global survey on the behavioral modification towards food consumption during the third week of confinement, finding that stress, feeling of emptiness, and boredom were managed with food consumption and that these three emotional eating behaviors were significantly positively associated with lower physical activity [10].
Evidence on emotional distress, dietary intake, and body mass index (BMI) during the COVID-19 pandemic, either in candidates or patients that underwent metabolic and bariatric surgery, is scarce. A Spanish study in a cohort of patients waiting for bariatric surgery published in the end of 2020 showed that, during the COVID-19 lockdown, BMI increased, and both the obesity surgery score and health-related quality of life worsened mainly due to psychological issues [11]. Also, an online survey conducted in Poland during the pandemic revealed that 75% of pre- or postoperative patients felt anxiety, while 30% reported increased BMI [12]. Regarding both emotional distress and dietary intake, a survey, conducted in an academic hospital in the United States of America (USA) that included 208 patients who underwent surgery, reported increased depression, as well as increased snacking, loss of control when eating, and binge eating [13]. Likewise, another study from the USA [14] reported higher anxiety and depression and stress eating, as well as lower time and intensity in exercise. These studies evaluated emotional distress either with a single question for anxiety [12], with few questions selected from distinct validated instruments for anxiety and depression [13], or by the complete 16-items Quick Inventory of Depressive Symptoms [14] and did not formally evaluate the association between emotional distress and EDF consumption.
Formal estimation of associations of emotional distress with dietary intake, as well as of diet with BMI during the COVID-19 pandemic, is of particular importance among patients with obesity that underwent metabolic and bariatric surgery. In our practice, patients are followed at 1, 3, 6, 9, and 12 months during the first year, and every 6 months afterwards. During the first Portuguese confinement (March to May 2020), scheduled in-person follow-up appointments were postponed and replaced by remote video or telephone calls. Considering that higher emotional distress, lower practice of physical exercise, and lower adherence to a healthy diet were likely, we aimed to evaluate these associations. In addition, we considered that evaluation of consumption of energy-dense micronutrient-poor foods and beverages (EDF) was crucial, as weight regain in these patients has been related to snacking behaviors and to excessive intake of sweets and fatty foods [15, 16].
As such, the objective of the current study was to estimate the association of emotional distress with both consumption of EDF and BMI, as well as to evaluate the association between consumption of EDF and BMI, during the first COVID-19 lockdown in Portugal, among patients with prior metabolic and bariatric surgery.
Materials and Methods
Participants and Settings
During the first mandatory confinement in Portugal (from the 18th of March until the 3rd of May 2020), access to non-urgent care was halted in most Portuguese health services. This confinement affected both the public and the private health services, including Hospital CUF Tejo, a private Portuguese hospital, where our Obesity and Metabolic Surgery Unit is embedded. Bariatric surgery, as well as in-person appointments, were cancelled. Hence, patients with prior bariatric surgery had to be monitored by alternative means (telephone, telemedicine, and an application (Nutrium ©, HEALTHIUM – Healthcare Software Solutions, Braga, Portugal) which was already used by the nutrition service for medical nutrition therapy). During this distanced follow-up, several difficulties were reported by our patients including increased anxiety and snacking. Keeping in mind these reported behaviors, we designed a cross-sectional study that aimed to collect information during the confinement period.
This study included patients with obesity from the Obesity and Metabolic Surgery Unit of Hospital CUF Tejo who underwent metabolic and bariatric surgery prior to the lockdown. As shown in the flow-chart (Figure 1), enrollment started 6 weeks after the mandatory lockdown between the 29th of April and the 5th of May 2020. A total of 122 adult patients met the inclusion criteria (> 18 years of age, submitted to bariatric surgery prior to the lockdown between September 2018 and March 2020), of which 81 accepted to participate (participation proportion, 66.4%). Exclusion criteria were patients still following modified texture diets (n = 4), with reoperation (n = 1), or duodenal switch (n = 1). As such, 75 patients who underwent laparoscopic sleeve gastrectomy or Roux-en-Y gastric bypass (RYGB), either laparoscopic or robotic, remained for final analysis. Information was collected through an online structured questionnaire to obtain data on emotional distress (anxiety and depression), dietary intake, and BMI during the mandatory confinement due to COVID-19.

This figure illustrates the study time frame, inclusion and exclusion criteria. A total of 75 patients were included in the analysis
The study was approved by the ethics research committees of NOVA Medical School and of CUF Tejo, and all procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments, as well as with the standards laid down by the Portuguese Data Protection Authority. An online informed consent was collected for each individual participant.
Emotional Distress (Anxiety and Depression)
Emotional distress was evaluated by the Portuguese version of the Hospital Anxiety and Depression Scale (HADS) [17], previously validated for the Portuguese population with chronic disease [18], applied online. Anxiety and depression subscales each included seven items rated in a 4-point Likert scale ranging from 0 to 3. Total scores for each subscale were computed ranging from 0 to 21. These scores can be categorized into normal (0–7), mild (8–10), and moderate/severe (11–21) [17]. A total HADS score was also computed by summing up the scores for the 14 items, ranging from 0 to 42 points. According to the cut-offs proposed for each of the subscales [17], these scores were further categorized into normal (0 to 14 points, reference category), mild (15 to 20 points), and moderately/severely (≥ 21 points).
Dietary Information
Dietary intake was evaluated by a semi-quantitative Food Frequency Questionnaire (FFQ) adapted from a questionnaire previously validated for the Portuguese general adult population [19], shortened for application in the current study. The FFQ was embedded in the online questionnaire and was self-completed by participants, querying about how many times, on average, participants consumed 40 food items during the previous month. Considering the purpose of the current study, 20 food items within the questionnaire evaluated consumption of EDF. Seven response options were available, ranging from never to ≥ 2 times/day. These were further converted into daily frequencies (e.g., ≥ 2 times per day was converted into 2 times/day, 5–6 times/week was considered as 5.5 times/week which, divided by 7 days, corresponds to 0.79 times/day). By summing up these daily frequencies, three groups of EDF were defined: sweets (cakes, biscuits, chocolate, sugar, candies, ice cream, deserts); fatty foods (processed meat, crisps, french fries, salty pastry, fast food); and sugar-sweetened beverages (colas, other carbonated beverages, iced tea, non-carbonated beverages). Total consumption of EDF was also computed by the sum of daily consumption frequencies of these items and was used as continuous in all analyses.
Anthropometrics
Weight prior to and weight at the end of the confinement period were self-reported, patients being instructed to measure their weight at the same time with light clothes. Height and weight prior to surgery were retrieved from electronic clinical records of the first face-to-face visit to the nutrition appointment. Height was measured to the nearest 0.1 cm with a wall stadiometer (SECA®, Hamburg, Germany) and weight was measured to the nearest 0.1 kg with the InBody 770 (InBody® Co. Ltd., Seoul, Korea).
Participants’ BMI was computed for three moments (pre-operative, pre-confinement, at the end of confinement). Change in BMI during confinement was computed as BMI at the end of confinement minus BMI prior to it, further categorized into maintained/increased vs. decreased (reference category).
Potential Confounding Factors
Potential confounders considered were education, defined as the number of completed schooling years; monthly per capita income; participants exact age in years; sex; time since surgery; type of surgical procedure; BMI prior to surgery; and exercise practice during confinement, defined as no vs. yes.
Statistical Analysis
To evaluate the association of participants’ characteristics with the main exposure of interest (EDF consumption) and the outcome (BMI), linear regression models, crude and adjusted, were fitted to estimate regression coefficients and respective 95% confidence intervals (ẞ, 95% CI).
To assess the association between EDF consumption and BMI change during confinement (categorized into maintained/increased vs. decreased as reference category), crude and adjusted odds ratios (OR) and respective 95% CI were estimated using binomial logistic regression models. Four separately fitted models were considered: total EDF consumption; sweets; fatty foods; and sugar-sweetened beverages.
Potential confounding factors were individually assessed in each model, and those that did not change the associations of interest (HADS with EDF, and EDF with BMI) were not included in the final analyses (participants’ age and income). Hence, final models were adjusted for education (completed schooling years), sex (female vs. male as reference category), exercise practice (no vs. yes as reference category), time since surgery (months, continuous variable), and type of procedure (sleeve gastrectomy vs. RYGB as reference category).
Statistical analysis was conducted using SPSS statistical software package version 27 (SPSS Inc., Chicago, IL, USA) and a significance level of 5% was adopted.
Results
Participants’ characteristics are presented in Table 1. Physical exercise practice during confinement was reported only by 34.7% of participants. Mean time since surgery was 9.8 months (standard deviation (SD) = 5.14) and 29.3% individuals were submitted to sleeve gastrectomy. HADS scores were mild in 18.7% and moderate/severe in 8.0% participants. Total daily EDF consumption frequency was high during the confinement period (mean = 0.9 times/day, SD = 0.96), and 37.3% of participants did not decrease BMI during confinement.
In fully adjusted models (Table 2), moderate/severe score in HADS, when compared to normal (reference), was significantly positively associated with consumption of EDF (ẞ = 0.799; 95% CI: 0.051, 1.546). Likewise, patients with sleeve gastrectomy, when compared to those with RYGB, showed increased daily consumption frequency of total EDF by 0.530 times/day (95%CI: 0.070, 0.990).
Increased scores in HADS were not associated with BMI at the end of the confinement period, neither in crude nor in fully adjusted models (Table 2). Other variables independently and significantly positively associated with BMI at the end of confinement were time since surgery (ẞ = 0.102; 95% CI: 0.054, 0.149), BMI prior to confinement (ẞ = 0.883; 95% CI: 0.826, 0.940), and physical exercise practice (ẞ = 0.576; 95% CI: 0.198, 0.955). A positive association between consumption of EDF and BMI at the end of the confinement period was observed in fully adjusted models but did not reach statistical significance (p value = 0.083).
When considering BMI change, in fully adjusted models (Table 3), for each increase in daily consumption of EDF, a three-fold increase in the odds of maintaining or increasing BMI during confinement, vs. decreasing BMI, was observed (OR = 3.34; 95% CI: 1.18, 9.45). Regarding separate groups of EDF, only sweets were positively and significantly associated with the odds of a worse BMI outcome (OR = 4.01; 95% CI: 1.13, 14.22).
Discussion
This study shows that, among Portuguese individuals with previous metabolic and bariatric surgery, moderately to severely increased emotional distress during confinement due to the COVID-19 pandemic is associated with higher consumption of EDF which, in turn, is significantly positively associated with a worse outcome in BMI change, particularly for sweets’ consumption. It also shows that time since surgery and lack of physical exercise practice are associated with higher BMI at the end of confinement.
Increased BMI during lockdown due to the COVID-19 outbreak and mildly worsened health-related quality of life and changes in diet have been reported in a Spanish study among a cohort of patients on the waiting list for metabolic and bariatric surgery [20]. In a Brazilian cohort of recently operated patients, during the COVID-19 lockdown, a relatively high intake of ultra-processed foods was shown [21]. In a study conducted in the USA [14] including patients who underwent metabolic and bariatric surgery, increased anxiety and depression were also reported during stay-at-home orders, as were difficulty in achieving weight loss goals, lower time spent practicing physical exercise, and increased stress eating. Yet, these findings are only partially comparable to those in the present sample, as these studies did not formally evaluate associations of emotional distress with dietary intake, nor associations between diet and BMI.
In contrast, the association between dietary intake and BMI was formally assessed in a sample of 208 patients with previous metabolic and bariatric surgery, during the COVID-19 outbreak in the USA [13]. Increased BMI, depression, snacking behavior, and lower activity levels were observed, and consumption of less healthy food was positively associated with weight gain. These findings give strength to those of the current study. Still, results are comparable to current findings only in part, as in the sample from USA depression and anxiety were assessed with 2 questions each derived from distinct instruments which may not capture the same construct as in the current sample where a complete validated instrument with 14 items (7 for anxiety and 7 for depression) was applied. Also, in the sample from the USA, the association of depression or anxiety with dietary intake was not formally assessed.
Finding that sleeve gastrectomy was positively associated with consumption of EDF deserves to be discussed. Two studies in Spanish samples [22, 23] evaluated weight changes during confinement in patients with prior sleeve gastrectomy. In one sample [22], confinement did not show a detrimental effect on weight loss, while in the other [23], increased self-reported weight was shown during confinement for patients that underwent sleeve gastrectomy with lower weight gain being reported among those practicing regular physical exercise. We did not find an association between sleeve gastrectomy and BMI, but we did find that, in comparison to patients that underwent RYGB, those with sleeve gastrectomy had significantly higher consumption of EDF. A possible explanation for this is that, although patients after either RYGB or sleeve gastrectomy show changes in taste and preference for sweets, fatty foods, and EDF, these changes tend to decrease with time post-sleeve gastrectomy but not post-RYGB [24].
Considering that dumping syndrome is frequent in RYGB [25], decreased fear of this syndrome among patients with sleeve gastrectomy, could be another explanation for current findings. Still, this syndrome may occur in procedures involving partial gastric resection and may appear in patients with sleeve gastrectomy [26]. In addition, sleeve gastrectomy is restrictive, while RYGB is also malabsorptive, which could explain a higher effect of EDF consumption in sleeve gastrectomy compared to RYGB. Another possible explanation could be the nuanced differences in the effect of RYGB and sleeve gastrectomy upon biological mechanisms that determine eating behavior, namely, a distinct impact upon gut-derived hormones and gut-brain signaling pathways [24].
Also, the positive association between time since surgery and BMI at the end of the confinement period should be discussed. Time since surgery in the current sample varied between participants. Weight regain, maintenance, or lower weight decrease would be expected to be more likely in patients with longer time since surgery. Likewise, patients further out from the surgery could have increased EDF consumption. Indeed, in the USA sample [13], loss of control while eating was more common among patients further out from their date of surgery and was associated with more weight gain. As such, we considered time since surgery as a confounding factor and, after adjustment, higher emotional distress was independently associated with EDF consumption which, in turn, was associated with higher odds of patients not decreasing their BMI independently of time since surgery. Still, patients further out from surgery may be more vulnerable and may require different support strategies during confinement.
Keeping in mind that in stressful circumstances BMI maintenance, as opposed to BMI increase, could be regarded as a reasonable outcome, aggregating patients that either maintained or increased their BMI within the same category should be addressed. A total of 20 patients showed BMI maintenance, while 17 patients increased their BMI during the confinement (mean = 0.8 kg/m2, SD = 0.55). The remaining 38 patients showed, clearly, a better outcome with a mean decrease in BMI of − 1.7 kg/m2 (SD = 1.20). Considering the small sample size, subgroup analysis could increase the likelihood of false negative findings [27]. In addition, mean time since surgery did not differ between participants maintaining or increasing their BMI (mean = 14.0, SD = 5.1 vs. mean = 14.2, SD = 4.00; p value = 0.907). As such, both maintenance and increases in BMI were considered as a worse outcome compared to BMI decrease and aggregation of patients within the same category was considered appropriate.
The cross-sectional nature of this study is a limitation that must be acknowledged, as it precluded the possibility of assessing indirect and direct effects of emotional distress, EDF consumption, and changes in BMI. However, considering evidence that emotional dysregulation can increase emotional eating and binge eating behaviors before and after metabolic and bariatric surgery [28, 29]; that stress, feeling of emptiness, and boredom were managed with food consumption during confinement [10]; and that increased emotional distress affects dietary compliance [28], we would expect that during the COVID-19 pandemic, increased levels of emotional distress would increase consumption of EDF which, in turn, would have a direct effect on BMI. Also, use of self-reported weight prior to and at the end of the confinement period is a limitation, as underreporting is common among patients with obesity [30]. Yet, our patients are instructed during nutritional appointments to monitor themselves, measuring weight always at the same circumstances (same scales, with light clothes, at the same time preferably in the morning). In addition, self-reported dietary intake is prone to social desirability bias. However, considering the positive association between increased emotional distress and EDF consumption, as well as between EDF consumption and worse outcome in post-confinement BMI, this bias, if present, did not obscure the expected associations of interest. Small sample size may have precluded enough statistical power for detecting an association between emotional distress and BMI, especially considering the adjustment for multiple potential confounding factors. Yet, statistical power was enough to show an association between EDF consumption and BMI. Still, current findings warrant confirmation in future studies.
Using the HADS total score instead of the scores of each subscale (anxiety and depression) should be addressed. Prior to categorizing the HADS total score, we performed a sensitivity analysis to assess if the separate subscales, as continuous variables, showed distinct associations with EDF consumption and BMI but did not find evidence of such differences (Supplementary material). As such, considering that HADS total has shown good performance in other patients [31], we deemed this approach as adequate.
Evaluating both emotional distress and EDF as exposures and their association with BMI is a strength of the current study since, to the best of our knowledge, this is the first study formally evaluating such associations. Also, the evaluation of patients with previous bariatric surgery during confinement due to the COVID-19 pandemic is a strength, considering that little is known regarding the pandemic’s effect in these patients [9]. In addition, using instruments validated for the Portuguese population is an advantage.
This study has implications for clinical practice. Considering that although telemedicine implementation is not yet widely adopted [32], its adoption was shown to increase follow-up visit volume [33]; protocols for monitoring patients after metabolic and bariatric surgery should implement measures that enable remote follow-up of these patients during confinement to minimize its detrimental effects on emotional distress, diet, and weight outcomes. Our patients were followed remotely during confinement and, still, increased levels of emotional distress were associated with EDF consumption, which was, in turn, associated with worse BMI outcome. As such, developments of new follow-up protocols for remote surveillance of these patients are warranted.
In conclusion, current results show that patients with previous bariatric surgery during the COVID-19 pandemic reporting higher levels of emotional distress are likely to increase consumption of EDF and that they are more likely to maintain or increase BMI, instead of decreasing it, during confinement periods. These patients are especially vulnerable to emotional distress and to inadequate lifestyle behaviors. As such, specific follow-up strategies with extra focus on emotional distress and consumption of EDF and emphasis on sweets’ consumption should be implemented in the clinical setting during confinement, with attention to exercise practice and a possible particular care for patients with sleeve gastrectomy.
References
Yang W, Wang C, Shikora SKL. Recommendations for metabolic and bariatric surgery during the COVID-19 pandemic from IFSO. Obes Surg. 2020;30(6):2071–3.
Rubino F, Cohen RV, Mingrone G, et al. Bariatric and metabolic surgery during and after the COVID-19 pandemic: DSS recommendations for management of surgical candidates and postoperative patients and prioritisation of access to surgery. Lancet Diabetes Endocrinol. 2020;8(7):640–8.
Lazaridis II, Kraljević M, Schneider R, et al. The impact of the COVID-19 pandemic on bariatric surgery: results from a worldwide survey. Obes Surg. 2020;30(11):4428–36.
Sockalingam S, Leung SE, Cassin SE. The impact of coronavirus disease 2019 on bariatric surgery: redefining psychosocial care. Obesity (Silver Spring). 2020;28(6):1010–2.
Direção-Geral da Saúde. Casos de infeção por novo Coronavírus (COVID-19) [Internet]. Lisboa; 2020. Available from: https://www.dgs.pt/a-direccao-geral-da-saude/comunicados-e-despachos-do-director-geral/atualizacao-de-02032020-1728-casos-de-infecao-por-novo-coronavirus-covid-19-pdf.aspx. Accessed 30 July 2020.
Direção Geral da Saúde. Relatório de Situação no 016 [Internet]. 2020. Available from: https://covid19.min-saude.pt/wp-content/uploads/2020/03/i026029.pdf. Accessed 30 July 2020.
República Portuguesa: XXII Governo. Decreto n.o 2-A/2020 [Internet]. Portugal: Diário da República n.o 57/2020, 1o Suplemento, Série I de 2020-03-20; 2020. Available from: hhttps://www.portugal.gov.pt/download-ficheiros/ficheiro.aspx?v=3f8e87a6-3cf1-4d0c-b5ee-72225a73cd4f. Accessed 30 July 2020.
Halpern BMM. Bariatric and metabolic surgery during and after the COVID-19 pandemic. Lancet Diabetes Endocrinol. 2020;8(9):741–2.
Yeo C, Ahmed S, Oo AM, et al. COVID-19 and obesity-the management of pre- and post-bariatric patients amidst the COVID-19 pandemic. Obes Surg. 2020;30(9):3607–9.
Cherikh F, Frey S, Bel C, et al. behavioral food addiction during lockdown: time for awareness, time to prepare the aftermath. Obes Surg. 2020;30(9):3585–7.
Beisani M, Vilallonga R, Petrola C, Acosta A, Pérez JAC, de Gordejuela AGR, et al. Effects of COVID-19 lockdown on a bariatric surgery waiting list cohort and its influence in surgical risk perception. Langenbeck's Arch Surg. 2021;406:393–40.
Walędziak M, Różańska-Walędziak A, Pędziwiatr M, et al. Bariatric surgery during covid-19 pandemic from patients’ point of view-the results of a national survey. J Clin Med. 2020;9(6):1697.
Athanasiadis DI, Hernandez E, Hilgendorf W, et al. How are bariatric patients coping during the coronavirus disease 2019 (COVID-19) pandemic? Analysis of factors known to cause weight regain among postoperative bariatric patients. Surg Obes Relat Dis. 2020;S1550-7289(20):30682-1.
Almandoz JP, Xie L, Schellinger JN, et al. Impact of COVID-19 stay-at-home orders on weight-related behaviours among patients with obesity. Clin Obes. 2020;10(5):e12386.
Freire RH, Borges MC, Alvarez-Leite JI, et al. Food quality, physical activity, and nutritional follow-up as determinant of weight regain after Roux-en-Y gastric bypass. Nutrition. 2012;28(1):53–8.
Karmali S, Brar B, Shi X, et al. Weight recidivism post-bariatric surgery: a systematic review. Obes Surg. 2013;23(11):1922–33.
Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–70.
Silva I, Pais-Ribeiro J, Cardoso H. Contributo para a adaptação da Hospital Anxiety and Depression Scale à população portuguesa com doença crónica. Psychologica. 2006;41:193–204.
Lopes C, Aro A, Azevedo A, et al. Intake and adipose tissue composition of fatty acids and risk of myocardial infarction in a male Portuguese community sample. J Am Diet Assoc. 2007;107(2):276–86.
Fakharian A, Moghadassi HA, Vasheghani M, Moghadasi AA. Bariatric surgery during the COVID-19 pandemic—the perspective of physicians and patients. Obes Surg. 2020;1–3. https://doi.org/10.1007/s11695-020-04998-z.
Nicoletti CF, Esteves GP, Genario R, Santo MA, de Cleva R, Gualano B, Roschel H. Nutritional inadequacies among post-bariatric patients during COVID-19 quarantine in Sao Paulo, Brazil. Obes Surg. 2020;1–5. https://doi.org/10.1007/s11695-020-05107-w [Epub ahead of print].
de Angulo DR, Román AB, Ruiz VM, Vázquez PJG, Merino GR, Escandell MAO, et al. Influence of the lockdown due to COVID-19 on weight-loss results during the first year after sleeve gastrectomy. Cir Esp. 2021;99(6):428–432. https://doi.org/10.1016/j.ciresp.2020.08.003.
de Luis D, Izaola O, Primo D, Gómez E, Torres B, López Gómez JJ, et al. Factors related to weight gain in subjects with sleeve gastrectomy during lockdown by the COVID-19 pandemic. Obes Surg. 2021;31(5):2197–2202. https://doi.org/10.1007/s11695-021-05253-9.
Zakeri R, Batterham RL. Potential mechanisms underlying the effect of bariatric surgery on eating behaviour. Curr Opin Endocrinol Diabetes Obes. 2018;25(1):3–11.
Malik S, Mitchell JE, Steffen K, et al. Recognition and management of hyperinsulinemic hypoglycemia after bariatric surgery. Obes Res Clin Pract. 2016;10(1):1–14.
Tack J, Deloose E. Complications of bariatric surgery: dumping syndrome, reflux and vitamin deficiencies. Best Pract Res Clin Gastroenterol. 2014;28(4):741–9.
Burke JF, Sussman JB, Kent DMHR. Three simple rules to ensure reasonably credible subgroup analyses. BMJ. 2015;351:h5651.
Shakory S, Van Exan J, Mills JS, et al. Binge eating in bariatric surgery candidates: the role of insecure attachment and emotion regulation. Appetite. 2015;91:69–75.
Taube-Schiff M, Van Exan J, Tanaka R, et al. Attachment style and emotional eating in bariatric surgery candidates: the mediating role of difficulties in emotion regulation. Eat Behav. 2015;18:36–40.
Sisto A, Vicinanza F, Tuccinardi D, Watanabe M, Gallo IF, D’Alessio R, et al. The psychological impact of COVID-19 pandemic on patients included in a bariatric surgery program. Eat Weight Disord. 2020;1–11. https://doi.org/10.1007/s40519-020-00988-3.
Vodermaier A, Millman RD. Accuracy of the Hospital Anxiety and Depression Scale as a screening tool in cancer patients: a systematic review and meta-analysis. Support Care Cancer. 2011;19(12):1899–908.
Runfola M, Fantola G, Pintus S, et al. Telemedicine implementation on a bariatric outpatient clinic during COVID-19 pandemic in Italy: an unexpected hill-start. Obes Surg. 2020;30(12):5145–9.
Brown AM, Ardila-Gatas J, Yuan V, et al. The impact of telemedicine adoption on a multidisciplinary bariatric surgery practice during the COVID-19 pandemic. Ann Surg. 2020;272(6):e306–10.
Acknowledgments
The authors gratefully acknowledge the participants enrolled in the current study for their kindness, generosity, and time in contributing with their personal information. We also acknowledge the support from the Obesity and Metabolic Surgery Unit of Hospital CUF Tejo, CUF Healthcare Group, and the support of the Lifestyle Medicine Unit of CUF Healthcare Group by NOVA Medical School.
Author information
Authors and Affiliations
Contributions
Catarina Durão performed statistical analyses and drafted the initial manuscript; Carlos Vaz contributed to the design of study, to the design of data collection instruments, and to the discussion of results. All authors contributed to the study’s conception and to the data collection instruments, revised the manuscript, and approved the final manuscript as submitted.
Corresponding author
Ethics declarations
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Keypoints
• In confinement, higher emotional distress is associated with higher EDF consumption, but not BMI.
• Sleeve gastrectomy is positively associated with EDF consumption during confinement.
• Higher EDF consumption is associated with a worse BMI outcome during confinement.
Supplementary information
ESM 1
(DOCX 23.1 kb)
Rights and permissions
About this article

Cite this article
Durão, C., Vaz, C., de Oliveira, V.N. et al. Confinement During the COVID-19 Pandemic After Metabolic and Bariatric Surgery—Associations Between Emotional Distress, Energy-Dense Foods, and Body Mass Index. OBES SURG 31, 4452–4460 (2021). https://doi.org/10.1007/s11695-021-05608-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-021-05608-2