
Abstract
Background
Gastroesophageal reflux disease (GERD) is a common disease among patients with obesity, with an associated prevalence of 39 to 61% between the population who attends a bariatric surgery evaluation. Laparoscopic sleeve gastrectomy (LSG) has become a popular and valid option for obesity treatment, even though the literature is ambivalent regarding the increase or decrease in GERD after this surgery. Thus, it is necessary to propose new surgical techniques as a solution to GERD in patients with a concomitant LSG or with a history of it. Therefore, we present a modified technique based on Hill’s gastropexy described originally in 1967.
Objective
Describe and propose a surgical procedure for GERD management based on the Hill technique that can be applied in all patients who undergo an LSG or with a history of it.
Methods
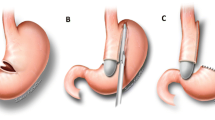
Retrospective observational study with a prospective database in which we described, Hill modified technique in a group of 16 patients with GERD who underwent this procedure concomitantly with an LSG or who presented with GERD after LSG with a 3-year follow-up. The surgical technique is based on an intra-abdominal esophageal length of a minimum of 3 cm and posterior fixation of the gastroesophageal junction to the crus.
Results
Postoperative controls have shown satisfactory results in the control and management of GERD symptoms in this group of patients, with very few to no complications associated with the procedure and without reintervention or medication out of the standard protocol.
Conclusion
Hill modified technique can be used and presented as an option for GERD control in patients with LSG.
Graphical abstract



Similar content being viewed by others


References
Moore M. Gastroesophageal reflux disease: a review of surgical decision making. World J Gastrointest Surg [Internet]. 2016;8(1):77–83. Available from: http://www.wjgnet.com/1948-9366/full/v8/i1/77.htm
Festi D, Scaioli E, Baldi F, et al. Body weight, lifestyle, dietary habits and gastroesophageal reflux disease. World J Gastroenterol. 2009;15(14):1690–701.
Hawasli A, Reyes M, Hare B, Meguid A, Harriott A, Almahmeed T, et al. Can morbidly obese patients with reflux be offered laparoscopic sleeve gastrectomy? A case report of 40 patients. Am J Surg [Internet] Elsevier Inc.; 2016;211(3):571–576. Available from: https://doi.org/10.1016/j.amjsurg.2015.11.006.
El-Serag HB. The association between obesity and GERD: a review of the epidemiological evidence. Dig Dis Sci. 2008;53(9):2307–12.
Kindel TL, Oleynikov D. The improvement of gastroesophageal reflux disease and Barrett’s after bariatric surgery. Obes Surg [Internet]. 2016;26(4):718–20. Available from: http://link.springer.com/10.1007/s11695-016-2116-1
Shabbir A, Dargan D. The success of sleeve gastrectomy in the management of metabolic syndrome and obesity. J Biomed Res [Internet]. 2015;29(2):93–7. Available from: www.jbr-pub.org\nhttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4389120&tool=pmcentrez&rendertype=abstract.
Bradley D, Magkos F, Eagon JC, et al. Matched weight loss induced by sleeve gastrectomy or gastric bypass similarly improves metabolic function in obese subjects. Obesity (Silver Spring). 2014;22(9):2026–31.
SAGES. Guidelines for Clinical Application of Laparoscopic Bariatric Surgery SAGES Guidelines Committee. Soc Am Gastrointest Endosc Surg. 2008;1–31.
De Luca M, Angrisani L, Himpens J, Busetto L, Scopinaro N, Weiner R, et al. Indications for surgery for obesity and weight-related diseases: position statements from the International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO). Obes Surg [Internet]. Obesity Surgery; 2016;26(8):1659–1696. Available from: http://link.springer.com/10.1007/s11695-016-2271-4.
Oor JE, Roks DJ, Ünlü Ç, et al. Laparoscopic sleeve gastrectomy and gastroesophageal reflux disease: a systematic review and meta-analysis. Am J Surg [Internet]. 2016;211(1):250–67. Available from: http://www.sciencedirect.com/science/article/pii/S0002961015004225
Hill LD. An effective operation for hiatal hernia: an eight year appraisal. Ann Surg [Internet]. 1967;166(4):681–92. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1477443&tool=pmcentrez&rendertype=abstract
Low DE. Hill antireflux operation. Chest Surg Clin N Am. 1995;5(3):411–22.
Gagner M, Hernandez JD, Zundel N. Laparoscopic Sleeve gastrectomy: technique and outcomes. In: Nguyen N, Blackstone R, Morton J, Ponce J, Rosenthal RJ, editors. The ASMBS Textbook of Bariatric Surgery, vol. 1. New York: Springer Science + Business Media; 2015. p. 205–10.
SAGES Guidelines Committee. Guidelines for Clinical Application of Laparoscopic Bariatric Surgery. Soc Am Gastrointes Endosc Surg 2008 p. 1–31.
Levi J, Rayburn J, Martín A, et al. The State of Obesity: Better policies for a healthier America [Internet]. Trust Am Health. 2015; Available from: http://content.healthaffairs.org/cgi/doi/10.1377/hlthaff.2015.0434\nhttp://stateofobesity.org/states/ok/\nhttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3252192&tool=pmcentrez&rendertype=abstract\nhttp://content.healthaffairs.org/cgi/doi/10.137.
Obesity Society. What is Obesity? [Internet]. Obes Soc. 2016; Available from: http://www.obesity.org/resources/facts-about-obesity/what-is-obesity
Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients With Obesity – Executive Summary. Endocr Pract [Internet]. 2016;22(7):842–84. Available from: http://journals.aace.com/doi/10.4158/EP161365.GL
Friedenberg FK, Xanthopoulos M, Foster GD, et al. The association between gastroesophageal reflux disease and obesity. Am J Gastroenterol. 2008;103(8):2111–22.
Khan A. Impact of obesity treatment on gastroesophageal reflux disease. World J Gastroenterol [Internet]. 2016;22(4):1627–38. Available from: http://www.wjgnet.com/1007-9327/full/v22/i4/1627.htm
Jacobson BC. Body mass index and the efficacy of acid-mediating agents for GERD. Dig Dis Sci. 2008;53(9):2313–7.
Becker V, Grotz S, Schlag C, et al. Positive predictors for gastroesophageal reflux disease and the therapeutic response to proton-pump inhibitors. World J Gastroenterol. 2014;20(14):4017–24.
Dickman R, Boaz M, Aizic S, et al. Comparison of clinical characteristics of patients with gastroesophageal reflux disease who failed proton pump inhibitor therapy versus those who fully responded. J Neurogastroenterol Motil [Internet]. 2011;17(4):387–94. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3228979&tool=pmcentrez&rendertype=abstract
Bello B, Herbella FA, Allaix ME, et al. Impact of minimally invasive surgery on the treatment of benign esophageal disorders. World J Gastroenterol. 2012;18(46):6764–70.
Varela JE, Hinojosa MW, Nguyen NT. Laparoscopic fundoplication compared with laparoscopic gastric bypass in morbidly obese patients with gastroesophageal reflux disease. Surg Obes Relat Dis [Internet]. American Society for Metabolic and Bariatric Surgery; 2009;5(2):139–143. Available from: https://doi.org/10.1016/j.soard.2008.08.021
Nadaleto BF, Herbella F a M, Patti MG. Gastroesophageal reflux disease in the obese: Pathophysiology and treatment. Surgery [Internet] Elsevier Inc. 2016;159(2):475–86. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0039606015003633
Pagé MP, Kastenmeier A, Goldblatt M, et al. Medically refractory gastroesophageal reflux disease in the obese: what is the best surgical approach? Surg Endosc Other Interv Tech. 2014;28(5):1500–4.
Reporter O Bariatric (weight loss) surgery statistics (updated 2015). Bariatric (Weight Loss) Surgery Statistics (Updated 2015). 2016.
ASMBS. New Procedure Estimates for Bariatric Surgery [Internet]. New Procedure Estimates for Bariatric Surgery. 2014. Available from: http://connect.asmbs.org/may-2014-bariatric-surgery-growth.html
Daes J, Jimenez ME, Said N, et al. Improvement of gastroesophageal reflux symptoms after standardized laparoscopic sleeve gastrectomy. Obes Surg. 2014;24(4):536–40.
DuPree CE, Blair K, Steele SR, et al. Laparoscopic sleeve gastrectomy in patients with preexisting gastroesophageal reflux disease: a national analysis. JAMA Surg [Internet]. 2014;149(4):328–34. Available from: http://archsurg.jamanetwork.com/article.aspx?doi=10.1001/jamasurg.2013.4323
Melissas J, Leventi A, Klinaki I, et al. Alterations of global gastrointestinal motility after sleeve gastrectomy: a prospective study. Ann Surg [Internet]. 2013;258(6):976–82. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23160151
Shah S, Shah P, Todkar J, Gagner M, Sonar S, Solav S. Prospective controlled study of effect of laparoscopic sleeve gastrectomy on small bowel transit time and gastric emptying half-time in morbidly obese patients with type 2 diabetes mellitus. Surg Obes Relat Dis [Internet] Elsevier Inc.; 2010;6(2):152–157. Available from: https://doi.org/10.1016/j.soard.2009.11.019
Laffin M, Chau J, Gill RS, et al. Sleeve gastrectomy and gastroesophageal reflux disease. J Obes. 2013;2013:1–6.
Schubert ML. Functional anatomy and physiology of gastric secretion. Curr Opin Gastroenterol. 2015;31(6):479–85.
Santoro S. Technical aspects in sleeve gastrectomy. Obes Surg. 2007;17(11):1534–5.
Fujiwara Y, Nakagawa K, Kusunoki M, et al. Gastroesophageal reflux after distal gastrectomy: possible significance of the angle of His. Am J Gastroenterol. 1998;93(1):11–5.
Tomita R. Surgical techniques to prevent reflux esophagitis in proximal gastrectomy reconstructed by esophagogastrostomy with preservation of the lower esophageal sphincter, pyloric and celiac branches of the vagal nerve, and reconstruction of the new His angle for. Surg Today [Internet] Springer Japan; 2016;46(7):827–834. Available from: https://doi.org/10.1007/s00595-015-1269-1.
Himpens J, Dapri G, Cadière G. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: Results after 1 and 3 Years. Obes Surg. 2006;16(11):1450–6.
Yehoshua RT, Eidelman LA, Stein M, Fichman S, Mazor A, Chen J, Bernstine H, Singer P, Dickman R, Beglaibter N, Shikora SA, Rosenthal RJ, Rubin M Laparoscopic Sleeve gastrectomy - volume and pressure assessment. Obes Surg. 2008;18(9):1083–1088.
Baumann T, Grueneberger J, Pache G, et al. Three-dimensional stomach analysis with computed tomography after laparoscopic sleeve gastrectomy: Sleeve dilation and thoracic migration. Surg Endosc Other Interv Tech. 2011;25(7):2323–9.
Chiu S, Birch DW, Shi X, Sharma AM, Karmali S. Effect of sleeve gastrectomy on gastroesophageal reflux disease: a systematic review. Surg Obes Relat Dis [Internet] Elsevier Inc.; 2011;7(4):510–515. Available from: https://doi.org/10.1016/j.soard.2010.09.011
Benaiges D, Más-Lorenzo A, Goday A, et al. Laparoscopic sleeve gastrectomy: more than a restrictive bariatric surgery procedure? World J Gastroenterol. 2015;21(41):11804–14.
Gero D, Ribeiro-Parenti L, Arapis K, et al. Sleeve Gastrectomy combined with the simplified Hill repair in the treatment of morbid obesity and gastro-esophageal reflux disease: preliminary results in 14 patients. World J Surg. 2017;41(4):1035–9. https://doi.org/10.1007/s00268-016-3829-y.
Zhang C, Liu D, Li F, et al. Systematic review and meta-analysis of laparoscopic mesh versus suture repair of hiatus hernia: objective and subjective outcomes. Surg Endosc. 2017;31(12):4913–22. https://doi.org/10.1007/s00464-017-5586-x.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Statements
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key Points
• GE junction fixation as a antireflux mechanism
• No need of PPIs after postoperative management (PPIs free period mean 29.57 months)
• GERD symptoms control in all patients 3-year follow-up period
• Hill modified technique is a feasible option for GERD management in patients with LSG
Dr Ricardo Nassar is first author, principal researcher and chief and chairman.
Rights and permissions
About this article

Cite this article
Nassar, R., Giron, F., Garcia, A.M. et al. Hill Modified, a Novel Approach: Technique Description and Experience in Patients with Laparoscopic Sleeve Gastrectomy. OBES SURG 31, 3646–3652 (2021). https://doi.org/10.1007/s11695-021-05465-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-021-05465-z