
Abstract
Purpose
Laparoscopic sleeve gastrectomy (LSG) has become the most commonly performed bariatric procedure worldwide. Newer studies providing long-term follow-up show a high incidence of weight regain and a high incidence of reflux. The study’s objective was to present 5 to 15-year follow-up results regarding weight loss, comorbidities, reoperation rate, and a potential learning curve.
Methods
This is a retrospective analysis of prospectively collected data. Patients who underwent LSG between August 2004 and December 2014 were included.
Results
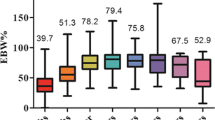
A total of 307 patients underwent LSG either as a primary bariatric procedure (n = 262) or as a redo operation after failed laparoscopic gastric banding (n = 45). Mean body mass index at the time of primary LSG was 46.4 ± 8.0 kg/m2, and mean age at operation was 43.7 ± 12.4 years with 68% females. Follow-up was 84% and 70% at 5 and 10 years, respectively. The mean percentage excess body mass index loss (%EBMIL) for primary LSG was 62.8 ± 23.1% after 5 years, 53.6 ± 24.6% after 10 years, and 51.2 ± 20.3% after 13 years. Comorbidities improved considerably (e.g., type 2 diabetes mellitus 61%), while the incidence of new-onset reflux was 32.4%. Reoperation after LSG was necessary in almost every fifth LSG-patient: 24 patients (7.8%) were reoperated due to insufficient weight loss, 12 patients (3.9%) due to reflux, 23 due to both (7.5%).
Conclusions
LSG provides a long-term %EBMIL from 51 to 54% beyond 10 years and a significant improvement of comorbidities. On the other hand, a high incidence of insufficient weight loss and de novo reflux was observed, leading to reoperation and conversion to a different anatomy in 19.2%.
Graphical abstract




Similar content being viewed by others


Change history
10 May 2021
A Correction to this paper has been published: https://doi.org/10.1007/s11695-021-05460-4
References
Arroyo-Johnson C, Mincey KD. Obesity epidemiology worldwide. Gastroenterol Clin N Am. 2016;45(4):571–9.
Schauer P, Bhatt DL, Kirwan JP, et al. Bariatric surgery versus intensive medical therapy for diabetes - 5-year outcomes. N Engl J Med. 2017;376(7):641–51.
Gagner M, Inabnet W, Pomp A. Laparoscopic sleeve gastrectomy with second stage biliopancreatic diversion and duodenal switch in the superobese. In: Inabnet W, DeMaria E, Ikramuddin S, editors. Laparoscopic bariatric surgery. Philadelphia: Lippincott Williams & Wilkins; 2005. p. 143–50.
Felberbauer FX, Langer F, Shakeri-Manesch S, et al. Laparoscopic sleeve gastrectomy as an isolated bariatric procedure: intermediate-term results from a large series in three Austrian centers. Obes Surg. 2008;18(7):814–8.
Angrisani L, Santonicola A, Iovino P, et al. Bariatric surgery and endoluminal procedures: IFSO worldwide survey 2014. Obes Surg. 2017;27(9):2279–89.
D’Hondt M, Vanneste S, Pottel H, et al. Laparoscopic sleeve gastrectomy as a single-stage procedure for the treatment of morbid obesity and the resulting quality of life, resolution of comorbidities, food tolerance, and 6-year weight loss. Surg Endosc. 2011;25(8):2498–504.
Peterli R, Wölnerhanssen BK, Peters T, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss in patients with morbid obesity. JAMA. 2018;319(3):255–65.
Felsenreich DM, Langer FB, Kefurt R, et al. Weight loss, weight regain, and conversions to Roux-en-Y gastric bypass: 10-year results of laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2016;12(9):1–8.
Felsenreich DM, Ladinig LM, Beckerhinn P, et al. Update: 10 years of sleeve gastrectomy—the first 103 patients. Obes Surg. 2018;28(11):3586–94.
Stenard F, Iannelli A. Laparoscopic sleeve gastrectomy and gastroesophageal reflux. World J Gastroenterol. WJG Press. 2015;21:10348–57.
Felsenreich DM, Kefurt R, Schermann M, et al. Reflux, sleeve dilation , and Barrett’s esophagus after laparoscopic sleeve gastrectomy: long-term follow-up. Multicenter Study. 2017:3092–101.
Genco A, Soricelli E, Casella G, et al. Gastroesophageal reflux disease and Barrett’s esophagus after laparoscopic sleeve gastrectomy: a possible, underestimated long-term complication. Surg Obes Relat Dis. 2017 Apr;13(4):568–74.
Wölnerhanssen B, Peterli R, Hurme S, et al. Laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy: 5-year outcomes of merged data from two randomized clinical trials (SLEEVEPASS and SM-BOSS). Br J Surg. 2021;108:49–57.
Zacharoulis D, Sioka E, Papamargaritis D, et al. Influence of the learning curve on safety and efficiency of laparoscopic sleeve gastrectomy. Obes Surg. 2012;22(3):411–5.
Buse JB, Caprio S, Cefalu WT, et al. How do we define cure of diabetes? Diabetes Care. 2009;32(11):2133–5.
Felsenreich DM, Langer FB, Prager G. Weight loss and resolution of comorbidities after sleeve gastrectomy: a review of long-term results. Scand J Surg. SAGE Publications Inc. 2019;108:3–9.
Arman GA, Himpens J, Dhaenens J, et al. Long-term (11+years) outcomes in weight, patient satisfaction, comorbidities, and gastroesophageal reflux treatment after laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2015;12(10):1778–86.
Gadiot RPM, Biter LU, van Mil S, et al. Long-term results of laparoscopic sleeve gastrectomy for morbid obesity: 5 to 8-year results. Obes Surg. 2016;27:1–5.
Sarela AI, Dexter SPL, O’Kane M, et al. Long-term follow-up after laparoscopic sleeve gastrectomy: 8-9-year results. Surg Obes Relat Dis. 2012;8(6):679–84.
Casella G, Soricelli E, Giannotti D, et al. Learning curve for laparoscopic sleeve gastrectomy: role of training in a high-volume bariatric center. Surg Endosc. 2016;30(9):3741–8.
Abdallah E, El Nakeeb A, Yousef T, et al. Impact of extent of antral resection on surgical outcomes of sleeve gastrectomy for morbid obesity (a prospective randomized study). Obes Surg. 2014;24(10):1587–94.
Eid GM, Brethauer S, Mattar SG, et al. Laparoscopic sleeve gastrectomy for super obese patients: forty-eight percent excess weight loss after 6 to 8 years with 93% follow-up. Ann Surg. 2012;256(2):262–5.
Schauer PR, Bhatt DL, Kirwan JP, et al. Bariatric surgery versus intensive medical therapy for diabetes - 3-year outcomes. N Engl J Med. 2014;370:1–12.
Chiu S, Birch DW, Shi X, et al. Effect of sleeve gastrectomy on gastroesophageal reflux disease: a systematic review. Surg Obes Relat Dis. 2011;7(4):510–5.
Daes J, Jimenez ME, Said N, et al. Improvement of gastroesophageal reflux symptoms after standardized laparoscopic sleeve gastrectomy. Obes Surg. 2014;24(4):536–40.
Boza C, Daroch D, Barros D, et al. Long-term outcomes of laparoscopic sleeve gastrectomy as a primary bariatric procedure. Surg Obes Relat Dis. 2014;10(6):1129–33.
Himpens J, Dobbeleir J, Peeters G. Long-term results of laparoscopic sleeve gastrectomy for obesity. Ann Surg. 2010;252(2):319–24.
Bevilacqua LA, Obeid NR, Yang J, et al. Incidence of GERD, esophagitis, Barrett’s esophagus, and esophageal adenocarcinoma after bariatric surgery. Surg Obes Relat Dis. 2020;16(11):1828–36.
Weiner RA, Theodoridou S, Weiner S. Failure of laparoscopic sleeve gastrectomy - further procedure? Obes Facts. 2011;4(Suppl 1):42–6.
Kraljević M, Süsstrunk J, Köstler T, et al. Short or long biliopancreatic limb bypass as a secondary procedure after failed laparoscopic sleeve gastrectomy. Obes Surg. 2020;31:170–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent does not apply as this is a database analysis.
Conflict of Interest
MK, VS, TP, MS, and BW declare no competing interests. RS reports grants from the University of Basel, grants from University Hospital Basel, Department of Surgery, grants from SFCS, grants from Gebauer Stiftung, and grants from Freiwillige Akademische Gesellschaft Basel, outside the submitted work. RP reports grants and personal fees from Ethicon Endo-Surgery, outside the submitted work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Keypoints
A retrospective study of 307 obese patients who underwent LSG as a primary or revisional procedure
LSG provides a mean %EBMIL from 51 to 54% beyond 10 years and a significant improvement of comorbidities.
The incidence of de novo reflux after LSG was 32.4% in the long-term.
Reoperation and conversion from LSG to different anatomy was necessary in almost every fifth patients.
Rights and permissions
About this article

Cite this article
Kraljević, M., Cordasco, V., Schneider, R. et al. Long-term Effects of Laparoscopic Sleeve Gastrectomy: What Are the Results Beyond 10 Years?. OBES SURG 31, 3427–3433 (2021). https://doi.org/10.1007/s11695-021-05437-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-021-05437-3