
Abstract
Introduction
One anastomosis gastric bypass (OAGB) was suggested as an option in the management of weight loss failure after sleeve gastrectomy (SG). In parallel, the length of the biliopancreatic limb (BPL) is currently debated.
Objectives
To evaluate morbidity and efficiency of the conversion of SG to OAGB using two lengths of BPL (150 cm versus 200 cm).
Methods
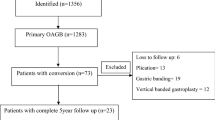
Retrospective analysis of a prospectively collected database on 72 patients operated on between 2007 and 2017: (200-cm BPL before 2014 versus 150-cm BPL since 2014).
Results
At revision, the mean body mass index (BMI) was 43.6 ± 7 kg/m2. Sixteen patients (20%) had type 2 diabetes (T2D) and 23 (29%) had obstructive sleep apnea (OSA). Early morbidity rate was 4.2% (n = 3). Mean BMI were 33.7 ± 6 and 34.8 ± 9 at 2 and 5 years, respectively. At 5 years, the rate of lost of follow-up was 34%. T2D and OSA improved in 80% (n = 12) and 70% (n = 16) of the patients, respectively. At revision, the mean BMI were 46 ± 8 kg/m2 and 41 ± 6 kg/m2 for patients with 200-cm BPL (n = 38) and 150-cm BPL (n = 34), respectively. Two years after conversion, the mean BMI were 34 ± 1 kg/m2 for 200-cm BPL and 32 ± 7 kg/m2 for 150-cm BPL. The rate of gastroesophageal reflux disease (GERD) and diarrhea was 13% and 5% in patients with 200-cm BPL versus 3% and 0% in patients with 150-cm BPL.
Conclusion
This study shows that the conversion of SG to OAGB is feasible and safe allowing significant weight loss and improvement in comorbidities. Weight loss seems comparable between the 150-cm and 200-cm BPL.

Similar content being viewed by others


References
Cottam S, Cottam D, Cottam A. Sleeve gastrectomy weight loss and the preoperative and postoperative predictors: a systematic review. Obes Surg. 2019:1–9. https://doi.org/10.1007/s11695-018-03666-7.
Felsenreich DM, Ladinig LM, Beckerhinn P, et al. Update: 10 years of sleeve gastrectomy-the first 103 patients. Obes Surg. 2018;28:3586–94.
Rebibo L, Fuks D, Verhaeghe P, et al. Repeat sleeve gastrectomy compared with primary sleeve gastrectomy: a single-center, matched case study. Obes Surg. 2012;22:1909–15.
Iannelli A, Schneck AS, Noel P, et al. Re-sleeve gastrectomy for failed laparoscopic sleeve gastrectomy: a feasibility study. Obes Surg. 2011;21:832–5.
Langer FB, Bohdjalian A, Shakeri-Leidenmühler S, et al. Conversion from sleeve gastrectomy to Roux-en-Y gastric bypass--indications and outcome. Obes Surg. 2010;20:835–40.
Poghosyan T, Lazzati A, Moszkowicz D, et al. Conversion of sleeve gastrectomy to Roux-en-Y gastric bypass: an audit of 34 patients. Surg Obes Relat Dis. 2016;12:1646–51.
Homan J, Betzel B, Aarts EO, et al. Secondary surgery after sleeve gastrectomy: Roux-en-Y gastric bypass or biliopancreatic diversion with duodenal switch. Surg Obes Relat Dis. 2015;11:771–7.
Dijkhorst PJ, Boerboom AB, Janssen IMC, et al. Failed sleeve gastrectomy: single anastomosis duodenoileal bypass or Roux-en-Y gastric bypass? A Multicenter Cohort Study. Obes Surg. 2018;28:3834–42.
Ceha CMM, van Wezenbeek MR, Versteegden DPA, et al. Matched short-term results of SADI versus GBP after sleeve gastrectomy. Obes Surg. 2018;28:3809–14.
Parmar CD, Mahawar KK. One anastomosis (mini) gastric bypass is now an established bariatric procedure: a systematic review of 12,807 patients. Obes Surg. 2018;28:2956–67.
De Luca M, Tie T, Ooi G, et al. Mini gastric bypass-one anastomosis gastric bypass (MGB-OAGB)-IFSO position statement. Obes Surg. 2018;28:1188–206.
Moszkowicz D, Rau C, Guenzi M, et al. Laparoscopic omega-loop gastric bypass for the conversion of failed sleeve gastrectomy: early experience. J Visc Surg. 2013;150:373–8.
Mahawar KK. Yet another mortality with a biliopancreatic limb of > 200 cm with one anastomosis gastric bypass. Obes Surg. 2018;28:3634–5.
Mahawar KK, Parmar C, Carr WRJ, et al. Impact of biliopancreatic limb length on severe protein-calorie malnutrition requiring revisional surgery after one anastomosis (mini) gastric bypass. J Minimal Access Surg. 2018;14:37–43.
Poghosyan T, Caille C, Moszkowicz D, et al. Roux-en-Y gastric bypass for the treatment of severe complications after omega-loop gastric bypass. Surg Obes Relat Dis. 2017;13:988–94.
Ahuja A, Tantia O, Goyal G, et al. MGB-OAGB: effect of biliopancreatic limb length on nutritional deficiency, weight loss, and comorbidity resolution. Obes Surg. 2018;28:3439–45.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Dapri G, Cadiere GB, Himpens J. Laparoscopic repeat sleeve gastrectomy versus duodenal switch after isolated sleeve gastrectomy for obesity. Surg Obes Relat Dis. 2011;7:38–43.
Greenstein AJ, Jacob BP. Placement of a laparoscopic adjustable gastric band after failed sleeve gastrectomy. Surg Obes Relat Dis. 2008;4:556–8.
Balibrea JM, Vilallonga R, Hidalgo M, et al. Mid-term results and responsiveness predictors after two-step single-anastomosis duodeno-ileal bypass with sleeve gastrectomy. Obes Surg. 2017;27:1302–8.
Chiappetta S, Stier C, Scheffel O, et al. Mini/one anastomosis gastric bypass versus Roux-en-Y gastric bypass as a second step procedure after sleeve gastrectomy-a retrospective cohort study. Obes Surg. 2018;29:819–27. https://doi.org/10.1007/s11695-018-03629-y.
Chevallier JM, Arman GA, Guenzi M, et al. One thousand single anastomosis (omega loop) gastric bypasses to treat morbid obesity in a 7-year period: outcomes show few complications and good efficacy. Obes Surg. 2015;25:951–8.
Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric-metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial. Lancet. 2015;386:964–73.
Schauer PR, Bhatt DL, Kirwan JP, et al. Bariatric surgery versus intensive medical therapy for diabetes - 5-year outcomes. N Engl J Med. 2017;376:641–51.
Guenzi M, Arman G, Rau C, et al. Remission of type 2 diabetes after omega loop gastric bypass for morbid obesity. Surg Endosc. 2015;29:2669–74.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval Statement
For this type of study, formal consent is not required.
Informed Consent Statement
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Poghosyan, T., Alameh, A., Bruzzi, M. et al. Conversion of Sleeve Gastrectomy to One Anastomosis Gastric Bypass for Weight Loss Failure. OBES SURG 29, 2436–2441 (2019). https://doi.org/10.1007/s11695-019-03864-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-03864-x