
Abstract
Background
Laparoscopic Roux-en-Y gastric bypass (LRYGB) is considered the golden standard for bariatric surgery. However, the potential risk for internal hernia after LRYGB remains a significant concern to both patients and surgeons. In addition, patients presenting with abdominal pain after LRYGB warrant careful attention to avoid missing or delaying the diagnosis of internal hernia. The aim of this study was to describe our technique to prevent internal hernia after LRYGB, intra-operative findings, and our management strategies for patients with internal hernia after LRYGB.
Methods
In this video, we review different technical tips and tricks to explore patients with suspected internal hernia after RYGB, how to reduce obstructed small bowel, and effectively close mesenteric defects to prevent internal hernia after LRYGB.
Results
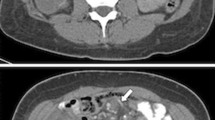
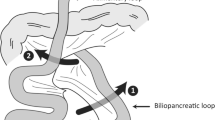
A high index of suspicion and evaluation of the CT scan of the patient by an experienced bariatric surgeon is essential to avoid missing cases of internal hernia after LRYGB. In addition, patients presenting with incarcerated small bowel due to an internal hernia are best managed by standing on the left side of the patient with the left arm tucked and starting at the ileocecal valve and running the small bowel backwards towards the ligament of Treitz. Furthermore, patients with bowel obstruction due to internal hernia may need to have a gastrostomy placed at the remnant of the stomach.
Conclusion
Recurrent abdominal pain is not uncommon after LRYGB. Systematic closure of mesenteric defects, the use of diagnostic laparoscopy, and high index of suspicion are all necessary to avoid delay in diagnosis.
Similar content being viewed by others

References
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724–37.
Steele KE, Prokopowicz GP, Magnuson T. Laparoscopic antecolic Roux-en-Y gastric bypass with closure of internal defects leads to fewer internal hernias than the retrocolic approach. Surg Endosc. 2008;22:2056–61.
Higa KD, Ho T, Boone KB. Internal hernias after laparoscopic Roux-en-Y gastric bypass: incidence, treatment and prevention. Obes Surg. 2003;13:350–4.
Rondelli F, Bugiantella W, Desio M, et al. Antecolic or retrocolic alimentary limb in laparoscopic roux-en-Y gastric bypass? A meta-analysis. Obes Surg. 2016;26(1):182–95.
Nimeri A, Mohamed A, El Hassan E, et al. Are results of bariatric surgery different in the Middle East? Early experience of an international bariatric surgery program and an ACS NSQIP outcomes comparison. J Am Coll Surg. 2013;216(6):1082–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest. Please refer to the ICMJE conflict of interest disclosure forms.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
This article does not contain any studies with human participants or animals performed by any of the authors.
For this type of study, formal consent is not required.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
(MP4 195233 kb)
Rights and permissions
About this article

Cite this article
Nimeri, A.A., Maasher, A., Al Shaban, T. et al. Internal Hernia Following Laparoscopic Roux-en-Y Gastric Bypass: Prevention and Tips for Intra-operative Management. OBES SURG 26, 2255–2256 (2016). https://doi.org/10.1007/s11695-016-2267-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-016-2267-0