
Abstract
Background
No bariatric procedure is perfect, and a plethora of such procedures itself is a proof for the same. Laparoscopic adjustable gastric banding has a high safety profile, but also a high rate of re-operation has been reported (Schouten, Wiryasaputra, van Dielen et al. Obes Surg 20(12):1617–26, 2010). Laparoscopic sleeve gastrectomy (LSG) is becoming popular, but has its own set of complications and is irreversible. We introduced laparoscopic adjustable gastric banded plication (LAGBP) in 2009 (Huang, Lo, Shabbir et al. Surg Obes Relat Dis 8(1):41–5, 2012) In a case matched comparative study with LSG, LAGBP showed similar results at 2 years in terms of weight loss, comorbidity resolution, and complications. (Huang, Chhabra, Goel et al. Obes Surg 23(8):1319–23, 2013). Several authors have reported variations in their technique, bougie size, and suture material used to perform plication. (Ramos, Galvao Neto, Galvao et al. Obes Surg 20(7):913–8, 2010, (Mui, Lee, Lam et al. Obes Surg 23(2): 179–83, 2013, Brethauer, Harris, Kroh et al. Surg Obes Relat Dis 7(1):15–22, 2011) Our initial technique of placing the band first and then plicating the stomach resulted in higher incidence of gastric fundus herniation compared to that reported in a systematic review (Abdelbaki, Huang, Ramos et al. Obes Surg 22(10):1633–9, 2012). After the first 65 cases, we reversed the order by performing the gastric plication first which ensures proper plication of the fundus and a more uniformly placed plication line. This technique has become our standard, and the same is described in this video in a stepwise fashion.
Materials and Methods
We performed LAGBP in 202 cases over the last 4 years and recorded the findings. Our standardized technique is shown in this video. The T-suspension technique was used for liver retraction. (Zachariah, Tai, Chang et al. J Laparoendosc Adv Surg Tech A 23(4):311–5, 2013) Gastric plication formula is shown in Fig. 1.

Gastric plication formula
Results
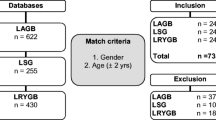
Two hundred two (69 male, 133 female) patients in over the last 4 years underwent LAGBP. Follow-up at 1 year was 168 patients, and 56 patients reached 4-year follow-up. Age was 16–60 years (mean = 31.1). Mean BMI was 39.5 ± 3.18 and body weight 110 kg ± 19.4. Mean operative time was 104 min ± 39 and length of hospital stay after surgery 2.1 ± 2.3 days. No mortality was recorded. Excess weight loss at 1 year was 57.84 % and at four years 68 %.
Conclusion
LAGBP has been proven to be an effective bariatric procedure in the midterm results. Standardization with plication first and then placement of the band could be important to achieve best outcomes.
Similar content being viewed by others


References
Schouten R, Wiryasaputra DC, van Dielen FM, et al. Long-term results of bariatric restrictive procedures: a prospective study. Obes Surg. 2010;20(12):1617–26.
Huang CK, Lo CH, Shabbir A, et al. Novel bariatric technology: laparoscopic adjustable gastric banded plication: technique and preliminary results. Surg Obes Relat Dis. 2012;8(1):41–5.
Huang CK, Chhabra N, Goel R, et al. Laparoscopic adjustable gastric banded plication: a case-matched comparative study with laparoscopic sleeve gastrectomy. Obes Surg. 2013;23(8):1319–23.
Ramos A, Galvao Neto M, Galvao M, et al. Laparoscopic greater curvature plication: initial results of an alternative restrictive bariatric procedure. Obes Surg. 2010;20(7):913–8.
Mui WL, Lee DW, Lam KK, et al. Laparoscopic greater curve plication in Asia: initial experience. Obes Surg. 2013;23(2):179–83.
Brethauer SA, Harris JL, Kroh M, et al. Laparoscopic gastric plication for treatment of severe obesity. Surg Obes Relat Dis. 2011;7(1):15–22.
Abdelbaki TN, Huang CK, Ramos A, et al. Gastric plication for morbid obesity: a systematic review. Obes Surg. 2012;22(10):1633–9.
Zachariah SK, Tai CM, Chang PC, et al. The “T-Suspension Tape” for liver and gallbladder retraction in bariatric surgery: feasibility, technique, and initial experience. J Laparoendosc Adv Surg Tech A. 2013;23(4):311–5.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
No identifying information is available in the article:
"Additional informed consent was obtained from all individual participants for whom identifying information is included in this article.”—does not apply.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
This article does not contain any studies on animals performed by any of the authors.
This is a retrospective studies, for this type of study formal consent is not required.
Disclosures
Jasmeet Singh Ahluwalia has no conflict of interest.
Hsin-Chih Kuo has no conflict of interest.
Po-Chih Chang has no conflict of interest.
Po-Lin Sun has no conflict of interest.
Kuo-Chuan Hung has no conflict of interest.
Chih-Kun Huang has no conflict of interest.
Funding
There is no external source of funding.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
(MP4 343789 kb)
Rights and permissions
About this article

Cite this article
Ahluwalia, J.S., Kuo, HC., Chang, PC. et al. Standardized Technique of Laparoscopic Adjustable Gastric Banded Plication with 4-Year Results. OBES SURG 25, 1756–1757 (2015). https://doi.org/10.1007/s11695-015-1756-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-015-1756-x