
Abstract
Summary
This study examines the relationship between socioeconomic status, comorbidities, and clinical outcomes of hip fracture patients. Lower socioeconomic status is not only associated with poorer comorbidities but is also independently impacting surgical access and outcomes. This can be considered a “double setback” in the management of hip fractures.
Purpose
The effect of socioeconomic status on hip fracture outcomes remains controversial. We examine the relationship between SES and patient comorbidity, care access, and clinical outcomes of surgically managed hip fracture patients.
Methods
Using healthcare payor status as a surrogate for SES, patients operated for fragility hip fractures between 2013 and 2016 were dichotomised based on payor status, namely private healthcare (PRIV) versus subsidised healthcare (SUB). PRIV patients were compared with SUB patients in terms of demographic data, ASA scores, co-morbidity burden (Charlson comorbidity index, CCI), time to surgery, length of acute hospitalisation, and 90-day readmission rates.
Results
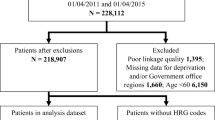
A total of 145 patients in group PRIV and 1146 patients in group SUB were included. SUB patients had a higher mean Charlson Co-morbidity Index (CCI) (p = 0.01), a longer length of hospitalisation (p = 0.001), an increased delay in surgery (p = 0.005), and higher 90-day readmission rates (p = 0.013). Lower SES (p = 0.01), older age (p = 0.01), higher CCI (p < 0.01), and a higher American Society of Anaesthesiologists score (ASA) (p = 0.03) were predictive of time to surgery. Lower SES (p = 0.02) and higher CCI (p < 0.001) were predictive of the length of hospitalisation. Lower SES (p = 0.04) and higher CCI (p < 0.001) were predictive of 90-day readmission rates.
Conclusions
Low SES is associated with higher CCI in surgically treated hip fracture patients. However, it is independently associated with slower access to surgery, a longer hospital stay, and higher readmission rates. Hence, lower SES, with its associated higher CCI and independent impact on surgical access and outcomes, can be considered a “double setback” in the management of fragility hip fractures.
Similar content being viewed by others


References
Braveman P, Gottlieb L (2014) “The social determinants of health: it’s time to consider the causes of the causes”
Denvir MA et al. (2006) “Influence of socioeconomic status on clinical outcomes and quality of life after percutaneous coronary intervention,” J Epidemiol Community Health (1978) 60(12):1085–1088. https://doi.org/10.1136/jech.2005.044255
Marshall IJ, Wang Y, Crichton S, McKevitt C, Rudd AG, Wolfe CDA (2015) “The effects of socioeconomic status on stroke risk and outcomes,” Lancet Neurol 14(12):1206–1218. Lancet Publishing Group, https://doi.org/10.1016/S1474-4422(15)00200-8
Gupta S, Wilejto M, Pole JD, Guttmann A, Sung L (2014) “Low socioeconomic status is associated with worse survival in children with cancer: a systematic review,” PLoS ONE 9:2. Public Library of Science https://doi.org/10.1371/journal.pone.0089482
Barrack RL et al (2014) Impact of socioeconomic factors on outcome of total knee arthroplasty knee. Clin Orthop Relat Res 472(1):86–97. https://doi.org/10.1007/s11999-013-3002-y
Maharlouei N, Jafarzadeh F, Lankarani KB (2019) Factors affecting recovery during the first 6 months after hip fracture, using the decision tree model,” Arch Osteoporos 14:1 https://doi.org/10.1007/s11657-019-0611-4
Hsu IL, et al. (2018) “Socioeconomic inequality in one-year mortality of elderly people with hip fracture in Taiwan,” Int J Environ Res Public Health 15:2 https://doi.org/10.3390/ijerph15020352
Auais M, Al-Zoubi F, Matheson A, Brown K, Magaziner J, French SD (2019) “Understanding the role of social factors in recovery after hip fractures: a structured scoping review,” Health Soc Care Commun 27(6):1375–1387. Blackwell Publishing Ltd https://doi.org/10.1111/hsc.12830
Reyes C et al (2015) Socioeconomic status and its association with the risk of developing hip fractures: a region-wide ecological study. Bone 73:127–131. https://doi.org/10.1016/j.bone.2014.12.019
Guilley E, Herrmann F, Rapin CH, Hoffmeyer P, Rizzoli R, Chevalley T (2011) Socioeconomic and living conditions are determinants of hip fracture incidence and age occurrence among community-dwelling elderly. Osteoporos Int 22(2):647–653. https://doi.org/10.1007/s00198-010-1287-1
Bhimjiyani A, Neuburger J, Jones T, Ben-Shlomo Y, Gregson CL (2018) The effect of social deprivation on hip fracture incidence in England has not changed over 14 years: an analysis of the English Hospital Episodes Statistics (2001–2015). Osteoporos Int 29(1):115–124. https://doi.org/10.1007/s00198-017-4238-2
Petit MP, Bryère J, Maravic M, Pallaro F, Marcelli C (2017) Hip fracture incidence and social deprivation: results from a French ecological study. Osteoporos Int 28(7):2045–2051. https://doi.org/10.1007/s00198-017-3998-z
Quah C, Boulton C, Moran C (2011) The influence of socioeconomic status on the incidence, outcome and mortality of fractures of the hip. J Bone Joint Surg [Br] 93(6):93–801. https://doi.org/10.1302/0301-620X.93B6
Farahmand BY, Persson P.-G, Èlsson KM, Baron JA, Parker MG, Ljunghall S. “Socioeconomic status, marital status and hip fracture risk: a population-based case±control study.”
Zingmond DS, Soohoo NF, Silverman SL (2006) The role of socioeconomic status on hip fracture. Osteoporos Int 17(10):1562–1568. https://doi.org/10.1007/s00198-006-0161-7
Valentin G, et al. (2020) “Socio-economic inequalities in fragility fracture outcomes: a systematic review and meta-analysis of prognostic observational studies,” Osteoporosis Int 31(1):31–42. Springer https://doi.org/10.1007/s00198-019-05143-y
Roberts SE, Goldacre MJ. “Papers time trends and demography of mortality after fractured neck of femur in an English population, 1968–98: database study.”
Tosteson ANA, Gottlieb DJ, Radley DC, Fisher ES, Melton LJ (2007) Excess mortality following hip fracture: the role of underlying health status. Osteoporos Int 18(11):1463–1472. https://doi.org/10.1007/s00198-007-0429-6
Bentler SE et al (2009) The aftermath of hip fracture: discharge placement, functional status change, and mortality. Am J Epidemiol 170(10):1290–1299. https://doi.org/10.1093/aje/kwp266
Kristensen PK, Thillemann TM, Pedersen AB, Søballe K, Johnsen SP (2017) Socioeconomic inequality in clinical outcome among hip fracture patients: a nationwide cohort study. Osteoporos Int 28(4):1233–1243. https://doi.org/10.1007/s00198-016-3853-7
Barone AP et al. (2009) “Effects of socioeconomic position on 30-day mortality and wait for surgery after hip fracture,” Int J Qual Health Care 21:6 https://doi.org/10.1093/intqhc/mzp046
Petrelli A, de Luca G, Landriscina T, Costa G, Gnavi R (2017) Effect of socioeconomic status on surgery waiting times and mortality after hip fractures in Italy. J Healthc Qual 40(4):209–216. https://doi.org/10.1097/JHQ.0000000000000091
Tomioka S, Fujino Y, Nakaya T, Ohtani M, Kubo T, Matsuda S (2018) Equality of treatment for hip fracture irrespective of regional differences in socioeconomic status: analysis of nationwide hospital claims data in Japan. Tohoku J Exp Med 247(3):161–171. https://doi.org/10.1620/tjem.247.161
Ministry of Health Singapore, “Community health assist scheme - eligibility and application.” https://www.chas.sg/eligibility-and-application
Darin-Mattsson A, Fors S, Kåreholt I (2017) Different indicators of socioeconomic status and their relative importance as determinants of health in old age. Int J Equity Health 16(1):173. https://doi.org/10.1186/s12939-017-0670-3
Sheehy-Skeffington J (2020) The effects of low socioeconomic status on decision-making processes. Curr Opin Psychol 33:183–188. https://doi.org/10.1016/j.copsyc.2019.07.043
Salma Khalik, “All you need to know about the standard B1 class Integrated Shield Plan,” The Straits Times, Singapore, Mar. 15, 2016. [Online]. Available: https://www.straitstimes.com/singapore/health/all-you-need-to-know-about-the-standard-b1-class-integrated-shield-plan
Ministry of Health Singapore, “MOH - subsidies for services and drugs at public healthcare settings.” https://www.moh.gov.sg/cost-financing/healthcare-schemes-subsidies/subsidies-for-services-and-drugs-at-public-healthcare-settings
Deyo RA, Cherkin DC, Ciol MA (1992) Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 45(6):613–619. https://doi.org/10.1016/0895-4356(92)90133-8
Neuhaus V, King J, Hageman MG, Ring DC (2013) Charlson comorbidity indices and in-hospital deaths in patients with hip fractures trauma. Clin Orthop Relat Res 471(5):1712–1719. https://doi.org/10.1007/s11999-012-2705-9
Dy CJ, Lane JM, Pan TJ, Parks ML, Lyman S (2016) Racial and socioeconomic disparities in hip fracture care. Journal of Bone and Joint Surgery - American 98(10):858–865. https://doi.org/10.2106/JBJS.15.00676
Freburger JK, Holmes GM, Ku LJE (2012) Postacute rehabilitation care for hip fracture: who gets the most care? J Am Geriatr Soc 60(10):1929–1935. https://doi.org/10.1111/j.1532-5415.2012.04149.x
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed consent
Formal consent was not required due to the retrospective nature of this study.
Conflict of interest
None.
Statement of human and animal rights
This article does not contain any studies with human participants of animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wong, K.C., Tan, E.SE., Liow, M.H.L. et al. Lower socioeconomic status is associated with increased co-morbidity burden and independently associated with time to surgery, length of hospitalisation, and readmission rates of hip fracture patients. Arch Osteoporos 17, 139 (2022). https://doi.org/10.1007/s11657-022-01182-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-022-01182-x