
Abstract
Background
Estimates suggest 30% of health care expenditures are wasteful. This has led to increased educational interventions in graduate medical education (GME) training aimed to prepare residents for high value, cost-conscious practice. International health electives (IHE) are widely available in GME training and may be provide trainees a unique perspective on principles related to high value, cost-conscious care (HVCCC).
Objective
The purpose of this study was to explore how trainee reflections on IHE experiences offer insight into HVCCC.
Design
The authors conducted an applied thematic analysis of narrative reflective reports of GME trainees’ IHE experiences to characterize their perceptions of HVCCC.
Participants
The Mayo International Health Program (MIHP) supports residents and fellows from all specialties across all Mayo Clinic sites. We included 546 MIHP participants from 2001 to 2020.
Approach
The authors collected post-elective narrative reports from all MIHP participants. Reflections were coded and themes were organized into model for transformative learning during IHEs, focusing on HVCCC.
Key Results
GME trainees across 24 different medical specialties participated in IHEs in 73 different countries. Three components of transformative learning were identified: disorienting dilemma, critical reflection, and commitment to behavior change. Within the component of critical reflection, three topics related to HVCCC were identified: cost transparency, resource stewardship, and reduced fear of litigation. Transformation was demonstrated through reflection on future behavioral change, including cost-aware practice, stepwise approach to health care, and greater reliance on clinical skills.
Conclusions
IHEs provide rich experiences for transformative learning and reflection on HVCCC. These experiences may help shape trainees’ ideology of and commitment to HVCCC practices.
Similar content being viewed by others


Introduction
The United States has the highest level of health care spending in the world, and costs are continuing to rise at an unsustainable level.1,2,3 Estimates suggest that 30% (more than $700 billion per year) of health care costs are “wasted,” defined as adding cost without benefit to the patient.4,5 This has led prominent professional medical societies, such as the American College of Physicians (ACP), to create high-value, cost-conscious care (HVCCC) initiatives within graduate medical education (GME) to promote health care that evaluates the benefits, harms, and costs of interventions and adds value to the patient.1,6,7
The GME environment is a powerful influencer of practice patterns related to healthcare cost and quality, the two main aspects of value. Training program affiliation has been identified as a main contributor to practice intensity (i.e., resource utilization and costliness).8,9 Residents who trained at residency programs with low-intensity practices were more likely to choose appropriately conservative management on the American Board of Internal Medicine certifying examination.9 Studies have also shown that the GME environment influences prescribing patterns,10 quality of patient care,11 and health outcomes.12 Further, physicians trained in high-spending environments go on to practice more costly medicine than those who train in low-spending environments, with differences persisting over a decade post-training.13,14 These studies demonstrate a clear relationship between the GME training environment and subsequent quality and cost of care.
Given the influence of the GME environment, there have been increasing calls to engage residents during their training to reduce costs. The Accreditation Council on Graduate Medical Education (ACGME) has refined the core competency of systems-based practice to address HVCCC; the common program requirements state that residents must demonstrate competence in “incorporating considerations of value, cost awareness, delivery and payment, and risk-benefit analysis in patient and/or population-based care as appropriate” and “understanding health care finances and its impact on individual patients’ health decisions.”15 The Alliance for Academic Internal Medicine (AAIM) and ACP collaborated to develop an online module-based curriculum to support efforts to train physicians to provide HVCCC.16 Further, many accreditation and certification organizations require quality improvement activities to encourage ongoing behavioral and cultural changes among faculty members and institutions.17,18 Despite these efforts, moving the needle towards HVCCC has proven difficult.
International health electives (IHEs) are widely available in GME and may provide trainees exposure to HVCCC principles.19,20,21 IHEs provide varied educational benefits, including improvement in medical knowledge, physical examination skills, resourcefulness and cost-effectiveness, and enhanced learning across the ACGME core competencies.22,23,24,25 While previous studies suggest that IHEs may provide an environment that influences how trainees think about HVCCC, we are not aware of any studies that specifically examine the relationship between IHEs and HVCCC.
The purpose of this study was to explore how trainee reflections on IHE experiences offer insights into HVCCC. Examining IHEs through the lens of HVCCC may provide a greater understanding of how IHE experiences shape trainee HVCCC perceptions and practice patterns.
Method
We conducted an applied thematic analysis26 of reflective reports of GME trainees’ IHE experiences to characterize their perceptions of HVCCC.
This study was deemed exempt by the Mayo Clinic Institutional Review Board.
Context and participants
The Mayo International Health Program (MIHP) was established in 2001 to fund and support residents’ and fellows’ participation in IHEs in low- or low-middle income countries. Residents and fellows across all Mayo Clinic training sites (Minnesota/Wisconsin, Arizona, and Florida) were eligible to participate in one week to one month IHEs at one of 14 designated partnership sites or at an independent site of their choosing that met the program requirements.
We included all narrative reflective reports from MIHP participants between the years 2001 and 2020, excluding three reports containing incomplete data (n = 546).
Data collection
Each MIHP participant was required to complete a post-elective report. This report included demographic information, a case log, a “minimum one-page personal reflection of your experience including “a statement indicating how this experience has impacted you either personally and/or professionally” and a reflection on “areas of our healthcare system (local or national) which could be improved based on your reflections of your MIHP experience.” The narrative report was the source of data for this study.
Data processing and analysis
The narrative reports were uploaded to NVivo 10 (QSR International, Australia), a computer software program to support the analysis of qualitative data. Three members of the research team (H.C.N., M.U.B., A.P.S.) read all reports completed between 2001 and 2014 (n=377). Through open coding, analytic memos, and group discussion we created a codebook a priori from the ACGME core competencies. Then within the core competency of systems-based practice a unique HVCCC codes were identified. This codebook was applied to 377 reports; three team members (H.C.N., M.U.B., A.P.S.) coded the first three years (2001-2003) of reports in duplicate until appropriate agreement was reached, and the remaining reports were coded individually. Codes were then organized into axial codes representing the components of the transformative learning process identified in prior work27, including “disorienting dilemma,” “critical reflection,” and “commitment to behavior change.”
To add to our sample size, two authors (C.L.M., A.P.S.) subsequently coded all reports completed between 2015 and 2020 (n=169) in duplicate. Through group discussion, we agreed that we achieved thematic continuity (i.e., persistence of afore identified themes in subsequent years) and thematic saturation, with no new thematic concepts identified in the data set, and a comprehensive understanding of the identified concepts was achieved.
Transformative learning
Transformative learning is defined as “the process of effecting change in a frame of reference.” The transformative process begins with a “disorienting dilemma,” proceeds through critical reflection, and leads to an alternative perspective. We utilized transformative learning as a lens to organize our data during analysis.
Results
From 2001 to 2020, 546 trainees completed post-elective reports following participation in an IHE through the MIHP. Trainees came from 24 specialties across the three Mayo Clinic and Mayo Clinic Health System training sites and participated in IHEs in 73 different countries (Table 1).
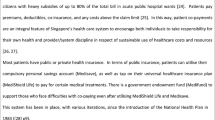
Through analysis of post-elective reports, we identified 3 components of transformative learning related to HVCCC reflection: disorienting dilemma, critical reflection, and commitment to behavioral change (Figure 1). Below, we outline and expand upon each step in the process of reflection on HVCCC that most trainees experienced during IHEs.

The process of transformative learning in international health electives, from a study of residents’ high-value, cost-conscious care reflections during international health electives, Mayo Clinic, 2001-2019. This figure demonstrates high-value, cost-conscious care transformative learning identified in resident reflective reports after participation in an international health elective, with an example from a single report (2009/Thailand/Cardiology).
Disorienting dilemma
IHEs afford trainee the opportunity to learn about and practice medicine in low-resource settings. Trainees experienced a stark contrast in the provision of healthcare between host and home institutions. This created a disorienting dilemma that served as a catalyst for reflection on HVCCC principles.
Most trainees reflected on the stark contrast between their host and home settings. Widespread was their reflection on poverty: “We rode through some of the poorest villages I have ever seen. The contrast with the affluence seen here in America was stark” (2002/Mexico/ Otorhinolaryngology). Another trainee remarked, “the depth of poverty is striking” (2003/Ecuador/Neurology). Poverty was linked to access to health care resources: “lack of financial resources directly affected the individual’s ability to access resources and care” (2007/Philippines/Internal Medicine). Lack of resources contrasted with residents’ home settings: “The substantial lack of access to medical resources amongst the patients we encountered strikingly contrasts with the situation in the United States. I find it surreal to conceptualize that by mere virtue of being born a few miles on one side or the other of a man-made imaginary line, an individual’s socioeconomic fate can be so radically affected” (2002/Mexico/Internal Medicine). In addition to poverty and resource limitations, trainees also contrasted home and host site infrastructure: “the stark differences between equipment and facilities here and in the United States is incomprehensible” (2012/Malawi/Preventative Medicine). Another trainee stated, “the lack healthcare infrastructure compared to the United States challenged our provision and coordination of care” (2017/Uganda/Family Medicine).
The stark contrast between host and home settings created a disorienting dilemma that provided the impetus for critical reflection on HVCCC.
Critical reflection
We identified three categories of themes within trainees reflections that related to HVCCC: cost transparency, resource stewardship, and reduced fear of litigation.
Cost transparency
Cost transparency was contrasted between host and home healthcare systems. Trainees often reflected on increased cost transparency at host institutions: “One aspect of health economics I appreciated was cost transparency. For all testing, the cost of testing was clearly stated to the patients and they would pay before testing was ordered. In the U.S. we order a multitude of tests and neither the patient nor provider knows exactly how much it costs. It takes the conversation of health care costs away and contributes to the rising costs of healthcare in the U.S.” (2020/Kenya/Neurology). Trainees reflected on how greater cost-transparency at home institutions may provide benefit in cost-containment: “Additional cost transparency could be beneficial in controlling medical costs in the U.S. With improved transparency [patients and physicians] may better understand of the costs of medical care and thereby make shared decisions taking cost into consideration” (2009/Nepal/Internal Medicine).
Resource stewardship
Working in resource-limited settings challenged residents to reflect on issues of resource stewardship. Trainees reflected on the contrast in resource use between host and home intuitions: “All the supplies were used to the fullest extent. No supplies were discarded but repurposed until no longer functional. This contrasts the wasteful consumption in the United States” (2014/Ghana/Ophthalmology). Trainees further reflected on appropriate allocation of resources: “Many patients had limited funds and the hospital also had limited resources. Therefore, more attention was paid to whether a particular diagnostic test or therapeutic intervention would provide benefit to the patient. Careful stewardship of resources was central to the care provided. [The United States] healthcare systems could benefit from more stringent and appropriate allocation of healthcare resources” (2013/Cameroon/Pathology).
Reduced fear of litigation
Many trainees reflected on reduced fear of litigation at host institutions versus home institutions: “In the United States we have high rates of litigation, but here litigation is rare. It was refreshing to practice medicine without this fear of litigation – focusing only on what’s best for the patient” (2011/Ethiopia/Family Medicine). Reduced fear of litigation translated to less “defensive medicine” practices, as one trainee reflected: “I found that when the bureaucracy of medicine (e.g., litigation) was removed, the doctor-patient relationship flourished. Very little “defensive medicine” was exercised, which allowed for more efficient utilization of resources. This represented the ideal setting to deliver high quality care” (2009/China/Otorhinolaryngology).
Commitment to behavioral change
We identified three major themes of behavior change related to HVCCC: cost-aware practice, stepwise approach to health care, and greater reliance on clinical skills. Trainees utilized these practices during IHE and expressed a commitment to carrying forward these high-value practices after participation in IHE experiences.
Cost-aware practice
Trainees acknowledged changes in perspective regarding cost-aware medical practice: “This experience opened my eyes to cost and challenged my previously known standards of practice” (2017/Ghana/Pediatrics). Limited resources created opportunity for learning how to “provide excellent medical care with simplicity, flexibility and creativity,” becoming more “cost-efficient” in the process (2010/Honduras/General Surgery). Trainees linked cost-transparency to cost-aware medical practice: “Because costs are clearly stated at the time of care, I became very aware of the cost of care and it heavily influenced my clinical decisions when devising a plan of care” (2017/Peru/General Surgery). Trainees expressed a commitment to change the way they approach their future practice: “As I return to the U.S., I plan to remain mindful of cost of medical care and determine if ordering tests will ultimately change management” (2019/Tanzania/Pediatrics).
Stepwise approach
Trainees described how consideration of cost and resource limitations influenced clinical decisions: “We were forced to take into account financial and logistical constraints when coming up with a diagnosis and plan for testing and/or therapy” (2009/Colombia/Psychiatry). This challenged trainees to approach clinical decisions in an organized, stepwise fashion. As one trainee reflected: “In Ecuador the cost to the family and the hospital for repeated testing, or even diagnostic testing at times, was not feasible. Therefore, physicians tended to treat empirically and follow day-to-day clinical status before testing or re-testing. This was an important lesson to take back to my own practice” (2014/Ecuador/Neurology).
Reliance on clinical skills
Trainees reflected on the impact of IHEs on their comfort with clinical and diagnostic skills, commonly siting improvement of and greater reliance on the physical exam and reduced dependence on expensive diagnostics. As one trainee reflected: “My experience in Nairobi taught me to rely more heavily on my improved history taking and physical exam and less on laboratory testing and other diagnostics” (2001/Kenya/Internal Medicine). Trainees commented on the durable impact of these experiences: “One of the most important skills I have learned is to rely heavily on my physical exam skills. This rotation opened my eyes to being conscientious about cost of medical care and determining if ordering tests will ultimately change management. I will carry this with me throughout my career” (2019/Tanzania/Family Medicine).
Discussion
Previous research demonstrated the transformative nature of IHE experiences27, with several studies pointing towards influence on learners’ cost-effectiveness.9,13,28 In this study, we characterized how IHE experiences may contribute to high-value clinical training. We identified three components of transformative learning – disorienting dilemma, critical reflection, and commitment to behavioral change – and their relation to trainees’ reflections on HVCCC after participation in IHEs. The contrast in resource availability between host and home institutions served as a catalyst for HVCCC reflection. Critical reflection centered on three main themes: cost transparency, resource stewardship, and reduced fear of litigation. Operating within and reflecting on practicing in a resource-limited setting led trainees to express a commitment to approach their future practices with an eye toward cost-conscious care. Our findings both support and augment the previous literature that suggest IHEs impact how residents view HVCCC.
Trainees reported engaging in high-value behaviors, including those specifically identified as important within the ACP-AAIM High Value Care Curriculum. The high-value behaviors most frequently described by trainees were regarding heightened cost-aware practices (e.g., questioning how a test will change management or considering resource availability) or interactions with patients (e.g., mindfulness of financial hardships). Trainee reflections suggested that cost-consideration influenced practices, including decreased unnecessary testing, increased reliance on clinical skills, risk-benefit analysis, and consideration of cost impact on the patient and system. These results are encouraging and demonstrate how IHEs can integrate the ACP-AAIM High Value Care principles with experiential learning in the clinical setting.
This data also enables us to further understand the role of IHEs in competency-based education. Researchers have found that IHEs enhance learning across the ACGME core competencies .22,29 Specifically, the University of Minnesota identified three themes of reflection related to systems-based practice: awareness of the larger context of health care, cost awareness, and coordinating care within larger system.29 We identified a link between transformative learning and HVCCC; transformative learning, through presenting disorienting dilemmas, can facilitate learner reflection on HVCCC concepts. More broadly, capitalizing on disorienting dilemmas and facilitating critical reflection could be applied to competency-based teaching within and outside of IHEs to create transformation in systems and personal practice related to HVCCC.
Our findings also highlight opportunities for improvement within U.S. healthcare systems. Trainees regularly reflected on heighted cost-transparency at host institutions, and positively correlated cost-transparency with cost-conscious practice. This supports existing literature that points to price transparency improving HVCCC practice.30 For example, cost displayed within the electronic medical record ordering systems led to reduced health care expenditures.30 Working towards continued improvement of cost-transparency within U.S. hospital systems may mark a first step along the path towards equipping trainees with the information needed to make HVCCC recommendations.
Key components of GME training include clinical experiences, faculty models, and formal curricula, and each of these components can imprint both desirable and undesirable practices related to cost and quality.9,10,11,13,28 While IHEs provide exposure to other models of health care delivery that can stimulate reflection on HVCCC, this is clearly not feasible for most trainees. There are other opportunities for transformative learning within medical curricula. For example, a social pediatrics elective foster reflection on social determinants of health, including the effect of poverty on health outcomes.31 Exposing trainees to community-based settings caring for vulnerable populations provided trainees with greater awareness, encouraged the development of critical perspectives of the healthcare system, and a renewed vision of medical practice.32 In general, providing exposure to diverse practices, encouraging questioning one’s beliefs and the values of the system, and facilitating reflection provide a learning environment conducive to transformative learning.33 While IHEs provide an opportunity for transformation in HVCCC practices, educators can be intentional to create other spaces for critical reflection on HVCCC.
Limitations
There are limitations of this study. First, the data were originally collected for rotation evaluation and were not designed to specifically evaluate trainee HVCCC reflections. This limits our ability to access participants’ predilection toward HVCCC prior to their IHE experience and, in turn, limits our ability to analyze the extent to which IHEs influence trainees’ HVCCC perceptions. Second, as reflections were unguided and experiences were highly variable, it is possible that other potentially meaningful HVCCC themes were excluded. However, the open-ended prompt allowed trainees to freely reflect on HVCCC topics, so conclusions derived from this analysis are likely significant. Given the large amount of collected reflections, we felt as a research team we were able to achieve thematic saturation. Third, our data is from a single institution and therefore transferability may be limited. For example, residents who train in contexts with larger numbers of underserved patients may not experience the same contrast as residents in our context. Fourth, the findings of this study are framed in an American context (i.e., ACGME core competencies) and do not speak towards the reciprocity of these international collaborations; this is a direction for future studies. Lastly, IHEs afford trainees experiential learning opportunities within different national health care models and systems, which may impact cost-awareness and practices. Further research is required to determine if these experiences result in lasting change.
Conclusion
Resident reflections point to the transformative nature of participation in IHEs, highlighting a perspective change and deeper commitment to HVCCC principles. These rich experiences are one facet of GME training that may be leveraged to prepare trainees for high-value practice. Transformative learning may be a useful framework, both within IHEs and the normal training environment, to help trainees understand and foster HVCCC practices.
References
Stammen LA, Stalmeijer RE, Paternotte E, et al. Training physicians to provide high-value, cost-conscious care: a systematic review. JAMA. 2015;314(22):2384-2400.
Moses H, III, Matheson DHM, Dorsey ER, et al. The anatomy of Health Care in the United States. JAMA. 2013;310(18):1947-1964.
Burner ST, Waldo DR, McKusick DR. National health expenditures projections through 2030. Health Care Financ Rev. 1992;14(1):1-29.
Hood VL, Weinberger SE. High value, cost-conscious care: an international imperative. European Journal of Internal Medicine. 2012;23(6):495-498.
Shrank WH, Rogstad TL, Parekh N. Waste in the US Health Care System: estimated costs and potential for savings. JAMA. 2019;322(15):1501-1509.
P D. The ABIM Foundation’s Choosing Wisely communication module Available: http://modules.choosingwisely.org/modules/m_00/. Accessed May 2021.
Physicians ACo. High value care curriculum Available: https://hvc.acponline.org/curriculum.html. Accessed May, 2021.
Dine CJ, Bellini LM, Diemer G, et al. Assessing correlations of physicians' practice intensity and certainty during residency training. Journal of Graduate Medical Education. 2015;7(4):603-609.
Sirovich BE, Lipner RS, Johnston M, et al. The association between residency training and internists’ ability to practice conservatively. JAMA Internal Medicine. 2014;174(10):1640-1648.
Epstein AJ, Asch DA, Barry CL. Effects of conflict-of-interest policies in psychiatry residency on antidepressant prescribing. LDI Issue Brief. 2013;18(3):1-4.
Asch DA, Nicholson S, Srinivas S, et al. Evaluating obstetrical residency programs using patient outcomes. JAMA. 2009;302(12):1277-1283.
Bansal N, Simmons KD, Epstein AJ, et al. Using patient outcomes to evaluate general surgery residency program performance. JAMA Surgery. 2016;151(2):111-119.
Chen C, Petterson S, Phillips R, et al. Spending patterns in region of residency training and subsequent expenditures for care provided by practicing physicians for medicare beneficiaries. JAMA. 2014;312(22):2385-2393.
Phillips RL, Jr., Petterson SM, Bazemore AW, et al. The effects of training institution practice costs, quality, and other characteristics on future practice. Ann Fam Med. 2017;15(2):140-148.
(ACGME) ACfGME. ACGME Common Program Requirements (Residency) Available: https://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/CPRResidency2020.pdf. Accessed 5/2021.
Teaching high-value, cost-conscious care to residents: the Alliance for Academic Internal Medicine–American College of Physicians Curriculum. Annals of Internal Medicine. 2012;157(4):284-286.
Phillips RL, Jr., Holmboe ES, Bazemore AW, et al. Purposeful imprinting in graduate medical education: opportunities for partnership. Fam Med. 2021.
Iglehart JK, Baron RB. Ensuring physicians' competence--is maintenance of certification the answer? N Engl J Med. 2012;367(26):2543-2549.
Drain PK, Holmes KK, Skeff KM, et al. Global health training and international clinical rotations during residency: current status, needs, and opportunities. Acad Med. 2009;84(3):320-325.
Nelson BD, Lee AC, Newby PK, et al. Global Health Training in Pediatric Residency Programs. Pediatrics. 2008;122(1):28-33.
Tupesis JP, Babcock C, Char D, et al. Optimizing global health experiences in emergency medicine residency programs: a consensus statement from the Council of Emergency Medicine Residency Directors 2011 Academic Assembly global health specialty track. Int J Emerg Med. 2012;5(1):43.
Nordhues HC, Bashir MU, Merry SP, et al. Graduate medical education competencies for international health electives: A qualitative study. Med Teach. 2017;39(11):1128-1137.
Sawatsky AP, Rosenman DJ, Merry SP, et al. Eight years of the Mayo International Health Program: what an international elective adds to resident education. Mayo Clin Proc. 2010;85(8):734-741.
Thompson MJ, Huntington MK, Hunt DD, et al. Educational effects of International Health Electives on U.S. and Canadian Medical Students and Residents: a literature review. Academic Medicine. 2003;78(3):342-347.
Battat R, Seidman G, Chadi N, et al. Global health competencies and approaches in medical education: a literature review. BMC Med Educ. 2010;10:94.
Guest G MK, Namey E. Applied Thematic Analysis. Thousand Oaks, California: SAGE Publications Inc 2012.
Sawatsky AP, Nordhues HC, Merry SP, et al. Transformative learning and professional identity formation during international health electives: a qualitative study using grounded theory. Acad Med. 2018;93(9):1381-1390.
Weng W, Van Parys J, Lipner RS, et al. Association of regional practice environment intensity and the ability of internists to practice high-value care after residency. JAMA Network Open. 2020;3(4):e202494-e202494.
Gladding S, Zink T, Howard C, et al. International electives at the university of Minnesota global pediatric residency program: opportunities for education in all Accreditation Council for Graduate Medical Education competencies. Acad Pediatr. 2012;12(3):245-250.
Lewkowicz D, Wohlbrandt A, Boettinger E. Economic impact of clinical decision support interventions based on electronic health records. BMC Health Serv Res. 2020;20(1):871.
van den Heuvel M, Au H, Levin L, et al. Evaluation of a social pediatrics elective: transforming students' perspective through reflection. Clin Pediatr (Phila). 2014;53(6):549-555.
Massé J, Dupéré S, Martin É, et al. Transformative medical education: must community-based traineeship experiences be part of the curriculum? A qualitative study. International Journal for Equity in Health. 2020;19(1):94.
Van Schalkwyk SC, Hafler J, Brewer TF, et al. Transformative learning as pedagogy for the health professions: a scoping review. Med Educ. 2019;53(6):547-558.
Acknowledgements
Contributors
None
Ethics declarations
The authors declare that they do not have a conflict of interest.
Ethical approval: This study was deemed exempt by the Mayo Clinic Institutional Review Board (IRB ID 14-008381).
Funding
None
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Prior presentations
A portion of this work was presented in abstract form at the Society of General Internal Medicine 2017 Annual Meeting in Washington, DC and has been accepted in abstract form for presentation at the Mayo Clinic 2021 Education Science and Scholarship Symposium in Rochester, MN
Rights and permissions
About this article

Cite this article
Matchett, C.L., Nordhues, H.C., Bashir, M.U. et al. Residents’ Reflections on Cost-Conscious Care after International Health Electives: A Single-Center Qualitative Study. J GEN INTERN MED 38, 42–48 (2023). https://doi.org/10.1007/s11606-022-07556-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-022-07556-8