
Abstract
Background
Splenic littoral cell angioma (LCA) is a rare vascular tumor with malignant potential originating from the red pulp of the spleen.1,2 Although laparoscopic splenectomy is the treatment choice for LCA,3 patients suffer from long-term complications of sepsis, thrombosis, and tumor.4,5 Laparoscopic central splenectomy (LCS) for LCA is a technically challenging operation mainly due to the risk of intraoperative hemorrhage. However, it can be a valuable alternative particularly for adolescent patients in whom maximum preservation of splenic function outweighs the risks associated with organ preservation.
Methods
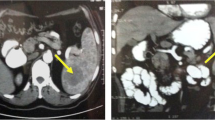
A 15-year-old young man was admitted with left upper abdominal dull pain for 1 month. Laboratory tests and enhanced abdominal CT scans were performed. Laboratory test results were all normal, as follows: complete blood count showed normal WBC: 5.74 × 109/l, platelets: 173 × 109/l, Hb: 151 g/l, tumor markers (CEA: 1.62 ng/ml, CA19–9: 10.30 U/ml, AFP: 1.13 ng/ml) which were within normal limits. CT scan showed that a 5 × 5.9-cm solid tumor was discovered in the middle part of the spleen during diagnosis, and the density of this tumor was high in the early artery phase and low in the late portal venous phase of contrast-enhanced CT. LCS was performed where the trunk of the splenic artery was intermittently occluded and several branches of the vessels were freed from the tumor which was then resected. The splenic parenchyma was dissected by following a line 0.5 cm from demarcation line. The tumor was completely removed with the activity of the splenic parenchyma being preserved to the maximum extent. Total operation time was 175 min, with an estimated blood loss of 200 ml; thus, no blood transfusion was required. Intraoperative frozen section suggested vascular tumor-like lesions, and then the tumor was completely removed with the resection margin being free of tumor involvement.
Results
The patient was fully recovered after a 7-day hospital stay. The reason for the 7-day hospital stay is that the patient maintains normal ambulating independent assistance on POD-3 and can eat without intravenous fluids on POD-4. Meanwhile, the patient needs to remove the drainage tube after the abdominal CT scan on POD-6, rather than postoperative complications. Diagnosis of LCA was confirmed using histology, and the symptoms disappearing after the operation was done. A total of 86·laparoscopic partial splenectomy (LPS) procedures were performed at the Department of Pancreatic Surgery, West China Hospital and Department of Hepatopancreatobiliary Minimal Invasive Surgery, Chengdu ShangJin NanFu Hospital from May 2011 to May 2020. Five patients among the total number of patients were diagnosed with LCA of which LPS was performed in four patients and LCS performed for one patient. The mean duration of surgery for LPS was 100 min (range of 80-120 min) while the mean estimated blood loss was 125 ml (range of 100-200 ml). On the other hand, the mean length of hospital stay was 7.5 days (range of 5-11 days) and the mean tumor diameter was 5.1 cm (range of 3.2-7 cm). All patients recovered without complications. In addition, there were no signs of immune insufficiency, thrombosis, and tumor recurrence during the follow-up which had a mean of 31.2 months (range from 10 to 53 months).
Conclusion
LCS is a technically feasible technique for a select group of patients with centrally located LCA. The technique helps to maximize preservation of splenic function and maintains the advantages of minimally invasive surgery.
Similar content being viewed by others


References
Falk S, Stutte HJ, Frizzera G. Littoral cell angioma. A novel splenic vascular lesion demonstrating histiocytic differentiation. Am J Surg Pathol. 1991;15(11):1023-1033.
Takayoshi K, Doi G, Tsuruta N, Yoshihiro T, Nio K, Tsuchihashi K, Ariyama H, Odawara J, Shimoda S, Kohashi K. Successful chemotherapeutic treatment for metastatic littoral cell angioma: A case report. Medicine. 2018;97(15). e0378
Cai Y-Q, Wang X, Ran X, Liu X-B, Peng B. Laparoscopic splenectomy for splenic littoral cell angioma. World J Gastroenterol. 2015;21(21):6660-6664.
Di Sabatino A, Carsetti R, Corazza GR. Post-splenectomy and hyposplenic states. Lancet. 2011;378(9785):86-97.
Kristinsson SY, Gridley G, Hoover RN, Check D, Landgren O. Long-term risks after splenectomy among 8,149 cancer-free American veterans: a cohort study with up to 27 years follow-up. Haematologica. 2014;99(2):392-398.
Author information
Authors and Affiliations
Contributions
Yongbin Li wrote the paper; Xin Wang and Yunqiang Cai edited the video. Bing Peng made the final approval of the version to be published.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent Statement
This study was approved by IRB at West China Hospital of Sichuan University, and informed consent was obtained before the operation and publication.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This abstract has been accepted as a video presentation at the 2020 SAGES Annual Meeting, Cleveland, OH.
Electronic supplementary material
(MP4 351003 kb)
Rights and permissions
About this article

Cite this article
Li, Y., Wang, X., Cai, Y. et al. Laparoscopic Central Splenectomy for Littoral Cell Angioma. J Gastrointest Surg 25, 576–577 (2021). https://doi.org/10.1007/s11605-020-04829-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-020-04829-7