
Abstract
Purpose
The aim of this feasibility study was to evaluate the diagnostic accuracy of ultra-low-dose CT colonography using iterative reconstruction algorithms with reference to standard colonoscopy.
Materials and methods
Prior to this study, a phantom study was performed to investigate the optimal protocol for ultra-low-dose CT colonography. A total of 206 patients with average/high risk of colorectal cancer were recruited. After undergoing full bowel preparation, the patients were scanned in the prone and supine positions with the CT conditions set to 120 kV, standard deviation 45 to 50, and an adaptive iterative reconstruction algorithm applied. Two expert readers read the images independently. The main outcome measures were the per-patient and per-polyp accuracies for the detection of polyps ≥ 10 mm, with colonoscopy results as the reference standard.
Results
Two hundred patients (102 females, mean age 67.5 years) underwent both ultra-low-dose CT colonography and colonoscopy on the same day. The mean radiation exposure dose was 0.64 ± 0.34 mSv. On colonoscopy, 39 patients had 45 polyps ≥ 10 mm (non-polypoid morphology 7), including 4 cancers. Per-patient sensitivity, specificity, and accuracy of CT colonography for polyps ≥ 10 mm were 0.74, 0.96, and 0.92 for reader one, and 0.74, 0.99, and 0.94 for reader two, respectively. Per-polyp sensitivities for polyps ≥ 10 mm were 0.73 for reader one and 0.71 for reader two. On subgroup analysis by morphology, non-polypoid polyps ≥ 10 mm were not detected by both readers.
Conclusion
Extreme ultra-low-dose CT colonography had an insufficient diagnostic performance for the detection of polyps ≥ 10 mm, because it was unable to detect non-polypoid polyps. This study showed that the problem with ultra-low-dose CT colonography was the lack of detectability of small-size polyps, especially non-polypoid polyps. To use ultra-low-dose CT colonography clinically, it is necessary to resolve the problems identified by this study.



Similar content being viewed by others
References
Pickhardt PJ, Choi JR, Hwang I, et al. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med. 2003;349:2191–200.
Johnson CD, Chen MH, Toledano AY, et al. Accuracy of CT colonography for detection of large adenomas and cancers. N Engl J Med. 2008;359:1207–17.
Tsurumaru D, Nishimuta Y, Kai S, Oki E, Nishie A. Factors of incomplete colonoscopy for stenosing colorectal cancer: CT colonography features. Jpn J Radiol. 2020;38:973–8.
Tsurumaru D, Takatsu N, Kai S, Oki E, Ishigami K. Measurement of circumferential tumor extent of colorectal cancer on CT colonography: relation to clinicopathological features and patient prognosis after surgery. Jpn J Radiol. 2021;39:966–72.
Nagata K, Endo S, Honda T, et al. Accuracy of CT colonography for detection of polypoid and non-polypoid neoplasia by gastroenterologists and radiologists: a nationwide multi-center study in Japan. Am J Gastroenterol. 2017;112:163–71.
Utano K, Nagata K, Honda T, et al. Diagnostic performance and patient acceptance of reduced-laxative CT colonography for the detection of polypoid and non-polypoid neoplasms: a multi-center prospective trial. Radiology. 2017;282:399–407.
Brenner DJ, Hall EJ. Computed tomography—an increasing source of radiation exposure. N Engl J Med. 2007;357:2277–84.
Costello JE, Cecava ND, Tucker JE, Bau JL. CT radiation dose: current controversies and dose reduction strategies. AJR Am J Roentgenol. 2013;201:1283–90.
Candela-Juan C, Montoro A, Ruiz-Martínez E, Villaescusa JI, Martí- BL. Current knowledge on tumour induction by computed tomography should be carefully used. Eur Radiol. 2014;24:649–56.
Flicek KT, Hara AK, Silva AC, Wu Q, Peter MB, Johnson CD. Reducing the radiation dose for CT colonography using adaptive statistical iterative reconstruction: a pilot study. AJR Am J Roentgenol. 2010;195:126–31.
Yoon MA, Kim SH, Lee JM, et al. Adaptive statistical iterative reconstruction and Veo: assessment of image quality and diagnostic performance in CT colonography at various radiation doses. J Comput Assist Tomogr. 2012;36:596–601.
Shin CI, Kim SH, Lee ES, et al. Ultra-low peak voltage CT colonography: effect of iterative reconstruction algorithms on performance of radiologists who use anthropomorphic colonic phantoms. Radiology. 2014;273:759–71.
Nagata K, Fujiwara M, Kanazawa H, et al. Evaluation of dose reduction and image quality in CT colonography: comparison of low-dose CT with iterative reconstruction and routine-dose CT with filtered back projection. Eur Radiol. 2015;25:221–9.
Lubner MG, Pooler BD, Kitchin DR, et al. Sub-milli Sievert (sub-mSv) CT colonography: a prospective comparison of image quality and polyp conspicuity at reduced-dose versus standard-dose imaging. Eur Radiol. 2015;25:2089–102.
Song JS, Choi EJ, Kim EY, et al. Attenuation-based automatic kilovoltage selection and sinogram-affirmed iterative reconstruction: effects on radiation exposure and image quality of portal-phase liver CT. Korean J Radiol. 2015;16:69–79.
Chang W, Lee JM, Lee K, et al. Assessment of a model based, iterative reconstruction algorithm (MBIR) regarding image quality and dose reduction in liver computed tomography. Invest Radiol. 2013;48:598–606.
Kang HJ, Kim SH, Shin CI, et al. Sub-millisievert CT colonography: effect of knowledge-based iterative reconstruction on the detection of colonic polyps. Eur Radiol. 2018;28:5258–66.
Liu JJ, Xue HD, Liu W, et al. CT colonography with spectral filtration and advanced modeled iterative reconstruction in the third-generation dual-source CT: image quality, radiation dose and performance in clinical utility. Acad Radiol. 2021;28:e127–36.
Shin CI, Kim SH, Im JP, et al. One-mSv CT colonography: Effect of different iterative reconstruction algorithms on radiologists’ performance. Eur J Radiol. 2016;85:641–8.
Nagata K, Fujiwara M, Shimamoto T, Iida N, Mogi T, Mitsushima T. Colonic distension at CT colonography: randomized evaluation of both intravenous hyoscine butyl bromide and automated insufflation. AJR Am J Roentgenol. 2015;204:76–82.
No authors listed. The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon—November 30 to December 1, 2002. Gastrointest Endosc. 2003;58:S3–43.
Utano K, Takayanagi D, Nagata K, et al. A novel volume-reduced CT colonography regimen using hypertonic laxative (polyethylene glycol with ascorbic acid): randomized controlled trial. Eur Radiol. 2019;29:5236–46.
Neri E, Halligan S, Hellström M, et al. The second ESGAR consensus statement on CT colonography. Eur Radiol. 2013;23:720–9.
ACR–SAR–SCBT-MR practice parameter for the performance of computed tomography (CT) colonography in adults. Available via: https://www.acr.org/-/media/ACR/Files/Practice-Parameters/CT-Colonog.pdf. Accessed 5 September 2021
Liedenbaum MH, Venema HW, Stoker J. Radiation dose in CT colonography–trends in time and differences between daily practice and screening protocols. Eur Radiol. 2008;18:2222–30.
Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2016;315:2564–75.
Provenzale D, Jasperson K, Ahnen DJ, et al. Colorectal cancer screening, version 1.2015. J Nat Compr Cancer Netw. 2015;13:959–68.
Sakane H, Ishida M, Shi L, et al. Biological effects of low-dose chest CT on chromosomal DNA. Radiology. 2020;295:439–45.
Cianci R, Delli Pizzi A, Esposito G, et al. Ultra-low dose CT colonography with automatic tube current modulation and sino2019gram-affirmed iterative reconstruction: effects on radiation exposure and image quality. J Appl Clin Med Phys. 2019;20:321–30.
Liedenbaum MH, van Rijn AF, de Vries AH, et al. Using CT colonography as a triage technique after a positive fecal occult blood test in colorectal cancer screening. Gut. 2009;58:1242–9.
Fidler JL, Johnson CD, MacCarty RL, et al. Detection of flat lesions in the colon with CT colonography. Abdom Imaging. 2002;27:292–300.
Togashi K, Utano K, Kijima S, et al. Laterally spreading tumors: limitations of computed tomography colonography. World J Gastroenterol. 2014;20:17552–7.
Utano K, Katsuki S, Matsuda T, et al. Colon capsule endoscopy versus CT colonography in patients with large non-polypoid tumours: a multicentre prospective comparative study (4CN Study). Digestion. 2020;101:615–23.
Heresbach D, Djabbari M, Riou F, et al. Accuracy of computed tomographic colonography in a nationwide multicentre trial, and its relation to radiologist expertise. Gut. 2011;60:658–65.
Fidler JL, Zhang Z, Herman BA, et al. CT colonography for the detection of non-polypoid adenomas: sensitivity assessed with restricted national CT colonography trial criteria. AJR Am J Roentgenol. 2014;203:W614–22.
Tachibana R, Näppi JJ, Ota J, et al. Deep learning electronic cleansing for single- and dual-energy CT colonography. Radiographics. 2018;38:2034–50.
Uemura T, Näppi JJ, Ryu Y, Watari C, Kamiya T, Yoshida H. A generative flow-based model for volumetric data augmentation in 3D deep learning for computed tomographic colonography. Int J Comput Assist Radiol Surg. 2021;16:81–9.
Acknowledgements
The authors would like to thank Rika Ishizuka of Aizu Medical Center for providing administrative support.
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of the institution and with the Helsinki declaration. The study protocol was approved by the Institutional Review Board.
Informed consent
Written informed consent was obtained from all patients.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
11604_2022_1266_MOESM1_ESM.tif
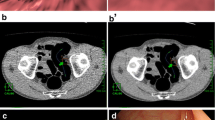
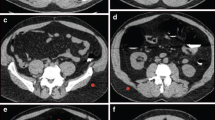
Supplementary file1 0-Is+IIa polyp, 14 mm in size, cecum, tubular adenoma. CT image at SD = 20. Flat component is recognizable around the ridge (arrow head). (TIF 4097 KB)
11604_2022_1266_MOESM2_ESM.tif
Supplementary file2 0-Is+IIa polyp, 14 mm in size, cecum, tubular adenoma. Almost no artifacts are seen, and the sessile part of the polyp is recognizable (arrow head). However, the surrounding flat component that could be seen at SD = 20 is difficult to recognize. It has been suggested that it is more difficult to depict non-polypoid components with ultra-low-dose CT colonography than with normal-dose CT colonography. (TIF 4096 KB)
11604_2022_1266_MOESM3_ESM.tif
Supplementary file3 0-Is+IIa polyp, 14 mm in size, cecum, tubular adenoma. Endoscopic image. Flat component is seen around the ridge (arrow head). (TIF 3757 KB)
About this article

Cite this article
Yasuda, T., Honda, T., Utano, K. et al. Diagnostic accuracy of ultra-low-dose CT colonography for the detection of colorectal polyps: a feasibility study. Jpn J Radiol 40, 831–839 (2022). https://doi.org/10.1007/s11604-022-01266-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11604-022-01266-1