
Abstract
Background
Androgen deprivation therapy (ADT), a cornerstone of prostate cancer treatment, is commonly co-prescribed as combination therapy.
Objective
To better understand the safety and tolerability profile of relugolix, an oral non-peptide gonadotropin-releasing hormone (GnRH) receptor antagonist, in combination with abiraterone acetate (abiraterone) and apalutamide, a phase I study was undertaken.
Patients and Methods
This is an ongoing, 52-week, open-label, parallel cohort study of relugolix in combination with abiraterone in men with metastatic castration-sensitive prostate cancer (mCSPC) or metastatic castration-resistant prostate cancer (mCRPC) [Part 1] and apalutamide in men with mCSPC or non-metastatic castration-resistant prostate cancer (nmCRPC) [Part 2]. Eligible patients treated with leuprolide acetate or degarelix with abiraterone or apalutamide prior to baseline, at which time they were transitioned to relugolix. Assessments included reporting of adverse events, clinical laboratory tests, vital sign measurements, electrocardiogram (ECG) parameters, and testosterone serum concentrations. In this interim report, patients completing ≥12 weeks were included.
Results
Overall, 15 men were enrolled in Part 1 and 10 in Part 2. Adverse events were mostly mild-to-moderate in intensity and were consistent with the known safety profiles of the individual medications. No transition (from prior ADT treatment)- or time-related trends in clinical laboratory tests, vital sign measurements, or ECG parameters were observed. Mean testosterone concentrations remained below castration levels.
Conclusions
Combination therapy of relugolix and abiraterone or apalutamide was associated with a favorable safety and tolerability profile consistent with the known profiles of the individual medications. Castration levels of testosterone were maintained after transitioning to relugolix from other ADTs.
Clinical Trial Registration
ClinicalTrials.gov identifier: NCT04666129
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Androgen deprivation therapy (ADT), a cornerstone of prostate cancer treatment, is commonly co-prescribed as combination therapy. |
To better understand the safety and tolerability profile of relugolix, an oral non-peptide gonadotropin-releasing hormone (GnRH) receptor antagonist, in combination with abiraterone acetate (abiraterone) or apalutamide, a phase I study was undertaken. |
In the study, we found that the combination therapy of relugolix and abiraterone or apalutamide was associated with a favorable safety and tolerability profile consistent with the known profiles of the individual medications. Castration levels of testosterone were maintained after transitioning to relugolix from other ADTs. |
1 Introduction
Relugolix is an orally active, non-peptide gonadotropin-releasing hormone (GnRH) receptor antagonist approved in the United States (US) and Europe for the treatment of advanced prostate cancer [1, 2]. After oral administration of relugolix, luteinizing hormone (LH) and follicle-stimulating hormone (FSH) concentrations rapidly decline, with corresponding reductions in systemic testosterone concentrations, consistent with its mechanism of action [3,4,5,6] In the phase III HERO trial, relugolix demonstrated suppression of testosterone concentrations to castration levels in 96.7% of patients from Day 29 through 48 weeks, which was superior to leuprolide, and resulted in a 54% lower risk of major adverse cardiovascular events [7].
As disease progresses, medications with complementary mechanisms are commonly co-prescribed with androgen deprivation therapy (ADT) to suppress extratesticular testosterone production or block androgen receptors on cancer cells, including abiraterone acetate (abiraterone) and apalutamide [8,9,10]. Abiraterone is an inhibitor of cytochrome P450 (CYP) 17A, an enzyme involved in the biosynthesis of testosterone from steroid precursors expressed in the testes, adrenal glands and prostatic tumor tissue. Abiraterone decreases testosterone production both systemically and locally [11, 12]. Apalutamide is an androgen receptor inhibitor that blocks testosterone from binding to androgen receptors on cancer cells, preventing their growth [13].
Treatment guidelines for prostate cancer, such as those issued by the National Comprehensive Cancer Network® (NCCN®), recommend combination therapy of ADT plus another medication as a treatment option for men with advanced prostate cancer [8]. Following regulatory approvals of relugolix, there was a need for additional safety and drug interaction data with common prostate cancer medications that could be used in a combination therapy. Increasingly, more clinical trial data are becoming available [14, 15]. In this study, we describe the interim results from assessments of safety and efficacy of relugolix combination treatment with abiraterone or apalutamide.
2 Methods
2.1 Trial Design and Treatments
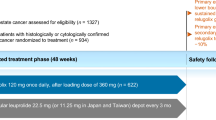
This is an ongoing phase I, 52-week, open-label, parallel-cohort, safety and tolerability study of relugolix in combination with abiraterone with a corticosteroid (Part 1), apalutamide (Part 2) or docetaxel with or without a corticosteroid (Part 3) in men with advanced prostate cancer (Clinical Trial identifier: NCT04666129). Part 3 has been discontinued due to a lack of enrollment and will not be reported herein. Each part of the study consisted of a 12-week primary study treatment period and a 40-week safety extension treatment period for a total of 52 weeks of combination treatment with relugolix and abiraterone (Part 1) or apalutamide (Part 2) [electronic supplementary Fig. S1]. Men with advanced prostate cancer were to be transitioned from leuprolide acetate or degarelix to relugolix (120 mg [Part 1] or 240 mg [Part 2], orally, once daily after a single loading dose of 360 mg) as the ADT component of treatment on the approximate date the next injection was due. For Part 2 only, the recommended daily dose of relugolix was increased to 240 mg considering that apalutamide is a combined permeability glycoprotein (P-gp) and strong CYP3A inducer that causes relugolix concentrations to be reduced by approximately half. Treatment with the combination medication was continued as previously prescribed. The dose and dosing regimen for study treatments are provided in Table 1.
The study was approved by local independent review boards and conducted in accordance with International Conference on Harmonization guidelines and ethical principles of the Declaration of Helsinki. All patients provided written informed consent prior to having any screening procedures performed. This study was conducted in the US.
2.2 Patients
Eligible patients had a documented medical history of either metastatic castration-sensitive prostate cancer (mCSPC) [Part 1 and Part 2], non-metastatic castration-resistant prostate cancer (nmCRPC) [Part 2] or metastatic castration-resistant prostate cancer (mCRPC) [Part 1]. Patients with a previous diagnosis of mCSPC (Part 1 and Part 2) were those with at least two of three of the following factors: total Gleason score of ≥6, presence of two or more metastatic lesions on bone scan or other imaging modality, or evidence of measurable visceral metastases, with the exception of hepatic metastases. Patients with a previous diagnosis of nmCRPC (Part 2 only) were those without evidence of metastatic disease by imaging and who demonstrated disease progression despite maintaining castration levels of testosterone with ADT, as evidenced by consecutive increases in prostate-specific antigen (PSA) concentrations (two measurements, at least 1 week apart) with an absolute PSA concentration ≥2 ng/mL. Patients with mCRPC (Part 1) were those with evidence of metastatic disease by imaging and who demonstrated disease progression despite maintaining castration levels of testosterone with ADT consistent with the Prostate Cancer Working Group 3 (PCWG3) guidelines [16, 17], as evidenced by consecutive increases in PSA concentrations (two measurements, at least 3 weeks apart) of ≥25% and ≥2 ng/mL above the nadir and the progression of pre-existing disease, either a worsening of symptoms and/or radiologic evidence of enlarged metastatic lesions, and/or the development of new metastases.
Patients were those being treated with leuprolide acetate (3-, 4- or 6-month injectable depot formulations: intramuscular [Lupron®], subcutaneous [Eligard®]) or degarelix (Firmagon®) in combination with either abiraterone plus a corticosteroid (Part 1) or apalutamide (Part 2). Prior treatment with abiraterone (Part 1) or apalutamide (Part 2) was to have been well tolerated, defined as no evidence of hepatotoxicity requiring dose adjustment for a minimum of 12 weeks or no fracture, fall or seizure episode, or need for dose adjustment due to an adverse event for a minimum of 6 weeks prior to the baseline (Day 1) visit, respectively. Patients were required to have an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1 at the baseline (Day 1) visit and a testosterone serum concentration <50 ng/dL at the screening visit or prior to the baseline (Day 1) visit.
Patients with mCSPC or nmCRPC were excluded from participation if they had received combination therapy for longer than 24 months and patients with mCRPC for longer than 6 months, or if they had abnormal clinical laboratory test value(s) for various hematologic parameters, or indicative of a clinically significant decrease in renal function, uncontrolled diabetes or hepatotoxicity (Part 1 only), a medical history of significant cardiac condition within 6 months prior to screening, an abnormal electrocardiogram (ECG) or a QTcF >470 ms, uncontrolled hypertension or hypotension or bradycardia.
2.3 Assessments
The primary study objective was to evaluate the safety and tolerability of relugolix as the ADT component of combination treatment during the 12-week primary study treatment period in each study part. Secondary objectives included the safety and tolerability of relugolix as the ADT component of combination treatment for up to 52 weeks, assessment of serum testosterone concentrations during the 12-week primary study treatment period, and measurement of drug concentrations (Part 2 only). Assessment of safety, which was the same in each study part, included clinical laboratory tests, vital sign measurements, ECG parameters at Weeks 3, 5, 9 and 13, reporting of adverse events throughout the 52 weeks of treatment, and measurement of vital signs at Week 53. Blood samples for determination of testosterone and PSA serum concentrations, and relugolix and apalutamide and N-desmethyl apalutamide concentrations (Part 2), were to be collected at the baseline (Day 1), Week 5, and Week 13/early termination (ET) visits during the 12-week primary study treatment period only.
2.4 Statistical Analysis
No formal calculation for sample size was provided as this was an exploratory phase I study. A sample size of approximately 24 patients was planned for each study part. In Part 1, no more than six patients with mCRPC were to be enrolled.
All safety parameters were to be analyzed on the Safety Population, defined as all patients who have been enrolled and initiated study treatment with at least a single administration of relugolix in combination with abiraterone (Part 1) or apalutamide (Part 2). In this interim analysis, patients completing ≥12 weeks as well as patients who terminated early were included.
The analyses supporting the primary study objective included a descriptive evaluation of safety and tolerability for each study Part based on the assessments of safety. Analyses supporting secondary study objectives included a descriptive summary of serum testosterone concentrations and the number and proportion of patients with testosterone concentrations ≥50 ng/dL at baseline, Week 5 and Week 13 by study part (Part 1, Part 2) and plasma concentrations of relugolix, apalutamide and N-desmethyl- apalutamide (Part 2 only) during the 12-week primary study treatment period.
3 Results
3.1 Patients
From March 2021 to October 2022, a total of 15 patients in Part 1 and 10 patients in Part 2 were enrolled into this ongoing trial. In Part 1, patients received relugolix in combination with abiraterone for a median of 281 days (range 48–367 days), with five patients completing the study through Week 53. One patient was discontinued from the study in the safety extension treatment period due to disease progression. In Part 2, patients received relugolix in combination with apalutamide for a median of 180 days (range 1–383 days), with one patient completing the study through Week 53. Two patients discontinued from the study in the safety extension treatment period due to disease progression and one patient discontinued from the study after approximately 4 weeks of treatment due to adverse events of fatigue, hot flash, and body aches. The mean (standard deviation) age was 72.3 (7.87) and 68.1 (7.14) years in Part 1 and Part 2, respectively (Table 2). The majority of patients in each study part had a diagnosis of mCSPC (Part 1: 86.7%; Part 2: 100%).
3.2 Safety
In Part 1, 79 non-serious adverse events were reported among 15 patients (100%) [Table 3], most of which were rated as mild or moderate in intensity (grade 1 or 2). A single serious adverse event (hospitalization due to a left femur fracture) was rated as severe in intensity (grade 3) and considered not to be related to study treatment. Eighteen of the 79 non-serious adverse events were considered by the investigator to be possibly or probably related to relugolix, 21 possibly or probably related to abiraterone and 4 possibly related to the corticosteroid. The most frequently reported adverse events in 2 or 3 of 15 (≥10%) patients included pain in extremity, alanine aminotransferase (ALT) increased, anemia, back pain, constipation, hypertension, memory impairment, rash, and vomiting. No transition (to relugolix from prior ADT treatment)- or time-related trends in clinical laboratory tests, vital signs or ECG parameters were observed.
In Part 2, 28 non-serious adverse events were reported among eight patients (80%) [Table 3], most of which were mild or moderate in intensity (grade 1 or 2). A total of two grade 3–4 adverse events were reported. Eleven of the 28 non-serious adverse events were considered by the investigator to be possibly or probably related to relugolix, with 12 possibly or probably related to apalutamide. The most frequently reported adverse events in 1 or 2 of 10 (≥10%) patients were pain in extremity, ALT increased, anemia, and vomiting. A single serious adverse event of a neuroendocrine tumor, considered an important medical event, was reported that was considered by the investigator not to be related to study treatment. No clinically significant transition (to relugolix from prior ADT treatment) or time-related trends in clinical laboratory tests, vital signs, or ECG parameters were observed.
3.3 Testosterone and Drug Concentrations
In Part 1, median (range) testosterone serum concentrations at the baseline (Day 1) visit were 1.0 (1.0–8.0) ng/dL, and following the transition to relugolix were 1.0 (1.0–14.0) and 1.0 (1.0–34.0) ng/dL at Week 5 and Week 13, respectively, well below castration levels (Table 4). In Part 2, median testosterone serum concentrations at the baseline (Day 1) visit were 14.5 ng/dL, and following the transition to relugolix were 15.0 and 14.0 ng/dL at Week 5 and Week 13, respectively, well below castration levels (Table 4). In both Part 1 and Part 2, there were no patients who were above castration levels (i.e., testosterone concentrations ≥50 ng/dL) at baseline (Day 1), Week 5, or Week 13/ET.
Mean relugolix trough plasma concentrations over 12 weeks of treatment (11.9, 11.6, 9.2 and 13.1 ng/mL at Weeks 3, 5, 9 and 13, respectively) [electronic supplementary Fig. 2SA] were similar to historical values (10.7 ng/mL) [2]. Mean apalutamide and N-desmethyl-apalutamide trough plasma concentrations prior to and after initiation of treatment with relugolix were similar (apalutamide: baseline = 3640 ng/mL vs. 3981, 3829, 3557 and 3559 ng/mL at Weeks 3, 5, 9 and 13, respectively; N-desmethyl-apalutamide: baseline = 4454 ng/mL vs. 4565, 4698, 4493 and 4626 ng/mL at Weeks 3, 5, 9 and 13, respectively) [electronic supplementary Figs. S2B and S2C] and also similar to historical values (3681 and 4646 ng/mL, respectively) [13].
4 Discussion
This report detailed the ongoing results of a phase I study assessing the safety and tolerability of relugolix in combination with abiraterone or apalutamide in men with advanced prostate cancer. Although a total of 24 patients per study part are planned for enrollment, this interim report provides an aggregate assessment of safety and tolerability for the first 15 and 10 patients enrolled in Part 1 and Part 2, respectively. The results show no change in the risk–benefit profile of relugolix when administered with abiraterone or apalutamide. Adverse events observed during the trial were mostly mild-to-moderate and were consistent with known safety profiles of the individual medications. No transition- or time-related trends in clinical laboratory tests, vital sign measurements, or ECG parameters were observed in either part of the study. Mean testosterone concentrations remained below castration levels following the transition from prior ADT to relugolix during the 12-week primary study treatment period.
For relugolix, the adverse events in this study were similar to those observed in the phase III HERO study [7]. Hot flash, fatigue, constipation, diarrhea, and arthralgia were the most frequently reported adverse events observed in men receiving relugolix in the HERO study (>10%). Similarly, adverse events considered by the investigator to be probably or possibly related to abiraterone or apalutamide were generally consistent with their known safety profiles [12, 13].
Based on the known metabolism and drug interaction profiles associated with relugolix and abiraterone, a drug interaction between these two medications is not anticipated; hence, no drug concentrations to assess a potential interaction were obtained in Part 1 of the current study. Abiraterone acetate is a prodrug that is hydrolyzed to the active moiety abiraterone, which subsequently undergoes biotransformation to two inactive metabolites, abiraterone sulfate and N-oxide abiraterone sulfate mediated by CYP3A and/or the sulfotransferase enzyme, SULT2A1 [12]. Relugolix does not inhibit CYP3A and although relugolix is a slight CYP3A inducer, no clinically meaningful reductions in systemic abiraterone concentrations are expected upon concomitant use with relugolix [1]. Conversely, abiraterone is an inhibitor of CYP2D6, for which relugolix is not a substrate, and CYP2C8, which is a minor metabolic pathway of relugolix; therefore, no effect of abiraterone on relugolix exposure is anticipated. Considering relugolix is a substrate for P-gp and apalutamide is a known combined P-gp and strong CYP3A inducer, the dose of relugolix should be increased to 240 mg once daily upon concomitant use with apalutamide [1]. Mean relugolix trough concentrations during combination treatment with apalutamide were consistent with historical concentrations with relugolix 120 mg, indicating that by increasing the dose of relugolix to 240 mg during concomitant administration with an inducer achieves similar exposures to those at the recommended daily dose of 120 mg without an inducer. Although apalutamide is primarily metabolized by CYP2C8 and CYP3A4 (to form the active metabolite N-desmethyl apalutamide), relugolix is not an inhibitor of these CYP enzymes. Mean apalutamide trough concentrations prior to and after initiation of treatment with relugolix on baseline (Day 1) were similar, demonstrating that there was no impact of relugolix on apalutamide concentrations upon concomitant use. A recently published study showed that relugolix administered at approved standard doses concurrently with apalutamide was effective in maintaining castrate testosterone levels in patients with high-risk localized prostate cancer without new safety signals [15].
Based on the available literature, combination therapy of ADT plus another agent is recommended as a treatment option by the NCCN guidelines [8]. Although relugolix was included as an ADT, the guideline also refers to the paucity of safety data and drug interaction information with relugolix as the ADT component of treatment in combination with other medications. The results of this study help to address this data gap and support the use of relugolix in combination with abiraterone or apalutamide. Another recent analysis of the HERO study showed treatment with relugolix was associated with similar efficacy and safety profiles with and without concomitant enzalutamide or docetaxel [14]. For relugolix, no clinically significant differences in the pharmacokinetics of relugolix were observed when coadministered with voriconazole (strong CYP3A inhibitor), atorvastatin, enzalutamide, or acid-reducing agents [1].
4.1 Study Limitations
The assessment of safety and tolerability for relugolix in combination with abiraterone or apalutamide in this study is based on a relatively small number of currently enrolled patients, and because of the lack of a comparator group, an objective assessment of safety is potentially limited. However, the intent of the study was to provide experiential data with relugolix as the ADT component of combination therapy to identify a potential safety signal in a phase I research setting. Furthermore, the original design was a limitation because all patients were transitioning from GnRH agonists to relugolix. The current study has been amended to reduce the screening period for Part 1 and Part 2 as well as enroll and evaluate new patients who are just starting combination therapy with relugolix (i.e., not transitioning) and patients taking relugolix prior to enrollment; these results will be reported in a future publication. Additional insight on relugolix used in combination therapy may be gained from a recently initiated observational study (OPTYX; NCT05467176).
5 Conclusions
In this interim analysis, combination treatment with relugolix and abiraterone or apalutamide was generally safe and well tolerated in patients with advanced prostate cancer. Safety profiles were consistent with the individual medications. Apalutamide plasma concentrations prior to and after initiation of treatment with relugolix were similar. Testosterone concentrations were maintained at castration levels following the transition to relugolix from prior ADT.
References
ORGOVYX (relugolix) tablets [package insert]. Brisbane: Myovant Sciences, Inc.; 2022.
ORGOVYX (relugolix) tablets [summary of product characteristics]. Barcelona, Spain: Accord Healthcare S.L.U. Available at: https://www.ema.europa.eu/en/documents/product-information/orgovyx-epar-product-information_en.pdf. Accessed 26 Jan 2023.
Suzuki H, Uemura H, Mizokami A, et al. Phase I trial of TAK-385 in hormone treatment-naïve Japanese patients with nonmetastatic prostate cancer. Cancer Med. 2019;8(13):5891–902.
MacLean DB, Shi H, Faessel HM, et al. Medical castration using the investigational oral GnRH antagonist TAK-385 (relugolix): phase 1 study in healthy males. J Clin Endocrinol Metab. 2015;100:4579–87.
Dearnaley DP, Saltzstein DR, Sylvester JE, et al. The oral gonadotropin-releasing hormone receptor antagonist relugolix as neoadjuvant/adjuvant androgen deprivation therapy to external beam radiotherapy in patients with localised intermediate-risk prostate cancer: a randomised, open-label, parallel-group phase 2 trial. Eur Urol. 2020;78(2):184–92.
Saad F, Bailen JL, Pieczonka CM, et al. Second interim analysis (IA2) results from a phase II trial of TAK-385, an oral GnRH antagonist, in prostate cancer patients (pts). J Clin Oncol. 2016;34(2 Suppl):200.
Shore ND, Saad F, Cookson MS, et al. Oral relugolix for androgen-deprivation therapy in advanced prostate cancer. N Engl J Med. 2020;382(23):2187–96.
National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology. Prostate Cancer. 2022. Version 1.2023. 16 Sep 2022. Available at: www.NCCN.org. Accessed 18 Dec 2022.
Lowrance WT, Breau RH, Chou R, et al. Advanced prostate cancer: AUA/ASTRO/SUO guideline PART I. J Urol. 2021;205(1):14–21.
Parker C, Castro E, Fizazi K, et al. Electronic address: clinicalguidelines@esmo.org. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31(9):1119–34.
Efstathiou E, Titus M, Tsavachidou D, et al. Effects of abiraterone acetate on androgen signaling in castrate-resistant prostate cancer in bone. J Clin Oncol. 2012;30(6):637–43.
Zytiga (abiraterone) Prescribing information. Horsham: Janssen Biotech, Inc.; 2021.
Erleada (apalutamide) Prescribing Information. Horsham: Janssen Pharmaceutical Companies; 2019.
George DJ, Shore ND, Saad F, et al. Impact of concomitant prostate cancer therapy on efficacy and safety of relugolix versus leuprolide in men with advanced prostate cancer: Subgroup analysis from the phase III HERO study. J Clin Oncol. 2021;39(Suppl 6):106.
Brown G, Belkoff L, Hafron JM, et al. Coadministration of apalutamide and relugolix in patients with localized prostate cancer at high risk for metastases. Target Oncol. 2023;18:95–103.
Scher HI, Morris MJ, Stadler WM, et al. Trial design and objectives for castration resistant prostate cancer: updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J Clin Oncol. 2016;34:1402–18.
Becker DJ, Iyengar AD, Punekar SR, et al. Treatment of metastatic castration-resistant prostate cancer with abiraterone and enzalutamide despite PSA progression. Anticancer Res. 2019;39(5):2467–73.
DeTora, et al. Good publication practice (GPP) guidelines for company-sponsored biomedical research: 2022 update. Ann Intern Med. 2022;175(9):1298–304.
Acknowledgments
This study was funded by Myovant Sciences GmbH, in collaboration with Pfizer Inc. The authors would like to acknowledge the patients who participated in these studies and their families, as well as all the investigators and site staff who made these studies possible. The authors would also like to acknowledge editorial support from J.D. Cox, PhD, and Mayville Medical Communications, funded by Myovant Sciences GmbH, in collaboration with Pfizer Inc., and in compliance with Good Publication Practice 4 ethical guidelines [18].
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Myovant Sciences GmbH in collaboration with Pfizer Inc.
Conflicts of interest
Elizabeth Migoya, Bruce Brown, and Sophia Lu are employees of Myovant. Sergio C. Gatoulis is an employee of Pfizer. Laurence Belkoff: Consultant for Marius Pharm and Astellas. Lawrence Gervasi: Speakers bureau for Astellas, Bayer, Dendreon, Janssen, and Myovant. Jose De La Cerda: Consulting or advisory role with Dendreon, Myriad Pharmaceuticals, and Pfizer/Astellas. Curtis Dunshee: Consulting/advisory role and research funding from Astellas and Pfizer; consulting/advisory role for Pfizer during the conduct of this study; and research funding from Janssen Oncology, Dendreon, Myovant Sciences, and AstraZeneca. Paul Sieber: Advisory role for Pfizer and Verity; research funding from Astellas, AstraZeneca, Bayer, Dendreon, Janssen, Merck, Myovant, Orion, and Pfizer; and speaker’s bureau for Astellas, Bayer, Dendreon, Janssen, Merck, Myovant, and Pfizer. Neal Shore: Consulting or advisory role for Bayer, Janssen Scientific Affairs, Dendreon, Tolmar, Ferring, Medivation/Astellas, Amgen, Pfizer, AstraZeneca, Genentech, and Myovant Sciences; speakers’ bureau for Janssen, Bayer, and Dendreon. Ronald Tutrone: Speakers bureau for Myovant Sciences, Astellas, Pfizer, and Exosome; consultant/advisory board for Propella Pharm, Myovant Sciences, and Bayer.
Availability of data and material
Myovant is the owner of the raw data, which it considers to be proprietary and does not share the data with anyone other than regulatory authorities. At the conclusion of the study, results will be available through ClinicalTrials.gov and other public outlets.
Ethics approval
Independent Institutional Review Boards at all participating institutions approved the study, which was conducted in accordance with International Council for Harmonisation guidelines for Good Clinical Practice and according to the principles of the Declaration of Helsinki.
Consent to participate
All patients provided written informed consent.
Consent to publish
Informed consent was obtained from all individual participants included in the study. No patient-identifying information is included in this article, therefore consent to publish was not required.
Code availability
Not applicable.
Author contributions
All authors participated in the design and conduct of this study, had access to the data, drafted the manuscript with input from the sponsor (Myovant), reviewed and approved the manuscript before submission, made the decision to submit the manuscript for publication, and agreed to be accountable for all aspects of this work. Sophia Lu had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
De La Cerda, J., Dunshee, C., Gervasi, L. et al. A Phase I Clinical Trial Evaluating the Safety and Dosing of Relugolix with Novel Hormonal Therapy for the Treatment of Advanced Prostate Cancer. Targ Oncol 18, 383–390 (2023). https://doi.org/10.1007/s11523-023-00967-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11523-023-00967-5