
Abstract
Gambling-related harms can impact the lives of children living with someone experiencing a gambling problem. These harms have been associated with impacts across a number of domains. However, previous studies exploring gambling-related effects on the health and wellbeing of children have had conflicting results. This study aimed to further understand the impact of parental gambling problems on children's health and wellbeing using nationally representative data from Growing up in Australia: The Longitudinal Study of Australian Children. The subsample of interest contained 3,695 children (49.1% female) across two cohorts aged around 12 and 16 years. Parental gambling problems were measured by the Problem Gambling Severity Index (PGSI). Child health and wellbeing was measured via the Child Health Utility 9D (CHU9D), the Spence Anxiety Scale, the Short Mood & Feelings Questionnaire, the Strengths and Difficulties Questionnaire (SDQ), and self-harm and happiness questions. Across both cohorts, the study found significant associations between parental gambling problems and poorer health, anxiety and/or low mood symptoms, and behavioural and emotional problems in children. The study found that more than 10% of Australian children were living in households with adults experiencing some level of gambling problems, including 1.2% in households with severe problems. Policymakers and educators might help ensure that the appropriate information and support is being provided to these children.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Harms associated with excessive gambling can affect the health and wellbeing of people close to the affected gambler (close significant others [CSO]; Langham et al., 2016) and can especially have an impact on children living in households where someone is experiencing a gambling problem. These harms affect many areas of the children’s lives. Financial problems are one of the more significant harms associated with gambling. Patford (2009) found that children are often unaware or too young to understand the financial issues related to harmful gambling. However, they can experience their consequences (Langham et al., 2016; Wurtzburg & Tan, 2011), such as missing out on necessities (Landon et al., 2018) or school supplies and trips (Darbyshire et al., 2001; Langham et al., 2016). In addition, gambling problems are associated with relationship difficulties between parents, and between parents and children (Wurtzburg & Tan, 2011), which can contribute to stress and tension within the household, and lead to a child’s loss of trust in the parent (Darbyshire et al., 2001). Many studies have found that children of gamblers are likely to be victims of violence or anger towards them from parents (Iusitini et al., 2011; Landon et al., 2018; Lorenz & Shuttlesworth, 1983). However, using a large nationally representative sample, Afifi et al. (2010) found problem gamblers were less likely to perpetrate minor physical assaults on their children than those classified as non-problem gamblers. Thus, the full picture of how gambling problems affect children is still to be discovered. Overall, households with people living with gambling problems can be tense and chaotic places (Darbyshire et al., 2001; Patford, 2009) that have householders who often struggle with multiple comorbid stressors (Tulloch et al., 2020).
A person who gambles with attendant problems spends less time with their family (Langham et al., 2016), and this has been associated with ineffective (Vitaro et al., 2008) and absent (Darbyshire et al., 2001) parenting, and can lead to children being left unattended (Landon et al., 2018) or neglected (Li et al., 2017). In some cases, other family members are required to support the children (Landon et al., 2018). There is a risk of separation from parents due to divorce (Darbyshire et al., 2001; Jacobs et al., 1989) or the child’s removal from the household (Langham et al., 2016). The children tend to take on increased responsibility (Wurtzburg & Tan, 2011), including household tasks normally viewed as parental responsibilities. Older children and adolescents help in managing finances and providing support to the other parent (Landon et al., 2018; Langham et al., 2016). Children can suffer from stigma, social isolation and lack of social support due to difficulties talking about family problems with those outside the household (Wurtzburg & Tan, 2011), or estrangement from extended family due to gambling problems (Darbyshire et al., 2001). Socialisation to gambling is also associated with the increased risk of the child developing their own gambling problems (Vachon et al., 2004; Walters, 2021; Wurtzburg & Tan, 2011).
Gambling-related harms have been associated with decrements in health and wellbeing. However, findings around the impacts of parental gambling problems on the health and wellbeing of children have been mixed, particularly concerning psychological health. For example, poor child health outcomes are associated with financial problems within the household (Langham et al., 2016), such as a lack of healthy food (Darbyshire et al., 2001) or limited funds for medications, health or dental care (Darbyshire et al., 2001; Dickson-Swift et al., 2005). In addition, children of a parent with a gambling problem have also been shown to experience conduct (Vitaro et al., 2008), delinquency (Walters, 2021), and behavioural problems (Lorenz & Shuttlesworth, 1983), and increased impulsivity-hyperactivity and inattention (Carbonneau et al., 2018). Furthermore, they can have feelings of anger (Lesieur & Rothschild, 1989; Patford, 2009) and distress (Darbyshire et al., 2001; Patford, 2009), and increased risk of suicide attempts (Lesieur & Rothschild, 1989). There are also associations with tobacco, drug and alcohol use (Jacobs et al., 1989) and eating problems (Jacobs et al., 1989; Lesieur & Rothschild, 1989). Overall, Jacobs et al. (1989, p. 265) found that children of problem gamblers reported poorer “quality of youth” than others.
In looking specifically at psychological health, Vitaro et al. (2008) found parental problem gambling associated with symptoms of depression in their children. However, other studies have found no significant difference between children who are CSOs and non-CSOs concerning their psychological health. Comparing children of parents categorised as ‘problem gamblers’ to a normative sample, Dowling et al. (2009) found no statistically significant differences in either depression or anxiety. Lesieur and Rothschild’s (1989) study had a larger percentage of controls unexpectedly experiencing an unhappy state of mind or low mood when compared with children of treatment-seeking gamblers. There may be several reasons for these differences. Vitaro et al.'s (2008) participants were drawn from an extensive community study, while Lesieur and Rothschild (1989) and Dowling et al. (2009) used smaller samples related to treatment-seeking gamblers. Treatment may have a positive effect on the family’s psychological wellbeing (Kourgiantakis et al., 2013).
Additionally, many other factors are associated with a child’s mental health and wellbeing. For example, sports participation is associated with both physical and psychological health benefits (Granger et al., 2017; Graupensperger et al., 2021) and children have reported utilising activities like sports to cope with gambling problems in the family (Wurtzburg & Tan, 2011). However, sports participation can reduce during early adolescence (Rullestad et al., 2021), and there may be barriers to participation such as gender diversity (Storr et al., 2021) or socioeconomic status (Rullestad et al., 2021; World Health Organization (WHO), 2020), although findings can be inconsistent (Sagatun et al., 2008). Overall, a Scottish Government (2020) report found that in children, general health, physical activity, and experiences at home and school were stronger predictors of mental health and wellbeing than socio-demographic factors. In short, household gambling problems are only one determinant, amongst many, that can potentially impact on children’s health and wellbeing.
Aims and Objectives
This study aimed to understand further the impacts of a parental gambling problem on the health and wellbeing of children using population-representative data on Australian children. Specifically, it explores whether harms to the health and wellbeing of children increase with parental problem gambling severity, and if so, whether these associations continue after controlling for selected factors that contribute to children’s wellbeing.
Methods
Study Design
The cross-sectional study is a secondary analysis using data from the Growing up in Australia: The Longitudinal Study of Australian ChildrenFootnote 1 study (LSAC; Mohal et al., 2021). The LSAC is a longitudinal study that began in 2004 and follows two large representative samples of Australian children; cohort B began assessing participants from birth, and cohort K started at kindergarten age (4–5 years). The study has a broad focus, examining development and wellbeing topics such as health, family, education, parenting, and peers. Participants were recruited using a probability sample design. Full details of the study design can be found at Mohal et al. (2021) and Usback et al. (2018).
Participants and Procedure
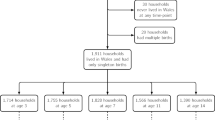
This study utilised only LSAC Wave 7, conducted in 2016. Wave 7 was the only wave in which parental gambling and children's health and wellbeing were both measured. The LSAC follows two age cohorts separated by around 4 years. Both age cohorts were used in the current study; however, they were analysed and reported separately due to slight differences in variables across cohorts and the differences across age and development. Therefore, no statistical comparison of the two cohorts was conducted. At the time of Wave 7, participants in cohort B were aged around 12 years and cohort K was about 16 years. The sub-samples of interest are described in the results and consisted of participants who completed the health and wellbeing questions and whose parent/s completed the Problem Gambling Severity Index (PGSI; Ferris & Wynne, 2001).
Measures
Parental problem gambling severity was assessed via the PGSI (Ferris & Wynne, 2001), which was self-completed by the adults in the household. The 9-item PGSI is a well-validated measure of gambling problems and identifies symptoms of potentially harmful gambling behaviours (Currie et al., 2013). Summed scores range from 0 to 27, with higher scores representing more severe gambling problems. From these scores, parents can be classified as either a “non-problem gambler” (total score of 0), “low-risk gambler” (1 or 2), “moderate-risk gambler” (3 to 7), or “problem gambler” (8 +).
Health-related quality of life (HRQoL) was assessed via the Child Health Utility 9D (CHU9D; Stevens, 2009). The CHU9D is an HRQoL instrument for young people, validated for use in Australia (Stevens & Ratcliffe, 2012). The utility scores range from 0 to 1, representing the worst health status to full health, respectively.
Mental Health was assessed via several measures. Anxiety symptoms were measured by 8-items drawn from the Spence Anxiety Scale (S. Spence, 1998; S. Spence et al., 2014), which has reported good internal consistency (Cronbach alpha = 0.80; S. Spence et al., 2003). Participants were asked to rate “how often these things happen to you” on a 4-point scale from 0 (never), 1 (sometimes), 2 (often), or 3 (always). Total scores range from 0 to 24, with higher scores reflecting greater anxiety symptoms. Depressed feelings were measured by the 13-item Short Mood & Feelings Questionnaire (Angold et al., 1995). Participants were asked about how much they “felt or acted this way in the past two weeks” about aspects such as “I felt miserable or unhappy” or “I didn’t enjoy anything at all”. Valid responses were true (0), sometimes (1), and not true (2). Total summed scores ranged from 0 to 26, with higher scores indicative of a lower mood. Self-harm and suicide intentions were assessed in the older children (Cohort K). Participants were asked to respond Yes (1) or No (0) to the following questions referring to the previous 12 months. “Have you thought about hurting yourself on purpose in any way?”, “Have you hurt yourself on purpose in any way?”, “Did you ever seriously consider attempting suicide?” and “Did you make a plan about how you would attempt suicide?” Responses were summed to create total ‘self-harm’ scores ranging from 0 to 4, with higher scores indicating greater self-harm thoughts or actions.
Subjective wellbeing was assessed via a single-item question about happiness. Participants were asked, “In general, I am happy with how things are for me in my life right now”. Responses range from strongly disagree (1) to strongly agree (5).
Behavioural attributes are measured by the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997), a brief behavioural screen developed to identify behavioural and emotional problems in children and adolescents. Participants are asked to rate each question as “not true”, “somewhat true”’, or “certainly true”. The 25 questions assess behavioural attributes across five subscales (prosociality, hyperactivity, emotional symptoms, peer problems and conduct problems), with scores ranging from 0 to 10 for each scale. Higher scores on the prosocial subscale reflect greater strength, higher scores on the remaining subscales reflect greater difficulties. A total score is also generated by summing scores from all scales except prosociality (which is analysed separately). Valid scores range from 0 to 40, with higher total scores reflecting greater difficulties.
A binary sports participation variable was derived from questions which asked the parent in the case of the younger cohort: “In the last week, has the child participated in any of the following activities? Regularly? means at least once a week, for three months or more, e.g. a sports season. Team sport (e.g. football, cricket or netball)” and a similar question asking about “Individual sport, coached or lessons (e.g. swimming, tennis, karate or gymnastics)”. In the older cohort, the children were asked “In the last 12 months, did you regularly participate in any of the following organised activities outside of school hours/organised activities? Team sport” and a similar question about “Individual sport, coaching or lessons”. “Yes” answers to either question were categorised as “yes” for the variable sports participation.
Socioeconomic and demographic characteristics of the household were assessed with questions probing weekly household income, the parents’ age and their highest level of education. Education was ranked from postgraduate degree (1) through to no non-school qualification (6). The Index of Relative Socioeconomic Disadvantage (IRDS; Australian Bureau of Statistics, 2018) summarises a range of economic and social factors. Low scores indicated greater disadvantage in the area, and high scores reflect a lack of disadvantage.
Statistical Analysis
Both cohorts were analysed separately. Descriptive statistics were used to describe the samples. Due to the skewed nature of the health and wellbeing variables, non-parametric tests (Spearman’s rho correlations) were used to explore the relationship between parental problem gambling severity and the health and wellbeing of children in the household. Logistic regression was conducted to examine the significant relationships while controlling for demographic and socio-economic factors. Skewed variables were transformed for these analyses. There was independence of residuals, as assessed by Durbin-Watson. There was no evidence of multicollinearity, as evaluated by tolerance values greater than 0.1 and variance inflation factor (VIF) values less than 10. Visual inspections of plots confirmed the assumption of normality and homoscedasticity. Bonferroni adjusted significance values were used due to the increased risk of Type 1 errors associated with multiple analyses. Supplied data weights were used for all analyses; for details, see Usback et al. (2018).
Ethics
The LSAC study was approved by the Australian Institute of Family Studies Ethics Committee. Approval for secondary analysis was granted by Central Queensland University Human Research Ethics Committee (#23,269).
Results
Descriptive statistics of Cohort B are detailed in Table 1. Cohort B (N = 1,979) has a mean age of 12.5 years (SD = 0.50; 50.0% females). The parental PGSI scores ranged from 0 to 23. In this cohort, looking at the parent in the household with the most severe gambling problem, 0.9% had at least one parent categorised in the problem gambling category of the PGSI, and a further 7.9% categorised as ‘at risk’ (i.e. low- or moderate- risk gamblers, scores 1–7). As outlined in Table 2, Cohort K’s (N = 1,716) mean age was 16.5 years (SD = 0.50; 48.2% females). The parental PGSI scores ranged from 0 to 24. In this cohort, 1.6% of children had at least one parent in the problem gambling category of the PGSI, and a further 11.0% had at least one parent at risk.
As detailed in Tables 1 and 2, across both cohorts, parents scoring one or greater on the PGSI were slightly younger, less educated, had a lower household income and lived in an area of greater disadvantage than those without a gambling problem. Children across both cohorts, whose parental PGSI score was one or greater, reported significantly worse HRQoL, lower mood and greater anxiety symptoms than those with a parental PGSI score of 0. The younger children also reported significantly lower happiness scores when the parental PGSI score was one or greater, and the older children had a greater number of self-harm thoughts and behaviours when the parental PGSI score was one or greater in comparison to those with a parental PGSI score of 0. Children living with parental gambling problems reported increased difficulties across the total SDQ, and its four subscales (hyperactivity, emotional symptoms, peer problems and conduct problems). In both cohorts, there was no significant difference in sports participation between children who had a parent who scored one or more on the PGSI and those who were not experiencing a gambling problem.
Tables 3 and 4 provide correlation matrices of all variables for both cohorts. There was a significant relationship between parental PGSI scores and mood and anxiety in both younger and older children. The children in both cohorts reported greater anxiety and feelings of low mood as the parent’s gambling problems increased. Parental gambling problems were also associated with worse health and lower happiness in the younger children. In the older cohort, increasing parental gambling problems were also associated with greater self-harm thoughts and behaviours. There was a significant association between the children’s SDQ total scores and parental gambling in both cohorts, with overall increased difficulties associated with more severe parental gambling problems. Specific areas of association in the younger cohort were conduct problems, emotional problems and peer problems. In the older children, there were significant correlations between parental gambling and conduct problems, emotional symptoms, hyperactivity and peer problems.
Multiple regressions were conducted for each cohort to control for the children’s gender and other parental and household factors that could plausibly affect health and wellbeing. As shown in Table 5, in the younger group, parental PGSI was no longer a significant predictor of health or wellbeing factors. In the older cohort, parental PGSI continued to significantly predict mood, with increasing gambling problems associated with lower mood.
Discussion
This study used a representative sample of Australian children to explore the relationship between the health and wellbeing of the children and parental gambling problems. In the older cohort, 1.6% lived in a household with a parent categorised as a 'problem gambler', 3.8% with a 'moderate-risk gambler', and 7.2% 'low-risk gambler'. The prevalence rates were slightly lower in the younger cohort; however, these proportions are generally consistent with the national prevalence of problem gambling in Australia (Armstrong & Carroll, 2017; Hing et al., 2021). Households where gambling problems were present tended to have younger, less well-educated parents, lower incomes and be located in areas of greater disadvantage. This is consistent with known problem gambling risk factors (Armstrong & Carroll, 2017). Across both the younger and older cohorts, the study found significant associations between parental gambling problems and HRQoL, symptoms of anxiety, feelings of low mood, and behavioural and emotional problems in the children. Significant relationships between gambling problems and (low) happiness were also found in the younger cohort. The current study found no significant relationship between sports participation and parental PGSI. However, sports participation was associated with higher household income, less disadvantage and more highly educated parents.
Both younger and older children showed significantly increased behavioural difficulties as the parental gambling problem increased in severity. These manifested as conduct problems, emotional symptoms, hyperactivity and peer problems. This result supports previous findings associating parental gambling problems with conduct problems, delinquency and behavioural problems (Lorenz & Shuttlesworth, 1983; Vitaro et al., 2008; Walters, 2021). Conduct problems have also been found to be strongly associated with negative family experiences (Scottish Government, 2020). There was a significant relationship between parental gambling problems and self-harm, and suicidal thoughts and behaviours in this study; Lesieur and Rothschild (1989) had similar findings of increased suicide attempts amongst children of a parent with a gambling problem.
The current findings of an association with anxiety and low mood is in line with results found by (Vitaro et al., 2008) but not those of Lesieur and Rothschild (1989) and Dowling et al. (2009). This incongruence again may be due to our use of a community sample rather than a treatment-related sample. However, there may be an age factor involved too. Once other factors were controlled, the impact on mood only continued to have a significant relationship with the older children. It may be that younger children are less aware or more protected from gambling problems in the household. Older children are the ones who might be more likely to take on the physical and mental weight of extra responsibilities in the households, such as housework, managing finances, care of younger siblings, and emotionally supporting their parents (Langham et al., 2016). They may also be more aware of the stigma associated with gambling problems (Wurtzburg & Tan, 2011).
Limitations
The results of this study should be interpreted in light of several limitations. First, gambling problems are relatively uncommon in general population samples, especially severe problems. Therefore, this study may lack the statistical power to detect some small effects. For instance, the lack of findings for wellbeing decrements in younger children of households with gambling problems, after controlling for other factors, may only remain undetected due to low power. Second, as discussed, children’s health and wellbeing are also impacted by many factors (Scottish Government, 2020). Therefore, any single contributor tends to exert a small individual impact (Dolan et al., 2008; Geerling & Diener, 2020) and may be difficult to isolate due to the complex nature of the relationship of these variables. Further work might attempt to control for as many other health and wellbeing influences as possible as well as explore interaction effects. This might be achieved by using a more purposeful sample of children with many parents classified as at-risk and problem gamblers. Finally, our study was limited by a cross-sectional design. The LSAC did not begin asking about gambling until recently. Longitudinal studies that can follow children would be highly beneficial, since a time course of early gambling problems for parents impacting on later problems experienced by children would better support a presumed causal connection.
Conclusions
Across the cohorts, an average of more than 10% of Australian children reside in households with people experiencing some level of gambling problems, with around 1.2% living in homes with at least one parent with a severe gambling problem. In addition, many other children may be impacted by a parent with a gambling problem living outside their household due to divorce, separation or estrangement. Our study found associations between these parental gambling problems and the health and wellbeing of their children living in the same household. While the harm appears to manifest more seriously when children are older, preventative efforts and support might be provided to all children of parents with a gambling problem to minimise the impact of their harms. The results from this study could inform gambling education programs both for parents and children. The findings could be used to increase parental awareness of how their own gambling can affect their children. And programs, particularly school based as they cover most children, can educate and build awareness to reduce the harms associated with a child's own gambling. They also might help ensure that they include education about how and where children can seek support for any problem they are experiencing due to another person's gambling. Access to available interventions, particularly in the early teenage years may be vital in supporting children later in adolescence.
Notes
This paper uses unit record data from The Longitudinal Study of Australian Children [LSAC] conducted by the Australian Government Department of Social Services (DSS). The findings and views reported in this paper, however, are those of the author[s] and should not be attributed to the Australian Government, DSS, or any of DSS’ contractors or partners. https://doi.org/10.26193/BAA3N6
References
Afifi, T. O., Brownridge, D. A., MacMillan, H., & Sareen, J. (2010). The relationship of gambling to intimate partner violence and child maltreatment in a nationally representative sample. Journal of Psychiatric Research, 44(5), 331–337. https://doi.org/10.1016/j.jpsychires.2009.07.010
Angold, A., Costello, E., & Messer, S. (1995). Development of a Short Questionnaire for Use in Epidemiological Studies of Depression in Children and Adolescents: Factor Composition and Structure Across Development. International Journal of Methods in Psychiatric Research, 5, 251–262.
Armstrong, A., & Carroll, M. (2017). Gambling activity in Australia. Melbourne: Australian Gambling Research Centre, Australian Institute of Family Studies. https://apo.org.au/sites/default/files/resource-files/2017/11/apo-nid120736-1192821.pdf. Accessed August 2019.
Australian Bureau of Statistics. (2018). Census of Population and Housing: Socio-Economic Indexes for Areas (SEIFA), Australia, 2016. In Australian Bureau of Statistics. https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/2033.0.55.001~2016~Main%20Features~IRSD~19. Accessed August 2019.
Carbonneau, R., Vitaro, F., Brendgen, M., & Tremblay, R. E. (2018). The Intergenerational Association Between Parents’ Problem Gambling and Impulsivity-Hyperactivity/Inattention Behaviors in Children. Journal of Abnormal Child Psychology, 46(6), 1203–1215. https://doi.org/10.1007/s10802-017-0362-x
Currie, S. R., Hodgins, D. C., & Casey, D. M. (2013). Validity of the Problem Gambling Severity Index interpretive categories. Journal of Gambling Studies, 29(2), 311–327. https://doi.org/10.1007/s10899-012-9300-6
Darbyshire, P., Oster, C., & Carrig, H. (2001). The experience of pervasive loss: Children and young people living in a family where parental gambling is a problem. Journal of Gambling Studies, 17(1), 23–45. https://doi.org/10.1023/a:1014536315167
Dickson-Swift, V. A., James, E. L., & Kippen, S. (2005). The experience of living with a problem gambler: Spouses and partners speak out. Journal of Gambling Issues. https://doi.org/10.4309/jgi.2005.13.6
Dolan, P., Peasgood, T., & White, M. (2008). Do we really know what makes us happy? A review of the economic literature on the factors associated with subjective well-being. Journal of Economic Psychology, 29(1), 94–122. https://doi.org/10.1016/j.joep.2007.09.001
Dowling, N., Smith, D., & Thomas, T. (2009). The family functioning of female pathological gamblers. International Journal of Mental Health and Addiction, 7(1), 29–44. https://doi.org/10.1007/s11469-007-9126-0
Ferris, J., & Wynne, H. (2001). The Canadian Problem Gambling Index: Final report. Canadian Centre on Substance Abuse. Retrieved from www.ccgr.ca/en/projects/resources/CPGI-Final-Report-English.pdf. Accessed August 2019.
Geerling, D., & Diener, E. (2020). Effect size strengths in subjective well-being research. Applied Research in Quality of Life, 15(1), 167–185. https://doi.org/10.1007/s11482-018-9670-8
Goodman, R. (1997). The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x
Granger, E., Di Nardo, F., Harrison, A., Patterson, L., Holmes, R., & Verma, A. (2017). A systematic review of the relationship of physical activity and health status in adolescents. European Journal of Public Health, 27(suppl_2), 100–106. https://doi.org/10.1093/eurpub/ckw187
Graupensperger, S., Sutcliffe, J., & Vella, S. A. (2021). Prospective Associations between Sport Participation and Indices of Mental Health across Adolescence. Journal of Youth and Adolescence, 50(7), 1450–1463. https://doi.org/10.1007/s10964-021-01416-0
Hing, N., Russell, A. M. T., Browne, M., Rockloff, M., Greer, N., Rawat, V., Stevens, M., Dowling, N., Merkouris, S., King, D., Breen, H., Salonen, A., & Woo, L. (2021). The second national study of interactive gambling in Australia (2019–20). https://www.gamblingresearch.org.au/publications/new-second-national-study-interactive-gambling-australia-2019-20. Accessed December 2021
Iusitini, L., Gao, W., Sundborn, G., & Paterson, J. (2011). Parenting Practices Among Fathers of a Cohort of Pacific Infants in New Zealand. Journal of Cross-Cultural Psychology, 42(1), 39–55. https://doi.org/10.1177/0022022110361778
Jacobs, D. F., Marston, A. R., Singer, R. D., Widaman, K., Little, T., & Veizades, J. (1989). Children of problem gamblers. Journal of Gambling Behavior, 5(4), 261–268. https://doi.org/10.1007/BF01672427
Kourgiantakis, T., Saint-Jacques, M.-C., & Tremblay, J. (2013). Problem gambling and families: A systematic review. Journal of Social Work Practice in the Addictions, 13(4), 353–372. https://doi.org/10.1080/1533256X.2013.838130
Landon, J., Grayson, E., & Roberts, A. (2018). An exploratory study of the impacts of gambling on affected others accessing a social service. International Journal of Mental Health and Addiction, 16(3), 573–587. https://doi.org/10.1007/s11469-017-9785-4
Langham, E., Thorne, H., Browne, M., Donaldson, P., Rose, J., & Rockloff, M. (2016). Understanding gambling related harm: A proposed definition, conceptual framework, and taxonomy of harms. BMC Public Health, 16, 80. https://doi.org/10.1186/s12889-016-2747-0
Lesieur, H. R., & Rothschild, J. (1989). Children of Gamblers Anonymous members. Journal of Gambling Behavior, 5(4), 269–281. https://doi.org/10.1007/BF01672428
Li, E., Browne, M., Rawat, V., Langham, E., & Rockloff, M. (2017). Breaking bad: Comparing gambling harms among gamblers and affected others. Journal of Gambling Studies, 33(1), 223–248. https://doi.org/10.1007/s10899-016-9632-8
Lorenz, V. C., & Shuttlesworth, D. E. (1983). The impact of pathological gambling on the spouse of the gambler. Journal of Community Psychology, 11(1), 67–76. https://doi.org/10.1002/1520-6629(198301)11:1%3c67::AID-JCOP2290110107%3e3.0.CO;2-O
Mohal, J., Lansangan, C., Gasser, C., Taylor, T., Renda, J., Jessup, K., & Daraganova, G. (2021). Growing up in Australia: The Longitudinal Study of Australian Children - Data Users Guide, Release 9C1. https://growingupinaustralia.gov.au/data-and-documentation/data-user-guide. Accessed August 2021.
Patford, J. (2009). For worse, for poorer and in ill health: How women experience, understand and respond to a partner’s gambling problems. International Journal of Mental Health and Addiction, 7(1), 177–189. https://doi.org/10.1007/s11469-008-9173-1
Rullestad, A., Meland, E., & Mildestvedt, T. (2021). Factors Predicting Physical Activity and Sports Participation in Adolescence. Journal of Environmental and Public Health, 2021, 9105953. https://doi.org/10.1155/2021/9105953
Sagatun, A., Kolle, E., Anderssen, S. A., Thoresen, M., & Søgaard, A. J. (2008). Three-year follow-up of physical activity in Norwegian youth from two ethnic groups: Associations with socio-demographic factors. BMC Public Health, 8, 419. https://doi.org/10.1186/1471-2458-8-419
Scottish Government. (2020). Factors Affecting Children’s Mental Health and Wellbeing: Findings from the Realigning Children’s Services Wellbeing Surveys (2015–2017). https://www.gov.scot/publications/factors-affecting-childrens-mental-health-wellbeing-findings-realigning-childrens-services-wellbeing-surveys-2015-2017/documents/. Accessed September 2021.
Spence, S. (1998). A measure of anxiety symptoms among children. Behaviour Research and Therapy, 36(5), 545–566. https://doi.org/10.1016/s0005-7967(98)00034-5
Spence, S., Barrett, P., & Turner, C. (2003). Psychometric properties of the Spence Children’s Anxiety Scale with young adolescents. Journal of Anxiety Disorders, 17(6), 605–625. https://doi.org/10.1016/s0887-6185(02)00236-0
Spence, S., Sawyer, M., Sheffield, J., Patton, G., Bond, L., Graetz, B., & Kay, D. (2014). Does the absence of a supportive family environment influence the outcome of a universal intervention for the prevention of depression? International Journal of Environmental Research and Public Health, 11(5), 5113–5132. https://doi.org/10.3390/ijerph110505113
Stevens, K. (2009). Developing a descriptive system for a new preference-based measure of health-related quality of life for children. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 18(8), 1105–1113. https://doi.org/10.1007/s11136-009-9524-9
Stevens, K., & Ratcliffe, J. (2012). Measuring and valuing health benefits for economic evaluation in adolescence: An assessment of the practicality and validity of the child health utility 9D in the Australian adolescent population. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 15(8), 1092–1099. https://doi.org/10.1016/j.jval.2012.07.011
Storr, R., Nicholas, L., Robinson, K., & Davies, C. (2021). ‘Game to play?’: Barriers and facilitators to sexuality and gender diverse young people’s participation in sport and physical activity. Sport, Education and Society. https://doi.org/10.1080/13573322.2021.1897561
Tulloch, C., Browne, M., Hing, N., & Rockloff, M. (2020). The relationship between family gambling problems, other family stressors, and health indicators in a large population-representative sample of Australian adults. Journal of Gambling Studies, 37(4), 1139–1162. https://doi.org/10.1007/s10899-020-09990-x
Usback, S., & Australian Bureau of Statistics LSAC processing team and the Australian Bureau of Statistics Household Survey Methodology team. (2018). Growing Up in Australia: The Longitudinal Study of Australian Children (LSAC) LSAC Technical Paper No. 20: Wave 7 weighting and non-response. https://growingupinaustralia.gov.au/data-and-documentation/technical-papers. Accessed August 21.
Vachon, J., Vitaro, F., Wanner, B., & Tremblay, R. E. (2004). Adolescent gambling: Relationships with parent gambling and parenting practices. Psychology of Addictive Behaviors: Journal of the Society of Psychologists in Addictive Behaviors, 18(4), 398–401. https://doi.org/10.1037/0893-164X.18.4.398
Vitaro, F., Wanner, B., Brendgen, M., & Tremblay, R. E. (2008). Offspring of parents with gambling problems: Adjustment problems and explanatory mechanisms. Journal of Gambling Studies, 24(4), 535–553. https://doi.org/10.1007/s10899-008-9096-6
Walters, G. D. (2021). Parental Gambling as a Moderator of the Child Delinquency-Gambling Relationship: Does Having a Role Model in the Home Make a Difference? Journal of Gambling Studies / Co-Sponsored by the National Council on Problem Gambling and Institute for the Study of Gambling and Commercial Gaming, 37(1), 27–41. https://doi.org/10.1007/s10899-020-09962-1
World Health Organization (WHO). (2020). Spotlight on Adolescent Health and Well-Being. Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada International Report,. https://apps.who.int/iris/bitstream/handle/10665/332091/9789289055000-eng.pdf. Accessed May 2020.
Wurtzburg, S., & Tan, R. (2011). Sociology of gambling: Gambling parents’ impact on their children in Christchurch. New Zealand Sociology, 26(2), 36–57. https://www.scopus.com/inward/record.uri?eid=2-s2.0-84856049088&partnerID=40&md5=fbb2c5c5f4ab3f410e28a6f0e8d4f63d. Accessed May 2020.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions CT was supported by a Central Queensland University Research Stipend Scholarship and a New South Wales Office of Responsible Gambling part-PHD scholarship.
Author information
Authors and Affiliations
Contributions
CT was responsible for study conception and CT, NH, MB and MR all contributed to study design. Material preparation and analysis was performed by CT. The first draft of the manuscript was written by CT and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics
Ethics approval for secondary analysis was granted by CQUniversity Human Research Ethics Committee (#22878).
Conflict of Interest
The authors declare no conflict of interest for this study.
The 3-year declaration of interest for each author follows:
• CT was supported by a Central Queensland University Research Stipend Scholarship and a New South Wales Office of Responsible Gambling part-PHD scholarship. CT has contributed to research projects funded by Gambling Research Australia, New South Wales Office of Responsible Gambling, and the Victorian Responsible Gambling Foundation.
• NH has received research funds from the Victorian Responsible Gambling Foundation, New South Wales Office of Responsible Gambling, the South Australian Department of Human Services, Queensland Justice and Attorney-General, Gambling Research Australia, New Zealand Ministry of Health, Australian Communications and Media Authority, the Alberta Gambling Research Institute, Australian Government Department of Social Services, New Zealand Ministry of Health, and Australia’s National Research Organisation for Women’s Safety.
• MB has received funding from the New South Wales Office of Liquor and Gaming, the Victorian Responsible Gambling Foundation, the Queensland Government Department of Health, the Tasmanian Department of Treasury and Finance, the South Australian Department of Human Services, the Alberta Gambling Research Institute, Gambling Research Australia, the New Zealand Ministry of Health, the Department of Families, Housing, Community Services and Indigenous Affairs, the Australian Department of Innovation, Industry, Science and Research, and the Department of Foreign Affairs and Trade.
• MR has received research grants from the Queensland Treasury, the Victorian Treasury, the Victorian Responsible Gambling Foundation, the New Zealand Ministry of Health, the NSW Dept of Industry and Trade, the Department of Social Services, the Tasmanian Department of Treasury and Finance, the Alberta Gambling Research Institute, the South Australian Department of Human Services, the Alberta Gambling Research Institute and Gambling Research Australia.
• MH has received funding from the Alberta Gambling Research Institute (AGRI) for conference travel.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tulloch, C., Hing, N., Browne, M. et al. Parental Gambling and the Health and Wellbeing of Children Derived From Two Nationally Representative Cohorts of Australian Children. Applied Research Quality Life 17, 3049–3068 (2022). https://doi.org/10.1007/s11482-022-10052-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11482-022-10052-0