
Abstract
Until now, there has been no evidence-based, specific advice for people who gamble who want to reduce their risk of experiencing gambling harms. This paper presents the results from the first large-scale, comprehensive, international project to develop lower-risk gambling guidelines. Specifically, we calculated relative risk estimates to determine risk of harm across the range of possible limits for gambling frequency, expenditure, and number of types of gambling engaged in; conducted an online survey (n = 4583) of people who gamble to assess whether they understood and found credible the proposed quantitative limits; conducted a series of interviews and focus groups with people who gamble to assess self-control strategies and reactions to proposed quantitative limits; conducted a meta-analysis of problem gambling risk factors in the general population; and consulted with a pan-Canadian, multi-sectoral committee of stakeholders. Project outcomes were examined and deliberated by a working group of scientists who decided upon a set of recommendations for lower-risk gambling. This paper presents these recommendations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
For many individuals, gambling is associated with negative consequences ranging from minor financial pressures to devastating family, work, and emotional impacts. In many jurisdictions, including Canada, an important but insufficient regulatory response to this risk of harm is to provide public health advice for individuals to limit their gambling. To date, in the absence of a reasonable evidence base, the advice has been quite general and has not provided specific recommendations for how often to play and how much to spend to avoid risk. The key message is “set a limit and stick with it,” without elaboration for what the limit should involve.
The current paper describes the results of two studies that emerged from a 5-year, international, program of research to develop Lower-Risk Gambling Guidelines (LRGG). We began this program of research by publishing our research plan (Currie & Low Risk Gambling Guidelines Scientific Working, 2019) which identified the research necessary to develop a workable set of LRGGs. Emerging from this program was research examining self-control strategies among regular gamblers (Currie et al., 2020), a meta-analysis of problem gambling risk factors in the general adult population (Allami et al., 2021), interviews and focus groups with people who gamble (Flores-Pajot et al., 2021), and risk curve analyses conducted with eleven high-quality data sets from eight Western countries (Hodgins et al., submitted). To assist in the development of the complete set of guidelines that include the quantitative limits and the accompanying messaging, we conducted two additional studies: (1) an assessment of relative risk of harm across the full range of possible limits for gambling frequency, expenditure, and number of types of gambling; and (2) a survey of over 10,000 people who gamble to assess whether they understood and found credible the proposed quantitative limits. We end this paper with a description of the final recommendations of the scientific working group regarding lower-risk gambling.
Empirically Derived Ranges of Quantitative Limits
Over the past decades, data of increasing rigour are available to quantitatively assess the association between gambling involvement and harm in the general population. These data can be used to derive objective numerical limits to avoid risk and for identifying moderating factors (e.g., individual characteristics that moderate the association) (Currie et al., 2017; Currie et al., 2008; Dowling et al., 2018). As noted by Holmes et al. (2019), for guidelines to be widely adopted and to have public health impact, they must have credibility with the public and with other stakeholders. Thus, while empirically derived quantitative limits for risk are a critical input into the establishment of final guidelines, they may be influenced by other pragmatic considerations such as how acceptable these guidelines are to the general public, or how simple or complex the final messages will be. Holmes et al. (2019) urged transparency in these decisions. As reported in Hodgins et al. (submitted), a world-wide audit of available cross-sectional and longitudinal prevalence surveys suitable for risk curve analyses identified 11 high-quality datasets from 8 countries (Canada, the USA, Iceland, Finland, Sweden, France, New Zealand, and Australia). Gambling involvement indicators were monthly expenditure, percentage of income spent on gambling, monthly frequency, duration of gambling sessions, and number of different types of gambling. Harm indicators included self-reported financial, emotional, health, and relationship impacts; harms described in the Victoria framework (Langham et al., 2016). This framework recognizes that gambling-related harm can be experienced across the range of gambling involvement, and is not limited to individuals with a diagnosis of gambling disorder (Browne et al., 2016; Li et al., 2017).
Risk curve analyses were independently conducted for each dataset to examine differences and similarities in the optimal limits for increased risk of harm. These analyses found consistency in the results across harm indicators, cross nationally. Reliable ranges of values were obtained for all gambling indicators except gambling session duration. Risk of gambling-related harm is likely to increase if an individual gambles $60 to $120 CAD or more per month, gambles five to eight times or more per month, spends 1 to 3% or more of gross monthly income, or plays three to four or more different gambling types.
In addition to this large survey study, we also conducted a series of English and French focus groups and qualitative interviews with 56 individuals who gamble (Flores-Pajot et al., 2021). These interviews revealed that self-regulatory strategies involving expenditure limits were reported as more frequently employed by participants than those concerning gambling frequency or time devoted to gambling. Strategies concerning expenditure included restricting access to money, and keeping track of money allocated to gambling. Of note, participants described their personal limits as fluid from occasion to occasion and described numerous types of social and environmental influences on their limits at any given time, including use of alcohol. Participants tended to track their expenditure per occasion versus longer periods of time (e.g., weekly, monthly).
In related research, our team examined the self-regulatory efforts people naturally make to limit their involvement in gambling (Currie et al., 2020). A national online panel of English and French-speaking Canadians representing the range of gambling involvement from infrequent to heavy to problematic gambling (N = 10,054) revealed that over 70% of the sample reported using at least one strategy at least occasionally, and the likelihood of using a strategy increased with increased gambling involvement. This finding suggests that individuals who gamble more heavily find the concept of self-regulation to be relevant to their gambling decisions. Setting personal frequency and expenditure limits were common and were viewed as helpful in limiting gambling. Another commonly endorsed strategy was to limit alcohol consumption while gambling. Although many people set personal limits, almost half also acknowledged exceeding them. Greater problem gambling severity was associated with less success in adherence. A more concerning finding was that 9% of the nearly 1500 people with gambling problems in the sample did not use any of the quantitative limit strategies.
Together these results aligned with the quantitative limit ranges we derived and supported their applicability and potential value. However, they also underscore a challenge with public health guidelines. Guidelines, by their nature, apply to the typical or average person, but it is also important to identify and communicate modifying factors or clear exceptions that reflect individual and situational variability. For example, for Canada’s drinking guidelines, individuals with a personal or family history of alcohol problems are encouraged to consider drinking less than the recommended limits, and pregnant women are advised to abstain (Butt et al., 2011). To identify similar contextual factors for gambling-related harm, we conducted a meta-analyses of 104 population prevalence studies (to 2019) to identify the consistency and strength of correlates of problem gambling (Allami et al., 2021). The key factors increasing the risk of developing a gambling problem that emerged were gambling type, mental health, and substance use, and whether someone had a family history of gambling problems. Interestingly, the smallest effect sizes were found among demographic variables and no gender differences were detected. The specific correlates with moderate to strong effect sizes formed the basis of the contextual factors that we included in our final guideline recommendations.
Goal of This Paper
The goal of this paper is to present the results of two studies conducted that permitted us to arrive at our final guidelines, and to present our final evidence-based advice and messaging that should be included when communicating lower-risk gambling guidelines to the public.
The results of risk curve analyses described above were ranges of gambling limits (expenditure, frequency, and number of gambling types) associated with increased risk of harm. Having valid and reliable ranges of gambling limits, it was important to determine recommendations for specific values suitable for public health messaging.
To accomplish this, two studies were conducted. First, following a procedure used in the development of lower risk drinking guidelines (Butt et al., 2011; Stockwell et al., 2012), we examined datasets from the eight participating countries that identified ranges of harm changes across a range of quantitative gambling involvement indicators (i.e., expenditure, frequency, and number of gambling types). These descriptive data, along with information gleaned from the other research projects, were used to determine appropriate quantitative guidelines for lower-risk gambling.
The second study sought feedback from Canadians who gamble, through an online survey, about whether they understood proposed quantitative limits, and whether they found them credible and personally relevant. The results of these studies were the final inputs into the recommendation for the lower-risk gambling guidelines.
Study 1: Determining Risk of Harm Across the Range of Possible Gambling Limits
Materials and Methods
Analyses were conducted on an aggregated dataset that included all 11 datasets used to conduct the risk curve analyses (N = 59,099 to 66,873 depending on variables assessed). Detailed descriptions of these datasets and how they were selected are included in Hodgins et al. (submitted). The data were aggregated to ensure sufficient sample sizes for each of the possible values of each gambling indicator. For example, for gambling frequency, 7238 individuals gambled 2 days per month, 10,417 gambled 3 to 4 days, and so forth. The gambling indicators were amount spent per month, percentage of income spent per month, frequency of gambling per month, and number of types of gambling engaged in per year. Relative risk ratios were calculated to describe the increase in risk of harm for each possible value of each indicator, including points above and below the upper and lower limit ranges identified in the risk curve analyses (Hodgins et al., submitted). The reference group (RG) for determining RR was the group of individuals reporting the lowest level of gambling involvement assessed across surveys for that indicator. The use of people who do not gamble as a RG would not be valid because our harm measure, derived from the PGSI (Ferris & Wynne, 2001), only considered harm arising from gambling. Seven of the PGSI items ask about negative consequences from gambling; these items were used as indicators of four harm categories—financial (3 items), emotional (2 items), relationship (1 item), and health harms (1 item). Responses to the items were dichotomized (not at all = 0, sometimes, most of the time, always = 1). Specifically, for gambling expenditure, we constructed two RGs—those spending $10 CAD or less per month and those spending 0.1% or less of gross family income per month. For frequency, the RG was those who gambled one or fewer days per month. For gambling type, it was those gambling on a maximum of one type of gambling per year.
Results and Discussion
Expenditure
We began by assessing the relative risk ratio (RR) of experiencing each gambling-related harm (financial, relationship, emotional and psychological, and health) or whether they reported two or more of the PGSI items assessing these harms compared to the RG as expenditure increases. First, these RRs are described for those spending greater than $10 CAD per month to those spending more than $200 in Table 1 and for those spending > 0.1% of gross family income to those spending more than 5% in Table 2. Among those spending between $11 and $60 per month, the risk of gambling related harm was between 1.7 and 2 times the RG (depending on gambling harm). However, when examining the RRs associated with expenditure of $60 to $90, risk of gambling-related harm increased to 3.6 to 5.1 times from the RG. Other expenditure ranges were associated with RRs greater than 5.8. When examining expenditure as a percentage of monthly gross income, the RRs associated with expenditure of 0.51 to 1.00%, ranged from 2.4 to 3.0 but steeply increased to 3.9 to 4.7 times the RG when expenditure was between 1.1 and 2.0%. Expenditure of more than 2.1% of gross monthly income was associated with RRs greater than 5.0.
Thus, according to this analysis, risk of gambling-related harm more than doubles for all harms assessed if one spends more than $60 CAD per month and increases almost fourfold if one spends more than 1% of gross monthly income.
Frequency
Next, we assessed the relative risk of experiencing gambling-related harms compared to the RG as gambling frequency increases. These RRs are described for those gambling 2 days, 3 to 4 days, 5 to 6 days, 7 to 8 days, and more than 9 days per month in Table 3. Among those gambling 2 days per month, risk of gambling-related harm was between 1.8 and 2.2 times the RG (depending on gambling harm) and 2.7 times the more likely to report 2 or more harms. Among those gambling 3–4 days, increased risk of harm ranged from 2.0 to 2.8 times. However, when examining the RRs associated with gambling 5–6 days, risk of gambling-related harm ranged from 2.1 to 2.5 (3.3 for two or more harms), 7–8 days ranged from 2.9 to 3.7 (5.2 times for two or more harms), and 9 or more days more than 7.2 times.
Gambling Types
Finally, we assessed the relative risk of experiencing gambling-related harms as the number of gambling types people played in the past year increased from two to six or more. RRs compared to the RG (those reporting playing one or fewer types of gambling in the last year) are described in Table 4. RRs among those gambling two types ranged from 1.2 to 1.4 (1.6 for two or more harms). When gambling three types per year, risk doubled (for all harms but health). Playing four types in the last year was associated with almost a tripled increased risk and five, a four-fold increased risk of harm (with the exception of health harms).
Study 2: Credibility and Relevance of Gambling Guidelines
The purpose of Study 2 was to acquire feedback from Canadians who gamble about whether they understood the proposed quantitative limits, and whether they found them credible and personally relevant.
Methods
Two online surveys of Canadians who gamble regularly were conducted with the survey firm Leger360 as part of the Alberta Gambling Research Institute’s National Study on Gambling and Problem Gambling in Canada (Williams et al., 2022). The first was conducted in August 2018 to examine the self-control strategies used by people who gamble regularly and whether such strategies were effective in reducing gambling-related harm. A total of 10,199 people participated in the survey. Results are available in Currie et al. (2019). In August 2019, all those who responded to the first survey were asked to complete a follow-up survey. Forty-six percent of the original sample completed the follow-up survey (n = 4707). After excluding participants who reported no gambling in the past 12 months, the final sample for this analysis consisted of 4583 individuals. Participants were paid $10 CDN to complete the survey in addition to Leger’s standard panel participation incentives (monthly lottery draws for merchandise and points). Demographics of the sample are shown in Table 5.
Survey Instrument
Participants completed an online questionnaire including basic demographic questions, gambling participation, problem gambling (Problem Gambling Severity Index; Ferris & Wynne, 2001), mental health and substance use, general health, and awareness of and opinions on responsible gambling initiatives. Included were a series of questions designed to test comprehension and acceptability of different ways of presenting messages designed to promote lower-risk gambling. To do so, participants were shown two messages and asked a series of questions. One message (Fig. 1) presented lower, more conservative, limits for frequency and expenditure. Specifically, no more than 4 days per month (corresponding to the lower range estimate of 5 days per month) and no more than 1% of gross annual household income (equivalent to $60/month for most Canadians). The other message (Fig. 2) contained identical wording, but higher, more liberal, limits (6 days and 1.5% or approximately $90). Number of gambling types was not initially included as a possible quantitative limit early in the project and therefore was not included in the survey.

Lower-risk gambling message based on lower, more conservative, quantitative limits

Lower-risk gambling message based on higher, more liberal, quantitative limits
Following, participants were asked to rate the messages in terms of either being too conservative or too liberal. First, the participants were asked whether gambling no more than 4 days per month seemed too high, too low, or just right for most people who gamble. Following, they were asked the same question about 6 days per month. Each participant was also asked the same question about gambling more than 1% and 1.5% of household income per month. The order of the presentation of the figures and the questions were randomized across respondents.
Results and Discussion
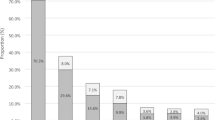
Figure 3 presents the percentage of sample responding to the question: “To reduce the risk of experiencing problems, does the message of gambling no more than 4 days or 6 days per month seem too high, too low or just right for most people who gamble?” (n = 4583). The same question was also asked about and 1% and 1.5% of household income (n = 4583). Overall, participants felt 4 days were a more appropriate cut-off than 6 days. Less than 5% of the sample felt the message was unclear. Figure 3 also presents the results for the different percent of income. Again, the sample indicated they felt the lower limit was more appropriate.

Participant assessment of appropriateness of gambling frequency and percentage of income gambling limits (n = 4583). Data labels represent numbers of particpants
To determine whether respondents’ assessment of the appropriateness of the lower limits versus the upper limits was influenced by their problem gambling severity, we examined their responses by problem gambling category. Specifically Fig. 4 presents the percent of sample (n = 4583) responding to the question: “To reduce the risk of experiencing problems, does the message of gambling no more than (4 or 6) days per month seem too high, too low or just right for most people who gamble?” by problem gambling severity category (no problem or low risk (n = 4072), moderate risk (n = 169), or problem (n = 342)). The chart on the left asks about 4 days and the chart on the right 6 days. When presented with no more than 4 days per month, there was very little difference in response between problem gambling severity categories. However, when presented with no more than six days those reporting gambling-related problems were more likely to indicate that this was an appropriate limit and those at low risk of problems were more likely to report it was too high.

Participant assessment of appropriateness of gambling frequency limits by problem gambling severity (n = 4583). Data labels represent numbers of particpants
As was done for frequency, to determine whether respondents’ assessments of the appropriateness of the lower percent of income limit (i.e., 1%) versus the upper limit (i.e., 1.5%) were influenced by their problem gambling severity, we examined their responses by problem gambling category. Figure 5 presents the percent of the sample (n = 4583) responding to the question: “To reduce the risk of experiencing problems, does the message of gambling no more than (1% or 1.5%) per month seem too high, too low or just right for most people who gamble?” by problem gambling severity category (no problem or low risk (n = 4,072), moderate risk (n = 169), or problem (n = 342)) (Fig. 5). A similar pattern of responses as was observed with frequency emerged. When presented with 1%, similar percentages of respondents indicated that this limit was “just right.” However, when presented with the upper limit (1.5%), the majority of those reporting gambling-related problems indicate that this was an appropriate limit, whereas the majority of those at low risk of problems reported that 1.5% was a little too high.

Note: This data is mandatory. Please provide.
Next, participants were asked which of the two options, if either, would be more effective in helping people reduce their risk of gambling-related harms. Forty-one percent of respondents indicated that they felt that the lower range (4 days and 1%) would be more effective than the upper range (6 days and 1.5%). In contrast, 8% of the sample indicated the upper range, 22% indicated either would effective, and 30% said neither. Finally, respondents were asked which set of guidelines they would be most likely to use personally. Although the largest proportion of respondents (41%) indicated they would be most likely to use the guidelines of 4 days and 1%, an almost equal proportion (39%) of the sample indicated they would use neither set of guidelines. Eleven percent indicated they would use either and 10% indicated they would use 6 days and 1.5%. To better understand this result, we examined the composition of the sample who responded neither to this question (n = 1776). The group who responded they would use neither set of limits was similar to the whole sample in terms of gambling characteristics (mean monthly expenditure = $952; mean gambling days per month = 4.4; proportion of people with moderate risk or problem gambling = 7.8%).
General Discussion
The lower-risk gambling limits for frequency, expenditure, and number of different gambling types played were derived from a large 5-year international collaborative project and first published in 2021 (Young et al., 2021). The present studies were conducted to (1) examine how risk of harm changes across the range of possible limits for gambling frequency, expenditure, and number of types of gambling; and (2) assess how people who regularly gamble would respond to and apply the limits. The findings presented above as well as those conducted as part of the larger program of research (Allami et al., 2021; Currie et al., 2020; Currie & Low Risk Gambling Guidelines Scientific Working, 2019; Flores-Pajot et al., 2021; Hodgins et al., submitted) were overseen by the LRGG Scientific Working Group (LRGG-SWG; authors of this manuscript) to not only provide expert advice, conduct research to support developing the LRGGs, but also formulate guidelines for quantitative limits on frequency, expenditure, and number of different gambling types that are associated with a reduced risk of experiencing the harms related to gambling. To do so, the LRGG-SWG reviewed all the research in detail and adopted a consensus approach to determining the final recommendations described below.
Recommended Quantitative Limits
Frequency and Expenditure
According to relative risk assessments, risk of gambling-related harm more than doubles for all harms assessed if, in a single month, one gambles more than four times or spends more than $60 CAD. Further risk of harm increases almost fourfold if one spends more than 1% of gross monthly income. According to the last Canadian Census, in 2015, the median Canadian household pre-tax income was $70,336 (Statistics Canada, 2016). One percent of $70,000 is equivalent to approximately $60 per month. Therefore, even though increased risk of harm associated with expenditure of more than 1% per month was greater than $60 per month, there is some consistency in the finding. When presented with a higher and a lower set of limits (6 days per month and 1.5% or $90 versus 4 days per month and 1% or $60), survey respondents indicated they felt that the lower limit was more appropriate and would be more effective than the higher limit in helping people lower the risk of gambling-related harm. It is also noteworthy that the optimal monetary and frequency limits emerging from this project were also very similar to the self-imposed limits set by people who gamble regularly. Among those who naturally set quantitative limits, the median spending limit was $69 per month and the median frequency limit was 4 days per month (Currie et al., 2020).
Finally, the simplicity and thus memorability of the messages were also important considerations. In this regard, 4 days a month (or roughly once a week) was easy to understand and remember. In addition, information acquired via focus groups (Flores-Pajot et al., 2021) indicated that, for many, an exact dollar figure would not be credible given the variability of income among Canadians: percentage of household income was preferred. For these reasons, we recommend 1% gross monthly income and 4 days per month. However, percentage household income before tax is challenging to communicate clearly to the general population and challenging for some to calculate. For this reason, focus group participants suggested including a table describing the monthly equivalent of 1% of household income for a variety of different gross income (Flores-Pajot et al., 2021). Included in Table 6 are the final expenditure and frequency recommendations.
Number of Gambling Types
We found that gambling on three game types in the past year resulted in a doubling of risk of harm and gambling on four game types results in almost a tripling of risk for financial and relationship harms and more than a quadrupling of risk for emotional and psychological harms. However, different from frequency, dollar expenditure, and percent of income, we were only able to assess how risk of harm increased based on the number of gambling types played in the past year. Because the other limits are expressed as monthly guidelines and we could not do so for this limit, we decided to recommend that people should not gamble regularly at more than two types of games. In focus groups with people who gamble, Flores-Pajot et al. (2021) found that people sometimes had difficulty understanding what is meant by gambling type. Therefore, it is recommended that examples of types of gambling accompany the guidelines.
Recommended Messages Aimed at Addressing Special Risk Populations
A recent comprehensive meta-analysis of problem gambling risk factors in the general adult population provided the basis for identifying special risk populations (Allami et al., 2021). This review revealed 30 problem gambling correlates that have a medium or strong effect size across a number of studies of community samples. Among these correlates, 16 were associated with the type of gambling activity individuals engaged in, and seven were associated with psychosocial risk factors such as a history of attempted suicide, anxiety issues, or other mental health problems. Six out of the 30 correlates were associated with substance use such as problems due to alcohol, binge drinking, illicit drug use, or daily tobacco use, and one was whether a family member had ever had a gambling problem. Based on these findings, we recommend the messages in Table 6 be included in the final guidelines.
Recommended messages aimed at gambling type
It is well established that some types of gambling are associated with a higher potential for harm than others (Breen & Zimmerman, 2002; Hollingshead et al., 2019; Welte et al., 2004). Allami et al. (2021) found evidence of a large increased risk of problem gambling among people who gamble on the Internet and play electronic gaming machines (EGM) or poker. Notably, because of their speed of play, visual and auditory effects, illusionary control features (e.g., stop buttons, near misses), and payout intervals, EGMs have been identified as higher-risk gambling types. Therefore we recommend including a statement that describes how engaging in some gambling types may make it harder to adhere to the guidelines (Table 6).
When communicating the LRGGs to the public, care should be taken to emphasize that if a person occasionally exceeds the guidelines, this does not necessarily mean the individual has gambling problems or will experience harm. It simply means their risk of experiencing harm is greater than those who gamble below the recommended limits. The present project adapted a relative risk method whereby the probability of experiencing harm is estimated in people who gamble who exceed specific low-risk limits compared to people who gamble below the limits. This approach is well suited for dose–response curves that display a visible change in slope associated with higher levels of consumption. The same pattern is observed with the lower-risk drinking limits. Most people who exceed the drinking limits don’t experience alcohol-related consequences. However, people who exceed the limits are more likely to experience harm than people who stay below the limits. Furthermore, the chances of experiencing harm increases with heavier consumption—a trend we also found. Similar finding was observed in Currie et al. (2021), who applied survival analysis to Canadian longitudinal data and showed that gamblers who exceeded lower-risk gambling limits reported gambling-related harm and met criteria for gambling disorder faster than persons who stayed below the limits.
Limitations
Guidelines Are Not Specific to Gambling Type
Because of the variety of gambling types and the different structural characteristics of each, concern has been raised about constructing aggregate risk curves that collapse multiple game types into a single metric and applying the same lower-risk limits to all gambling types (Abbott, 2017). Unlike alcohol where different drink types can be converted to standard drinks, there is no standard unit of gambling (e.g., 10 min of EGM play as equivalent to 60 min of bingo).
The development of game-specific risk curves and limits is one possible resolution to this limitation. However, gambling type-specific guidelines introduce other problems: (1) most people who regularly gamble engage in multiple forms of gambling; (2) some gambling types are played by too few individuals (e.g., horse betting) to construct robust risk curves for expenditure and frequency of play (sample sizes would be too small to derive reliable limits); (3) types of games available to the public are highly variable across jurisdictions and international borders, which would hinder attempts to consolidate findings from different data sources; and (4) providing different expenditure and frequency limits for different game types would complicate the messaging to people who gamble.
Lotteries are the most prevalent form of gambling in most Western countries. Lotteries and raffle draws are generally considered lower-risk gambling types because they are not as structurally conducive to frequent engagement and higher expenditure than Internet gambling, EGMs, or poker. Currie et al. (2006) conducted a sensitivity analysis to determine the impact on the risk curve and lower-risk limits of removing people who only played lottery games. The risk curve and limits were largely unchanged when lottery players were removed. The most likely explanation for this finding is that individuals who only gamble on low-risk game types would typically fall below the guidelines in terms of frequency and amount spent, resulting in no appreciable impact to the dose–response curves that include the remaining forms of gambling. Certain gambling types are higher risk precisely because the structural characteristics of the game encourage greater gambling involvement. For example, as a continuous form of gambling, someone using an electronic gaming machines is more likely than someone playing a discontinuous form of gambling like the lottery to play more frequently and for longer, and to spend more money. The dose–response curve for gambling indicates that higher levels of gambling involvement lead to more harm, regardless of the game type in which the person who gambles chooses to invest time and money. Furthermore, number of gambling types is a robust and independent predictor of harm. Individuals who gamble on the riskiest types are typically also gambling on less risky forms.
In light of the above information, we concluded that the construction of game-specific risk curves and limits was not warranted and guidelines should be targeted to those engaging in all forms of gambling, including lottery play. Instead, we decided that to include specific messaging to highlight that some gambling types carry a greater risk of harm because their structural characteristics encourage more gambling involvement (Table 6).
Guidelines Focus on Individual Behavior and Do Not Take into Consideration the Gambling Environment
While these guidelines focus on what individuals can do to decrease their risk of gambling-related harms, we recognize that this is an insufficient public health response to the issue of gambling harms. Environmental influences such as gambling availability, accessibility, marketing and promotion, regulation, gambling education, and ensuring that near wins as well as wins appear randomly in electronic gaming machines are also critical to reducing harms related to gambling. Thus, the recommendations presented here are one tool to be used as part of a comprehensive approach to reducing gambling-related harm.
In addition, one should keep in mind that these data were collected from adults. These guidelines do not apply to minors who, by Canadian regulations, cannot gamble legally.
Conclusion
While several countries have developed and promote quantitative guidelines or limits that aim to reduce the amount of alcohol-related harm in their populations (e.g., Australia (National Health & Medical Research Council, 2020), Canada (Butt et al., 2011), the UK (Department of Health, 2016), and France (Santé publique France, 2017)), similar guidelines for gambling have not been developed and promoted. The recommended content presented in the paper is the result of the first large-scale, comprehensive project in the world to develop recommendations for lower-risk gambling. In Canada, we have used the recommended content presented here in a variety of knowledge mobilization products available at www.gambling-guidelines.ca including an infographic presenting all the recommended content on a single page, as well as infographics providing more detail about the harms of gambling, why the type of gambling matters, and the specific risk factors to note when considering whether to use the guidelines. We have also developed a risk assessment tool that allows people to answer key questions about their income, gambling involvement, and risk factors which will present personalized feedback. All products are available in English and in French.
It is hoped that the recommended content presented here will be useful to all those dedicated to reducing the harms related to gambling.
References
Abbott, M. W. (2017). Commentary on currie et al. (2017): Low-risk gambling limits—a bridge too far? Addiction, 112(11), 2021–2022.
Allami, Y., Hodgins, D. C., Young, M., Brunelle, N., Currie, S. R., Dufour, M., Flores-Pajot, M.-C., & Nadeau, L. (2021). A meta-analysis of problem gambling risk factors in the general adult population. Addiction. https://doi.org/10.1111/add.15449
Breen, R. B., & Zimmerman, M. (2002). Rapid onset of pathological gambling in machine gamblers. Journal of Gambling Studies, 18(1), 31–43.
Browne, M., Langham, E., Rawat, V., Greer, N., Li, E., Rose, J., Rockloff, M. Donaldson, P., Thorne, H., Goodwin, B., Bryden, G., & Best, T. (2016). Assessing gambling-related harm in victoria: A public health perspective (V. R. G. Foundation Ed.). Melbourne: Vicotia Responsible Gambling Foundation
Butt, P., Giliksman, L., Paradis, C., & Stockwell, T. (2011). Alcohol and health in canada: A summary of evidence and guidelines for low-risk drinking. Canadian Centre on Substance Abuse.
Currie, S. R., Low Risk Gambling Guidelines Scientific Working G. (2019). A research plan to define Canada’s first low-risk gambling guidelines. Health Promotion International, 34(6), 1207–1217. https://doi.org/10.1093/heapro/day074
Currie, S. R., Hodgins, D. C., Wang, J., El-Guebaly, N., Wynne, H., & Chen, S. (2006). Risk of harm among gamblers in the general population as a function of level of participation in gambling activities. Addiction, 101(4), 570–580. https://doi.org/10.1111/j.1360-0443.2006.01392.x
Currie, S. R., Hodgins, D. C., Wang, J., El-Guebaly, N., & Wynne, H. (2008). In pursuit of empirically based responsible gambling limits. International Gambling Studies, 8(2), 207–227. https://doi.org/10.1080/14459790802172265
Currie, S. R., Hodgins, D. C., Casey, D. M., El-Guebaly, N., Smith, G. J., Williams, R. J., & Schopflocher, D. P. (2017). Deriving low-risk gambling limits from longitudinal data collected in two independent canadian studies. Addiction, 112(11), 2011–2020. https://doi.org/10.1111/add.13909
Currie, S. R., Brunelle, N., Dufour, M., Flores-Pajot, M. C., Hodgins, D., Nadeau, L., & Young, M. (2020). Use of self-control strategies for managing gambling habits leads to less harm in regular gamblers. Journal of Gambling Studies, 36(2), 685–698. https://doi.org/10.1007/s10899-019-09918-0
Currie, S. R., Hodgins, D. C., Williams, R. J., Fiest, K. (2021). Predicting future harm from gambling over a five-year period in a general population sample: A survival analysis. BMC Psychiatry 21(15).
Department of Health [United Kingdom]. (2016). UK Chief Medical Officers’ Low Risk Drinking Guidelines.
Dowling, N., Youssef, G., Greenwood, C., Merkouris, S., Suomi, A., & Room, R. (2018). The development of empirically derived australian responsible gambling limits Retrieved from Victorian Responsible Gambling Foundation:
Ferris, J., & Wynne, H. (2001). The canadian problem gambling index: Final report. Retrieved from: https://www.greo.ca/Modules/EvidenceCentre/files/Ferris%20et%20al(2001)The_Canadian_Problem_Gambling_Index.pdf
Flores-Pajot, M.-C., Atif, S., Dufour, M., Brunelle, N., Currie, S. R., Hodgins, D. C., Nadeau, L., & Young, M. M. (2021). Gambling self-control strategies: A qualitative analysis. International Journal of Environmental Research and Public Health, 18.https://doi.org/10.3390/ijerph18020586
Hodgins, D. C., Young, M. M., Currie, S. R., Abbott, M., Billi, R., Brunelle, N., . . . Nadeau, L. (submitted). Cross national consistency in lower-risk gambling limits: Linked analyses across eight countries. Manuscript submitted for publication.
Hollingshead, S. J., Wohl, M. J. A., & Santesso, D. (2019). Do you read me? Including personalized behavioral feedback in pop-up messages does not enhance limit adherence among gamblers. Computers in Human Behavior, 94(1), 122–130. https://doi.org/10.1016/j.chb.2019.01.015
Holmes, J., Angus, C., Meier, P. S., Buykx, P., & Brennan, A. (2019). Drinking guidelines and the need for evidence beyond the epidemiological. Addiction, 114(4), 607–608. https://doi.org/10.1111/add.14564
Langham, E., Thorne, H., Browne, M., Donaldson, P., Rose, J., & Rockloff, M. (2016). Understanding gambling related harm: A proposed definition, conceptual framework, and taxonomy of harms. BMC Public Health, 16, 80. https://doi.org/10.1186/s12889-016-2747-0
Li, E., Browne, M., Rawat, V., Langham, E., & Rockloff, M. (2017). Breaking bad: Comparing gambling harms among gamblers and affected others. Journal of Gambling Studies, 33(1), 223–248. https://doi.org/10.1007/s10899-016-9632-8
National Health and Medical Research Council. (2020). Australian guidelines to reduce health risks from drinking alcohol. National Health and Medical Research Council. Commonwealth of Australia, Canberra
Santé publique France (2017). Avis d'experts relatif à l'évolution du discours public en matière de consommation d'alcool en France. Institut national du cancer France, Mission interministérielle de lutte contre les drogues et les conduites addictives. Santé publique France, France.
Statistics Canada. (2016). Income highlight tables, 2016 census. Retrieved from: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/hlt-fst/inc-rev/Table.cfm?Lang=Eng&T=102&PR=0&D1=1&RPP=25&SR=1&S=108&O=D
Stockwell, T., Butt, P., Beirness, D., Gliksman, L., & Paradis, C. (2012). The basis for canada’s new low-risk drinking guidelines: A relative risk approach to estimating hazardous levels and patterns of alcohol use. Drug and Alcohol Review, 31(2), 126–134. https://doi.org/10.1111/j.1465-3362.2011.00342.x
Welte, J. W., Wieczorek, W., Tidwell, M. C., & Parker, J. C. (2004). Risk factors for pathological gambling. Addictive Behaviors, 29, 323–335.
Williams, R. J., Belanger, Y. D., Christensen, D. R., el-Guebaly, N. A., Hodgins, D. C., McGrath, D. S., Nicoll, F., Smith, G. J., & Stevens, R. J. (2022). National gambling study. Available at https://research.ucalgary.ca/alberta-gambling-research-institute/research/national-gambling-study
Young, M. M., Hodgins, D. C., Brunelle, N., Currie, S., Dufour, M., Flores-Pajot, M.-C., Paradis, C., & Nadeau, L. (2021). Developing lower-risk gambling guidelines. Retrieved from Canadian Centre on Substance Use and Addiction,: https://gamblingguidelines.ca/resource/developing-lower-risk-gambling-guidelines-report/
Funding
Funding for the project came from the Mise sur toi (MST) Foundation. MST was created in 2002 as an independent, private, and non-profit organization whose mission was to develop a Responsible Gambling (RG) culture in Quebec. When Loto-Québec decided to operate RG programming internally in 2012, MST ceased to exist. However, before it could be dissolved or reorganized, the corporate entity MST was left with assets that had to be distributed. The MST Board of Directors chose, among other decisions, to support the development of lower risk gambling guidelines, akin to those developed for alcohol. The funder had no role in study design, data analysis, data interpretation, or the writing of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). Informed consent was obtained from all participants for being included in the study.
Conflict of Interest
Matthew M. Young declares that he has no conflict of interest. David C. Hodgins declares that he has no conflict of interest. Shawn R. Currie declares that he has no conflict of interest. Natacha Brunelle declares that she has no conflict of interest. Magali Dufour declares that she has no conflict of interest. In May 2021, when research for the project had been completed, Flores-Pajot accepted a position at the Massachusetts Gaming Commission and ceased working on this project. Louise Nadeau declares that she has no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Young, M.M., Hodgins, D.C., Currie, S.R. et al. Not Too Much, Not Too Often, and Not Too Many: the Results of the First Large-Scale, International Project to Develop Lower-Risk Gambling Guidelines. Int J Ment Health Addiction 22, 666–684 (2024). https://doi.org/10.1007/s11469-022-00896-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-022-00896-w