
Abstract
While comorbidity of problematic alcohol and gambling use is well established, much less is known about the way in which alcohol consumption while gambling interacts with problem-gambling severity and other individual differences. We hypothesised three factors that would interact with alcohol consumption while gambling on electronic gaming machines (EGMs) to influence four behavioural gambling measures: preferred number of lines bet, average duration of play, average spend per session and preferred electronic gaming machine denomination. The latter is a measure of gambler’s preference for the monetary denomination in which EGM bets are placed (e.g. 1 cent, 2 cents, 5 cents, 10 cents, 20 cents, $1), with higher denomination EGMs being higher risk since bets can be placed in larger amounts and money can be lost more rapidly. The three hypothesised interacting factors were problem-gambling severity, presence/absence of alcohol use disorder and biological gender. A total of 1557 male and female participants completed a questionnaire, measuring their problem-gambling status, problem alcohol status, consumption of alcohol at the gambling venue, preferred EGM denomination, preferred number of lines bet, average duration of play and average spend per session. We found the anticipated gender-differential spending effect with males spending more than females, but we also found a surprising reverse differential spending effect for problem gamblers such that females spent more than males. We also found that alcohol consumption while gambling was generally associated with a preference for higher denomination machines and that those players without alcohol problems who drank at the venue preferred to bet on more lines, suggesting a double-max strategy amongst gamblers who drank at the venue. Finally, for non-problem and low-risk gamblers, concurrent alcohol consumption was related to preference for higher denomination EGMs in female players, but not for male players. These findings are discussed in the context of the physiological and psychological effects of alcohol.
Similar content being viewed by others

The extent to which alcohol consumption might influence gambling behaviours is poorly understood (Bussu & Detotto, 2015), and few studies have examined the effects of alcohol consumption on gambling amongst non-problematic alcohol drinkers (Harries et al., 2017; Pino-Gutierrez et al., 2017). However, from a theoretical perspective, we predict an impact of alcohol consumption on gambling behaviour since there is clear evidence that alcohol intake leads to an increase in risk-taking and impairs judgement/decision making (Chesher & Greeley, 1989; Fillmore, 2007), including judgements of time that can be affected by even very small levels of alcohol (Hernández-Collados et al., 1997; Ogden et al., 2011). Thus far, researchers have investigated the effects of alcohol consumption on gambling duration, bet size and expenditure with mixed results.
Physiological and Cognitive Effects of Alcohol
In predicting the effects of alcohol on gambling behaviour, there are several important physiological and cognitive effects to consider and these are the general effect, the effects of biological sex and the effects of long-term abuse. First, even at low levels of blood concentration (0.048% BAC), alcohol has been shown to impair cognitive function on tasks requiring attentional inhibition, working memory, speed of processing (Dry et al., 2012) and reaction time (Kerr & Hindmarch, 1998). From a psychophysiological perspective, alcohol causes an increase in concentrations of the neurotransmitter norepinephrine. Because of its widespread distribution of cortical projections, norepinephrine modulates many sensory and cognitive cortical regions, including the regulation of memory function in the hippocampus and motivation/emotion in the forebrain, leading to an increase in impulsiveness (Vazey et al., 2018). Norepinephrine is also associated with executive functions, including behavioural flexibility and response inhibition (see Robbins & Arnsten, 2009, for a review). Small amounts of alcohol can activate the inhibitory GABA-A receptors, concentrations of which are found in the prefrontal and temporal cortices and cerebellum. Decreased activity in these areas can lead to loss of inhibition, loss of long-term memory and loss of coordinated motor function (see Olsen et al., 2007, for a review). But there are important sex differences in effects of alcohol, so for the same alcohol intake, females develop higher levels of blood alcohol concentration than males, possibly due to less efficient basal gastric metabolism in females (Baraona et al., 2001), and even small doses of alcohol (below 0.5 g/kg) have been shown to impair cognitive skills and manual performance in females to a greater extent than in males (e.g. Banks et al., 2004; Miller et al., 2009; see Erol & Karpyaka, 2015, for an overview of biological gender differences with alcohol). The last consideration is that of long-term abuse since chronic alcohol use disorder can lead to lasting cognitive impairments, particularly in executive functions and visuospatial abilities (Cermak, 1990; Koob, 1997; Sullivan et al., 2000), and it is important to note that these impairments can extend beyond detoxification (Dick et al., 2010).
General Effects of Alcohol Consumption on Gambling Behaviour
From the broad review above, we would expect alcohol consumption to be associated with increases in impulsiveness (Vazey et al., 2018) and risk-taking in a gambling context and this has found support from studies by Phillips and Ogeil (2007). Distortion of emotion (Vazey et al., 2018) and impairment in working memory (Dry et al., 2012) are also likely to determine the extent to which a player evaluates losses, both emotionally and financially, and we would expect to find specific gambling behaviour effects such as higher bet size. Again, there is some evidence of this, though thus far the findings have been mixed. For example in their laboratory study, Cronce and Corbin (2010) reported that participants in their alcohol condition made significantly larger bets than a placebo group, a result also reported in an earlier laboratory study by Ellery et al. (2005). Similarly, Sévigny et al. (2016) reported circumstantial evidence that those drinking moderate amounts of alcohol in the venue spent more money per hour on gambling than those who did not drink alcohol. Although Sévigny et al.’s finding was confounded by the size of the venue, Baron and Dickerson (1999) also reported a significant positive correlation between the amount of alcohol consumed and size of the initial stake. In contrast to these findings, Bussu and Detotto (2015) found no association between the consumption of alcohol in venue and the bet size amongst a sample of gamblers that included electronic gaming machine (EGM) players; however, the bet size of those gambling with concurrent consumption of alcohol, nicotine and illicit drugs was significantly higher than that of those who abstained.
Considering the potential effects that alcohol can have in overriding cues to quit by diminishing capacity for attentional inhibition, working memory (Dry et al., 2012), perception of time (Hernández-Collados et al., 1997; Ogden et al., 2011), behavioural flexibility and response inhibition (Robbins & Arnsten, 2009), the combined effect is likely to lead to increased length of play, compounded by a decrease in reaction time (Kerr & Hindmarch, 1998). In support of this hypothesis, several laboratory-based studies, using precisely administered doses of alcohol, have shown such a positive correlation with time spent on EGMs (Ellery et al., 2005; Giacopassi et al., 1998; Kyngdon & Dickerson, 1999), although in contrast, Stewart et al. (2002) found no correlation between play duration and alcohol consumption in their laboratory study. As useful as they are, laboratory studies may be sensitive to unintended participant strategies. For example, Cronce and Corbin (2010) also reported a null effect of administered alcohol on participants’ duration of laboratory-simulated EGM play. However, their participants were told that they could convert their unused credits into cash at any point in the experiment, highlighting a difficulty in non-naturalistic studies insofar as participants may have correctly anticipated that the simulation was programmed to take all their credits through a methodically implemented progressive loss schedule over the experimental period. In the first large-scale ethnographic survey of alcohol consumption and gambling, Markham et al. (2012) reported that moderate alcohol consumption (between 1 and 4 standard units) was negatively, rather than positively, associated with EGM gambling duration when compared with zero alcohol consumption and this negative correlation was particularly strong with problem gamblers (see similar findings from Baron & Dickerson, 1999). Although Markham et al.’s findings are counterintuitive and in the opposite direction to the one we predict on the basis of what we know about the effects of alcohol on cognitive processing, the findings of all these studies highlight the importance of not treating gamblers as a homogeneous group when looking at effects of alcohol. In jurisdictions such as Australia, where this study was conducted, the level of direct cognitive involvement in EGM play is minimal, and therefore, reaction time would make a small effect on the time spent playing each game, although there is an increasing trend for games that combine random play of traditional EGMs with elements of low-level skills such as hand–eye coordination and reaction time that effectively act as a multiplier for any wins associated with random play (c.f. Skill Based Games Inc.’s GotSkill games) and might have also have a minor impact on winnings (Delfabbro & Gainsbury, 2020).
Alcohol Use Disorder and Gambling
So far, we have discussed the potential and reported effects of concurrent alcohol consumption on occasional gambling, but heavy alcohol consumption is also a known risk factor for problem-gambling (Ellery & Stewart, 2014; Smart & Ferris, 1996) and there is a high co-occurrence of gambling and alcohol problems (Barnes et al., 2015; Harries et al., 2017; Harvanko et al., 2012; Hing et al., 2016; Shen et al., 2015). Petry et al. (2005) found the prevalence of alcohol use disorder amongst problem gamblers to be as high as 73.2% (see Park et al., 2010; Shek et al., 2012, for similar findings), although the strength of this correlation varies widely according to the type of gambling and the type of venue (Gainsbury et al., 2012; Sévigny et al., 2016). A meta-analysis reported by Lorains et al. (2011) identified a mean prevalence of 28.1% comorbidity of alcohol use disorder (unaccompanied by other substance disorders) and pathological gambling. Although the level of alcohol disorder amongst problem gamblers is far higher than the population norm, these findings nevertheless indicate that most problem gamblers do not have an alcohol use disorder. Given the evidence of lasting cognitive impairments in executive and visuospatial functions that extend beyond detoxification (Cermak, 1990; Dick et al., 2010; Koob, 1997; Sullivan et al., 2000), we predict that pre-existing alcohol-related impairments will mean those with alcohol problems will already be exhibiting high-risk-taking behaviours and will therefore be less susceptible to temporary cognitive deficits normally associated with concurrent drinking.
Taken together, when EGM players consume alcohol in a naturalistic setting, they are likely to spend more money but play for less time than those abstaining. The latter part of this hypothesis is supported by Leino et al. (2017) in a study of players in Norwegian state gambling venues where there is a legally imposed daily gambling limit. In one of the few studies to compare EGM gambling in venues that do and do not serve alcohol, they found that of the players who quit before reaching their gambling limit, players in venues where alcohol was served did indeed play for less time and lost more money than when playing in non-alcohol serving venues; however, they also bet less money than when in the non-alcohol serving venues. Here, it is important to distinguish between gross and net expenditures during an EGM session. While gross expenditure may be low, it is still possible for players to walk away with a greater net loss than those with a higher gross expenditure, and vice versa. Whether these differences were directly related to the availability of alcohol is uncertain since availability does not necessarily equate to consumption and there was no record of those who did or did not consume alcohol in the venue. However, in explaining the results of their study, Leino et al. (2017) suggest this may have been due to greater risk-taking when gambling in alcohol serving venues.
Biological Gender, Alcohol Use and Gambling
Another factor known to influence gambling behaviour is biological gender. Female gamblers are generally more risk averse than male gamblers (Wong et al., 2013), and this may in part be because females are more likely to use gambling as a means of escape from mentally or emotionally challenging situations and mood states (Sacco et al., 2011; Strong & Kahler, 2007; Wenzel & Dahl, 2009) whereas males are driven more by gambling urges and an overestimation of their ability to control the outcome (Smith et al., 2015; Wenzel & Dahl, 2009). In general terms, men spend more money and more time on gambling than women (Delfabbro, 2012; Hing & Breen, 2001), and although non-problem gamblers of both sexes prefer to play low-stake (one cent) EGMs, at-risk and problem-gambling males are significantly more likely to bet on more than one credit line than at-risk or problem-gambling females (Delfabbro, 2012; Hing et al., 2016). Given the higher levels of alcohol-related cognitive impairment for the equivalent dose in females than males (Erol & Karpyaka, 2015), we would expect to find greater effects in females than males.
Given the common availability of alcohol in gambling venues, such as hotels, clubs and casinos, and given that both alcohol and biological gender have previously been demonstrated to have an influence on gambling behaviour in terms of duration and bet size, we were interested to explore these factors in more detail. Indeed, in acknowledging the baseline differences between male and female risk-taking behaviour discussed above, and given that alcohol is known to increase risk-taking behaviour (Chesher & Greeley, 1989; Fillmore, 2007), we expected to find a complex pattern of interaction between alcohol consumption and biological gender. To contain the number of variables, and given the different behavioural patterns associated with different forms of gambling, we restricted the scope of this paper to EGMs. In this study, we surveyed the gambling behaviour of a large sample that could be subdivided according to biological gender, use of alcohol during game play, problem alcohol use, problem-gambling status and playing EGMs in a gaming venue when either consuming or not consuming alcohol. We wished to test three specific hypotheses. Despite previously inconsistent empirical findings, the first hypothesis was that those drinking alcohol at the venue would prefer to spend more time gambling, prefer higher denomination machines, prefer to bet on more lines (a behaviour that will lead to more rapid financial loss) and spend more overall (net expense) than those not drinking alcohol. This hypothesis was based on several physiological and neurological effects of alcohol discussed earlier, including a reduction in cognitive processing speed, reduction in reaction time, lowering of response inhibition, reduction in behavioural flexibility and increase in impulsivity.
Our second hypothesis was based on the understanding that alcohol misuse can lead to long-term cognitive deficits that mirror the short-term impairments experienced during alcohol intoxication (Hayes et al., 2016). On this basis, we predicted that the cognitive deficits from concurrent alcohol consumption described above would be apparent only in non-problem drinkers. Those with alcohol problems would likely already be experiencing chronic cognitive deficits, and therefore, we would not expect much additional effect from concurrent alcohol consumption. Specifically, we predicted that when consuming alcohol at the venue, those without alcohol problems who usually consumed alcohol at the venue would prefer to bet more lines on higher denomination machines and spend more time/money than those who did not consume alcohol. For those with alcohol problems, we predicted that the consumption of alcohol would have no effect on these dependent variables since these gamblers would be more likely to take high financial risks, regardless of alcohol intake.
Our third hypothesis was that, given the differences in male and female metabolism of alcohol, there would be an interaction between alcohol consumption, problem-gambling status and biological gender for a preferred number of lines bet, preferred machine denomination, expenditure and duration. Although females are generally more risk averse than males, we know that problem gamblers are more risk-tolerant than non-problem gamblers and that alcohol, as discussed earlier, increases risk-taking behaviour. Without alcohol consumption, low-risk or non-problem-gambling females without alcohol problems would minimise their risk with a preference for lower denomination EGMs, fewer lines and spending less time and money gambling than low-risk or non-problem-gambling males without alcohol problems. However, since alcohol has a greater effect on females than on males, we predicted that concurrent alcohol consumption would eliminate biological gender differences for these same dependent variables. Since problem gamblers are—necessarily—risk-takers and cognitive deficits in problem drinkers also make them high-risk takers, we predicted no biological gender differences for non-alcohol-problematic players, either in those consuming or not consuming alcohol.
Method
Recruitment and Sampling
Having received approval from Southern Cross University Human Research Ethics Committee, with reciprocal approval from Central Queensland University, panel aggregator Qualtrics contacted members of several online research panels with a request to take part in an online survey. Following informed consent, respondents completed a series of screening questions and Australian residents over 18 years old who played EGMs on an at least a monthly basis over the preceding 12 months were permitted to continue.
Of the 11,893 respondents who initiated the survey, 7870 were screened out due to not playing EGMs on a monthly basis, 23 were screened out for being under 18 and nine were screened out because they were not located in Australia. A further 142 were not invited to continue with the survey because age and gender quotas had been applied in order to ensure a mix of ages and genders in the final sample.
The survey also included data quality checks, including two attention checks (1698 discontinued for failing to pay attention), and a speed limit (based on the \({~}^{1}\!\left/ \!{~}_{3}\right.\) median response time of a small pilot study, 133 were discontinued). Of the remaining 2018, a further 448 were excluded on the basis of incomplete data (failure to complete the Problem Gambling Severity Index (PGSI) scale; Ferris & Wynne, 2001), leaving 1570 included in the subsequent analyses (919 males, 651 females). Participant’s ages ranged from 18 to 99 (mean age = 42.3, SD = 16.6).
Measures and Procedure
In choosing a survey design, we aimed to offset any loss of fine-grained control over the variables with the natural averaging produced by retrospective self-report. All participants completed an online questionnaire, hosted on the Qualtrics online survey platform. Having indicated their age and biological gender, participants were presented with the PGSI (Ferris & Wynne, 2001). The PGSI consists of nine items, each rated on a 4-point scale from 0 = never to 3 = almost always. Five items assessed the negative consequences of gambling, for example How often have you felt you might have a problem with gambling?, while four of the items assessed problem-gambling behaviours, for example How often have you bet more than you could afford to lose? Using the categories recommended by Ferris and Wynne (2001), respondents were put into four groups based on the sum of their scores across the nine items: non-problem gamblers (0 points), low-risk gamblers (1 to 2 points), moderate-risk gamblers (3 to 7 points) and problem gamblers (8 to 27 points). Alcohol use disorders were assessed using CAGE (Cut down, Annoyed, Guilty, and Eye-opener; Ewing, 1984) which appraises four aspects of potential alcohol problems by asking the question Have you ever; felt the need to cut down your drinking; felt annoyed by criticism of your drinking; had guilty feelings about drinking; taken a morning eye opener? Each item was scored as either yes = 1 or no = 0. CAGE is a clinical screening method that has been validated in both clinical and general populations (Chan et al., 1994). Although a score of ≥ 2 is considered to be clinically significant (Ewing, 1984), we elected to use the more sensitive scoring method of a score ≥ 1, which retains a high level of specificity (85%) and sensitivity (89%) in predicting those with alcohol problems (Bush et al., 1987) and is commonly used for research purposes (Imperatori et al., 2020), although there is some evidence that this scoring may overestimate high alcohol consumption levels in a general population. However, in anticipating our results, we found that our participants scored either 0 or > 1 on the CAGE. Finally, alcohol use while gambling was assessed by a single question, where respondents indicated whether they usually drank one or more alcoholic beverages while gambling at their favourite EGM venue (yes or no).
The first of the dependent variables, expenditure, was a free response item in which participants estimated their recent average within-session spending (net expense) on EGMs, not counting recycling of winnings. Both median and modal spend were $50; however, the distribution of this variable was skewed due to 14 extreme values of $1000 or more that were removed in order to normalise the distribution, leaving a total of 1557 participants. Denomination of the player’s preferred (most played) EGM was assessed with the following response options: 1c, 2c, 5c, 10c, 20c, 25c, $1 and $2 or more, although respondents also had the option to select other and provide their own answer. Answers in the other category were subsequently re-coded, and a 50c category was added. Mode and median preferred denomination were both 1c. The number of lines typically played per spin on the participant’s favourite machine was recorded using the following response options: 1, 2, 5, 10, 20, 25 and more than 25 lines, with respondents being able to select other and provide their own answer. Most respondents who selected other said “maximum number of lines” and were reclassified into the more than 25 lines category. The modal number of lines bet was 25, whereas the median number of lines bet was 10. In describing the usual length of a session, participants could select from the following: 1–5 min, 6–15 min, 16–30 min, 31–59 min, 1–2 h, 2–3 h, 3–5 h or 5 h or more. Modal length of play was 16–30 min, and median was 31–59 min.
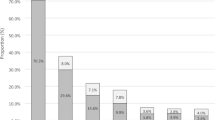
Fewer participants (n = 645) reported that they usually drank alcohol at the venue than those who usually abstained (n = 925) although with our sensitive scoring of CAGE there were only slightly fewer participants with alcohol problems (n = 756) than those without (n = 814). PGSI scores were skewed towards the problem-gambler category (n = 625) which represented approximately 40% of the sample, and fewest were represented in the low-risk category (n = 234) which represented less than 15% of the sample. The number of moderate-risk gamblers (n = 310) represented almost 20% of the sample, but was slightly lower than the number of non-problem gamblers (n = 401) which represented approximately 25% of the sample. Figs. 1, 2 and 3 present the frequency distributions of these variables. Panel samples are known to have higher rates of gambling problems compared to the general population (Russell et al., 2021).

Contingency table for the number of participants drinking or not drinking at the venue, with or without alcohol problems

Frequency of participant preferred EGM denomination

Frequency of participant preferred number of lines bet
Statistical Analysis
As a first step, we wished to investigate the degree to which our population samples overlapped. In particular, we wanted to know the degree to which players with alcohol problems were also those who drank alcohol at the venue. To do this, we performed a 2 × 2 chi-square with alcohol at the venue (yes/no) and alcohol problems (yes/no). There was no significant overlap between the groups, \({X}^{2}\) (1, n = 1557) = 0.01, p = 0.93. As can be seen from the contingency table in Fig. 4, the groups were fairly evenly distributed.

Frequency of participant preferred number of lines bet
The data were entered in a multivariate analysis of variance (MANOVA) with participant biological gender (male vs female), drink-at-venue (yes vs no), alcohol problems (yes vs no) and PGSI group as the independent variables. The four dependent variables were preferred EGM denomination (ranging from 1c to $2 or higher), the usual number of lines bet (ranging from 1 to more than 25), the typical length of play (ranging from 1–5 min to more than 5 h) and the average amount spent per session (free response in Australian dollars). The first three dependent variables had non-continuous ordinal values and while this does not pose a problem for our research question, the data are necessarily non-parametric. In order to test our hypotheses, we required the flexibility of parametric tests to identify both main effects and interactions and so, following Conover and Iman (1981), we analysed rank-transformed data for the non-parametric dependent variables. Therefore, we report mean ranks, rather than median values, where appropriate.
Results
Biological Gender, CAGE and PGSI
Since all our hypotheses involved the concurrent consumption of alcohol and gambling, we made no predictions about the main effects for biological gender, alcohol problems (CAGE) or gambling problems (PGSI), though we found a significant effect of PGSI on average spend, such that there was an increase in average expenditure from AUD39.76 for PGSI1 players to AUD133.31 for PGSI players (F(1, 1525) = 45.99, p = 0.00), and a marginal main effect of CAGE for preferred machine denomination which increased as the level of gambling problem increased (F(1, 1525) = 3.24, p = 0.07), and there were no other main effects for these independent variables. There was, however, a significant interaction between PGSI and biological gender for average expenditure (F(3, 1525) = 5.06, p = 0.00). Figure 5 suggests that the generally higher level of spending for male players was consistent for all but problem gamblers, for whom the gender difference was reversed. This was confirmed by a post hoc t-test showing that female problem gamblers spent significantly more (mean expenditure = $169.36) in an average EGM session than male problem gamblers (mean expenditure = $109.70) (t(612) = 4.97, p = 0.00 (two tailed)).

Participants’ estimated average spend per EGM according to biological gender and PGSI rank. Error bars show standard error. *Significance p = .000
Drinking Alcohol at the Venue
Our first hypothesis was that those who usually drank alcohol at the venue would spend more time and money gambling and prefer to bet on more lines using higher denomination machines than those who did not usually drink alcohol at the venue. In partial support of this hypothesis, we found a significant difference in preferred machine denomination such that those who usually drank alcohol at the venue preferred higher denomination machines (mean rank denomination = 826) than those who did not (mean rank denomination = 742) (F(1, 1525) = 9.06, p = 0.00). However, drinking alcohol at the venue did not independently affect any other dependent variable.
Alcohol by CAGE Interaction
In partial support of our second hypothesis, there were numerical differences in terms of the number of lines bet for payers with and without alcohol problems who either drank alcohol at the venue or did not. Players without alcohol problems who usually drank alcohol at the venue bet on more lines (mean rank = 804) than those who did not usually drink alcohol at the venue (mean rank lines = 748). For those with alcohol problems, players who usually drank alcohol at the venue bet on fewer lines (mean rank = 767) than those who did not usually drink alcohol at the venue (mean rank lines = 823) (see Fig. 6). Although the predicted Alcohol × CAGE interaction did not reach a conventional level of significance (F(1, 1525) = 3.57, p = 0.06), we continued to explore this interaction given that more power is needed to detect a significant interaction than a main effect, and that our a priori hypothesis had led us to predict that those without alcohol problems would bet on more lines when drinking alcohol than those not drinking alcohol, whereas drinking alcohol at the venue would make no difference to those with pre-existing alcohol problems.

Mean rank score of the number of preferred lines bet by EGM players who usually drink at the venue and those who do not, subdivided into those with alcohol problems (CAGE) and those without alcohol problems (no CAGE). Error bars show standard error
This was supported by a planned t-test confirming that of the players without alcohol problems, those who usually consumed alcohol at the venue bet significantly more lines than those who did not usually drink (t(808) = 1.72, p = 0.04 (1 tailed)). The numerical difference for players with alcohol problems between those who usually drank at the venue and those who did not was marginally significant (t(745) = 1.53, p = 0.06 (1 tailed)), though in the opposite direction as seen in Fig. 6. An alternative account of the interaction, still in line with our hypothesis, is that those with alcohol problems who did not drink at the venue behaved like high-risk gamblers compared to those without alcohol problems, whereas the number of lines bet for those drinking at the venue was unaffected by pre-existing alcohol problems. This pattern was also supported with t-tests showing that for non-drinkers, those with alcohol problems bet on significantly more lines than those without alcohol problems (t(634) = 2.10, p = 0.02 (1 tailed)). For those that drank at the venue, there was no significant difference in the number of lines bet for those with and without alcohol problems (t(674) = 1.06, p = 0.15 (1 tailed)). There was no indication of an interaction for the other three dependent variables (DVs).
Biological Gender by Alcohol by PGSI Interaction
In partial support of our third hypothesis, there were significant 3-way interactions between biological gender, alcohol consumption at the venue and PGSI score for preferred bet denomination (F(3, 1525) = 4.11, p < 0.01) and for average spend (F(3, 1525) = 3.251, p = 0.02). As predicted, for those who usually did not consume alcohol at the venue, non-problem and low-risk male gamblers preferred higher denomination machines (mean rank = 863.56 and mean rank = 805.91, respectively) than non-problem and low-risk female gamblers (mean rank = 689.69 and mean rank = 696.97, respectively). However, for those who usually consumed alcohol at the venue, the preferred machine denominations of female non-problem and low-risk gamblers (mean rank = 901.18 and mean rank = 831.94, respectively) were similar to those for non-problem and low-risk male gamblers (mean rank = 801.87 and mean rank = 809.03, respectively). The pattern was reversed for at-risk and problem gamblers such that for those who usually did not consume alcohol at the venue, male at-risk and problem gamblers preferred lower denomination machines (mean rank = 598.25 and mean rank = 721.37, respectively) than female at-risk and problem gamblers (mean rank = 789.19 and mean rank = 767.57, respectively). However, for those who usually consumed alcohol at the venue, the preferred machine denominations of female at-risk and problem gamblers (mean rank = 789.91 and mean rank = 811.84, respectively) were lower than those for male at-risk and problem gamblers (mean rank = 841.65 and mean rank = 819.73, respectively).
Since none of the simple two-way interactions was significant, we went on to directly test our hypothesis by first selecting only non-problem and low-risk gamblers (collapsed) and conducted two planned orthogonal t-tests. The first test confirmed that for those who did not usually consume alcohol at the venue, males preferred higher denomination machines than females (t(210) = 2.07, p = 0.02 (1 tailed)). The second test confirmed that for those who usually consumed alcohol at the venue, males and females had similar machine denomination preferences (t(421) = 1.39, p = 0.08 (1 tailed)). We then took the same approach by collapsing the at-risk and problem gamblers and conducted two further planned orthogonal t-tests; however, the differences in preferred machine denomination between high-risk/problem gambler males and females, either drinking or not drinking, were not significant (t(497) = 0.27, p = 0.18 (1 tailed), and t(422) = 1.01, p = 0.40 (1 tailed), respectively). For the significant interaction with average spend as the DV, there was a somewhat different pattern such that drinking at the venue and gender had little effect for no-risk, low-risk and at-risk players, but female problem gamblers who did not drink at the venue spent far more on an average session ($212.94) than any other group of problem-gambling participants, as clearly seen in Figs. 7 and 8.

Mean rank score of the number of preferred EGM denomination for male and female players in each of the 4 PGSI categories, subdivided into those who usually drink alcohol at the venue (DAV) and those who do not drink alcohol at the venue (NDAV). Error bars show standard error

Participant estimated average expenditure (AUD) for male and female players in each of the 4 PGSI categories, subdivided into those who usually drink alcohol at the venue (DAV) and those who do not drink alcohol at the venue (NDAV). Error bars show Standard Error
Discussion
While the positive correlation between problematic alcohol consumption and problematic gambling behaviour has been well established in the literature (Barnes et al., 2015; Harries et al., 2017; Harvanko et al., 2012; Hing et al., 2016; Shen et al., 2015), little has been established about the factors that might potentially interact with alcohol consumption while gambling, such as alcohol dependency/abuse, biological gender and gambling risk (Bussu & Detotto, 2015). In summarising our significant findings, players who usually drank alcohol while gambling at a venue preferred higher denomination machines than those not usually drinking. Players without alcohol problems who consumed alcohol at the venue preferred to bet on more lines than their peers who did not drink alcohol at the venue. However, since players with alcohol problems already bet on a high number of lines when not drinking alcohol, drinking alcohol at the venue made no difference to the number of lines bet for this group. When we examined only non-problem and low-risk gamblers who did not usually drink at the venue, we found that whereas male gamblers preferred to bet on higher denomination EGMs than female gamblers, there was no difference in machine denomination preference between males and females who drank alcohol at the venue, suggesting that drinking at the venue is more likely to increase risk-taking in females. Although the pattern of numerical differences for at-risk and problem gamblers was opposite to that for non-problem and low-risk gamblers, these differences were not statistically significant. In contradiction to our hypothesis, we found that problem-gambling females who did not drink at the venue spent more in an average EGM session than any other group, including male and female problem gamblers who drank at the venue. Finally, although we had made no prior hypothesis about the observed interaction between PGSI and biological gender, examination of Fig. 5 suggests that while male gamblers generally spent more on EGMs than female gamblers, this biological gender difference was reversed for problem gamblers (PGSI 4). This reverse-differential spending effect was both interesting and unexpected and warrants further investigation.
From a physiological perspective, we know that alcohol binds to GABA-A neurotransmitter receptors, leading to a depressive effect on the central nervous system and subsequent slowing of reaction times. From this, we had hypothesised that we might find an increase in average length of play amongst those who usually consumed alcohol while gambling at a venue, though previous findings had been ambiguous, with some studies showing an effect (Baron & Dickerson, 1999; Ellery et al., 2005; Giacopassi et al., 1998; Kyngdon & Dickerson, 1999; Markham et al., 2012) and others, like ours, showing no effect on duration of play (Cronce & Corbin, 2010; Stewart et al., 2002). Together, these findings suggest that factors other than alcohol alone are determinants in the decision of a player to end a session, e.g. hunger, boredom threshold, wins or losses (Rockloff et al., 2019). However, since we employed a survey methodology, asking about general alcohol consumption habits at venues, we cannot rule out a dose-based effect that would be more accurately determined by a laboratory study (e.g. Dry et al., 2012) or an in-venue observation study focusing on a single gambling session. Indeed, studies showing a positive correlation between alcohol consumption and play duration have been largely laboratory based. It is therefore interesting to note that the negative association between alcohol consumption and EGM gambling duration reported by Markham et al. (2012) was strongest with problem gamblers, indicating that alcohol may differentially affect gambling amongst different types of gamblers. As we have shown in our interaction between PGSI, alcohol and biological gender, different types of gamblers are differentially affected by alcohol consumption such that there was a greater preference for higher denomination machines amongst non-drinking, non-problem and low-risk males than amongst non-drinking, non-problem and low-risk females. This biological gender difference was eliminated amongst equivalent groups of participants that usually drank alcohol while gambling at the venue.
In contrast to the findings of Leino et al. (2017), those who usually drank alcohol at the venue in our study did not differ in average spend per session; however, they bet on higher denomination machines than non-drinkers. This is consistent with findings from both laboratory (Cronce & Corbin, 2010; Ellery et al., 2005) and field (Baron & Dickerson, 1999; Sévigny et al., 2016) studies and may represent an alcohol-induced increase in risk-taking behaviour (Chesher & Greeley, 1989; Fillmore, 2007), although Bussu and Detotto (2015) reported an increase in bet size only when alcohol was consumed concurrently with nicotine and illicit drugs. We had no measure of either smoking or illicit drug consumption, but there is much evidence to show a positive correlation between the consumption of alcohol, nicotine and illicit drugs (e.g. Kendler et al., 2008), and we might therefore assume that at least some of our sample also consumed cigarettes and illicit drugs. Although we are not able to make any claims about causality, we do nevertheless suggest it is important to take some measure of smoking and commonly used illicit drugs in any future investigation of preferred EGM denomination or bet size.
Our finding that those who drank alcohol at the venue preferred higher-denomination EGMs than those who did not drink alcohol at the venue makes an interesting contrast with the often used mini-max strategy whereby experienced EGM players place minimum bets on the maximum number of credit lines (Harrigan et al., 2011; Walker, 2001; Williamson & Walker, 2001). Indeed, Williamson and Walker (2001) found that around half of the players they sampled used the mini-max strategy. In contrast, our findings suggest an alternative strategy amongst players without an alcohol use disorder who drank alcohol at the venue, since they preferred higher denomination EGMs and betting on more lines than their peers who did not drink alcohol at the venue. By using a double-max strategy, these gamblers potentially maximised the size of any win, albeit offset by more rapid loss. Such choice of strategy can be accounted for by the fact that the effects of alcohol lead to greater risk-taking (Chesher & Greeley, 1989; Fillmore, 2007) and a short-term increase in impulsiveness (Vazey et al., 2018). However, once again, there is a need for replication and precise measurement of bet size in order to investigate this possibility.
Although it has been generally reported that male players have a preference for higher denomination EGMs than females (Delfabbro, 2012; Hing et al., 2016; Wong et al., 2013), it is interesting to note that low-risk female gamblers consuming alcohol at the venue had a higher EGM denomination preference than all other groups in our study, and that at-risk male gamblers who did not drink at the venue had the lowest EGM denomination preference. Moreover, we also found that female problem gamblers who did not drink at the venue made a far higher average expenditure than any other group. These findings suggest that the conception of females being more risk averse than males holds true only under certain conditions and that the pattern of interactions with biological gender is complex, and we hope these finding will prompt further research.
Limitations
While having the advantage of reporting the experiences of authentic EGM players in a naturalistic environment, our study lacked the tight control of a laboratory study. In particular, we lacked precise measurement of alcohol consumed at the venue and we relied on retrospective reports rather than observed behaviour. Rather than assessing alcohol consumption while gambling with a single yes or no response, a continuous response scale from never to always and a measure of quantity would have enabled more fine-grained analysis of the effects of alcohol on gambling behaviour. Furthermore, since drinking at the venue was an uncontrolled variable, we cannot assume causality. There is the possibility that both the decision to drink and the decision to take higher risks in gambling were determined by a latent variable and this can only be ruled out by direct experimental manipulation of alcohol consumption. But another potential issue is the accuracy of the players’ self-reports in terms of the amount spent which tends to be an underestimate, particularly with high expenditure (Auer & Griffiths, 2017) which may be compounded by the detrimental effects of alcohol consumption on memory (Dry et al., 2012), and this may explain the lack of significant differences in terms of expenditure. Moreover, while our measure of preferred machine denomination was useful, we could gain more insight by asking about preferred bet size per spin (c.f. number of credits per line and number of lines). In the light of our findings, we believe this may be important, particularly for players who drink at the venue since we have some indication of a strategy adopted by that subgroup. Finally, since we did not ask participants about their use of drugs, illicit or otherwise, we were not in a position to directly address the finding by Bussu and Detotto (2015) that a combination of alcohol and illicit drugs, rather than just alcohol alone, would influence the amount bet.
Conclusion and Implications
In summary, this study examined individual differences in response to concurrent alcohol consumption and gambling to more precisely identify their association with elements of EGM gambling behaviour. The double-max strategy we found amongst gamblers with an alcohol use disorder who consumed alcohol at the venue may be accounted for by increases in neural dopamine caused by alcohol, in addition to that already resulting from gambling (Goodman, 2008). Dopamine acts as a signal for imminent reward (Montague & Berns, 2002), but it has also been shown to correlate with the expected magnitude and probability of the reward (Rolls et al., 2008). It is possible therefore that alcohol intensifies the anticipation of reward, thus encouraging riskier bets. In order to examine this in more detail, future studies should determine the preferred bet size rather than preferred EGM denomination, ideally with measurement of neural dopamine levels.
While the use of retrospective questionnaires is widespread in psychology, it is nevertheless susceptible to involuntary distortions of memory (self-deceptive enhancement) and impression management (Goldstein et al., 2017). An in situ observational study is theoretically possible, though such close observation would be looked upon with suspicion and would pose ethical problems, particularly in terms of monitoring alcohol consumption. Moreover, it would likely influence behaviour in unintended ways, c.f. a reduction in drinking and/or gambling. However, given that we have a clear indication of the important dependent variables, further investigation of these phenomena could employ at least a real-time diary study, with participants recording their alcohol consumption, along with other variables of interest, over the period of a single session.
Our findings have practical implications, particularly regarding the sale and consumption of alcohol in gambling venues, since we have shown that concurrent consumption of alcohol is associated with a preference for higher denomination machines that increase the risk of more rapid financial loss. A practical way to minimise such harm would be in the form of information available to gamblers, making them aware of the ways in which alcohol may affect their decision making and the potential financial impact it could have. As is currently the case with pregnancy, it is also important to alert female gamblers to their greater physiological susceptibility to alcohol and the ways in which it may adversely affect their judgement while playing EGMs. In addition, reducing the maximum denomination amount allowable on EGMs would help to reduce the more rapid losses associated with higher-denomination EGMs, and may reduce their attraction to gamblers affected by alcohol. Further, venues need to adhere to regulations governing responsible service of alcohol to prevent EGM players from gambling while intoxicated. Finally, the evidence presented here gives support to the recommendation that sale of alcohol should not be permitted at gambling venues.
References
Auer, M., & Griffiths, M.D. (2017). Self-reported losses versus actual losses in online gambling: An empirical study. Journal of Gambling Studies, 33(3), 795–806. https://doi.org/10.1007/s10899-016-9648-0
Banks, S., Catcheside, P., Lack, L., Grunstein, R. R., & McEvoy, R. D. (2004). Low levels of alcohol impair driving simulator performance and reduce perception of crash risk in partially sleep deprived subjects. Sleep, 27, 1063–1067.
Baraona, E., Abittan, C. S., Dohmen, K., Moretti, M., Pozzato, G., Chayes, Z. W., Schaefer, C., & Lieber, C. S. (2001). Gender differences in pharmacokinetics of alcohol. Alcoholism: Clinical and Experimental Research, 25, 502–507.
Barnes, G. M., Welte, J. W., Tidwell, M., & Hoffman, J. H. (2015). Gambling and substance use: Cooccurrence among adults in a recent general population study in the United States. International Gambling Studies, 15, 55–71.
Baron, E., & Dickerson, M. (1999). Alcohol consumption and self-control of gambling behaviour. Journal of Gambling Studies, 15, 3–15.
Bush, B., Shaw, S., Cleary, P., Delbanco, T. L., & Aronson, M. D. (1987). Screening for alcohol abuse using the CAGE questionnaire. American Journal of Medicine, 82, 231–235.
Bussu, A., & Detotto, C. (2015). The bidirectional relationship between gambling and addictive substances. International Gambling Studies, 15, 285–308.
Cermak, L. S. (1990). Cognitive-processing deficits in chronic alcohol abusers. Alcohol Health and Research World, 14, 130–136.
Chan, A. W. K., Pristach, E. A., & Welte, J. W. (1994). Detection by the CAGE of alcoholism or heavy drinking in primary care outpatients and the general population. Journal of Substance Abuse, 6, 123–135.
Chesher, G., & Greeley J. (1989). The effect of alcohol on cognitive & psychomotor functioning. In: Greeley, J. & Gladstone, W., National Drug & Alcohol Research Centre, Monograph No 8.
Conover, W. J., & Iman, R. L. (1981). Rank transformations as a bridge between parametric and nonparametric statistics. The American Statistician, 35, 124–129.
Cronce, J. M., & Corbin, W. R. (2010). Effects of alcohol and initial gambling outcomes on within-session gambling behavior. Experimental and Clinical Psychopharmacology, 18, 145–157.
Delfabbro, P. H. (2012). Australasian gambling review (5th ed.). Independent Gambling Authority.
Delfabbro, P. H., & Gainsbury, S. M. (2020). Understanding gambling and gaming skill and its implications for the convergence of gaming with electronic gaming machines. International Gambling Studies, 20, 171–183.
Dick, D. M., Smith, G., Olausson, P., Mitchell, S. H., Leeman, R. F., O’Malley, S. S., & Sher, K. (2010). Understanding the construct of impulsivity and its relationship to alcohol use disorders. Addiction Biology, 15, 217–226.
Dry, M. J., Burns, N. R., Nettelbeck, T., Farquharson, A. L., & White, J. M. (2012). Dose-related effects of alcohol on cognitive functioning. PLoS ONE, 7, e50977.
Ellery, M., & Stewart, S. H. (2014). Alcohol affects video lottery terminal (VLT) gambling behaviors and cognitions differently. Psychology of Addictive Behaviors, 28, 206–216.
Ellery, M., Stewart, S. H., & Loba, P. (2005). Alcohol’s effects on video lottery terminal (VLT) play among probable pathological and non-pathological gamblers. Journal of Gambling Studies, 21, 299–324.
Erol, A., & Karpyaka, V. M. (2015). Sex and gender-related differences in alcohol use and its consequences: Contemporary knowledge and future research considerations. Drug and Alcohol Dependence, 156, 1–13.
Ewing, J. A. (1984). Detecting alcoholism. The CAGE questionnaire. Journal of the American Medical Association, 252, 1905–1907.
Ferris, J., & Wynne, H. (2001). The Canadian Problem Gambling Index: Final report. Canadian Centre on Substance Abuse.
Fillmore, M. T. (2007). Acute alcohol-induced impairment of cognitive functions: Past and present findings. International Journal on Disability and Human Development, 6, 115–125.
Gainsbury, S., Wood, R., Russell, A., Hing, N., & Blaszczynski. (2012). A digital revolution: Comparison of demographic profiles, attitudes and gambling behavior of Internet and non-Internet gamblers. Computers in Human Behavior, 28, 1388–1398.
Giacopassi, D., Stitt, B. G., & Vandiver, M. (1998). An analysis of the relationship of alcohol to casino gambling among college students. Journal of Gambling Studies, 14, 135–149.
Goldstein, A. L., Vilhena-Churchill, N., Munroe, M., Stewart, S. H., Flett, G. L., & Hoaken, P. N. S. (2017). Understanding the effects of social desirability on gambling self-reports. International Journal of Mental Health and Addiction, 15, 1342–1359.
Goodman, A. (2008). Neurobiology of addiction: An integrative review. Biochemical Pharmacology, 75, 266–322.
Harries, M. D., Redden, S. A., Leppink, E. W., Chamberlain, S. R., & Grant, J. E. (2017). Sub-clinical alcohol consumption and gambling disorder. Journal of Gambling Studies, 33, 473–486.
Harrigan, K., Dixon, M., MacLaren, V., Collins, K., & Fugelsang, J. (2011). The maximum rewards at the minimum price: Reinforcement rates and payback percentages in multi-line slot machines. Journal of Gambling Issues, 26, 11–29.
Harvanko, A. M., Odlaug, B. L., Schreiber, L. R., & Grant, J. E. (2012). Cognitive task performance and frequency of alcohol usage in young adults. Journal of Addiction Medicine, 6, 106–111.
Hayes, V., Demirkol, A., Ridley, N., Withall, A., & Draper, B. (2016). Alcohol-related cognitive impairment: Current trends and future perspectives. Neurodegenerative Disease Management, 6, 509–523.
Hernández-Collados, A., Sánchez-Turet, M., Antonijoan, R., Massana, E., & Barbanoj, M. (1997). Time perception is distorted under alcohol effects, even at BAC value near to zero. International Journal of Psychophysiology, 25, 45.
Hing, N., & Breen, H. (2001). An empirical study of sex differences in gaming machine play amongst club members. International Gambling Studies, 1, 67–86.
Hing, N., Russell, A., Tolchard, B., & Nower, L. (2016). Risk factors for gambling problems: An analysis by gender. Journal of Gambling Studies, 32, 511–534.
Imperatori C, Corazza O, Panno A, Rinaldi R, Pasquini M, Farina B, Biondi M, Bersani FS. (2020). Mentalization impairment is associated with problematic alcohol use in a sample of young adults: A cross-sectional study. International Journal of Environmental Research and Public Health, 17, 8664. https://doi.org/10.3390/ijerph17228664
Kendler, K. S., Schmitt, E., Aggen, S. H., & Prescott, C. A. (2008). Genetic and environmental influences on alcohol, caffeine, cannabis, and nicotine use from early adolescence to middle adulthood. Archives of General Psychiatry, 65, 674–682.
Kerr, J. S., & Hindmarch, I. (1998). The effects of alcohol alone or in combination with other drugs on information processing, task performance and subjective responses. Human Psychopharmacology, 13, 1–9.
Koob, G. F. (1997). Drug abuse: Hedonic homeostatic dysregulation. Science, 278, 52–58.
Kyngdon, A., & Dickerson, M. (1999). An experimental study of the effect of prior alcohol consumption on a simulated gambling activity. Addiction, 94, 697–707.
Leino, T., Molde, H., Griffiths, M. D., Mentzoni, R. A., Sagoe, D., & Pallesen, S. (2017). Gambling behavior in alcohol-serving and non-alcohol-serving-venues: A study of electronic gaming machine players using account records. Addiction Research & Theory, 25, 201–207.
Lorains, F., Cowlishaw, S., & Thomas, S. (2011). Prevalence of comorbid disorders in problem and pathological gambling: Systematic review and meta-analysis of population surveys. Addiction, 106, 490–498.
Markham, F., Young, M., & Doran, B. (2012). The relationship between alcohol consumption, gambling behaviour and problem gambling during a single visit to a gambling venue. Drug and Alcohol Review, 31, 770–777.
Miller, M. A., Weafer, J., & Fillmore, M. T. (2009). Gender differences in alcohol impairment of simulated driving performance and driving-related skills. Alcohol & Alcoholism, 44, 586–593.
Montague, P. R., & Berns, G. S. (2002). Neural economics and biological substrates of valuation. Neuron, 36, 265–284.
Ogden, R., Wearden, J., Gallagher, D. T., & Montgomery, C. (2011). The effect of alcohol administration on human timing: A comparison of prospective timing, retrospective timing and passage of time judgements. Acta Psychologica, 138, 254–262.
Olsen, R., Hanchar, H., Meera, P., & Wallner, M. (2007). GABAA receptor subtypes: The “one glass of wine” receptors. Alcohol, 41, 201–209.
Park, S., Cho, M. J., Jeon, H. J., Lee, H. W., Bae, J. N., Park, J. I., Sohn, J. H., Lee, Y. R., Lee, J. Y., & Hong, J. P. (2010). Prevalence, clinical correlations, comorbidities, and suicidal tendencies in pathological Korean gamblers: Results from the Korean Epidemiologic Catchment Area Study. Social Psychiatry and Psychiatric Epidemiology, 45, 621–629.
Petry, N. M., Stinson, F. S., & Grant, B. F. (2005). Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: Results from the national epidemiologic survey on alcohol and related conditions. Journal of Clinical Psychiatry, 66, 564–574.
Phillips, J. G., & Ogeil, R. P. (2007). Alcohol consumption and computer blackjack. The Journal of General Psychology, 134, 333–353.
Pino-Gutierrez, A., Fernandez-Aranda, F., Granero, R., Tarrega, S., Valdeperez, A., Aguera, Z., Håkansson, A., Sauvaget, S., Aymamí, N., Gómez-Peña, M., Moragas, L., Baño, M., Honrubia, M., Menchón, J. M., & Jiménez-Murcia, S. (2017). Impact of alcohol consumption on clinical aspects of gambling disorder. International Journal of Mental Health Nursing, 26, 121–128.
Robbins, T. W., & Arnsten, A. F. (2009). The neuropsychopharmacology of fronto-executive function: Monoaminergic modulation. Annual Review of Neuroscience, 32, 267–287.
Rockloff, M., Stuart, G., Kim, H.S., & Hodgins, D.C. (2019). Free-spins spur gamblers to quit EGMs early: An online EGM study. Journal of Gambling Studies, 36, 435–443
Rolls, E. T., McCabe, C., & Redoute, J. (2008). Expected value, reward outcome, and temporal difference error representations in a probabilistic decision task. Cerebral Cortex, 18, 652–663.
Russell, A. M. T., Browne, M., Hing, N., Rockloff, M., & Newall, P. (2021). Are any samples representative or unbiased? Reply to Pickering and Blaszczynski. International Gambling Studies. https://doi.org/10.1080/14459795.2021.1973535
Sacco, P., Torres, L. R., Cunningham-Williams, R. M., Woods, C., & Unick, G. (2011). Differential item functioning of pathological gambling criteria: An examination of gender, race/ethnicity and age. Journal of Gambling Studies, 27, 317–330.
Sévigny, S., Leclerc, M., Goulet, A., Côté, K., Jacques, C., Ladouceur, R., & Giroux, I. (2016). Electronic gambling machine gamblers’ characteristics vary according to the type of gambling venue: A Canadian study. International Gambling Studies, 16, 116–139.
Shek, D. T. L., Chan, E. M. L., & Wong, R. H. Y. (2012). Associations between pathological gambling and psychiatric comorbidity among help-seeking populations in Hong Kong. The Scientific World Journal, 2012, 1–15.
Shen, Y., Kairouz, S., Nadeau, L., & Robillard, C. (2015). Comparing problem gamblers with moderate-risk gamblers in a sample of university students. Journal of Behavioral Addictions, 4, 53–59.
Smart, R., & Ferris, J. (1996). Alcohol, drugs and gambling in the Ontario adult population, 1994. Canadian Journal of Psychiatry, 41, 36–45.
Smith, D. P., Battersby, M., & Harvey, P. W. (2015). Does gender moderate the subjective measurement and structural paths in behavioural and cognitive aspects of gambling disorder in treatment-seeking adults? Addictive Behaviors, 48, 12–18.
Stewart, S. H., McWilliams, L. A., Blackburn, J. R., & Klein, R. M. (2002). A laboratory-based investigation of relations among video lottery terminal (VLT) play, negative mood, and alcohol consumption in regular VLT players. Addictive Behaviors, 27, 819–835.
Strong, D. R., & Kahler, C. W. (2007). Evaluation of the continuum of gambling problems using the DSM-IV. Addiction, 102, 713–721.
Sullivan, E. V., Rosenbloom, M. J., & Pfefferbaum, A. (2000). Pattern of motor and cognitive deficits in detoxified alcoholic men alcoholism. Clinical and Experimental Research, 24, 611–621.
Vazey, E. M., den Hartog, C. R., & Moorman, D. E. (2018). Central noradrenergic interactions with alcohol and regulation of alcohol-related behaviors. Handbook of Experimental Pharmacology, 48, 239–260.
Walker, M.B. (2001). Strategies for winning on poker machines. In A. Blaszczynski (Ed.). Culture and the gambling phenomenon: Proceedings of the 11th annual conference of the National Association for Gambling Studies (pp. 391–396).
Wenzel, H. G., & Dahl, A. A. (2009). Female pathological gamblers: A critical review of the clinical findings. International Journal of Mental Health and Addiction, 7, 190–202.
Williamson, A., & Walker, M. (2001). Strategies for solving the insoluble: Playing to win Queen of the Nile. In G. Coman (Ed.) Lessons of the Past: Proceedings of the 10th annual conference of the National Association for Gambling Studies (pp. 444–452).
Wong, G., Zane, N., Saw, A., & Chan, A. K. K. (2013). Examining gender differences for gambling engagement and gambling problems among emerging adults. Journal of Gambling Studies, 29, 171–189.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions This study was funded by the Centre for Gambling Education and Research at Southern Cross University of which Professor Nerilee Hing was a member at the time of data collection.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval
The research described herein complies with the National Statement on Ethical Conduct in Human Research (NHMRC) and was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Stuart, G., Hing, N. & Russell, A.M.T. Interactive Effects of Problem-Gambling Severity, Gender and Alcohol Consumption on Electronic Gaming Machine Behaviour. Int J Ment Health Addiction 21, 4179–4198 (2023). https://doi.org/10.1007/s11469-022-00849-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11469-022-00849-3