
Abstract
Background
A high signal intensity cleft between the labrum and articular cartilage of the posterior glenoid is commonly visible on MRI and has been suggested to be anatomic variation [3, 10, 23]. The association of a posterior cleft with variations in glenoid morphology or with shoulder instability is unknown.
Questions/Purposes
The purposes of this study were to determine if posterior chondrolabral clefts are associated with variations in glenoid morphology, and to determine if they are associated with shoulder instability.
Patients and Methods
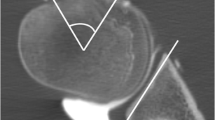
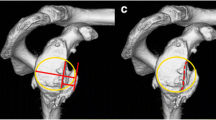
Shoulder MRI was performed in 1,264 shoulders, 1,135 male (89.8%), and 129 female (10.2%). A musculoskeletal radiologist blinded to history and outcomes evaluated the MR images for linear high signal intensity at the posterior chondrolabral junction and a rounded or truncated contour of the posterior glenoid. Glenoid version and depth were measured. Patients were followed prospectively for shoulder instability for 4 years. Univariate and multivariate statistical analysis were performed.
Results
Posterior chondrolabral cleft was present in 114/1,264. Posterior chondrolabral cleft was associated with a rounded or truncated posterior glenoid. There were 9.5° retroversion in shoulders with a posterior cleft, and 7.7° retroversion in shoulders without a cleft. Shoulders with a posterior chondrolabral cleft were more likely to develop shoulder instability.
Conclusions
Posterior chondrolabral clefts are not uncommon on MRI. They are associated with a rounded or truncated posterior glenoid and a small but significant increase in glenoid retroversion. They are associated with shoulder instability.





Similar content being viewed by others

References
Bigliani LU, Kelkar R, Flatow EL, Pollock RG, Mow VC. Glenohumeral stability. Biomechanical properties of passive and active stabilizers. Clin Orthop Relat Res. 1996; 330: 13-30.
Blasier RB, Guldberg RE, Rothman ED. Anterior shoulder stability: contributions of rotator cuff forces and capsular ligaments in a cadaver model. J Shoulder Elbow Surg. 1992; 1: 140-150.
Cooper DE, Arnoczky SP, O’Brien SJ, Warren RF, DiCarlo E, Allen AA. Anatomy, histology, and vascularity of the glenoid labrum. J Bone Joint Surg Am. 1992; 74A(1): 46-52.
Edelson JG. Localized glenoid hypoplasia: an anatomic variation of possible clinical significance. Clin Orthop Relat Res. 1995; 321: 189-195.
Gibb TD, Sidles JA, Harryman DT, McQuade KJ, Matsen FA III. The effect of capsular venting on glenohumeral laxity. Clin Orthop. 1991; 268: 120-127.
Harper KW, Helms CA, Haystead CM, Higgins LD. Glenoid dysplasia: incidence and association with posterior labral tears as evaluated by MRI. Am J Roentgenol. 2005; 184: 984-988.
Ikeda H, Tsukanishi S, Nobuhara K. Shoulder instability: its relationship to glenoid dysplasia. Seikeisaigaigeka. 1984; 27: 1757-1765 (in Japanese).
Inui H, Sugamoto K, Miyamoto T, et al. Glenoid shape in atraumatic posterior instability of the shoulder. Clin Orthop. 2002; 403: 87-92.
Kim SH, Ha KI, Yoo JC, Noh KC. Kim’s lesion: an incomplete and concealed avulsion of the posteroinferior labrum in posterior or multidirectional posteroinferior instability of the shoulder. Arthroscopy. 2004; 20: 712-720.
Lee GY, Choi JA, Oh JH, Choi JH, Hong SH, Kang HS. Posteroinferior labral cleft at direct CT arthrography of the shoulder by using multidetector CT: is this a normal variant? Radiology. 2009; 253: 765-770.
Lee SB, Kim KJ, O'Driscoll SW, Morrey BF, An KN. Dynamic glenohumeral stability provided by the rotator cuff muscles in the mid-range and end-range of motion. A study in cadavera. J Bone Joint Surg Am. 2000; 82(6): 849-857.
Legan JM, Burkhard TK, Goff WB II, et al. Tears of the glenoid labrum: MR imaging of 88 arthroscopically confirmed cases. Radiology. 1991; 179: 241-246.
Lippert WC, Mahlman CT, Cornwall R, et al. The intrarater and interrater reliability of glenoid version and glenohumeral subluxation measurements in neonatal brachial plexus palsy. J Pediatr Orthop. 2012; 32(4): 378-384.
Lippitt WB, Vanderhooft JE, Harris SL, Sidles JA, Harryman DT, Matsen FA III. Glenohumeral stability from concavity-compression: a quantitative analysis. J Shoulder Elbow Surg. 1993; 2: 27-35.
Mallon WJ, Brown HR, Vogler JB, Martinez S. Radiographic and geometric anatomy of the scapula. Clin Orthop Relat Res. 1992; 277: 142-154.
Mohana-Borges AV, Chung CB, Resnick D. Superior labral anteroposterior tear: classification and diagnosis on MRI and MR arthrography. Am J Roentgenol. 2003; 181: 1449-1462.
Nyffeler RW, Jost B, Pfirrmann CWA, Gerber C. Measurement of glenoid version: conventional radiographs versus computed tomography scans. J Shoulder Elbow Surg. 2003; 12(5): 493-496.
Owens BD, Campbell SE, Cameron KL. Risk factors for posterior shoulder instability in young athletes. Am J Sports Med. 2013; 41: 2645-2649.
Owens BD, Duffey ML, Nelson BJ, DeBerardino TM, Taylor DC, Mountcastle SB. The incidence and characteristics of shoulder instability at the United States Military Academy. Am J Sports Med. 2007;35(7):1168-73.
Owens BD, Nelson BJ, Duffey ML, et al. Pathoanatomy of first-time, traumatic, anterior glenohumeral subluxation events. J Bone Joint Surg Am. 2010; 92: 1605-1611.
Randelli M, Gambrioli PL. Glenohumeral osteometry by computed tomography in normal and unstable shoulder. Clin Orthop Rel Res. 1986; 208: 151-156.
Snyder SJ, Karzel RP, Del Pizzo W, et al. SLAP lesions of the shoulder. Arthroscopy. 1990; 6: 274-279.
Tuite MJ, Currie JW, Orwin JF, Baer GS, Munoz del Rio A. Sublabral clefts and recesses in the anterior, inferior, and posterior glenoid labrum at MR arthrography. Skeletal Radiol 2012. doi:10.1007/s00256-012-1496-0.
Warner JJ, Bowen MK, Deng X, Torzilli PA, Warren RF. Effect of joint compression on inferior stability of the glenohumeral joint. J Shoulder Elbow Surg. 1999; 8(1): 31-36.
Warren RF. Subluxation of the shoulder in athletes. Clin Sports Med. 1983; 2(2): 339-354.
Disclosures
ᅟ
Conflict of Interest:
Scot E. Campbell, MD, Robert M. Dewitt, MD, MPH, ATC, and Adrianne K. Thompson, MD have declared that they have no conflict of interest. Kenneth L Cameron, PhD reports grants from Orthopedic Research and Education Foundation, during the study. Brett D. Owens, MD reports grants from OREF, during the conduct of the study; personal fees from Mitek Sports Medicine and Musculoskeletal Transplant Foundation, outside the work.
Human/Animal Rights:
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 [5].
Informed Consent:
Informed consent was obtained from all patients for being included in the study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Level of Evidence: Level IV: Cohort study.
The views and opinions expressed in this manuscript are those of the author(s) and do not reflect the official policy of the Department of the Army, the US Air Force, the Department of Defense, or the US Government.
Rights and permissions
About this article

Cite this article
Campbell, S.E., Dewitt, R.M., Cameron, K.L. et al. Posterior Chondrolabral Cleft: Clinical Significance and Associations with Shoulder Instability. HSS Jrnl 10, 208–212 (2014). https://doi.org/10.1007/s11420-014-9404-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11420-014-9404-x