
Abstract
Environmental pollution has been a major concern for researchers and policymakers. A number of studies have been conducted to enquire the causes of environmental pollution which suggested numerous policies and techniques as remedial measures. One such major source of environmental pollution, as reported by previous studies, has been the garbage resulting from disposed hospital wastes. The recent outbreak of the COVID-19 pandemic has resulted into mass generation of medical waste which seems to have further deteriorated the issue of environmental pollution. This necessitates active attention from both the researchers and policymakers for effective management of medical waste to prevent the harm to environment and human health. The issue of medical waste management is more important for countries lacking sophisticated medical infrastructure. Accordingly, the purpose of this study is to propose a novel application for identification and classification of 10 hospitals in Iraq which generated more medical waste during the COVID-19 pandemic than others in order to address the issue more effectively. We used the Multi-Criteria Decision Making (MCDM) method to this end. We integrated MCDM with other techniques including the Analytic Hierarchy Process (AHP), linear Diophantine fuzzy set decision by opinion score method (LDFN-FDOSM), and Artificial Neural Network (ANN) analysis to generate more robust results. We classified medical waste into five categories, i.e., general waste, sharp waste, pharmaceutical waste, infectious waste, and pathological waste. We consulted 313 experts to help in identifying the best and the worst medical waste management technique within the perspectives of circular economy using the neural network approach. The findings revealed that incineration technique, microwave technique, pyrolysis technique, autoclave chemical technique, vaporized hydrogen peroxide, dry heat, ozone, and ultraviolet light were the most effective methods to dispose of medical waste during the pandemic. Additionally, ozone was identified as the most suitable technique among all to serve the purpose of circular economy of medical waste. We conclude by discussing the practical implications to guide governments and policy makers to benefit from the circular economy of medical waste to turn pollutant hospitals into sustainable ones.
Similar content being viewed by others


Introduction
In 2015, all the member states of the United Nations adopted the 2030 agenda for sustainable development as a plausible solution to the social, economic, and environmental issues. This commitment highlights the significance of sustainability of the environment for the survival of humans as well as of organizations. Future economic growth is highly dependent on the sustainable business models (Despeisse et al., 2012; Akanbi et al., 2018; Sassanelli et al., 2019). Sustainability, thus, is one of the major concerns for contemporary organizations and it exceeds the environmental concerns. Consumers have prompted manufacturers to redesign their products for the purpose of reuse and recycling to generate added value (Aitken et al., 2021; Qiu et al., 2021; Aboramadan et al., 2021). Consequently, manufacturers have moved away from the traditional business models to sustainable ones—(Kulkarni, & Anantharama, 2020; Shuv-Ami & Shalom, 2020; Purnomo et al., 2021)—models based on the concept of circular economy (Eneizan et al., 2019; Al-Abrrow et al., 2021a; Abdulaali et al., 2019; Khaw et al., 2022a).
Circular economy is a mode of economic development that complies with the environmental and ecological standards and is based on the principles of “reduce the usage of resources, reuse and recycle” (Zhijun & Nailing, 2007). Its economic framework seeks to eliminate “waste” and turns it into useable materials and, thus, promotes the reuse of resources to optimum levels. The entire circular economic system is aimed at re-exploitation, regeneration, repair, and recycling of the resources to develop a closed-loop system that minimizes the input resources (Suresh et al., 2020; Nandi et al., 2021; Silva et al., 2021). The reuse of resources works as raw materials for the production of other goods (Rume & Islam, 2020; Teymourian et al., 2021). This also reduces the production cost incurred on the acquisition of raw materials. Resultantly, greater efficiency in production can be achieved by dismantling the critical elements and focusing more on the sub-processes which increase the overall production cost of the entire production process (MacNeill et al., 2020; Moraes et al., 2021).
Circular economy in the production medical item has started to catch the attention of scientists, researchers, and professionals, especially after the voluminous generation of medical waste during and after the COVID-19 pandemic. Medical waste management and disposal is closely linked to the future sustainability goals. The current practices of managing and disposing medical waste are not according to the approved standards of WHO, whereas the situation in developing and less developed countries is rather graver vis-a-vis the developed world. Developed countries are more focused on the growth of supply chain of medical equipment industry to curtail the medical waste and increase reuse and recycling of medical waste (Solomon et al., 2020; Iyengar et al., 2020). On the other hand, appropriate management of medical waste is an essential matter for the medical organizations in countries like Iraq which is facing economic development issues. The relevant studies have found that medical waste generated in the wake of COVID-19 is more contagious (Rupani et al., 2020; Ibn-Mohammed et al., 2021). Medical waste is generated not only in hospitals but also at home by healthcare users. The first one is classified as hazardous and the second one as non-hazardous waste (Mekonnen et al., 2021). According to the WHO, the hazardous medical waste is more harmful to human health than the non-hazardous one (Kumar et al., 2020a; Rupani et al., 2020). Though the uses of plastic-made personal protective equipment (PPE) have protected the medical workers form coronavirus, at the same time, it sought proper attention toward their disposal as they could become carrier of viruses. People have been afraid of infection, and the mandatory instructions implemented by many countries to use masks, gloves, and other tools have led to increased consumption of PPE and the consequent disposal (Debnath et al., 2021; Vanapalli et al., 2021). Although the PPE reduced the incidence of COVID-19 infection, the discardable PPE led to an enormous increase in environmental pollution (Ranjbari et al., 2022). Thus, effective methods must be provided to ensure safety and reduce infection rates by increasing the effectiveness of waste disposal (Teymourian et al., 2021).
Ibn-Mohammed et al. (2021) provided a critical review of the negative impacts of the global epidemic in terms of medical waste from the perspective of the circular economy. Similarly, Chojnacka et al. (2021) and Debnath et al. (2021) comprehensively discussed the issue of medical waste and its disposal techniques. There are various studies to this end but none of them has focused on “how to classify the hospitals according to their treatment of medical waste?,” especially in the context of Iraq.
Previous studies (e.g., Teymourian et al., 2021; Ranjbari et al., 2022) have found that there is lack of evidence as to rank hospitals with respect to their medical waste generation in the view of circular economy. Also, there are no appropriate methods on which Iraqi hospitals rely to dispose of medical waste. Ranking of hospitals according to their respective medical waste generation can help policymakers to devise appropriate methods for dealing the issues of increased consumption and usage of medical waste during the COVID-19 pandemic (Wuyts et al., 2020). Previous research suggested a few methods for weighing the volume and type of medical waste generated by hospitals and other medical facilities. These methods include AHP, Technique for Order of Preference by Similarity to Ideal Solution (TOPSIS), VIšekriterijumsko KOmpromisno Rangiranje (VIKOR), and FDOSM. Among these, FDOSM is the latest one (Khaw et al., 2021) which addresses many of the issues of uncertainty, increased comparisons, and the problem of consistency associated with other methods (Mohammed et al., 2022). Generally, all these techniques come under the umbrella of MCDM methods. MCDM has some major issues of ambiguity and unclear information. It is considered a unique MCDM technique in a fuzzy environment that employs the idea of an optimal situation and an opinion matrix to address the earlier mentioned issues of other techniques (Albahri et al., 2022a). In addition, it makes reasonable conclusions by seeking experts’ opinions. For the comparison process, FDOSM is able to reduce the wasting time because of its ability to overcome human unreliability. It also mitigates the number of mathematical equations required. As a result, this method saves data and makes intelligent decisions. Besides, the normalization and the weight of the mathematical method issues are also addressed by FDOSM. By using fuzzy numbers, it is possible to overcome the uncertainty of the data (Mohammed et al., 2022). Several types of fuzzy sets have been used with FDOSM to address the issue of uncertainty such as intuitionistic fuzzy sets, interval-valued fuzzy sets, and T-spherical fuzzy environments (Mohammed et al., 2022; Albahri et al., 2022b). Until now, according to the best of the authors’ knowledge, there is currently no study that expanded the FDOSM method with the LDFN environment to rank hospitals based on the generation of medical waste and proposed a smart solution to the problem of hospitals’ waste. When compared to other fuzzy concepts such as hesitant fuzzy sets, Pythagorean fuzzy, and T-spherical fuzzy sets, LDFN is considered an easy to use and flexible tool (Narayanamoorthy et al., 2022).
Earlier studies have used, specifically, Decision-Making Testing and Evaluation method (DEMATEL), to provide information about hospitals with a high rate of medical waste. However, these hospitals were not ranked according to the kinds of medical waste. Our study addresses this issue and simultaneously helps to rank hospitals with respect to the amount and type of medical waste. Additionally, hospitals in Iraq have limited methods to deal with the medical waste during the COVID-19 epidemic (Chauhan et al., 2020). Studies relevant to medical waste during COVID-19 have presented some effective techniques to avoid COVID-19 dissemination through waste, such as incineration technique, pyrolysis technique, microwave technique, autoclave chemical technique, vaporized hydrogen peroxide, dry heat, ozone, and ultraviolet light (Teymourian et al., 2021; Liu et al., 2021).
The coronavirus global epidemic had already affected the world due to the general rise of ecological concerns caused mainly by the quantity of used PPE. Besides the need for protection, the circular economy strategies of plastic recycling systems and ecologically benign and renewable alternatives for balancing sustainability need to be observed. According to the hospital rank in the MCDM analysis, the ANN analysis would suggest an applicable approach to the disposal of medical waste by determining the most suitable method of disposal of medical waste and providing a solution with high consistency and certainty. This study is focusing on hospitals in Iraq to rank and prioritized them according to volume of medical waste generated and treated in the aftermath of COVID-19 using a dual-stage MCDM and ANN approach. Thus, the main contribution of this study is the classification of hospitals on the basis of medical waste using the novel method LDFN-FDOSM. In addition, we have adopted a non-compensatory method (i.e., ANN) to provide a solution to hospitals about the best way to dispose of medical waste.
As we have been living in the times of the coronavirus, concern for human health is one of the most important aspects of health and environmental institutions. Controlling medical waste has become a critical challenge confronting medical fraternity worldwide, particularly during the COVID-19 pandemic crisis. The waste produced by hospitals is considered one of the essential sources that caused the spread of the virus. Therefore, our study aims to prevent the spread of the virus and mitigate environmental phenomena, such as global warming and emissions. Besides, the selection and evaluation of the best and the worst hospitals contribute to solving environmental and economic problems by providing insights into policymakers to reduce hospital waste. Furthermore, the study tends to inform the decision-makers about the circular economy’s contribution to decreasing resource waste and misuse. The final motivation is to decrease the time and expense of disposing of medical waste and to establish the best strategy for each institution during the coronavirus outbreak. Theoretically, when selecting the most suitable hospital, multiple variables must be taken into account. The situation clearly shows that the MCDM method can be used to tackle the ideal and worst hospital while AHP with LDFN-FDOSM is the most appropriate method of dealing with this condition.
This research paper is organized to present literature review and the current state of the circular economy for medical research. The next section, “Methodology,” explains the research procedures, followed by the “Results and discussion” section. In the end, “Conclusion” has been derived based on the findings and discussion.
Literature review
This section describes medical waste management and the circular economy. Furthermore, the following subsections explain the effectiveness of the circular economy in the disposal of medical waste.
Medical waste
In the recent past, pandemics (COVID-19, Ebola, SARS) and other infectious diseases (avian influenza, cholera, diphtheria, etc.) have exposed the world health systems and posed major health challenges for researchers and medical policymakers and practitioners. The spread of these diseases across various countries has posed different medical issues depending upon the fragility of the respective health system. To meet the challenges of pandemics and infectious diseases, the demand for medical equipment and other medical supplies has increased multifold (Singh, Ogunseitan & Tang, 2022). As a result of the mass production, the disposal of medical waste has become a humungous task to manage. Medical waste from the hospitals and private medical institutions is increasing regularly. It has been found that hospitals and other healthcare facilities are one of the major sources of environmental pollution and, according to one study, it is estimated to be contributing 4.4% of the greenhouses gas emissions (Karliner et al., 2020). In addition to environmental issue, the medical waste is also expensive to manage. It is reported that the cost of managing medical waste will reach to $17.89 billion in 2026 as compared to $11.77 billion in 2018, which is equivalent to the compound annual increase of 5.3% (RD Reports and Data, 2020). Also, due to the strict regulations by the governments especially after the outbreak of COVID-19, there is huge increase in medical waste particularly in developing countries. Thus, the gradual growth in medical waste after COVID-19 is posing a major threat not only to the environment but it is also emerging as a serious health concern all over the world (Peng et al., 2020, Singh et al., 2020a).
Pachauri et al. (2019) reported that more than half of the globe’s population was exposed to a variety of environmental and health issues due to the hazardous disposal of medical waste even before COVID-19. The hazardous disposal of medical waste is considered to be one of the major reasons of infectious diseases in economically less developed countries (Williams et al., 2019). The World Health Organization reported in 2018 that due to the repeated usage of infected syringes the spread of infectious diseases including hepatitis B has been 21 million, hepatitis C 2 million, and HIV aids 0.26 million around the globe. Similarly, another study of the WHO in 2015 across 24 countries reported that 18–64% of hospitals in less developed countries do not dispose of their medical waste in an appropriate way. The study revealed that among the countries in South-East Asia region, only 44% of the hospitals have proper mechanism of collection and disposal of the medical waste. Medical waste refers to all the wastage produced in hospital during the treatment which consists of excretions of the patients through blood and other ways. It also includes the used medical equipment and supplies like syringes, bottles, gloves and other personal protective equipment (PPE) (Fadhil et al., 2021; Hadi et al., 2018; AL-Abrrow et al., 2021b; Abbas et al., 2022).
COVID-19 and medical waste
The abrupt upsurge of COVID-19 has increased the requirements for medical equipment and other medical supplies. There has been spontaneous usage of medical equipment, especially the PPE. Accordingly, the disposal of medical waste has become a strategic management issue across various countries, particularly in those countries where the medical infrastructure is not much developed and where there are no regulations to medical waste disposal (Singh et al., 2020b). Lack of preparedness in many countries to combat the challenge of COVID-19 resulted into numerous social, economic, environmental, and medical issues due to the limited recycling and inappropriate dumping facilities (Kumar et al., 2020b; Ogunseitan, 2020). It has been reported that the collection and disposal of harmful medical waste have decreased by almost 80% at the start of the COVID-19 pandemic. This means that it was much difficult to manage and dispose of the additional medical waste generated in the aftermath of COVID-19 due to insufficient management and disposal facilities (Langley, 2020). Accordingly, the International Solid Waste Agency (ISWA) in 2020 warned against the proper management and disposal of medical waste because of approximately 305–50% extra burden of medical waste which would lead to failure of entire waste management system, especially in economically less developed countries. A study revealed improper disposal of medical waste (used and infectious equipment and supplies) in developing countries where the situation has been exacerbated by the infectious diseases (Zafar, 2019; Zar et al., 2020). Despite the immediate response to COVID-19 and other regulatory measures, there are still concerns about the safe and proper disposal of medical waste especially in less developed countries (Oruonye & Ahmed, 2020; Dieng et al., 2022). Public health authorities and other stakeholders are constantly raising their concerns about the safe and protected disposal of medical waste to address the environmental and public health issues. Countries need to revisit their medical waste disposal policies and to regulate the medical waste (Alnoor et al., 2022a; Sandberg et al., 2022; Alharbi & Alnoor, 2022; Albahri et al., 2022c; Alnoor et al., 2022b).
The World Health Organization has warned that medical waste carries agents that spread infections. The improper disposition of medical waste can cause the contamination of other wastes with virus and result in the wider transmission of virus into humans. There has been a greater need of appropriate disposal and management of medical waste, including its separation from other municipal wastes, proper collection, accumulation, and storage, and efficient disposal of waste (Ilyas et al., 2020). The WHO and other regulatory bodies have initiated awareness programs across the countries to inform and help people understand the importance and need of proper medical waste disposal and as in threatening medical issue which can cost long-term consequences if not addressed properly (Alnoor et al., 2022c; Alnoor et al., 2022d; Abdullah et al., 2022; Jabbar et al., 2020). It has been reported that the virus can survive for 6 to 8 h on polymer and for 5 to 6 h on metals, whereas in case of infectious PPE and other equipment, it may survive as long as 7 days if not disposed of properly. There is a need for greater care during the disposal; otherwise, it can contaminate the workers involved in discharge of waste disposal (Chin et al., 2020). Due to the lack of facilities, the situation is alarming in less developed countries because medical workers are vulnerably prone to infections (Cutler, 2020).
Various medical supplies like masks, aprons, and overalls are made from polymer which cannot be recycled due to their ability to survive longer in comparison to other materials. The workers which come into contact with such material can easily get contaminated. To protect the workers, certain regulations and practices have been made mandatory at hospitals and other medical facilities. These include regular cleaning of the PPEs, usage of fresh gloves and masks, proper disinfection of the supplies and equipment, and regular hand washing. Such measures can effectively control the spread of infection out of the hospitals and medical facilities. Nonetheless, after the outbreak of COVID-19, the medial waste is considered to be more infectious and dangerous with greater chances of spreading the virus and hence requires proper disposal and management (Dharmaraj et al., 2021). There is a need for a separate and isolated medical waste management system to curtail its hazardous effects. The WHO has advised laboratory workers and others who come in contact with medical equipment to use proper PPEs and directed the medical waste collectors to gather debris and dispose properly at the designated facilities without risk. This will decrease the harmful effects of the infections on public health and will lessen environmental concerns (Sharma et al., 2020).
The usage of medical accessories (hand sanitizers, gloves, and masks, etc.) has considerably increased in public places to stop the spread of COVID-19; resultantly, hospitals are not the only places which produce the medical waste (Ferasso et al. 2020). Usually, these protectives are not properly disposed of and serve as virus carriers. Studies have found that during COVID-19, it has become difficult for hospitals to properly and timely manage the medical waste (Singh et al., 2020a). The problem is more severe in less developed countries due to lack of appropriate facilities, insufficient resources, and technological backwardness (Bourouiba, 2020).
Circular economy
The concept of circular economy (CE) is catching the attention of both scholars and practitioners as evinced by the tremendous increase in the research articles in the recent years (Geissdoerfer et al., 2017, b) along with many other working papers and reports published on the topic. Some renowned consultancy firms, e.g., Accenture, Deloitte, EY, and McKinsey & Company, have published their reports on circular economy (Gartner, 2016; Hannon et al., 2016). The interest of both scholars and practitioners has increased in the topic because of its practical implications for business sustainability (Murray et al., 2017) and is viewed as one of the major issues to attract research intents. Despite the growing research interest, there is no mutually agreed upon definition of the concept (Kirchherr et al., 2017). The concept revolves around 3Rs, i.e., reduce, reuse, and recycle. Circular economy is a mode of economic development that complies with the environmental and ecological standards and it is based on the principles of “reduce the usage of resources, reuse and recycle of resources” (Zhijun & Nailing, 2007). Yuan et al. (2006: 5) in Kirchherr et al. (2017) stated that “the core of circular economy are the ‘3Rs’ principle – reduction, reuse and recycling of materials and energy. The approach is expected to achieve an efficient economy while discharging fewer pollutants. The strategy requires complete reform of the whole system of human activity”. Scholars have even proposed 4Rs, 6Rs, and 9Rs framework to conceptualize the circular economy (see Sihvonen & Ritola, 2015; van Buran et al., 2016 & Kirchherr et al., 2017). However, the widely used concept revolves around the 3Rs framework of “reduction, reuse, and recycling.” Kirchherr et al. (2017: 229) analyzed 114 definitions of CE and developed a coding framework and defined CE as “an economic system that replaces the ‘end-of-life’ concept with reducing, alternatively reusing, recycling and recovering materials in production/distribution and consumption processes.” They further argued that CE operates at both micro- and macro-levels with the purpose to achieve the goal of sustainable economic, human, and environment development and thus ensures the quality of economic, social, and environmental aspects of human life to the benefit[s] of current and coming generations. Similarly, CE safeguards the remodeling of businesses and responsible consumers’ conduct (Alnoor et al., 2023; Khaw et al., 2022b; Sadaa et al., 2022; Wah et al., 2022; Ahmed et al., 2022). The work of Kirchherr et al. (2017) acknowledges the disagreement in the definition of CE among various scholars. Some of the authors relate CE to “recycling” only, whereas majority of the authors are supportive of the 3Rs framework and argue that “recycling” is just one of the components of CE, not the CE per se. Similarly, another group of authors claims that the purpose of CE is only economic development, while its opponents favor the idea that CE chiefly concerns with environmental goals. Still there are others who claim that CE overlooks the social considerations or social equity concerns (Murray et al., 2017; Moreau et al., 2017).
A number of scholars, for example, Andersen (2007), Ghisellini et al. (2016), and Su et al. (2013), refer to the work of Pearce and Tuner (1989) as the pioneer study to have introduced the concept of circular economy. They studied the features of economic system[s] of the time and discovered how natural resources affect an economic system through provision of input for variety of products and their consumption by the end users. They argued that natural resources also serve as a “sink” in the shape of wastage. They discussed the concept of CE in terms of “loop economy”—an industry’s strategies are focused on the prevention of industrial waste, provision of employment opportunities, efficient utilization of resources, and dematerialization of the industrial economy. To achieve sustainability, Stahel (1982) argued that it would be better to sell “use” of the goods and not the “ownership.” This protects businesses from extra cost and risk associated with the industrial and other business wastes. The current conceptualization of CE and its economic implications has grown out of different concepts with different features and characteristics. Similarly, another promising definition of CE was given by the Ellen MacArthur Foundation (2013: 14) stating that circular economy is “an industrial economy that is restorative or regenerative by intention and design.” Yet in another definition, Geng and Doberstein (2008: 231) described CE as a “realization of closed loop material flow in the whole economic system.” Likewise, according to Webster (2015), the objective of CE is to ensure maximum utilization and value of the products and material[s], whereas Yuan et al. (2008) emphasized that the CE is related to the flow and usage of raw materials and energy during different stages in an economic system. Finally, Geissdoerfer et al. (2017, b: 759) gave one of the most precise and comprehensive definitions of CE. They defined it as “a regenerative system in which resource input and waste, emission, and energy leakage are minimized by slowing, closing, and narrowing material and energy loops. This can be achieved through long-lasting design, maintenance, repair, reuse, remanufacturing, refurbishing, and recycling.”
The essence of the circular economy is that it turns the products which are nearly at the end of their useful life into “input resources” for the other products and thus reduces the industrial waste, termed as “closing the industrial loop[s].” It aims to convert “un-useful” to “useful” through optimum utilization, recycling, repairing, and manufacturing. A study across different European regions found that CE would lower the greenhouse gas emissions by 70% and increase employability by 4% (Stahel, 2008). Stahel contended that there are two business models which align with the concept of circular economy. One is based on the “reuse” of goods and services through repair and upgradation and the second is based on the notion of “recycling,” i.e., converting old into new ones. In both cases, people [human resources] are central as they are involved in all the phases of the two models. In this way, CE does not only extend the life of old goods but it also creates employment opportunities during the different phases of the two models. Stahel further argued that CE resembles a lake—the reprocessing of products and material creates employment and preserves energy while also curtails the resource utilization and waste.
The concept of circular economy is largely followed by the European and other developed countries, i.e., China, Canada, and Japan. In 2018, European Commission reported that circular economy can generate a revenue of 600 billion euros annually for European manufacturing units. Similarly, it has been estimated that Finland can benefit from circular economy worth 2.5 billion euros annually and global economy can generate economic gain of $1000 billion per annum. China is reported to be the first country to formally regulate the circular economy (Korhonen et al., 2018; CIRAIG, 2015). Circular economy is considered to be closely linked with the sustainable economic and environmental growth. It provides an alternative economic system based on the flow of goods and material (3R), low industrial waste, and less harm to the environment with more business opportunities. More than theoretical, the nature of the concept is closer to its practical implications. It has been argued that the concept is largely developed by the practitioners, businessmen, policymakers, and consultants, while the theoretical aspect of circular economy remained unexplored and unattended. Nonetheless, CE draws it theoretical understanding form the ecological economic system which is attuned to the recycling of products.
Environmental pollution
Last year, the COPE conference was held from November 16 to 18 in Egypt where 198 countries gathered to discuss one of the biggest environmental challenges of climate change in the recent times. The five major issues discussed during COPE were nature, food, water, industry decarbonization, and climate adaptation. In recent times, we have seen some serious concerns from the governments around the world and the UN about the climate change and its negative implications for human beings. A number of movements have been launched to address the issues related to climate change and environmental pollution. Scholars, practitioners, governments, NGOs, and many other bodies agreed that environmental pollution is a serious threat to humanity and is emerging as a major health issue in the recent years. WHO called environmental pollution as a “silent killer” as it damages unnoticeably which can go beyond the estimates. Surveys and various studies by the WHO and other organizations show that environmental pollution is a major cause of death, especially in newborns in African and South Asian regions. WHO further reported that 90% of the global population is not able to get clean air to breathe and in 2015, 4.2 million deaths were reported around the world because of environmental pollution and another 100 million deaths are expected to be caused annually along with disability issues. The European Environmental Agency (EEA) observed that environmental pollution is a common problem worldwide and a bad atmosphere at one place can impact the neighborhood. For instance, the agents which cause environmental pollution travel faster in the air from one territory to another. Similarly, industrial waste of one country easily pollutes the water in the adjacent country[ies]. Same is the case with the wildfire in different regions and the environment polluting agents travel through air and reach the distant areas, thus causing various diseases especially related to the respiratory system, such as asthma. Other sources causing environmental pollution agents to travel are dust storm, ozone concentration, burning of industrial waste and drugs, pollen, etc. Pollen allergy is a common disease caused by air-polluting agents. Studies have found that there exists a relationship between the production of air-polluting agents and the inhabitants of a certain region with respect to the workplace setting. For example, the movement of workers from rural areas to the factories in the urban area might commute the infecting agents. The movement from rural to urban areas for the economic opportunities thus enhances industrial activities and emission of industrial waste into air, consequently damaging the environment. Additionally, change in living patterns and lifestyle, especially when people prefer indolence at home or stay longer at offices, results in indoor pollution.
Liu and Lin (2019) argued that environmental pollution in China is directly related to the industrial structure which is heavily mechanical and coal based. In earlier studies, the major factors identified as causes of environmental pollution include investment in research and development activities, foreign direct investment, and technological development (Lau et al. 2014). Urbanization has brought the socio-economic growth but at the same time it has hasten the consumption and misuse of limited natural resources which has triggered environmental pollution at larger scale (Wu et al., 2014). The continuous growth in urban population resulted into a number of environment-related issues like carbon emissions, industrial pollutants, smoke and dust, industrial solid waste, and pollution in the atmosphere due to fuel consumption. These environmental pollution-related issues have burdened the economies of various countries and the governments have started taking initiatives of green economy, sustainable development, and newer housing policies to lessen the burden on cities and to conserve the resources (Yang & Peng, 2017). In recent years, the development of smart cities and ecological societies is being promoted. However, it is not sufficient to take practical steps only to address the issue of environmental pollution, but there is a need to initiate the research efforts across the disciplines to better address the challenges of environmental pollution (Acuto et al., 2018).
Waste Management Theory
The dawn of the nineteenth century brought with it the technological revolution and a lot of research across various scientific disciplines. With the development of information technology, the availability of luxurious electronics reached millions of people and their usage resulted into different areas to be dealt with by the scientist, legislators, and environmental bodies. This technological development probably ignored the need for parallel advancement in environmental science. Technology[ies] continued to develop, and products evolved without considering the manipulation and depletion of materials and other resources. No attention was paid to “reuse” and “recycling” of the products and materials. This resulted into mass generation of electronic waste because electronic products were not designed keeping in view the reuse and recycling. This arises the need for proper legislations to deal with the issue of [electronic] waste. However, only legislation is not enough as there seems to be a wider gap between science and technology which needs to be filled with the development of more sophisticated technical theories.
Waste management theory accomplishes the same purpose and has been designed to help scientists and technologist address environmental issues during product design, i.e., engineering design. Waste Management Theory (WMT) provides a comprehensive and deeper theoretical understanding of the waste and waste management. The theory is aimed to accumulate and organize the variety of variables relevant to the waste management. WMT has emerged from the field of industrial ecology and it has been gradually building on other related theories, for instance, the design theory. It is a relatively recent approach which provides useful insights into the development of other technical theories. Hempel (1966, 1965) argued that the purpose of any scientific theory is to provide an explanation of a system of regularities which otherwise is difficult to explain through scientific laws. The basic purpose of WMT is that it defines the term “waste” clearly. The issue of defining “waste” surfaced during the conference of European Commission and Member States in Leipzig in early 2004. The participants were of the opinion that it is important to define “what constitutes ‘waste’ and what does not?” It was important to define and classify the waste treatment. WMT suggests that there are four classifications of “waste.” The first class consists of the things and materials which are not required—created without any purpose. The second class contains those things and materials which can be used for a limited time and afterwards they become useless. The third category constitutes the products and materials with specific purpose, but their performance has decreased from the required performance standards because of flaws in their design. The last category consists of products and material which have been designed for a definite purpose and have acceptable performance standards but are not used for their intended purpose.
The above classifications of waste help us to identify wastes according to the class they belong to and then suggest appropriate treatment for operation. For example, reuse of a product happens when it has met the purpose assigned and a new purpose is assigned to it. A product which has fulfilled its purpose is not necessarily considered waste because it can be used for other purposes. This means that “being waste” is dependent on the structure and design of a product not on the purpose of the product. As long as the design of a product allows it to be used for other purposes, it cannot be considered “waste.” An empty bottle of “coke” is not a waste until its structure allows to be used for a variety of other purposes (water, juice, petrol, etc.). Same is the case with the equipment and vehicles. They cannot be considered “waste” when they reach their end of useful life. The replacement and repair of faulty parts can extend their life and make them useful beyond the designated useful life. WMT has been developed under the umbrella of industrial ecology (IE). The principles of ecology suggest that industries should avoid the use of toxic materials in product design and development and products must be designed in a way to preserve the utility of materials used in products. IE principles further argue that industries need to obtain required maximum material through recycling and the products should be designed in a way that at the end of their life they can be productive and useful for other purposes. Industries should design their operations in ways to minimize the hazardous effects on the natural resources and the environment. Industries also need to build closer networks with suppliers and consumers, and local and other legislative authorities to minimize the packaging, develop eco-friendly packaging, and encourage the reuse and recycling of products and materials. IE asks for designing the products keeping in view the dual purpose of product competitiveness and environment friendliness. Product design and entire manufacturing process should be aligned with the environmental goals. An understanding and application of WMT is instrumental in optimum use of resources. The notion of optimum resources utilization is derived from the paradigm of IE. In addition to the concerns of IE, WMT also takes into account social concerns related to morals and responsibilities and thus derives its tenants from social theory as well. The existence of “real world” cannot be overlooked and human needs and expectations must be incorporated into the objectives of WMT. Scholars are of the view that WMT is not mature yet and new realities, facts, and observation must update the continuous development of WMT.
To develop an effective waste management system, there is a need for the theoretical understanding of waste-related issues to which is sufficiently addressed by WMT. For the understanding of the scientific system and the establishment of an explanatory model to gauge the problems of waste management, a theory is prerequisite. Though the WMT is built on the notion of IE, a consideration of the other relevant issues (social and environmental) is important for enriching WMT in order to attain the agenda of sustainable development. The WMT is built on the principles of prevention and effective management of waste that can help avoid the harm to humans and environment and aid to conserve the resources for future generations. There is a need for continuous research efforts to further develop WMT and to incorporate environmental concerns into industrial processes and design.
COVID-19
The outbreak of a pandemic is not a novel phenomenon in the human history. A number of pandemics have been reported in different regions at different times causing loss of thousands of lives along with myriads of social and economic consequences. For instance, Plague of Athens 430Mbc, Antonine Plague AD 165–180, Plague of Cyprian AD 250–271, The Black Death 1346–1353, Great Plague of London 1665–1666, Spanish Flu in 1918–1920 at the end of the World War I (affected the young people mostly between the ages 15 and 45), smallpox pandemic in North America during 1775–1782, Swine flue 2009–2010, West African Ebola 2014–2016, and Zika virus 2015 to date are just few of the horrific instances that humans have faced. The recent outbreak of COVID-19 is addition to this long list of pandemics. Before COVID-19, the Spanish Flu was considered the last of the deadliest pandemics which affected around 500 million people and caused 50 million deaths around the affected regions. The medical scientists are of the view that COVID-19 is among the deadliest pandemics witnessed so far. According to WHO as of January 5, 2023, the total number of confirmed COVID-19 cases is more than 650 million; more than 6 million deaths have been reported since it began. Europe is the most affected region with more than 270 million confirmed cases followed by America (186 million), Western Pacific (107 million), Southeast Asia (60 million), East Mediterranean (23 million), and Africa (9 million). The novel coronavirus is highly contagious and easily transmittable which makes it even more harmful.
Medical research reveals that there are numerous types and numbers of viruses which are from the coronavirus family and there are only few which cause respiratory issues in humans. Among these two widely known viruses, i.e., sever acute respiratory syndrome coronavirus (SARS-Cov) and Middle East respiratory syndrome coronavirus (MERS-Cov) were reported in November 2002 and September 2012 respectively. These were reported to be transmitted from animals to humans, causing complex respiratory issues and deaths. In December 2019, a novel type of coronavirus was identified and reported in the city of Wuhan, China, when a number of people were rushed to hospitals with respiratory issues due to unknown reasons. The virus was named as novel severe acute respiratory syndrome coronavirus-2 (SARS-Cov-2). Over the next few weeks, the virus spread to 18 more countries and on January 30, 2020, WHO declared COVID-19 as Public Health Emergency of International Concern (PHEIC). Later on, the virus spread to 113 countries with rapid speed affecting more people, especially the elderly people and taking big toll on human lives in various countries. WHO prognosticated it as a serious health risk and threat to humans and on March 11, 2020, WHO declared it a global pandemic and asked for more aggressive initiatives to curtail the spread of the virus. Due to unprecedented speed and unpreparedness of the hospitals, the virus proved to be more harmful not only taking toll on human lives but also incurred massive financial losses. In addition to the health issues, COVID-19 also resulted into number of psychological social and economic problems and challenged the intellectuals, policymakers, and other stakeholders to seek saner ways to address the situation. A series of initiatives were taken yet the spread of the virus badly exposed the loopholes in the healthcare facilities across the globe. Unavailability of medical treatment, less space in hospitals, absence of vaccine, lack of trained medical workers, and international travel were the major reasons which accelerated the pace of COVID-19. It took more a year when the first vaccine Pfizer BioNTech was prepared and WHO allowed it for emergency usage. Before the arrival of vaccines, WHO advised for personal protection and other measures such as wearing masks, social distancing, and quarantine arrangement. Once vaccines arrived, countering propaganda against it was another difficult task as people were hesitant to inject vaccines.
Though the efforts to curtail COVID-19 have been successful, recent re-emergence of viruses in China has alerted the authorities to go for extraordinary efforts. The world is facing a constant medical emergency due to the upsurge in COVID-19 cases from time to time. Recently reported new variant “Omicron” in some countries means that the virus is extremely smart and yet these countries are not fully guarded against the disease. Many of the countries are still in emergency situation and preventive measures like social distancing and isolation which pose multiple mental health and psychological issues (Ribot, Chang, & González, 2020). According to the reports of different health organizations, such as The Pan American Health Organization (PAHO) and Global Health Council (GHC), the Delta variant of coronavirus is the most widely spread and transmittable among all other variants.
The World Health Organization emphasizes on widespread vaccination campaigns to counter propaganda and increase public awareness to effectively curtail the virus transmission of COVID-19 (Romero et al., 2021; Wang et al., 2021). Different variants of coronavirus have been identified in different countries since the occurrence of the pandemic; the Delta variant was first reported in India and then transmitted to the USA. Similarly, the newly reported variant Omicron is spreading rapidly across different countries and is found to be more contagious than Delta. However, with the availability of various vaccines and their administration to a large portion of population, these variants are now less mortal and the psychological impact has been dampened. Medical scientists are positive that timely identification of various emerging SARS-Cov-2 variants can help develop the medical treatment and other non-medical measures to curtail their spread and transmission (Dong, 2021).
Current state of the art of circular economy for medical research
WHO recommended that health waste should be placed in containers and unique bags as more than its infectious nature waste can exacerbate climate change and environmental pollution. Thus, treating and destroying medical waste are a critical need (Pandey et al., 2020). Many countries focus on medical waste treatment by handling it quickly, tidily, effectively, and harmlessly (Manupati et al., 2021). To this end, an enormous stream of research and empirical contributions have been shown on the best hospital waste disposal practices (Kandasamy et al., 2022). Many studies focused on a single company (e.g., Despeisse et al., 2012; Huysman et al., 2017; Akanbi et al., 2018). Most of the studies that focused on industries of developed countries have not fully provided a comprehensive understanding and conclusive evidence of the effects on the environment in this context. Rolewicz-Kalinska (2016) investigated the logistical issues of hospital waste management and suggested short- and long-term solutions. According to Devi et al. (2019), proper hospital waste management reduces health risks and mitigates environmental damage (Singh et al., 2021).
The inefficiency of the medical waste management system is exacerbated by factors, such as incorrect use of funds, a shortage of funds, overbuying of pharmaceuticals instruments, poor logistics, carelessness on the part of the staff, and a general lack of knowledge (Wei et al., 2021). Minoglou et al. (2017) investigated the impact of medical waste on economic, social, and environmental parameters. In this context, many factors were found exacerbating the problems of improper management of medical waste. Tabash et al. (2016) proved that the lack of professional and systematic training of healthcare workers affects medical waste management. Few previous studies have utilized the concept of circular economy for medical waste treatment. The challenges of adopting a circular economy in medical waste management were identified. Reprocessing and lack of infrastructure are among the biggest challenges to hospital waste management (Kandasamy et al., 2022). The COVID-19 epidemic has made it difficult for governments to control medical waste. This is the reason they completed a state-of-the-art assessment to identify difficulties in managing medical waste both during and after COVID-19 (Felix et al., 2022; Mahyari et al., 2022; Nandy et al., 2022; Ranjbari et al., 2022). Previous literature adopted MCDM methods to design effective medical waste disposal systems. A dynamic multi-objective immune system has been used to improve the performance indicators of wastewater plants (Li et al., 2021; Jafarzadeh Ghoushchi et al. 2022). In order to compensate for the drawbacks of failure modes and the impact analysis approach, we implemented a multi-objective optimization using ratio analysis in the domain of spherical fuzzy sets. In addition, a multi-criteria evaluation model based on type-2 neutrosophic numbers was adopted to assess the factors causing the failure of blockchain and IOT adoption for medical waste management (Torkayesh et al., 2021).
According to our knowledge, the scarcity of literature in ranking hospitals on the basis of medical waste and proposing the best circular economy method for removing hospital waste would render the results of the previous literature inconclusive. This lack stimulates research in targeting several sectors and industries in developing countries, making the results more generalizable and decisive (Laso et al., 2016; Kirchherr, Reike, & Hekkert, 2017; Nandi et al., 2021). Furthermore, there is an apparent lack of literature on merging the medical waste problem during the coronavirus pandemic with the circular economy to mitigate the effects of healthcare waste on environmental pollution and climate change. Therefore, by closing the loop, the circular economy contributes to the development of products in many industries. The adoption of the MCDM approach has been increasing in many aspects. For instance, it has been used in the electrical and renewable energy sectors (Ecer, 2021) and transportation sectors lately (Lin et al., 2020) as well as in online commerce in order to recommend the most appropriate products for customers (Bączkiewicz et al., 2021; Tirkolaee & Aydın, 2021). Since medical waste treatment significantly affects many healthcare stakeholders, the MCDM approach has been considered effective in addressing medical waste issues by opting it for healthcare suppliers (Stević et al., 2020). Besides, MCDM methods are also adopted to determine the best way to help physicians expedite the treatment of COVID-19 (Albahri et al., 2020).
On this basis, this study attempts to bridge the gaps found in the literature. The current research is in line with the recent trend to address a critical problem that resulted from the emergence of the COVID-19 epidemic. Among the opportunities available, multiple and diverse industries will give this study more accurate results and further possibility of adding implications for theory and practice. Besides, discussing the economic importance of the topics under study at the national and company levels will benefit academics and practitioners. According to the accumulated medical waste, the rank of hospitals is critical for many governments when choosing an appropriate method for removing hazardous medical waste based on the weight assigned through the ANN method (Kargar et al., 2020; Liu et al., 2021).
Medical waste management
Efficient waste management is vital to the development of societies in developing countries (Kandasamy et al., 2022). The increasing global economic growth has naturally expanded the need for medical equipment in line with the expansion of healthcare systems. As a consequence, the continued use of medical equipment and tools increases medical waste (Singh et al., 2021). The medical waste consists of 67% of general waste (e.g., food and others), 27% of infectious or toxic waste from pharmaceutical and pathological waste, and nearly 4% of sharps and contraptions such as syringes and scalpels (Klemeš et al., 2020; Singh et al., 2021). Expired medicines, chemicals, disinfectants, dressings, caps, sharps, and needles also constitute medical waste (Rolewicz-Kalinska, 2016). Healthcare organizations naturally generate medical waste because of treatment, medical diagnosis, or other medical activities. Healthcare waste may be toxic or infectious and cause diseases (Windfeld & Brooks, 2015; Ibn-Mohammed et al., 2021; Kumar et al., 2021). Inefficient removal of medical waste affects climate change, increases greenhouse gas emissions, and affects community health (Kandasamy et al., 2022). Consideration of the sustainability elements in managing medical waste is a critical issue in mitigating environmental pollution and health damages (Babaee Tirkolaee & Aydın, 2021). With the spread of the coronavirus pandemic, the risk of contagiousness caused by medical waste has increased. Medical waste disposal has become a critical challenge because failure in its disposal can threaten human lives (Chauhan et al., 2020). The trash included PPE such as gloves, masks, medical garments, testing, sampling tools, and vaccines. Healthcare equipment is considered a critical way of spreading the disease (Krishnan et al., 2021; Mekonnen et al., 2021) due to the increased demand for personal protective equipment for physicians, nurses, and all other health workers. Thus, used PPE and its associated devices are dangerous because they contain polymers, bacteria, and viruses (Parashar & Hait, 2021). The generated waste from health facilities is also considered hazardous and can be a vector for causing COVID-19 (Ilyas et al., 2020). Hence, the appropriate management of this waste is essential to deter the spread of the epidemic. Sustainable medical waste management would reduce improper medical health management (Kandasamy et al., 2022).
Circular economy in the medical system
Healthcare waste should be disposed of immediately, and special care is needed during disposal operations (Kulkarni, & Anantharama, 2020; Mekonnen et al., 2021). Empirical evidence confirmed that the circular economy is a systematic and vital approach to mitigate the impacts of medical waste on population health, environmental pollution, and climate change (Ma et al., 2020). It is defined as the effective participation of the economy in the production process to expand the productive culture and achieve sustainable production (Korhonen et al., 2018). It allows the use of material more than once because it deals regenerated waste as a new raw material. The circular economy operates on societal and industrial systems and contributes in environmental friendly development (Korhonen et al., 2018). The COVID-19 pandemic caused significant disturbances which led to the deterioration of social and economic life and disruption in supply chains and financial markets. These issues decreased overall efficiency and created a need for recycling under the circular economy precepts (Neumeyer et al., 2020; Singh et al., 2021). Reusing many medical tools and devices will lower discard and destruction costs. In addition, getting rid of waste also reduces the spread of the epidemic (Van Straten et al. 2021; Ibn-Mohammed et al., 2021). Creating a closed loop for materials will significantly enhance organizational effectiveness (Fregonara et al., 2017; Han, Liu, Liu, & Cui, 2017). The effect of COVID-19 on health infrastructure and waste treatment was significant because it caused health risks and escalated the spread of coronavirus (Sarkodie & Owusu, 2020). The medical tools of COVID-19 led to a rise in hospital waste management system problems (Huysman et al., 2017). As a result, waste recycling could innovate current products to reach sustainability through the circular economy perspective (Vanapalli et al., 2021).
Several businesses have embraced circular economy in order to reduce waste. They have been aware of the fact that adopting the circular economy perspective contributes to the development of many emerging industries and sectors (Amicarelli et al., 2021; Chirani et al., 2021). Recycling and reusing organizational resources are a vital issue for the survival of organizations as modern organizations are attempting to replace the linear concept with the circular one (Sassanelli, Rosa, Rocca, & Terzi, 2019; Lal et al., 2020). Several examples of the implementation of the principles of circular economy are obvious such as in construction and building industry (Akanbi et al., 2018; Mohammad et al., 2019), water and environmental sustainability (Angelis-Dimakis et al., 2016), electrical equipment or electronic waste (Awasthi et al., 2018), and transportation sector (Berzi et al., 2016; Delogu et al., 2017). The circular economy mainly contributes to two important aspects: the first is to reduce costs by reusing resources or production tools in the best possible way to achieve economic benefits for organizations in the short term; secondly, the circular economy contributes to sustainability in the long term (Despeisse et al., 2012; Awasthi et al., 2018). The benefits of a circular economy include achieving sustainability, reducing overall costs, and environmental improvements (Eastwood & Haapala, 2015). The circular economy is related to the economic, environmental, and social aspects, and integrating such dimensions in product development or innovation processes is widely desired (Favi et al., 2017; Fregonara et al., 2017). Additionally, the circular economy creates value for materials during the last stage of the resource life cycle (Franklin-Johnson et al., 2016; Favi et al., 2017). Figure 1 illustrates the basic principles of circular economy for mitigating and disposing of the hospital waste (Teymourian et al., 2021).

Key concepts of a circular economy for medical waste disposal
-
1.
Incineration technique: It disposes of medical waste and converts it into energy based on level of temperature to kill bacteria and viruses.
-
2.
Pyrolysis technique: Pyrolysis operates on a temperature range of approximately 540 to 830 °C and includes induction-based pyrolysis, laser, and pyrolysis oxidation.
-
3.
Microwave technique: Microwave disinfection works by adopting electromagnetic waves with wavelengths ranging from approximately 1 to 1000 mm. Such technology helps reduce energy consumption, increase heat productivity, and reduce toxic waste.
-
4.
Autoclave chemical technique: Autoclave chemical technique works on heat and uses water vapor for sterilization. Water vapor releases heat that kills viruses and bacteria and eliminates medical waste.
-
5.
Vaporized hydrogen peroxide: Disinfection for used devices (such as respirators) to eliminate bacteria and viruses.
-
6.
Dry heat: The temperature is at 60 degrees for not less than 30 min, causing structural damage that prevents cell attachment.
-
7.
Ozone: Ozone works to disrupt oxidation by exposing the essential embryonic materials in its shell and breaks down the proteins and fats it contains.
-
8.
Ultraviolet light: The radiation that damages molecules and destroys the DNA of viruses with a photodimerization procedure.
Methodology
Consistent with the study’s aims, we will first attempt to sort the types of medical waste and match them with hospitals which will be followed by a weight assigned to each type of medical waste. According to the assigned weight, a benchmark will be proposed among hospitals based on medical waste generation. Finally, the study suggests the best ways to treat medical waste using the ANN approach. Classifying hospitals based on the generated clinical waste is a multipart process that must be resolved. According to the literature, MCDM methods are considered effective also in the healthcare sector. MCDM is the fastest-growing method of problem-solving in multiple disciplines under uncertainty (Triantaphyllou, 2000; Weistroffer & Li, 2016; Krishnan et al., 2021).
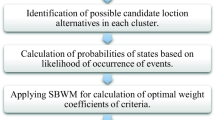
MCDM methods are divided into two types. The first is to assign the weight, and the second is to rank the alternatives. For weight methods, there are many types, such as Analytic Hierarchy Process (AHP), Best Worst Method (BWM), Fuzzy Weighted with Zero Inconsistency (FWZIC), and Analytic Network Process (ANP). The AHP method is commonly used, and it is in fact the first method which found support among scholars to assign weight to criteria (Albahri et al., 2020; Alsalem et al., 2022). The literature review suggested that researchers in the past adopted many methods such as VIKOR, multi-objective optimization based on ratio analysis (MULTIMOORA), and Fuzzy Decision by Opinion Score Method (FDOSM) to rank the alternatives (Khaw et al., 2021). Nevertheless, the LDFN-FDOSM method has been confirmed to outperform existing MCDM ranking techniques (Albahri et al., 2022a; Narayanamoorthy et al., 2022). Consequently, the methodology was implemented in three phases. Firstly, the decision matrix phase proposal involves hospitals (alternatives) and the five critical concepts for waste types. Secondly, the development phase explains the integration of AHP and LDFN-FDOSM methods. Thirdly, the ANN method recommends proper medical waste disposal based on the hospital’s ranking. Figure 2 shows the recommended solution for this study.

An intelligent medical waste management framework
Proposal of decision matrix phase
At this stage, two main steps need to be defined: (1) pre-processing for the five fundamental medical waste types, and (2) hospital (alternatives) concepts. To this end, this section discusses and proposes matrices for assessing hospitals according to medical waste types, and creates two decision matrices. Each decision matrix is a cross between alternatives and criteria. As previously mentioned, five main types of medical waste have been identified (Mekonnen et al., 2021):
-
1.
General waste: The result of the most significant percentage of waste produced by health activities.
-
2.
Sharps waste: This waste includes sharps often used in surgery, being dangerous and must be handled with care.
-
3.
Pharmaceutical waste: This waste comes from medicines, vaccines, and plastic containers that may be infectious.
-
4.
Infectious waste: This waste comes from items used for prevention while dealing with pathogens (e.g., gloves and masks).
-
5.
Pathological waste: Comprises the hazardous waste generated in hospital halls, especially for gynecological diseases.
These five fundamental concepts of medical waste types (criteria) allow the assessment of hospitals in the aftermath of the COVID-19 pandemic. This study underlines the disinfection technologies for waste infected by coronavirus 2, such as incineration technique, autoclave chemical technique, microwave technique, pyrolysis technique, vaporized hydrogen peroxide, dry heat, ozone, and ultraviolet light. By matching the hospitals’ ranking based on medical wastes and disinfection technologies for coronavirus 2–infected wastes, the study attempts to overcome medical waste disposal challenges and issues. As discussed in the following section, the intersection between the identified alternatives and criteria created a decision matrix which is presented and discussed.
Decision matrix
As can be seen in Table 1, the decision matrix was constructed using the crossover of a set of hospitals representing the alternatives and a set of five criteria representing different categories of medical waste.
Ten hospitals in Iraq that showed excellent performance during the COVID-19 pandemic were targeted. Managers with long experience in medical waste disposal were selected to obtain data. The data collection process lasted about a month through a questionnaire prepared to identify and sort the kinds of clinical waste. Table 1 shows the study results of medical waste during the coronavirus disease outbreak. Hospitals have stocked common trash along with hazardous waste. Based on the global reports about healthcare in Iraq, there were no designated waste storage areas in the investigated hospitals. In addition to the administrated questionnaire, online interviews were performed with inventory managers that work in the ten investigated hospitals. The interviews provided complementary information to fill the first matrix data regarding the volume according to the types of medical waste. Table 2 shows hospitals’ characteristics.
Results showed the capacity of the investigated hospitals, where the Baghdad Teaching Hospital (Baghdad Medical City) has the highest capacity. At the same time, Central Children Teaching Hospital, Ibn Al-Baladi, Al-Imam Ali, Al-Kindi Teaching Hospital, and Al-Shaheed Al-Sadr General Hospital have the lowest capacity. The hospitals have a high degree of generated medical waste. Therefore, there is a critical need to determine the appropriate method to dispose of medical waste. Table 3 illustrates the decision matrix of disinfection technologies for coronavirus 2–infected wastes.
Table 3 shows the disinfection technologies that will be weighed using ANN. The classification of the hospitals relied on integrating LDFN-FDOSM and AHP based on medical waste types.
Development phase
Weighing and ranking MCDM methods must be addressed to develop a dynamic hospital approach. The weighing method was achieved using AHP, while LDFN-FDOSM was used to rank the alternatives (Albahri et al., 2020; Albahri et al., 2022a; Narayanamoorthy et al., 2022).
AHP for weighting criteria
This part focuses on applying the AHP for weighing criteria (Tirkolaee et al., 2019).
-
Step 1: The hierarchy contains the decision matrix and the conditions in each decision matrix. This procedure is adopted to establish the connection between the criteria in the decision matrix of the hospitals.
-
Step 2: The AHP builds a pairwise matrix comparison using Formula (1) to locate a weighing decision:
$$A=\left(\begin{array}{ccc}{X}_{11}& \cdots & {X}_{1n}\\ {}\vdots & \ddots & \vdots \\ {}{X}_{n1}& \cdots & {X}_{nn}\end{array}\right)$$(1)\(\mathrm{Where}\ {X}_{ii}=1,{X}_{ii}=\frac{1}{X_{ij}}\).
-
Step 3: This stage clearly shows the questionnaire’s design to the parameters for each judgment matrix of the hospital’s prioritization and according to the experts’ perceptions (for more details, check “Weight determination using AHP”).
-
Step 4: At this step, each element in matrix A (1) is standardized to construct the normalized matrix Anorm, Anorm (aij) as follows.
$${a}_{ij}=\frac{X_{ij}}{\sum_{i=1}^n Xij}$$(2)$${A}_{\mathrm{norm}}=\left(\begin{array}{ccc}{a}_{11}& \cdots & {a}_{in}\\ {}\vdots & \ddots & \vdots \\ {}{a}_{n1}& \cdots & {a}_{nn}\end{array}\right)$$(3)where A (xij) is given by Eq. (2).
-
Step 5: This phase includes AHP pairwise analysis using statistical equations, translating decisions, and assigning weights for each prioritization in the decision matrix.
$${W}_i=\frac{\sum_{j=1}^n{a}_{ij}}{n}\ \mathrm{and}\ {\sum}_{j=1}^n{W}_i=1$$(4) -
Step 6: This step checks the consistency ratio (CR) to the pairwise comparison matrix.
$$CR=\frac{CI}{RI}$$(5)$$CI=\frac{\lambda \max -n}{n-1}$$(6)$$RI=\frac{1.98\ \left(n-1\right)}{n} CI$$(7)To accept expert judgment, the CR value must be less than 0.1.
LDFN-FDOSM steps for prioritizing hospitals
The FDOSM method supports practitioners in making decisions with a high degree of certainty. In this context, a decision matrix is created, and after that, min, max, and critical values are determined, and the opinion matrix is generated. Furthermore, the opinion matrix is transformed into fuzzy numbers. Adopting the aggregation based on the arithmetic means helps in making the final decision.
This discussion presents the LDFN-FDOSM stages used in prioritizing hospitals on a medical waste basis. The first stage of LDFN-FDOSM is data conversion and the second stage is data processing.
The data was transformed by selecting the best solution based on three parameters: the critical, maximum, and minimum values. The critical value is considered the optimal solution; the minimum value is the cost of the criteria, and the maximum value is the benefit criteria.
Using a 5-point Likert scale, the significance of the differences between the perfect solution and the value of the alternatives is found.
where ⊗ symbolizes the comparison between the alternatives and the best solution. This operation creates an opinion matrix containing linguistic numbers. Using the LDFN fuzzy set, the matrix of linguistic numbers is converted to fuzzy numbers.
To convert the opinion matrix to ambiguous numbers, Table 4 displays linguistic terms and their corresponding LDFN.
According to Narayanamoorthy et al. (2022), the LDFN concerning linguistic terms were described based on intuitionistic fuzzy set. Therefore, the 5 Likert scale was employed to convert the linguistic terms into LDFN fuzzy set to produce the fuzzy opinion matrix. To aggregate the value of each alternative, the aggregation process has been used after completing the fuzzy decision matrix. Defuzzification phase has been accomplished to arrive at the final scoring rate and rank for each alternative. Hence, the highest score is considered the best alternative.

Artificial neural network
ANN approach deals with linear and non-linear interactions. ANN is a parallel distributed processor made up of processing units with a neural bias toward storing data. The simple units are nodes or neurons, similar to human neurons, preserved and retrieved by ANN through learning procedures in the communication weights of neurons (Féraud & Clérot, 2002). Multiple layers were adopted using the Feedforward-Back algorithm. Regarding error signals recorded, the reverse direction technology was used, and it includes three layers which are input layer, hidden layer, and output layer. Inward signals are fed forward order. Furthermore, there is an interconnection between the neurons of the other layers with each layer of neurons.
The movement is nourished onward through the hidden layers from input to output (Leong et al., 2020).
And for the kth output neuron:
The color space of a function with a real-world x-function ranging from 0 to 1 (that is, a monotonic and differentiable increase) is processed with the aid of a parameter. Equation 14 applies the weight modification procedure to the final layer weights V; Eq. 15 extracts the weights from the hidden layers. The dpk reflects the desirable result from neuron-k, while opk symbolizes the actual results of neuron-k of the input type. Weight values are reduced to try to minimize the square of the sum of the SSE (Eq. 17) across training modes.
Results and discussion
This part introduces the discussion on ranking hospitals according to medical waste types for COVID-19. “Weight determination using AHP” describes the weight assignment of the estimate criteria for the decision matrix by adopting the AHP method. In contrast, “Prioritization of hospitals using the LDFN-FDOSM method” exhibits the ranking of hospitals with the LDFN-FDOSM method.
Weight determination using AHP
In this part, we offer the evaluation score of measurement weights for each decision matrix used to rank hospitals by medical waste. Besides, it explains the AHP result for the assigned weight to the medical waste types.
Three experts with experience higher than 20 years in matters related to medical waste were requested to complete the assessment and preferences processes. These experts measured multiple standard levels through comparison questions. These questions were reassigned twice among experts as the first round presented the problem of inconsistency in the experts’ answers. Table 5 displays the weights scores for the three experts related to the multiple criteria for each decision matrix.
Table 5 shows the criteria used by experts for ranking hospital’s priorities. The experts’ relative importance ratings for different criteria varied. All experts assigned the most significant weight to pharmaceutical waste; in contrast, general waste took the lowest weight. Moreover, the consistency ratio results indicate the weighting result of the criteria extracted from all experts has acceptable values because the value was less than 0.1.
Prioritization of hospitals using the LDFN-FDOSM method
To determine which hospitals should immediately receive direct interventions to treat medical waste, these hospitals should prioritize hospital waste during the coronavirus epidemic. As mentioned in Section 3.1.2, the LDFN-FDOSM method has been used to prioritize different hospital levels during the coronavirus outbreak. The results and discussions were explained individually because the matching rate between hospitals was 100%. Hence, the need for grouping MCDM is considered worthless.
Individual LDFN-FDOSM prioritization for the investigated hospitals
This section presents LDFN-FDOSM-based hospital individual decision-making context results using the weight specified for assessment criteria derived from expert opinions (“Weight determination using AHP”). The results of priority ranking for hospitals are shown in Table 6.
Table 6 shows that hospitals were prioritized according to Q value in ascending order. According to all experts, hospital 6 ranked the best of the ten hospitals with a score of 0.925 followed by hospital 9 with a score of 0.879, while 0.894 and 0.887 for the first, second, and third experts, respectively. While hospital 1 was the worst with a score of 0.596 for all experts. In short, there is no unanimity among the experts involved in determining the rank of hospitals. Furthermore, all the experts assigned unique rankings across all the hospitals. Since there existed such a variety of ranks among hospitals, a unified ranking based on group decision-making is important to solve the variance problem in order to provide powerful evidence for academics and policymakers, as illustrated in Table 7.
In short, there is agreement among the experts involved in determining the weight of types of medical waste during COVID-19 since their weights for criteria of this level were close to each other. Furthermore, in the 1st scenario, the ranking between hospitals was 60% matched by the opinion of the experts. Hence, there is a difference between each expert and ranking hospital priorities. Given the sensitivity of the medical waste treatment procedure for COVID-19 according to the circular economy perspective, the benchmarking should be standardized for all hospitals to get more decisive results. Therefore, the group decision-making would provide powerful evidence for academics and policymakers, as illustrated in Table 7.
Table 7 provides insight into the ranking of hospitals based on medical waste production. Hospital 6 ranked in first place with a score of 0.940, followed by hospital 9 with a score of 0.890, and hospital 7 with a score of 0.861 emerged third in rank with the lowest production of medical waste, while hospitals 8, 5, and 1 occupied the bottom of the ranking with a score of 0.785, 0.836, and 0.590, respectively. The combination of the AHP with LDFN-FDOSM method provided insight into the hospitals with an environmental impact. Nevertheless, the issue of proposing a solution for the treatment of hospital waste on the basis of production is a critical issue. After getting the result of the group decision-making (GDM), this result should be evaluated for stability using the systematic ranking (evaluation) given in the next section.
Sensitivity analysis
Hospitals were prioritized and then split into three groups to verify the findings of the group prioritization process for each scenario. Several hospitals make up each group inside each tier. Depending on the situation, each group contains fewer or more hospitals vis-a-vis other groups. The number of subgroups inside each subgroup will not have any effect on the validation outcomes. However, the latter group should have the most prominent or equal number of hospitals compared to the others. The statistical approach (i.e., the mean) was calculated for the grade information of the priority hospitals to ensure the priority hospital group was subject to systematic ranking (Eq. 18).
The first group should achieve the highest value which should be proved when taking measurements of the average. The average of the first group must be higher than the second group. However, for the second group, the scores for the mean must be more than the third group. In terms of the third group, the average should be less than those in the first group and second groups. The results of the verification are shown in Table 8.
In the validation, the comparisons were made for every hospital. Based on the validation outcomes, group 1 is superior to groups 2 and 3. This is due to the fact that the LDFN-FDOSM method’s normalization methodology has broadened the data range of each hospital in the bottom-up phase, thus causing the mean value to be the greatest. To authenticate the significance of the proposed method, the sensitivity analysis predicts the impact on the ranking results of the hospitals with changing criteria weights. To start, the most important criterion should be identified for the purpose of analyzing sensitivity. Pharmaceutical waste was the most important consideration for all criteria listed in Table 9 in this research.
Experimentation with different weights of criteria was done to figure out how changing the weights of criteria would affect the outcomes. The relative change for each criterion over the most important one (pharmaceutical waste) with respect to 1.3 is shown in Fig. 3.

Sensitivity analysis of the hospitals benchmarking
where \({w}_{z1}^{\ast }\) indicates the max criterion’s weight coefficient at its revised value. The considered criterion’s value is diminished by \({w}_n^{\ast }\). wn providing the initial value of the criterion under consideration. The maximum criterion’s initial value is shown in wz1.
Hospitals one, six, and nine remain at the same rank in all scenarios which are ten, one, and two respectively. Hospital 2 ranked fifth in all scenarios, except for the original and first scenarios where it was in the third rank. In addition, hospital 3 remained fourth in the original and first scenario but dropped to the sixth rank in the second to 10th scenario. Moreover, the fourth hospital ranked fifth in the initial and first scenarios but dropped to seventh in the remaining scenarios. Hospital 5 continued in the eighth place until the third scenario, after which it fell to the ninth place in all remaining scenarios. Hospital 7 raised to the 3rd rank from S2 to S10 and kept the sixth rank in the original and first scenarios. In contrast to the fifth hospital, the eighth hospital was in the ninth place until the third scenario, after which it takes to the eighth place in all remained scenarios. Finally, hospital 10 was in the seventh place in only two scenarios, but in the rest of the scenarios, it was in the fourth rank.
In general, there were no significant changes; almost every five to six scenarios were similar to one alternative; for example, in hospital 2, hospital 3, and hospital 4, there was a change in only 2 scenarios from 10 scenarios, and the rest is similar, while in hospital 1, hospital 6, and hospital 9, it was stable in all scenarios. Spearman’s rank is one of the most powerful techniques for determining the correlation between a set of variables. It measures the strength of the correlation between two variables. Spearman’s rho (Spears’ rho) is the correlation coefficient between two ranking random variables. According to importance, pro and con factors are ranked according to their relative size.
The results showed that hospitals had a high correlation, as shown in Fig. 4.

Rank correlation in ten scenarios
For the ranking of hospitals, correlation analysis results are shown in Fig. 4. The rank correlation is 0.818 in two out of ten scenarios (S2 and S3). The rest seven scenarios had rank correlation values of 0.806 for S4 to S10, and 1 for S1. The combination of the AHP with LDFN-FDOSM method provided an insight into the hospitals’ environmental impact. Nevertheless, the issue of proposing a solution for the treatment of hospital waste based on production is critical. This study adopted the non-linear and non-compensatory relationship method based on the ANN approach. The following sections explain the recommended solution.
The ANN model used the sigmoid functions to activate the concealed and results layers. Through several stages of the learning procedure, failures can be limited, prediction accuracy enhanced, and 90% allocated to training processes. The remainder of the samples were utilized for testing. The accuracy of the ANN model was evaluated by computing the square root of the RMSE error (Leong et al., 2020). The results of the ANN activation function are shown in Fig. 5.

The ANN model. Note: IT incineration technique, PT pyrolysis technique, MT microwave technique, AC autoclave chemical technique, VH vaporized hydrogen peroxide, DH dry heat, OZ ozone, UL ultraviolet light, HR hospitals rank, H hidden layer
The three experts’ responses were distributed using the 5-point Likert scale. Table 10 illustrates the artificial intelligence to identify appropriate technologies for the circular economy perspective for hospital waste removal according to the ranking of hospitals generated by MCDM. Table 10 shows the variable importance. Hence, the circular economy perspective was applied to recommend appropriate hospital waste removal techniques depending on the hospital ranking during the COVID-19 pandemic.
Hospital’s data shows that the ozone method has the highest weight, while the autoclave chemical technique heat and the dry heat methods receive the worst weight. Table 11 presents the parameter estimates. The hidden neurons of H (1:1) are the chief contributing neurons, while H (1:2) are the most inhibitive neurons; following is H (1:3).
Theoretical implications
The coronavirus outbreak has led to multiple health and environmental problems; for instance, medical waste has been exacerbated because of the increased use of PPE and other medical tools by the frontline health workers and people. Managing medical waste has been quite a big challenge for countries like Iraq, which lack strong medical infrastructure. This study has been conducted in the context of hospitals in Iraq and it seeks to theoretically understand the medical waste issue and medical waste management in a developing country. Though the issue has been studied in the developed countries (MacNeill et al., 2020), it has different dimensions in the context of Iraq. The study investigated the role of circular economy in dealing with the medical waste. There are indications that circular economy can address the medical waste issues and be relevant, especially in developing countries (Suárez-Eiroa et al., 2019). Similarly, discussing the circular economy from the perspectives of the COVID-19 pandemic has proffered exciting and essential results. Therefore, the results obtained in this research can benefit scholars in two ways. Firstly, this research provides insights to deal wisely with the economic aspect (ongoing expenses because of the reinvestment of waste and the sustainability of the supply chain) of the effects of COVID-19. Secondly, the results may encourage many projects and investments in medical waste recycling, which will create new job opportunities. The current study was complementary to a technical aspect of many studies that used circular economy in the light of the coronavirus epidemic (e.g., Teymourian et al., 2021; Ibn-Mohammed et al., 2021; Nandi et al., 2021). The current research contributes in terms of ranking and classifying the hospitals with respect to the volume and type of medical waste generated and thus bridges the gap mentioned in the preceding studies (e.g., Wuyts et al., 2020; MacNeill et al., 2020; Nandi et al., 2021). By classifying hospitals based on the generation of medical waste using LDFN-FDOSM and providing a solution about the best circular economy method for medical waste disposal by employing the neural network approach, this study contributed to the literature by identifying the best and worst circular economy method for medical waste disposal. It also contributed to the literature by adopting the MCDM approach based on the LDFN-FDOSM method and the non-compensatory relationships approach according to the ANN approach to provide an insight into the circular economy of medical waste in a novel context. This research involved integrating AHP, LDFN-FDOSM, and ANN methods to classify and select the best alternative for ranking hospitals. The ranking of hospitals is essential for many governments to choose a proper technique for the disposal of hazardous medical waste based on the weight of the medical waste disposal determined by the size of the collected medical waste through artificial intelligence.
Practical implications
This study bears practical implications for hospitals and policymakers in Iraq. Private and governmental hospitals in Iraq are still growing, and as a consequence, the amount of medical waste produced will rise in the near future. At the same time, the Iraqi Ministry of Health has set recommendations to ensure appropriate medical waste management. However, little commitment and will is shown in adhering to guidelines and health standards rules. Decision-makers disregard apathy toward practices for waste management exacerbate climate change and environmental pollution significantly (Mensoor, 2020). Hospital waste is thrown directly into the Tigris River, contaminating it with harmful chemical and biological toxins. This requires immediate attention to lower the amounts of such toxic chemicals in the environment. The situation is compounded by the fact that that medical waste gets mixed with general waste in the studied hospitals of Baghda to make the matter worst.
The main practical implication of this study is the development of a methodology for prioritizing hospitals based on the MCDM and ANN approaches. This methodology assists professionals in the hospitals to be specialized in medical waste disposal and be assertive in decisions when choosing the appropriate medical waste disposal technology depending on the hospital rank and the types of medical waste in the aftermath of COVID-19. This study adopted multiple decision-makers (experts) in selecting weights for evaluation criteria and standardized measurement. This study provides many benefits and practical implications for practitioners and scholars by designing an application to identify hospitals that are generating medical waste the most in the aftermath of the COVID-19 pandemic. Moreover, MCDM and ANN techniques were used to identify the suitable technology for each hospital according to the rank obtained from MCDM methods and improve the possibility of recycling medical waste. This study suggests an opportunity to reduce the time and costs of disposing of medical waste and determine the most appropriate method for each hospital during the coronavirus global epidemic. Scholars and policymakers can benefit from the intelligent framework developed by this study to overcome the challenges of climate change. This study provides a guide for the development of the most important criteria to be adopted to assess the sustainability of many hospitals. In addition, the study complements the findings of previous literature by providing insights to policymakers about the role of the circular economy in reducing waste and misuse of resources.
The study suggests some important research guidelines for future scholars. It is recommended for future research that the consideration of assortment of sectors will provide more precise results and improve theoretical implications. The study recommends that Iraqi government take rapid action to overhaul incinerators and replace them if need be for hospitals that have been destroyed (Falih et al., 2021; Hama et al., 2021). The Health Ministry must strive diligently to educate waste management workers in hospitals. Additionally, the Iraqi government should consider implementing stricter rules prohibiting improper storage or transportation of medical waste to reduce environmental pollution. Reusing and recycling resources can create more robust and sustainable supply chains and enhance the transition to a circular economy society, allowing further expansion and innovation of blockchain technology.
Conclusion
A recent study about the current challenges in medical waste management and future sustainable management by Singh et al. (2022) revealed that many countries worldwide are facing challenges of proper disposal and management of medical waste generated during the COVID-19 pandemic. The cost of managing medical waste is estimated to the tune of $17.89 billion, which was $11.77 billion in 2018. The outbreak of the COVID-19 pandemic has aggravated medical waste production and thus caused immediate issues of environmental pollution and human health crises. Previous studies showed that even before the outbreak of COVID-19, almost half of the world population was facing environmental pollution and health issues due to unsafe and improper medical waste disposal. Hospitals around the world needed novel medical waste management techniques in addition to the already available ones. One possible solution to the problem could be the recycling of medical waste, especially plastic materials used in packaging and personal protection equipment. Recycling and other green measures can ensure future sustainability. This study has focused on the medical waste generated during COVID-19 in Iraqi hospitals. MCDM methods were used to make choice of hospitals for this study based on the production of medical waste. By using the ANN method, we proposed few medical waste management and disposal techniques for the selected hospitals. Our study has provided a detailed account of various coronavirus disinfection techniques including incineration, pyrolysis, microwave technique, autoclave chemical technique, vaporized hydrogen peroxide, dry heat method, ozone, and ultraviolet light. We proposed LDFN – FDOSM methods for prioritizing hospitals which need immediate interventions for medical waste management. Our proposed novel intelligent medical waste management framework can help hospitals to redefine their waste disposal strategies and design them within the perspective of circular economy.
Like all other research studies, we submit certain limitations of our study. First, only three experts were involved in prioritizing the hospitals based on the LDFN-FDOSM method. We believe that inclusion of more experts could further refine the prioritization of hospitals. Secondly, the application of the proposed methods in other contexts may be varied due to contextual differences and we proposed the application of proposed methods to other contexts for robust results. Circular economy is an evolving concept in the field of medical waste management and hence, we recommend using the proposed methods for its effectiveness. This is one of the possible ways out that the damage caused to environment and public health by medical waste can be mitigated and governments and policy makers can seek help to devise environmental policies aimed at minimizing the greenhouse gas emissions.
Data availability
The data of the paper, which support the analysis and results of this paper, are available with the corresponding author and the data can be obtained from the authors upon request.
Change history
25 April 2023
A Correction to this paper has been published: https://doi.org/10.1007/s11356-023-27165-0
References
Abbas S, Al-Abrrow H, Abdullah HO, Alnoor A, Khattak ZZ, Khaw KW (2022) Encountering COVID-19 and perceived stress and the role of a health climate among medical workers. Curr Psychol 41(12):9109–9122
Abdulaali AR, Alnoor A, Eneizan B (2019) A multi-level study of influence financial knowledge management small and medium enterprises. Pol J Manag Stud 19
Abdullah HO, Atshan N, Al-Abrrow H, Alnoor A, Valeri M, Bayram GE (2022) Leadership styles and sustainable organizational energy in family business: modeling non-compensatory and nonlinear relationships. J Fam Bus Manag (ahead-of-print). https://doi.org/10.1108/JFBM-09-2022-0113
Aboramadan M, Alolayyan MN, Turkmenoglu MA, Cicek B, Farao C (2021) Linking authentic leadership and management capability to public hospital performance: the role of work engagement. Int J Organ Anal 29(5):1350–1370
Acuto M, Parnell S, Seto KC (2018) Building a global urban science. Nat Sust 1(1):2–4
Ahmed MG, Sadaa AM, Alshamry HM, Alharbi MA, Alnoor A, Kareem AA (2022) Crisis, resilience and recovery in tourism and hospitality: a synopsis. In: Tourism and hospitality in Asia: crisis, resilience and recovery. Springer, Singapore, pp 3–19
Aitken M, Ng M, Horsfall D, Coopamootoo KP, van Moorsel A, Elliott K (2021) In pursuit of socially-minded data-intensive innovation in banking: a focus group study of public expectations of digital innovation in banking. Technol Soc 66:101666
Akanbi LA, Oyedele LO, Akinade OO, Ajayi AO, Delgado MD, Bilal M, Bello SA (2018) Salvaging building materials in a circular economy: a BIM-based whole-life performance estimator. Resour Conserv Recycl 129:175–186
AL-Abrrow H, Al-Maatoq M, Alharbi RK, Alnoor A, Abdullah HO, Abbas S, Khattak ZZ (2021a) Understanding employees’ responses to the COVID-19 pandemic: the attractiveness of healthcare jobs. Glob Bus Organ Excell 40(2):19–33
Al-Abrrow H, Fayez AS, Abdullah H, Khaw KW, Alnoor A, Rexhepi G (2021b) Effect of open-mindedness and humble behavior on innovation: mediator role of learning. Int J Emerg Mark (ahead-of-print). https://doi.org/10.1108/IJOEM-08-2020-0888
Albahri AS, Alnoor A, Zaidan AA, Albahri OS, Hameed H, Zaidan BB, Yass AA (2022a) Hybrid artificial neural network and structural equation modelling techniques: a survey. Complex Intell Syst 8(2):1781–1801
Albahri OS, Al-Obaidi JR, Zaidan AA, Albahri AS, Zaidan BB, Salih MM et al (2020) Helping doctors hasten COVID-19 treatment: towards a rescue framework for the transfusion of best convalescent plasma to the most critical patients based on biological requirements via ml and novel MCDM methods. Comput Methods Programs Biomed 196:105617
Albahri OS, Zaidan AA, Albahri AS, Alsattar HA, Mohammed R, Aickelin U, Al-Obaidi JR (2022c) Novel dynamic fuzzy decision-making framework for COVID-19 vaccine dose recipients. J Adv Res 37:147–168
Alharbi R, Alnoor A (2022) The influence of emotional intelligence and personal styles of dealing with conflict on strategic decisions. PSU Research Review, (ahead-of-print). https://doi.org/10.1108/PRR-08-2021-0040
Alnoor A, Abdullah HO, AL-Abrrow H, Wah Khaw K, Al-Awidi IA, Abbas S, Omrane A (2022c) A Fuzzy Delphi analytic job demands-resources model to rank factors influencing open innovation. Transnatl Corp Rev 14(2):178–192
Alnoor A, Al-Abrrow H, Al Halbusi H, Khaw KW, Chew X, Al-Maatoq M, Alharbi RK (2022d) Uncovering the antecedents of trust in social commerce: an application of the non-linear artificial neural network approach. Compet Rev
Alnoor A, Khaw KW, Chew X, Abbas S, Khattak ZZ (2023) The influence of the barriers of hybrid strategy on strategic competitive priorities: evidence from oil companies. Glob J Flex Syst Manag:1–20. https://doi.org/10.1007/s40171-022-00335-8
Alnoor A, Tiberius V, Atiyah AG, Khaw KW, Yin TS, Chew X, Abbas S (2022b) How positive and negative electronic word of mouth (eWOM) affects customers’ intention to use social commerce? A dual-stage multi group-SEM and ANN analysis. Int J Hum-Comput Int:1–30. https://doi.org/10.1080/10447318.2022.2125610
Alnoor A, Zaidan AA, Qahtan S, Alsattar HA, Mohammed RT, Alazab M et al (2022a) Toward a sustainable transportation industry: oil company benchmarking based on the extension of linear Diophantine fuzzy rough sets and multicriteria decision-making methods. IEEE Trans Fuzzy Syst 31(2):449–459
Alsalem MA, Albahri OS, Zaidan AA, Al-Obaidi JR, Alnoor A, Alamoodi AH, Jumaah FM (2022) Rescuing emergency cases of COVID-19 patients: an intelligent real-time MSC transfusion framework based on multi-criteria decision-making methods. Appl Intell:1–25. https://doi.org/10.1007/s10489-021-02813-5
Amicarelli V, Lagioia G, Sampietro S, Bux C (2021) Has the COVID-19 pandemic changed food waste perception and behavior? Evidence from Italian consumers. Socioecon Plann Sci 82:101095
Andersen MS (2007) An introductory note on the environmental economics of the circular economy. Sustain Sci 2(1):133–140
Angelis-Dimakis A, Alexandratou A, Balzarini A (2016) Value chain upgrading in a textile dyeing industry. J Clean Prod 138:237–247
Awasthi AK, Cucchiella F, D’Adamo I, Li J, Rosa P, Terzi S et al (2018) Modelling the correlations of e-waste quantity with economic increase. Sci Total Environ 613:46–53
Babaee Tirkolaee EB, Aydın NS (2021) A sustainable medical waste collection and transportation model for pandemics. Waste Manag Res 39(1_suppl):34–44
Babaee Tirkolaee EB, Goli A, Pahlevan M, Malekalipour Kordestanizadeh RM (2019) A robust bi-objective multi-trip periodic capacitated arc routing problem for urban waste collection using a multi-objective invasive weed optimisation. Waste Manag Res 37(11):1089–1101
Bączkiewicz A, Kizielewicz B, Shekhovtsov A, Wątróbski J, Sałabun W (2021) Methodical aspects of MCDM based E-commerce recommender system. J Theor Appl Electron Commer Res 16(6):2192–2229
Berzi L, Delogu M, Pierini M, Romoli F (2016) Evaluation of the end-of-life performance of a hybrid scooter with the application of recyclability and recoverability assessment methods. Resour Conserv Recycl 108:140–155
Bourouiba L (2020) Turbulent gas clouds and respiratory pathogen emissions: potential implications for reducing transmission of COVID-19. Jama 323(18):1837–1838
Chauhan A, Jakhar SK, Chauhan C (2020) The interplay of circular economy with industry 4.0 enabled smart city drivers of healthcare waste disposal. J Clean Prod 279:123854
Chin AWH, Chu JT, Perera MR, Hui KP, Yen HL, Chan MC, Peiris M, Poon LL (2020) Stability of SARS-CoV-2 in different environmental conditions. Lancet Microbe 1(1):e10
Chirani MR, Kowsari E, Teymourian T, Ramakrishna S (2021) Environmental impact of increased soap consumption during COVID-19 pandemic: biodegradable soap production and sustainable packaging. Sci Total Environ 796:149013
Chojnacka K, Skrzypczak D, Mikula K, Witek-Krowiak A, Izydorczyk G, Kuligowski K et al (2021) Progress in sustainable technologies of leather wastes valorization as solutions for the circular economy. J Clean Prod 313:127902
CIRAIG (International Reference Centre for the Life Cycle of Products, Processes and Services) (2015) Circular economy: a critical literature review of concepts. Polytechnique Montréal, Canada
Cutler, S. (2020). Mounting medical waste from COVID-19 emphasizes the need for a sustainable waste management strategy. Online blog.
Debnath B, Ghosh S, Dutta N (2021) Resource resurgence from COVID-19 waste via pyrolysis: a circular economy approach. Circ Econ Sustain 2(1):211–220
Delogu M, Del Pero F, Berzi L, Pierini M, Bonaffini D (2017) End-of-Life in the railway sector: analysis of recyclability and recoverability for different vehicle case studies. Waste Manag 60:439–450
Despeisse M, Ball PD, Evans S, Levers A (2012) Industrial ecology at factory level–a conceptual model. J Clean Prod 31:30–39
Devi A, Ravindra K, Kaur M, Kumar R (2019) Evaluation of biomedical waste management practices in public and private sector of health care facilities in India. Environ Sci Pollut Res 26(25):26082–26089
Dharmaraj S, Ashokkumar V, Pandiyan R, Munawaroh HSH, Chew KW, Chen WH, Ngamcharussrivichai C (2021) Pyrolysis: an effective technique for degradation of COVID-19 medical wastes. Chemosphere 275:130092
Dieng C, Mberu B, Dimbuene ZT, Faye C, Amugsi D, Aboderin I (2022) Biomedical waste management in Dakar, Senegal: legal framework, health and environment issues; policy and program options. Cities Health 6(1):208–222
Dong X, Goldswain H, Penrice-Randal R, Shawli GT, Prince T, Williamson MK et al (2021) Rapid selection of P323L in the SARS-CoV-2 polymerase (NSP12) in humans and non-human primate models and confers a large plaque phenotype. bioRxiv. https://doi.org/10.1101/2021.12.23.474030
Eastwood MD, Haapala KR (2015) A unit process model based methodology to assist product sustainability assessment during design for manufacturing. J Clean Prod 108:54–64
Ecer F (2021) A consolidated MCDM framework for performance assessment of battery electric vehicles based on ranking strategies. Renew Sustain Energy Rev 143:110916
Eneizan, B., Mohammed, A. G., Alnoor, A., Alabboodi, A. S., & Enaizan, O. (2019). Customer acceptance of mobile marketing in Jordan: an extended UTAUT2 model with trust and risk factors. Int J Eng Bus Manag, 11, 1847979019889484.
Fadhil SS, Ismail R, Alnoor A (2021) The influence of soft skills on employability: a case study on technology industry sector in Malaysia. Interdiscip J Inf Knowl Manag 16:255
Falih, A. M., Al Kasser, M. K., Abbas, M. D., & Ali, H. A. (2021). A study of medical waste management reality in health institutions in Al-Diwaniyah Governorate-Iraq. In IOP Conference Series: Earth and Environmental Science (Vol. 790, No. 1, p. 012032). IOP Publishing.
Favi C, Germani M, Luzi A, Mandolini M, Marconi M (2017) A design for EoL approach and metrics to favor closed-loop scenarios for products. Int J Sustain Eng 10(3):136–146
Felix CB, Ubando AT, Chen WH, Goodarzi V, Ashokkumar V (2022) COVID-19 and industrial waste mitigation via thermochemical technologies towards a circular economy: a state-of-the-art review. J Hazard Mater 423:127215
Féraud R, Clérot F (2002) A methodology to explain neural network classification. Neural Netw 15(2):237–246
Ferasso M, Beliaeva T, Kraus S, Clauss T, Ribeiro‐Soriano D (2020) Circular economy business models: the state of research and avenues ahead. Bus Strateg Environ 29(8):3006–3024
Franklin-Johnson E, Figge F, Canning L (2016) Resource duration as a managerial indicator for circular economy performance. J Clean Prod 133:589–598
Fregonara E, Giordano R, Ferrando DG, Pattono S (2017) Economic-environmental indicators to support investment decisions: a focus on the buildings’ end-of-life stage. Buildings 7(3):65
Gartner, 2016. Market share analysis: consulting services, Worldwide, 2015. Available at. https://www.gartner.com/doc/3317117/market-share-analysis-consultingservices
Geissdoerfer M, Savaget P, Bocken NM, Hultink EJ (2017) The circular economy–a new sustainability paradigm? J Clean Prod 143:757–768
Geng, Y., & Doberstein, B. (2008). Developing the circular economy in China: challenges and opportunities for achieving ‘leapfrog development’. Int J Sustain Dev World Ecol Int J Sust Dev World, 15(3), 231-239.
Ghisellini P, Cialani C, Ulgiati S (2016) A review on circular economy: the expected transition to a balanced interplay of environmental and economic systems. J Clean Prod 114:11–32
Hadi AA, Alnoor A, Abdullah HO (2018) Socio-technical approach, decision-making environment, and sustainable performance: role of ERP systems. Interdiscip J Inf Knowl Manag 13:397
Hama, A. R., Tahir, T. A., & Ali, B. J. (2021). A study on solid waste generation, composition and management in Sulaimania city, Kurdistan region, Iraq. In IOP Conference Series: Earth and Environmental Science (Vol. 779, No. 1, p. 012049). IOP Publishing.
Han F, Liu Y, Liu W, Cui Z (2017) Circular economy measures that boost the upgrade of an aluminum industrial park. J Clean Prod 168:1289–1296
Hannon E, Kuhlmann M, Thaidigsmann B (2016) Developing products for a circular economy. Cross-functional collaboration and customer-focused design thinking can help companies reap more value from the energy and resources they use. In: The circular economy moving from theory to practice. McKinsey Company
Hempel CG (1965) Aspects of scientific explanation, vol 1. Free Press, New York
Hempel CG (1966) Aspects of scientific explanation, and other essays Int He Philosophy of Science. Free Press
Huysman S, De Schaepmeester J, Ragaert K, Dewulf J, De Meester S (2017) Performance indicators for a circular economy: a case study on post-industrial plastic waste. Resour Conserv Recycl 120:46–54
Ibn-Mohammed T, Mustapha KB, Godsell J, Adamu Z, Babatunde KA, Akintade DD et al (2021) A critical analysis of the impacts of COVID-19 on the global economy and ecosystems and opportunities for circular economy strategies. Resour Conserv Recycl 164:105169
Ilyas S, Srivastava RR, Kim H (2020) Disinfection technology and strategies for COVID-19 hospital and bio-medical waste management. Sci Total Environ 749:141652
Iyengar K, Bahl S, Vaishya R, Vaish A (2020) Challenges and solutions in meeting up the urgent requirement of ventilators for COVID-19 patients. Diabetes Metab Syndr Clinical Res Rev 14(4):499–501
Jabbar AK, Almayyahi ARA, Ali IM, Alnoor A (2020) Mitigating uncertainty in the boardroom: analysis to financial reporting for financial risk COVID-19. J Asian Fin Econ Bus 7(12):233–243
Jafarzadeh Ghoushchi S, Memarpour Ghiaci A, Rahnamay Bonab S, Ranjbarzadeh R (2022) Barriers to circular economy implementation in designing of sustainable medical waste management systems using a new extended decision-making and FMEA models. Environ Sci Pollut Res 29(53):79735–79753
Kandasamy J, Kinare YP, Pawar MT, Majumdar A, Kek V, Agrawal R (2022) Circular economy adoption challenges in medical waste management for sustainable development: an empirical study. Sustain Dev 30(5):958–975
Kargar S, Paydar MM, Safaei AS (2020) A reverse supply chain for medical waste: a case study in Babol healthcare sector. Waste Manag 113:197–209
Karliner J, Slotterback S, Boyd R, Ashby B, Steele K, Wang J (2020) Health care’s climate footprint: the health sector contribution and opportunities for action. Eur J Public Health 30(Supplement_5):ckaa165-843
Khaw KW, Alnoor A, Al-Abrrow H, Chew X, Sadaa AM, Abbas S, Khattak ZZ (2022a) Modelling and evaluating trust in mobile commerce: a hybrid three stage Fuzzy Delphi, structural equation modeling, and neural network approach. Int J Hum Comput Interact 38(16):1529–1545
Khaw KW, Alnoor A, Al-Abrrow H, Tiberius V, Ganesan Y, Atshan NA (2022b) Reactions towards organizational change: a systematic literature review. Curr Psychol:1–24. https://doi.org/10.1007/s12144-022-03070-6
Khaw KW, Thurasamy R, AL-Abrrow H, Alnoor A, Tiberius V, Abdullah HO, Abbas S (2021) Influence of generational status on immigrants’ entrepreneurial intentions to start new ventures: a framework based on structural equation modeling and multi-criteria decision-making. J Entrep Emerg Econ, ahead-of-print. https://doi.org/10.1108/JEEE-04-2021-0141
Kirchherr J, Reike D, Hekkert M (2017) Conceptualising the circular economy: an analysis of 114 definitions. Resour Conserv Recycl 127:221–232
Klemeš JJ, Van Fan Y, Tan RR, Jiang P (2020) Minimising the present and future plastic waste, energy and environmental footprints related to COVID-19. Renew Sustain Energy Rev 127:109883
Korhonen J, Honkasalo A, Seppälä J (2018) Circular economy: the concept and its limitations. Ecol Econ 143:37–46
Krishnan E, Mohammed R, Alnoor A, Albahri OS, Zaidan AA, Alsattar H et al (2021) Interval type 2 trapezoidal-fuzzy weighted with zero inconsistency combined with VIKOR for evaluating smart e-tourism applications. Int J Intell Syst 36(9):4723–4774
Kulkarni BN, Anantharama V (2020) Repercussions of COVID-19 pandemic on municipal solid waste management: challenges and opportunities. Sci Total Environ 743:140693
Kumar H, Azad A, Gupta A, Sharma J, Bherwani H, Labhsetwar NK, Kumar R (2020a) COVID-19 Creating another problem? Sustainable solution for PPE disposal through LCA approach. Environ Dev Sustain 23:9418–9432
Kumar S, Panda TK, Behl A, Kumar A (2021) A mindful path to the COVID-19 pandemic: an approach to promote physical distancing behavior. Int J Organ Anal 29(5):1117–1143
Kumar V, Singh SB, Singh S (2020b) COVID-19: environment concern and impact of Indian medicinal system. J Environ Chem Eng 8(5):104144
Lal R, Brevik EC, Dawson L, Field D, Glaser B, Hartemink AE et al (2020) Managing soils for recovering from the COVID-19 pandemic. Soil Systems 4(3):46
Langley, J. (2020). WEEE sector expects Q2 lockdown hit. https://www.letsrecycle.com/news/latest-news/weee-sector-expects-q2-lockdown-hit/.
Laso J, Margallo M, Celaya J, Fullana P, Bala A, Gazulla C et al (2016) Waste management under a life cycle approach as a tool for a circular economy in the canned anchovy industry. Waste Manag Res 34(8):724–733
Lau LS, Choong CK, Eng YK (2014) Investigation of the environmental Kuznets curve for carbon emissions in Malaysia: do foreign direct investment and trade matter? Energy Policy 68:490–497
Leong LY, Hew TS, Ooi KB, Chong AYL (2020) Predicting the antecedents of trust in social commerce–a hybrid structural equation modeling with neural network approach. J Bus Res 110:24–40
Li F, Su Z, Wang G (2021) An effective dynamic immune optimisation control for the wastewater treatment process. Environ Sci Pollut Res 29:79718–79733. https://doi.org/10.1007/s11356-021-17505-3
Lin M, Huang C, Xu Z (2020) MULTIMOORA based MCDM model for site selection of car sharing station under picture fuzzy environment. Sustain Cities Soc 53:101873
Liu K, Lin B (2019) Research on influencing factors of environmental pollution in China: a spatial econometric analysis. J Clean Prod 206:356–364
Liu P, Rani P, Mishra AR (2021) A novel Pythagorean fuzzy combined compromise solution framework for the assessment of medical waste treatment technology. J Clean Prod 292(4):1–17
Ma Y, Lin X, Wu A, Huang Q, Li X, Yan J (2020) Suggested guidelines for emergency treatment of medical waste during COVID-19: Chinese experience. Waste Dispos Sustain Energy 2:81–84
MacArthur E (2013) Towards the circular economy. J Ind Ecol 2(1):23–44
MacNeill AJ, Hopf H, Khanuja A, Alizamir S, Bilec M, Eckelman MJ, Sherman JD (2020) Transforming the medical device industry: road map to a circular economy: study examines a medical device industry transformation. Health Aff 39(12):2088–2097
Mahyari KF, Sun Q, Klemes JJ, Aghbashlo M, Tabatabaei M, Khoshnevisan B, Birkved M (2022) To what extent waste management strategies need adaptation to post-COVID-19. Sci Total Environ 837:155829
Manupati VK, Ramkumar M, Baba V, Agarwal A (2021) Selection of the best healthcare waste disposal techniques during and post COVID-19 pandemic era. J Clean Prod 281:125175
Mekonnen B, Solomon N, Wondimu W (2021) Healthcare waste status and handling practices during COVID-19 pandemic in Tepi General Hospital, Ethiopia. J Environ Public Health 2021
Mensoor MK (2020) Medical waste management in Iraq: a case study of Baghdad. Waste Disp Sust Ener 2(4):329–335
Minoglou M, Gerassimidou S, Komilis D (2017) Healthcare waste generation worldwide and its dependence on socio-economic and environmental factors. Sustainability 9(2):220
Mohammad EB, Abdelqader AAA, Hadi AA, Alhamzah A (2019) An investigation into the relationship between emotional labor and customer satisfaction. J Manag Bus Admin Central Eur 27(4):23–47
Mohammed RT, Zaidan AA, Yaakob R, Sharef NM, Abdullah RH, Zaidan BB, Abdulkareem KH (2022) Determining importance of many-objective optimisation competitive algorithms evaluation criteria based on a novel fuzzy-weighted zero-inconsistency method. Int J Inf Technol Decis Mak 21(01):195–241
Moraes FTF, Gonçalves ATT, Lima JP, Lima RDS (2021) An assessment tool for healthcare waste management in Brazilian municipalities during the COVID-19 pandemic. Waste Manag Res 40(6):625–641
Moreau V, Sahakian M, Van Griethuysen P, Vuille F (2017) Coming full circle: why social and institutional dimensions matter for the circular economy. J Ind Ecol 21(3):497–506
Murray A, Skene K, Haynes K (2017) The circular economy: an interdisciplinary exploration of the concept and application in a global context. J Bus Ethics 140(3):369–380
Nandi S, Sarkis J, Hervani AA, Helms MM (2021) Redesigning supply chains using blockchain-enabled circular economy and COVID-19 experiences. Sustain Prod Consum 27:10–22
Nandy S, Fortunato E, Martins R (2022) Green economy and waste management: an inevitable plan for materials science. Prog Nat Sci 32(1):1–9
Narayanamoorthy S, Brainy JV, Sulaiman R, Ferrara M, Ahmadian A, Kang D (2022) An integrated decision-making approach for selecting a sustainable waste water treatment technology. Chemosphere 301:134568
Neumeyer X, Ashton W, Dentchev N (2020) Addressing resource and waste management challenges imposed by COVID-19: an entrepreneurship perspective. Resour Conserv Recycl 162:105058
Ogunseitan OA (2020) The materials genome and COVID-19 pandemic. Jom (Warrendale, Pa: 1989) 72(6):1–3
Oruonye ED, Ahmed AY (2020) COVID-19 and challenges of management of infectious medical waste in Nigeria: a case of Taraba State. Int J Waste Resour 10(3):381–385
Pachauri A, Shah P, Almroth BC, Sevilla NP, Narasimhan M (2019) Safe and sustainable waste management of self care products. bmj 365
Pandey D, Verma S, Verma P, Mahanty B, Dutta K, Daverey A, Arunachalam K (2020) SARS-CoV-2 in wastewater: challenges for developing countries. Int J Hyg Environ Health 113634
Parashar N, Hait S (2021) Plastics in the time of COVID-19 pandemic: protector or polluter? Sci Total Environ 759:144274
Pearce DW, Turner RK (1989) Economics of natural resources and the environment. Johns Hopkins University Press, Maryland
Peng J, Wu X, Wang R, Li C, Zhang Q, Wei D (2020) Medical waste management practice during the 2019-2020 novel coronavirus pandemic: experience in a general hospital. Am J Infect Control 48(8):918–921
Purnomo CW, Kurniawan W, Aziz M (2021) Technological review on thermochemical conversion of COVID-19-related medical wastes. Resour Conserv Recycl 167:105429
Qiu S, Xu Z, Bhatt B (2021) The sharing economy platforms in rural China: bridging institutional voids through institutional entrepreneurship. In: Sharing Economy at the Base of the Pyramid. Springer, Singapore, pp 75–99
Ranjbari M, Esfandabadi ZS, Shevchenko T, Chassagnon-Haned N, Peng W, Tabatabaei M, Aghbashlo M (2022) Mapping healthcare waste management research: past evolution, current challenges, and future perspectives towards a circular economy transition. J Hazard Mater 422:126724
Ribot V, Chang N, González A (2020) Effects of COVID-19 on the mental health of the population. Habanera Mag Med Sci 19(1)
Rolewicz-Kalinska A (2016) Logistic constraints as a part of a sustainable medical waste management system. Transp Res Procedia 16:473–482
Romero MDCV, Cárdenas AM, Fuentes AB, Barragán AAS, Gómez DBS, Jiménez MT (2021) Acute mesenteric arterial thrombosis in severe SARS-Co-2 patient: a case report and literature review. Int J Surg Case Rep 86:106307
Rume T, Islam SDU (2020) Environmental effects of COVID-19 pandemic and potential strategies of sustainability. Heliyon 6(9):e04965
Rupani PF, Nilashi M, Abumalloh RA, Asadi S, Samad S, Wang S (2020) Coronavirus pandemic (COVID-19) and its natural environmental impacts. Int J Environ Sci Technol 17:4655–4666
Sadaa AM, Ganesan Y, Khaw KW, Alnoor A, Abbas S, Chew X, Bayram GE (2022) Based on the perception of ethics in social commerce platforms: adopting SEM and MCDM approaches for benchmarking customers in rural communities. Curr Psychol:1–35. https://doi.org/10.1007/s12144-022-04069-9
Sandberg H, Alnoor A, Tiberius V (2022) Environmental, social, and governance ratings and financial performance: evidence from the European food industry. Bus Strateg Environ. https://doi.org/10.1002/bse.3259
Sarkodie SA, Owusu PA (2020) Impact of COVID-19 pandemic on waste management. Environ Dev Sustain 23:7951–7960
Sassanelli C, Rosa P, Rocca R, Terzi S (2019) Circular economy performance assessment methods: a systematic literature review. J Clean Prod 229:440–453
Sharma HB, Vanapalli KR, Cheela VS, Ranjan VP, Jaglan AK, Dubey B et al (2020) Challenges, opportunities, and innovations for effective solid waste management during and post COVID-19 pandemic. Resour Conserv Recycl 162:105052
Shuv-Ami A, Shalom T (2020) A new service quality scale for hospital emergency rooms. Int J Organ Anal 28(6):1133–1147
Sihvonen S, Ritola T (2015) Conceptualizing ReX for aggregating end-of-life strategies in product development. Procedia Cirp 29:639–644
Silva ALP, Prata JC, Walker TR, Duarte AC, Ouyang W, Barcelò D, Rocha-Santos T (2021) Increased plastic pollution due to COVID-19 pandemic: challenges and recommendations. Chem Eng J 405:126683
Singh N, Tang Y, Ogunseitan OA (2020a) Environmentally sustainable management of used personal protective equipment. Environ Sci Technol 54(14):8500–8502
Singh N, Tang Y, Zhang Z, Zheng C (2020b) COVID-19 waste management: effective and successful measures in Wuhan, China. Resour Conserv Recycl 163:105071
Singh N, Ogunseitan OA, Tang Y (2021) Medical waste: current challenges and future opportunities for sustainable management. Crit Rev Environ Sci Technol 52(11):2000–2022
Stahel WR (1982) The product life factor. An inquiry into the nature of sustainable societies: the role of the private sector. Houston Area Research Center, pp 72–105
Stahel WR (2008) In: Misra KB (ed) Handbook of Performability Engineering, vol Ch. 10. Springer, London, pp 127–138
Stahel WR, Reday G (1976) The potential for substituting manpower for energy, report to the Commission of the European Communities, Brussels
Stević Ž, Pamučar D, Puška A, Chatterjee P (2020) Sustainable supplier selection in healthcare industries using a new MCDM method: measurement of alternatives and ranking according to compromise solution (MARCOS). Comput Ind Eng 140:106231
Solomon MD, McNulty EJ, Rana JS, Leong TK, Lee C, Sung SH, Go AS (2020) The Covid-19 pandemic and the incidence of acute myocardial infarction. New Engl J Med 383(7):691–693
Su B, Heshmati A, Geng Y, Yu X (2013) A review of the circular economy in China: moving from rhetoric to implementation. J Clean Prod 42:215–227
Suárez-Eiroa B, Fernández E, Méndez-Martínez G, Soto-Oñate D (2019) Operational principles of circular economy for sustainable development: linking theory and practice. J Clean Prod 214:952–961
Suresh M, Vaishnavi V, Pai RD (2020) Leanness evaluation in healthcare organisations using fuzzy logic approach. Int J Organ Anal 28(6):1201–1225
Tabash MI, Hussein RA, Mahmoud AH, El-Borgy MD, AbuHamad BA (2016) Impact of an educational program on knowledge and practice of health care staff toward pharmaceutical waste management in Gaza, Palestine. J Air Waste Manag Assoc 66(4):429–438
Teymourian T, Teymoorian T, Kowsari E, Ramakrishna S (2021) Challenges, strategies, and recommendations for the huge surge in plastic and medical waste during the global COVID-19 pandemic with circular economy approach. Mater Circ Econ 3(1):1–14
Torkayesh AE, Deveci M, Torkayesh SE, Tirkolaee EB (2021) Analysing failures in adoption of smart technologies for medical waste management systems: a type-2 neutrosophic-based approach. Environ Sci Pollut Res 29:79688–79701
Triantaphyllou E (2000) Multi-criteria decision making methods. In: Multi-criteria decision making methods: a comparative study. Springer, Boston, pp 5–21
Van Buren N, Demmers M, Van der Heijden R, Witlox F (2016) Towards a circular economy: the role of Dutch logistics industries and governments. Sustainability 8(7):647
Van Straten B, Dankelman J, van der Eijk A, Horeman T (2021) A circular healthcare economy: a feasibility study to reduce surgical stainless-steel waste. Sustain Prod Consum 27:169–175
Vanapalli KR, Sharma HB, Ranjan VP, Samal B, Bhattacharya J, Dubey BK, Goel S (2021) Challenges and strategies for effective plastic waste management during and post COVID-19 pandemic. Sci Total Environ 750:141514
Wah KK, Omar AZ, Alnoor A, Alshamkhani MT (2022) Technology application in tourism in Asia: comprehensive science mapping analysis. In: Technology Application in Tourism in Asia. Springer, Singapore, pp 53–66
Wang P, Casner RG, Nair MS, Wang M, Yu J, Cerutti G et al (2021) Increased resistance of SARS-CoV-2 variant P. 1 to antibody neutralization. Cell Host Microbe 29(5):747–751
Webster K (2015) The circular economy: a wealth of flows. Ellen Macarthur Foundation Publishing, Isle of Wight, UK
Wei Y, Cui M, Ye Z, Guo Q (2021) Environmental challenges from the increasing medical waste since SARS outbreak. J Clean Prod 291:125246
Weistroffer HR, Li Y (2016) Multiple criteria decision analysis software. In: Multiple criteria decision analysis. Springer, New York, pp 1301–1341
Williams, M., Gower, R., Green, J., Whitebread, E., Lenkiewicz, Z., & Schröder, P. (2019). No time to waste: tackling the plastic pollution crisis before it’s too late.
Windfeld ES, Brooks MSL (2015) Medical waste management – a review. J Environ Manage 163:98–108
Wu J, Xiang WN, Zhao J (2014) Urban ecology in China: historical developments and future directions. Landsc Urban Plan 125:222–233
Wuyts W, Marin J, Brusselaers J, Vrancken K (2020) Circular economy as a COVID-19 cure? Resour Conserv Recycl 162:105016
Yang J, Wu T, Gong P (2017) Implementation of China’s new urbanization strategy requires new thinking. Sci Bull 62:81–82
Yuan Z, Bi J, Moriguichi Y (2006) The circular economy: a new development strategy in China. J Ind Ecol 10(1-2):4–8
Yuan Y, Gao Y, Zhao J, Mao L (2008) Characterization and stability evaluation of β-carotene nanoemulsions prepared by high pressure homogenization under various emulsifying conditions. Food Res Int 41(1):61–68
Zafar S (2019) Medical waste management in developing countries. Bioenergy Consult Accessed 12 Dec 2017
Zar HJ, Dawa J, Fischer GB, Castro-Rodriguez JA (2020) Challenges of COVID-19 in children in low-and middle-income countries. Paediatr Respir Rev 35:70–74
Zhijun F, Nailing Y (2007) Putting a circular economy into practice in China. Sustain Sci 2(1):95–101
Funding
This work is funded by Ministry of Higher Education Malaysia, Fundamental Research Grant Scheme [Grant Number: FRGS/1/2022/STG06/USM/02/4], for the Project entitled “Efficient Joint Process Monitoring using a New Robust Variable Sample Size and Sampling Interval Run Sum Scheme”.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by Dr. XinYing Chew, Dr. Khai Wah Khaw, and Dr. Alhamzah Alnoor with the supervision of Dr. Marcos Ferasso and Dr. Hussam Al Halbusi. The first draft of the manuscript was written by Dr. Yousif Raad Muhsen and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
All the procedures adopted by the study, involving human participants, were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was obtained from all individual participants of the study.
Conflict of interest
The authors declare no competing interests.
Additional information
Responsible Editor: Arshian Sharif
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: The 4th Author Marcos Ferasso has 2 affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chew, X., Khaw, K.W., Alnoor, A. et al. Circular economy of medical waste: novel intelligent medical waste management framework based on extension linear Diophantine fuzzy FDOSM and neural network approach. Environ Sci Pollut Res 30, 60473–60499 (2023). https://doi.org/10.1007/s11356-023-26677-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-26677-z