
Abstract
The concentrations and distribution of β-blockers, lipid regulators, and psychiatric and cancer drugs in the influent and effluent of the municipal wastewater treatment plant (WWTP) and the effluent of 16 hospitals that discharge into the wastewater treatment plant mentioned in this study at two sampling dates in summer and winter were examined. The pharmaceutical contribution of hospitals to municipal wastewater was determined. The removal of target pharmaceuticals was evaluated in a WWTP consisting of conventional biological treatment using activated sludge. Additionally, the potential environmental risk for the aquatic receiving environments (salt lake) was assessed. Beta-blockers and psychiatric drugs were detected in high concentrations in the wastewater samples. Atenolol (919 ng/L) from β-blockers and carbamazepine (7008 ng/L) from psychiatric pharmaceuticals were detected at the highest concentrations in hospital wastewater. The total pharmaceutical concentration determined at the WWTP influent and effluent was between 335 and 737 ng/L in summer and between 174 and 226 ng/L in winter. The concentrations detected in hospital effluents are higher than the concentrations detected in WWTP. The total pharmaceutical contributions from hospitals to the WWTP in summer and winter were determined to be 2% and 4%, respectively. Total pharmaceutical removal in the WWTP ranged from 23 to 54%. According to the risk ratios, atenolol could pose a high risk (risk quotient > 10) for fish in summer and winter. There are different reasons for the increase in pharmaceutical consumption in recent years. One of these reasons is the COVID-19 pandemic, which has been going on for 2 years. In particular, hospitals were operated at full capacity during the pandemic, and the occurrence and concentration of pharmaceuticals used for the therapy of COVID-19 patients has increased in hospital effluent. Pandemic conditions have increased the tendency of people to use psychiatric drugs. It is thought that beta-blocker consumption has increased due to cardiovascular diseases caused by COVID-19. Therefore, the environmental risk of pharmaceuticals for aquatic organisms in hospital effluent should be monitored and evaluated.
Similar content being viewed by others

Introduction
The growing population and the development of urbanization and industrialization have led to an increase in the concentration of some pollutants and introduced new pollutants in the environment (Belhaj et al. 2015). As a result of advances in medical treatment methods, the emergence of new diseases, the rising demand in the field of health care and economic advancements, and the production and consumption of pharmaceuticals have inevitably risen. Pharmaceuticals are complex molecules, and due to their extensive use, they have been determined to exist in different environmental matrices, such as wastewater, surface water, groundwater, drinking water, sewage sludge, and sediments. Pharmaceutical residues impose proven or predicted risks to microorganisms, fauna, and flora (Bartrons and Peñuelas 2017; Ashfaq et al. 2017). Pharmaceuticals are subdivided into different therapeutic groups, such as analgesics/anti-inflammatories, antibiotics, β-blockers, cardiac drugs, psychiatric drugs, lipid regulators, and cancer drugs. These pharmaceuticals are among the commonly used drugs in hospitals and homes. Beta-blockers have been extensively taken for the treatment of abnormal heart rhythms, high blood pressure, angina pectoris, hypertension, and cardiac dysfunction (Yi et al. 2020). Atenolol, metoprolol, propranolol, and sotalol are the most widely used β-blockers (Khasawneh and Palaniandy 2021). Because β-blockers are becoming more widely used and are one of the most commonly found pharmaceuticals in the environment, it is possible to measure β-blockers and their metabolites in wastewater up to μg/L (Yi et al. 2020; Wilde et al. 2013). When studies on the occurrence of β-blockers in wastewater were examined, different concentrations were determined depending on drug use and wastewater treatment technologies in different countries (Yi et al. 2020). For example; β-blockers were detected in the range of 64–474 ng/L in Italy (Al Aukidya et al. 2012), in the range of 35–1600 ng/L in Finland (Vieno et al. 2007), in the range of 0.4–2110 ng/L in Spain (Biel-Maeso et al. 2018a), and in the range of 25–1530 ng/L in Switzerland (Alder et al. 2010) at the output of the wastewater treatment plant (WWTP).
In addition, β-blockers (atenolol, acebutolol, bisoprolol, celiprolol, metoprolol, nadolol, pindolol, propranolol, and sotalol) have a half-life of 3–8.7 days in water and are classified as “pseudopersistent” (Hernando et al. 2006; Ramil et al. 2010). Lipid regulators are widely used for the treatment of hyperlipidemia and are among the most common pharmaceuticals in wastewater. The current commonly used lipid regulators are gemfibrozil, bezafibrate, fenofibrate, and clofibric acid (Wang et al. 2019). More than 264 million people worldwide suffer from depression. The consumption of psychiatric drugs is higher than the consumption of other medical drugs (Melchor-Martínez et al. 2021). Thus, with the increasing consumption of psychiatric drugs, they have begun to be detected in wastewater, surface waters, and even drinking water around the world. For instance, the concentrations of psychiatric pharmaceuticals ranged from <dl to 3124 ng/L in WWTP influent and from <dl to 2956 ng/L in WWTP effluent (Kosma et al. 2019; Wu et al. 2015; Yuan et al. 2013; Lajeunesse et al. 2012; Oliveira et al. 2015). Psychiatric pharmaceuticals were also found in surface water (24.3 ng/L for diazepam, 0.4 ng/L for fluoxetine, 4 ng/L for lorazepam, 25.3 ng/L for carbamazepine in Chinese rivers) (Wu et al. 2015). Furthermore, psychiatric pharmaceuticals were detected at 1.9 ng/L (Wu et al. 2015) and 23.5 ng/L (Zuccato et al. 2000) for diazepam in drinking water. Psychiatric drugs can be grouped into antidepressants, anxiolytics, sedatives and hypnotics, antipsychotics, and mood stabilizers (Kosma et al. 2019). It is foreseen that there will be 21.4 million new cancer patients by 2032. Cancer medicines will be used more frequently as a result of this in forthcoming years. As cancer drugs are classified into cytotoxic and endocrine therapy drugs, they are a cause for concern (Oliveira Klein et al. 2021). Additionally, 33 emerging contaminants, including diclofenac, ibuprofen, carbamazepine, and clofibric acid, were identified in surface waters by the European Union (Hena et al. 2021).
Pharmaceuticals can enter environmental matrices in different ways, such as pharmaceutical production plants, hospitals, improper disposal, households and WWTPs, irrigation with treated or untreated wastewater, and atmospheric wet deposition (Ma et al. 2018; Ferrey et al. 2018; Martínez-Alcala et al. 2021). After the COVID-19 pandemic, which emerged at the end of 2019, the consumption of pharmaceuticals has increased worldwide. The detection frequency and concentration of some pharmaceuticals post pandemic in Wuhan surface water increased before the pandemic. Additionally, some antibiotics pose a medium/high risk for aquatic organisms (Chen et al. 2021). The concentrations of antiviral drugs and paracetamol in wastewater increased 170% and 198% compared to prepandemic concentrations in Greece, respectively (Galani et al. 2021). Kuroda et al. (2021) reported that the removal efficiency of antiviral drugs used to treat coronavirus disease with conventional wastewater processes is below 20%. These drugs pose a high risk for aquatic organisms in the receiving environment. In particular, due to the increase in the number of patients receiving therapy in hospitals during the COVID-19 pandemic, the pharmaceutical contribution of hospitals to urban wastewater has increased (Khan et al. 2021). Commonly used conventional WWTPs, which include primary and secondary treatment processes to remove pollutants such as organic matter and suspended matter, are not designed to eliminate these compounds; therefore, many pharmaceuticals go through conventional WWTP without adequate treatment. In addition, the main sources of pharmaceuticals in WWTPs are households and hospital wastewater. Hospital wastewater containing a large number of pharmaceuticals is generally discharged into sewer networks and treated together with domestic wastewater in WWTPs. Hospitals produce different amounts of wastewater containing different types and numbers of pharmaceuticals according to hospital characteristics. Determining the contribution of hospitals to the pharmaceutical load in WWTPs is important for the pretreatment of hospital wastewater (Tormo-Budowski et al. 2021; Semerjian et al. 2018; Santos et al. 2013). Pharmaceuticals have been detected worldwide at ng/L, ng/g, or μg/L levels and at μg/g levels in wastewater and the receiving environment, respectively (Maniakova et al. 2020). Pharmaceuticals have effects significantly reducing fertility in species such as cladoceran Daphnia magna and fish, endocrine disruption in receiving environments, and development of bacterial pathogen resistance (Semerjian et al. 2018).
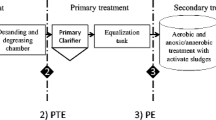
In this context, a total of 18 commonly used pharmaceuticals of different therapeutic classes (β-blockers, lipid regulators, psychiatric and cancer drugs) were analyzed in sixteen hospital effluents and the influent and effluent of municipal WWTP in Konya (Turkey) at two sampling dates in summer and winter Konya urban wastewater and examined 16 hospitals discharge to the Konya WWTP. For this reason, wastewater samples were taken from the Konya WWTP to determine the pharmaceutical load of the examined hospitals to the WWTP and to determine the treatment efficiency of pharmaceuticals. The plants have screening, grit removal, preliminary sedimentation, biological treatment with activated sludge process, and secondary sedimentation.
Pharmaceutical concentrations discharged into the sewer system of the examined hospitals were determined. Generally, hospital wastewater is an important source of pharmaceuticals in WWTPs. In this study, the pharmaceutical pollution load of the examined hospitals to the WWTP was revealed. The pharmaceutical removal of Konya WWTP was calculated with detected concentrations at influent and effluent of Konya WWTP. Konya WWTP effluent is discharged into the salt lake. Pharmaceuticals have some proven and predicted risks to the receiving environment. So, the potential ecotoxicological risk for pharmaceuticals was determined by using the risk quotient for aquatic organisms in the receiving environment.
Material and methods
Chemicals and equipment
Atenolol, sotalol, timolol, bezafibrate, pravastatin, tamoxifen, ifosfamide, and etoposide were obtained from Sigma (Switzerland), and metoprolol, propranolol, clofibric acid, fenofibrate, gemfibrozil, carbamazepine, diazepam, fluoxetine, lorazepam, and cyclophosphamide standards were obtained from Fluka (Switzerland). The physicochemical properties of the investigated pharmaceuticals are presented in the supplementary material (Table S1). HPLC-grade methanol, hydrochloric acid (37%), formic acid (98%), and ethylenediaminetetraacetic acid disodium salt solution (Na2EDTA) were obtained from Merck (Darmstadt, Germany). While a glass fiber filter with a 1.2 μm pore diameter was acquired from Whatman (USA), a 0.45-μm nylon membrane filter was acquired from Sartorius (Göttingen, Germany). The Oasis HLB cartridge (60 mg, 3 mL) used for solid phase extraction (SPE) was obtained from Waters Corporation. Deionized water was supplied from a Millipore brand ultrapure water device. High-purity nitrogen gas was provided by a nitrogen generator (Peak Scientific).
Wastewater samples
Hospital effluents were collected from 5 state hospitals and 5 private hospitals in Selcuklu District, 2 state hospitals and 3 private hospitals in Meram District, and 1 private hospital in Karatay District and the influent and effluent of the municipal WWTP, which receives wastewater from the three districts in Konya. Effluent samples were taken from the discharge points of the hospitals into the sewage system. The bed capacities of the sampled hospitals vary between 27 and 1298 beds. The Konya sewerage system is a combined sewerage system in which wastewater and rainwater are collected in the same channel. There are physical treatments, biological treatments, and disinfection processes in the WWTP. Wastewater samples were gathered twice a year in summer and winter using a composite micro sampler (Durko, Turkey) and were stored at 4 °C until analysis.
Analytical procedures
Wastewater samples before extraction were passed through a glass fiber filter and a nylon membrane filter. The Oasis HLB SPE cartridge was conditioned with 5 mL of deionized water followed by 5 mL of methanol at a flow rate of approximately 2 mL/min. Samples were loaded into the cartridge at a flow rate of approximately 1 mL/min. After preconcentration of the sample, the cartridge was washed with 5 mL of deionized water at a flow rate of approximately 2 mL/min, and air was passed through the cartridge for 5 min to remove excess water from the cartridge. Elution of the compounds in the cartridge was carried out with 10 mL of methanol at a flow rate of approximately 1 mL/min. The extract obtained was redissolved in 400 μL methanol/water (50/50, v/v) after drying under a rotary evaporator and gentle stream of nitrogen gas.
Quantitative analyses of target compounds were carried out with LC-MS/MS systems. The mobile phase was eluent A (deionized water with 0.1% formic acid and 5 mM ammonium formate) and eluent B (methanol) for positive ion mode and eluent A (deionized water with 10 mM ammonium acetate) and eluent B (methanol) for negative ion mode. The most suitable carrier phase flow rate was determined to be 0.6 mL/min. The column temperature was 35 °C, and the injection volume was 2 μL. Analytical parameters determined for the pharmaceuticals are given in Table S2.
Physicochemical analyses such as pH, electrical conductivity (EC), total suspended solids (TSS), and chemical oxygen demand (COD) of wastewater taken from hospitals and the influent and effluent of municipal WWTP were carried out. The pH and EC measurements of the wastewater samples were performed with a Hach brand portable pH and EC measuring device. TSS measurements were carried out according to standard methods (APHA 1992). COD values were measured with a WTW brand spectrophotometer using ready kits. The pH, EC, TSS, and COD values of wastewater samples ranged from 6.58 to 8.63, from 525 to 7970 μS/cm, from 18 to 1218 mg/L, and from 183 to 819 mg/L in hospital wastewater and from 7.2 to 7.93, from 1706 to 2510 μS/cm, from 592 to 644 mg/L, and from 539 to 944 mg/L in municipal wastewater, respectively. The pH, EC, and TSS values were higher in hospital wastewater than in municipal wastewater.
Environmental risk assessment
An environmental risk assessment approach was used to assess the impact of pharmaceutical pollution on the aquatic environment. Risk quotient (RQ) values were calculated for three different trophic levels (algae, crustaceans, and fish) using Eq. (1):
The meanings of the MECmax and PNEC are as follows: maximum measured environmental concentration and predicted no-effect concentration, respectively. The PNEC values used for the calculations are presented in Table S3. The risk assessment criteria, where RQ < 0.1, suggest no adverse effect with insignificant risk. A value of 0.1 < RQ < 1.0 suggests a low risk, and there is a potential adverse effect. Values of RQ between 1 and 10 indicate a moderate risk, while a high ecological risk indicates values equal to or above 10 (Gomez et al. 2006; Deblonde and Hartemann 2013).
Results and discussion
Pharmaceutical concentration in wastewater
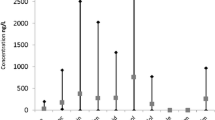
Table 1 demonstrates the minimum, average, and maximum concentrations of the pharmaceuticals detected in the wastewater samples. All compounds investigated were present in at least one influent, effluent, and hospital wastewater, with the exception of timolol and diazepam. This result indicates the widespread presence of pharmaceuticals in wastewater even after treatment. Pharmaceutical concentrations detected in previous studies are given in Tables 2, 3, 4, and 5. In this study, the maximum concentrations of β-blockers detected in hospital wastewater were 175 ng/L for metoprolol during the summer and 920 ng/L for atenolol during the winter. The concentrations of β-blockers in the influent and effluent of the municipal WWTP were <dl–424 ng/L in summer and <dl–153 ng/L in winter, and <dl–162 ng/L in summer and <dl–138 ng/L in winter, respectively. At the WWTP, atenolol was determined at maximum concentration in both summer and winter periods. Additionally, timolol compounds were not detected in hospital, influent, or effluent wastewater. When looking at the physicochemical properties of the β-blockers investigated, the atenolol compound has higher solubility than other β-blockers. In addition, the atenolol compound is excreted from the body at a rate of 40–50% in the main form and has a low log Kow value (0.16). Therefore, it has high mobility in aquatic environments. Due to these properties, it was detected in high concentrations in hospital and WWTP wastewaters. Even though the removal rates of the metoprolol, propranolol, and timolol compounds in the main form are low, the log Kow values are high. However, the sotalol compound is excreted in the main form at a rate higher than 75%, and the log Kow value is low. Atenolol was detected at high concentrations because there are many drugs containing atenolol as an active ingredient, and it is used in the treatment of more common diseases.
The minimum concentration of lipid regulators in hospital wastewater was 0.011 ng/L (fenofibrate) in summer and below the detection limit (clofibric acid) in winter. The maximum concentration in hospital wastewater was determined to be 1.76 ng/L (pravastatin) in the summer and 26.38 ng/L (pravastatin) in the winter. Lipid regulators were 0.15–3.61 ng/L in summer, <dl–13.51 ng/L in winter, 0.084–0.89 ng/L in summer, and <dl–8.18 ng/L in the influent and effluent of the WWTP, respectively. Gemfibrozil was detected at the highest concentrations in wastewaters taken from the influent and effluent of the WWTP in summer and winter. The lowest concentrations in the wastewater treatment plant were determined for fenofibrate compound in the influent, clofibric acid compound in the effluent in the summer, and clofibric acid compound in the influent and effluent in the winter. Lipid regulators have high persistence (log Kow: 2.5–5.2; half-life: 15–100 days). Bezafibrate and pravastatin compounds are excreted in the main form at high rates from the body. Lipid regulators have low water solubility, high log Kow values, and half-lives. Fenofibrate compounds are usually detected in wastewater at low concentrations due to their very small excretion from the body in the form of the parent compound. The oral doses of bezafibrate and pravastatin, which were predominantly detected in the samples, were excreted from the body at approximately 30% unchanged. Higher concentrations of lipid regulators were determined in all hospitals during the winter. This result can be explained by the tendency of the patients’ blood fat to increase during cold seasons (Ockene et al. 2004). Consumption of lighter foods during the summer months, depending on eating habits, reduces the consumption of cholesterol reducers.
In hospital wastewater, carbamazepine was detected at maximum concentrations of 7008 ng/L in summer and 85.9 ng/L in winter. In hospital wastewater, fluoxetine and diazepam were determined to be below the detection limit in all samples during the summer period. Lorazepam was determined to be below the detection limit in samples taken from hospitals, except for one hospital. Carbamazepine compounds were detected at 135 ng/L in the influent of the municipal WWTP and 100 ng/L in the effluent and in the summer period, while other compounds were detected to be below the detection limit. In the winter period, carbamazepine compound was determined as 11.9 ng/L, fluoxetine compound as 2.57 ng/L, lorazepam compound as 4.83 ng/L at the influent of the municipal WWTP, fluoxetine compound as 2.51 ng/L, and lorazepam compound as 2.53 ng/L at the effluent of the municipal WWTP. When the physicochemical properties of psychiatric drugs were examined, the water solubility of the fluoxetine compound was quite high compared to other compounds, and all of the investigated psychiatric compounds had high persistence (log Kow: 2.45–4.08). Most carbamazepine appears to be excreted from the body without being metabolized. Summer term sampling was carried out at the end of August. During the change of seasons, the rate of people experiencing depression increases, which may raise the use of psychiatric drugs. In addition, one factor affecting the pharmaceutical concentrations in wastewater is dilution during the rainy seasons. The most commonly detected carbamazepine compound is the most commonly used psychiatric drug in psychiatric conditions such as epilepsy, mania, bipolar disorder, and anxiety, and it is eliminated from the body in its main form at a rate of approximately 28–72% of the dose taken. It remains in the water phase due to its low adsorptive rate in the sludge.
The detected maximum concentrations of the cancer drugs in hospital wastewater were 5.59 ng/L for etoposide in summer and 3.93 ng/L for tamoxifen in winter in the present study. In the summer, tamoxifen was detected at 0.17 ng/L, which was the minimum concentration. The maximum concentrations in influent wastewater were 0.38 ng/L for cyclophosphamide in summer and 3.37 ng/L for tamoxifen in winter. The maximum concentrations in effluent wastewater were 0.11 ng/L for ifosfamide in summer and 3.31 ng/L for tamoxifen in winter. Etoposide was found below the limit of quantification in all the samples analyzed in winter. Concentrations of etoposide and cyclophosphamide in WWTP were lower than their concentrations in hospital effluent. Other cancer drugs have been detected in close concentrations in hospital wastewater and WWTP samples. Etoposide is a medicine that is supplied to hospitalized patients rather than for domestic use, and it is excreted from the body in the form of the parent compound at a rate of 5–22%. The log Kow value is quite low and tends to remain in the water phase. Etoposide can react rapidly with chlorine and decompose (Santana-Viera et al. 2019). Tamoxifen, which was detected at high concentrations in the winter period, has a longer half-life than other cancer drugs and was found at higher concentrations than other cancer drugs due to its persistence. Tamoxifen has a high consumption amount in breast cancer treatment. Additionally, it is used in reproductive control and hormone treatments for animals (Ferrando-Climent et al. 2014; Negreira et al. 2015). Cyclophosphamide is the most common drug and is a compound resistant to ozonation. Ifosfamide is prescribed less than the other investigated cancer drugs. Some studies have indicated that hospital wastewater and WWTPs contain low concentrations of cancer drugs (Santana-Viera et al. 2019; Ferrando-Climent et al. 2014; Ferre-Aracil et al. 2016). Santana-Viera et al. (2019) detected etoposide at concentrations of 376 ng/L and 620 ng/L in hospital wastewater in influent wastewater ranging from 620 to 5141 ng/L. Cyclophosphamide was detected in hospital wastewater at a concentration of 1218 ng/L and in effluent wastewater at a concentration of 91.3 ng/L. However, even at low concentrations, they can have a negative effect on aquatic biota, flora, and fauna. Additionally, continuous discharge, even at low concentrations, may cause their accumulation (Oliveira Klein et al. 2021).
In some studies, it has been determined that the pharmaceutical concentrations in wastewater show seasonal changes. For example, studies conducted in Switzerland and the USA have found that concentrations in winter were higher than those in summer (Valcarcel et al. 2013; Yu et al. 2013). Golovko et al. (2014) investigated 21 pharmaceuticals in WWTPs and reported that the total concentrations of target pharmaceuticals in WWTPs were higher during winter than during summer. Sui et al. (2011) and Yu et al. (2013) found higher pharmaceutical concentrations in wastewater in winter season. Seasonal conditions, regional factors, average age of the population, and processes of WWTPs can affect the presence of pharmaceuticals in wastewater (Golovko et al. 2014; Bueno et al. 2012). While the concentrations of pharmaceuticals in wastewater are generally higher in the winter season, the removals are higher in the summer season.
Pharmaceutical contribution from hospitals to municipal WWTP
The wastewater flow rate per bed was accepted as 1000 L/day for the purpose of determining the load brought by medicines used in hospitals in WWTPs (Metcalf and Eddy 2003), and the contributions from each hospital were calculated. The flow to the WWTP is 170,000 m3/day, with industrial flow accounting for 6%. Excluding industrial wastewater flow, the WWTP receives 159,800 m3/day. It is known that the foremost route of entry of pharmaceuticals into ecological systems is wastewater. Domestic usage, industry, and hospitals are thought to be the principal pharmaceutical sources in wastewater. According to some studies, hospitals are the most significant source of pharmaceutical load in municipal WWTPs, and it is recommended that their wastewater be discharged after pretreatment (Corre et al. 2012; Hawkshead 2008; Ternes et al. 2006). The pharmaceutical load and their contributions originating from each hospital are given in Table 6. In this study, the total pharmaceutical solids made from hospitals to the influent of WWTP were found to be 1.9% in the summer and 4.32% in the winter. Thomas et al. (2007) reported that the contribution from hospitals to municipal wastewater was less than 2% for other pharmaceuticals, excluding paracetamol compounds. Santos et al. (2013) determined the pharmaceutical contribution from hospitals to be between 0.03 and 8.9% for β-blockers, between 0.001 and 7.3% for lipid regulators, and between 0.009 and 11% for psychiatric drugs. Langford and Thomas (2009) discovered that hospitals contributed 11% of propranolol, 2% of atenolol, and less than 1% of carbamazepine and metoprolol. Azuma et al. (2016) detected 38 pharmaceutical compounds in the effluent of a hospital. The pharmaceutical contribution to the influent of the treatment plant at the effluent of the hospital ranged from < 0.1 to 14.8%. Ort et al. (2010) determined the contribution from hospitals to be 1.8%, 0.4%, 4.1%, and 4.1% for atenolol, carbamazepine, gemfibrozil, and metoprolol compounds, respectively. The contribution of analgesics and anti-inflammatories made to the municipal WWTP from 16 hospitals was determined to be 0.01–3.23% in the summer period and 0–1.74% in the winter for each hospital. The total contribution from hospitals was determined to be 11.3% and 7.09% in the summer and winter, respectively (Aydin et al. 2019a). The contribution of antibiotic for each hospital was determined to be 0.01–3.57% in the summer and 0.003–11.4% in the winter. The total contribution from hospitals was determined to be 13.07% and 28.19% in the summer and winter, respectively (Aydin et al. 2019b). When the previous studies and the results of this study were taken into account, it was concluded that the main pharmaceutical source in WWTPs was not hospitals.
Removal of pharmaceuticals in the WWTP
Pharmaceuticals are biologically active and resistant chemicals and are found in aquatic environments at levels of ng/L. The formation and concentration of pharmaceuticals in WWTP influents depend on socioeconomic status, consumption pattern, climatic conditions, and water consumption. However, the pharmaceutical concentrations in WWTP effluents depend on the properties of the pharmaceuticals and wastewater and the treatment processes applied (Khasawneh and Palaniandy 2021). The removal rates of pharmaceuticals in WWTPs are affected by the physicochemical properties of pharmaceuticals, such as polarity, volatility, persistence, adsorption, and lipophilicity (Majumder et al. 2019; Khasawneh and Palaniandy 2021). The removal performances of the four groups of pharmaceuticals in Konya WWTP are summarized in Fig. 1. It seems that pharmaceuticals had removal efficiencies between 0.68 and 100%. The Konya WWTP is designed to treat discharges from the equivalent of a population of 1,600,000. Its maximum treatment flow rate will be 300,000 m3/day by 2030. Considering the results, it can be said that the treatment provided the high removal of metoprolol, sotalol, and carbamazepine from target compounds in winter and propranolol, clofibric acid, gemfibrozil, pravastatin, tamoxifen, cyclophosphamide, and etoposide in summer. Low removal efficiencies were observed in winter for compounds with high removal rates in summer.

Removal efficiency of selected pharmaceuticals in municipal WWTP
Temperature is one of the foremost environmental factors inducing low removal efficiencies in cold seasons (Evgenidou et al. 2015). Biodegradation kinetic is slower than the one in summer on account of low temperatures in cold seasons on biological wastewater treatment processes (Ma et al. 2013). In distinct studies, it was reported that seasonal conditions have an influence on the elimination of pharmaceutical compounds found in wastewater treatment plants. For instance, it was reported that pharmaceutical compounds were removed in higher yields in summer in Greece (Kosma et al. 2014). Vieno et al. (2005) assigned a decrease in the removal efficiency of pharmaceutical compounds for the rate of biodegradation in winter. While Castiglioni et al. (2006) pointed out that the removal rates of pharmaceuticals are higher in summer than in winter, Yu et al. (2013) did not observe a substantial difference between the removal efficiencies obtained in both periods. Sun et al. (2014) determined that some pharmaceuticals were removed in the activated sludge biological treatment process at a higher rate in winter than in summer, and a positive correlation was found between hydraulic holding time and removal rates and it was stated that the treatment efficiency of some pharmaceuticals may decrease owing to the reduced hydraulic holding time in hot seasons. Similarly, in our study, most of the pharmaceuticals investigated were eliminated at higher rates during the summer period. Some pharmaceuticals showed higher removal rates in winter. Similar to the literature studies, these removals were observed in the biological treatment plant due to the temperature and hydraulic holding time.
The average removal efficiency was found to be 50–77% for atenolol and fluoxetine and < 50% for metoprolol, as reported by Kumar et al. (2019). A WWTP from which the samples were taken had a primary treatment and a secondary treatment containing a five-stage Bardenpho process and a membrane bioreactor (MBR). Papageorgiou et al. (2016) reported negative removal rates and high removal rates for 55 pharmaceuticals in different therapeutic groups. They reported that the investigated WWTP is not able to efficiently remove complex mixtures of pharmaceuticals. In our study, it was reported that the removal efficiencies varied in a wide range (0.73–100%). Similar to the work of Papageorgiou et al. (2016), WWTPs are said to be insufficient in pharmaceutical treatment. Pharmaceuticals cannot be completely removed from wastewater in conventional treatment processes. Advanced treatment processes can be applied to remove pharmaceuticals from wastewater. Successful results have been acquired in the removal of pharmaceuticals by advanced oxidation methods (Bautitz and Nogueira, 2007; Wang and Wang 2016). For example, diazepam and bezafibrate removed 100% (Bautitz and Nogueira, 2010; Trovo et al. 2008), carbamazepine removed > 90% (Mohapatra et al. 2013), and gemfibrozil removed > 80% (Li et al. 2012) from wastewater by the Fenton oxidation process. Kim et al. (2009) investigated that 100% removal of bezafibrate, atenolol, metoprolol, propranolol, diazepam, and carbamazepine and more than 90% removal of clofibric acid were achieved with the UV/H2O2.
Environmental risk assessment
More than 200 pharmaceuticals have been detected in environmental matrices, such as different water sources and wastewater. The fate of pharmaceuticals and their effects on humans and the environment are uncertain (Couto et al. 2019). Most pharmaceutical compounds have high polarity and low volatility. Even at extremely low concentrations in the aquatic environment, they can have substantial ecotoxicological consequences, such as bioaccumulation, endocrine disruption, and drug resistance. Pharmaceutical concerns include an increase in the prevalence of cancer, antibiotic resistance, reproductive harm, and aberrant physiological processes (Wang et al. 2021). Table 7 comprises the pharmaceutical risk assessments for effluent wastewater in this study and literature studies. When “insignificant risk” is identified, the result is “acceptable” for the receiving environment; when “low risk” is identified, “more research” is necessary, and “detailed assessment” is required for the receiving environment in cases where “medium and high risk” is detected. Additionally, in this study, hospital wastewater and influent wastewater were evaluated in terms of risk. In the summer period, atenolol compounds showed a medium risk for fish in hospital wastewater and a high risk in the influent of WWTP. In hospital wastewater, propranolol and carbamazepine compounds showed a low risk for fish, Daphnia magna, and algae. During the winter, while atenolol compounds showed a high risk for fish in hospital wastewater and a moderate risk in the effluent municipal WWTP, the fluoxetine compound demonstrated a low risk for algae both in hospital wastewater and in the influent of the municipal WWTP. When Table 7 was examined, atenolol showed a moderate risk for fish in the summer and winter periods in this study. Fluoxetine showed a low risk for algae, and an insignificant risk was detected with other pharmaceuticals in this study. Mendoza et al. (2015) showed a high environmental risk for fish from propranolol and a medium risk for Daphnia magna from bezafibrate. Biel-Maeso et al. (2018b) identified a moderate risk for algae from propranolol.
Conclusions
This study addresses the analysis of four groups of pharmaceutical concentrations in hospital wastewaters and WWTP in summer and winter. The 18 target pharmaceuticals were detected at different concentrations (maximum, 7008 ng/L for carbamazepine). Beta-blockers and psychiatric pharmaceuticals were detected at higher concentrations in wastewater. The total concentrations of pharmaceutical groups in hospital wastewater were higher during winter than during summer, except psychiatric pharmaceuticals. In the WWTP, the total concentrations of lipid regulators and cancer pharmaceutical groups were higher in winter. It is still necessary to perform detailed studies on seasonal change. The contribution of the 16 hospitals to WWTP influent varied between 0.00005 and 1.818%. Flow rates of hospital wastewater remained at very low levels compared to WWTP influent. Therefore, pharmaceuticals detected in high concentrations in hospital wastewater are a small contribution. It has been concluded that pharmaceutical discharge from hospitals does not create a serious load on WWTPs. However, it is thought that the continuous discharge of pharmaceuticals from hospitals should be controlled. In this study, the environmental risk for Daphnia, fish, and algae was evaluated. The obtained results highlight that pharmaceuticals in WWTP effluent may pose a medium–high risk to aquatic life. However, more studies are still needed to identify the toxicities of pharmaceuticals for nontarget organisms. The observed removal efficiencies vary over a wide range for the investigated pharmaceuticals in WWTPs. Some compounds (metoprolol and carbamazepine in winter seasons and propranolol and tamoxifen in summer seasons) were completely eliminated during treatment. Our current research has shown that conventional treatment can be efficient for pharmaceutical removal. However, pharmaceutical removal depends on many factors, such as social and environmental conditions. Conventional systems under different operating conditions should be examined in detail.
References
Ajo P, Preis S, Vornamoa T, Mänttäri M, Kallioinen M, Louhi-Kultanen M (2018) Hospital wastewater treatment with pilot-scale pulsed corona discharge for removal of pharmaceutical residues. J Environ Chem Eng 6:1569–1577
Al Aukidya M, Verlicchi P, Jelic A, Petrovic M, Barcelò D (2012) Monitoring release of pharmaceutical compounds: Occurrence and environmental risk assessment of two WWTP effluents and their receiving bodies in the Po Valley, Italy. Sci Total Environ 438:15–25
Alder AC, Schaffner C, Majewsky M, Klasmeier J, Fenner K (2010) Fate of beta-blocker human pharmaceuticals in surface water: comparison of measured and simulated concentrations in the Glatt Valley Watershed, Switzerland. Water Res 44:936–948
APHA (1992) Standard methods for the examination of water and waste water, 17th edn. American Public Health Association, Washington
Ashfaq M, Khan KN, Rehman MSU, Mustafa G, Nazar MF, Sun Q, Iqbal J, Mulla SI, Yu C-P (2017) Ecological risk assessment of pharmaceuticals in the receiving environment of pharmaceutical wastewater in Pakistan. Ecotoxicol Environ Saf 136:31–39
Aydin S, Aydin ME, Ulvi A (2019a) Monitoring the release of anti-inflammatory and analgesic pharmaceuticals in the receiving environment. Environ Sci Pollut Res 26:36887–36902
Aydin S, Aydin ME, Ulvi A, Kiliç H (2019b) Antibiotics in hospital effluents: occurrence, contribution to urban wastewater, removal in a wastewater treatment plant, and environmental risk assessment. Environ Sci Pollut Res 26:544–558
Azuma T, Arima N, Tsukada A, Hirami S, Matsuoka R, Moriwake R, Ishiuchi H, Inoyama T, Teranishi Y, Yamaoka M, Mino Y, Hayashi T, Fujita Y, Masada M (2016) Detection of pharmaceuticals and phytochemicals together with their metabolites in hospital effluents in Japan, and their contribution to sewage treatment plant influents. Sci Total Environ 548-549:189–197
Bartrons M, Peñuelas J (2017) Pharmaceuticals and personal-care products in plants. Trends Plant Sci 22:194–203
Bautitz IR, Nogueira RFP (2007) Degradation of tetracycline by photo-Fenton process—solar irradiation and matrix effects. J Photochem Photobiol A Chem 187(1):33–39
Bautitz IR, Nogueira RFP (2010) Photodegradation of lincomycin and diazepam in sewage treatment plant effluent by photo-Fenton process. Catal Today 151(1–2):94–99
Belhaj D, Baccar R, Jaabiri I, Bouzid J, Kallel M, Ayadi H, Zhou JL (2015) Fate of selected estrogenic hormones in an urban sewage treatment plant in Tunisia (North Africa). Sci Total Environ 505:154–160
Biel-Maeso M, Corada-Fernandez C, Lara-Martín PA (2018a) Monitoring the occurrence of pharmaceuticals in soils irrigated with reclaimed wastewater. Environ Pollut 235:312–321
Biel-Maeso M, Baena-Nogueras RM, Corada-Fernández C, Lara-Martín PA (2018b) Occurrence, distribution and environmental risk of pharmaceutically active compounds (PhACs) in coastal and ocean waters from the Gulf of Cadiz (SW Spain). Sci Total Environ 612:649–659
Bueno MJM, Gomez MJ, Herrera S, Hernando MD, Aguera A, Fernandez-Alba AR (2012) Occurrence and persistence of organic emerging contaminants and priority pollutants in five sewage treatment plants of Spain: two years pilot survey monitoring. Environ Pollut 164:267–273
Castiglioni S, Bagnati R, Fanelli R, Pomati F, Calamari D, Zuccato E (2006) Removal of pharmaceuticals in sewage treatment plants in Italy. Environ Sci Technol 40:357–363
Chen X, Lei L, Liu S, Han J, Li R, Men J, Li L, Wei L, Sheng Y, Yang L, Zhou B, Zhu B (2021) Occurrence and risk assessment of pharmaceuticals and personal care products (PPCPs) against COVID-19 in lakes and WWTP-river-estuary system in Wuhan. China. SciTotal Environ 792. https://doi.org/10.1016/j.scitotenv.2021.148352
Cleuvers M (2005) Initial risk assessment for three β-blockers found in the aquatic environment. Chemosphere 59:199–205
Corre KSL, Ort C, Kateley D, Allen B, Escher BI, Keller J (2012) Consumption-based approach for assessing the contribution of hospitals towards the load of pharmaceutical residues in municipal wastewater. Environ Int 45:99–111
Couto CF, Lange LC, Amaral MCS (2019) Occurrence, fate and removal of pharmaceutically active compounds (PhACs) in water and wastewater treatment plants—a review. J Water Process Eng 32:100927
Dai G, Huang J, Chen W, Wang B, Yu G, Deng S (2014) Major pharmaceuticals and personal care products (PPCPs) in wastewater treatment plant and receiving water in Beijing, China, and associated ecological risks. Bull Environ Contam Toxicol 92:655–661
Deblonde T, Hartemann P (2013) Environmental impact of medical prescriptions: assessing the risks and hazards of persistence, bioaccumulation and toxicity of pharmaceuticals. Public Health 127:312–317
Escher BI, Baumgartner R, Koller M, Treyer K, Lienert J, McArdell CS (2011) Environmental toxicology and risk assessment of pharmaceuticals from hospital wastewater. Water Res 45:75–92
Evgenidou EN, Konstantinou IK, Lambropoulou DA (2015) Occurrence and removal of transformation products of PPCPs and illicit drugs in wastewaters: a review. Sci Total Environ 505:905–926
Ferrando-Climent L, Rodriguez-Mozaz S, Barcelo D (2014) Incidence of anticancer drugs in an aquatic urban system: from hospital effluents through urban wastewater to natural environment. Environ Pollut 193:216–223
Ferre-Aracil J, Valcárcel Y, Negreira N, Lópezde Alda M, Barceló D, Cardona SC, Navarro-Laboulais J (2016) Ozonation of hospital raw wastewaters for cytostatic compounds removal. Kinetic modelling and economic assessment of the process. Sci Total Environ 556:70–79
Ferrey ML, Hamilton MC, Backe WJ, Anderson KE (2018) Pharmaceuticals and other anthropogenic chemicals in atmospheric particulates and precipitation. Sci Total Environ 612:1488–1497
Galani A, Alygizakis N, Aalizadeh R, Kastritis R, Dimopoulos MA, Thomaidis NS (2021) Patterns of pharmaceuticals use during the first wave of COVID-19 pandemic in Athens, Greece as revealed by wastewater-based epidemiology. Sci Total Environ 798. https://doi.org/10.1016/j.scitotenv.2021.149014
Golovko O, Kumar V, Fedorova G, Randak T, Grabic R (2014) Seasonal changes in antibiotics, antidepressants/psychiatric drugs, antihistamines and lipid regulators in a wastewater treatment plant. Chemosphere 111:418–426
Gomez MJ, Petrovic M, Fernandez-Alba AR, Barcelo D (2006) Determination of pharmaceuticals of various therapeutic classes by solid-phase extraction and liquid chromatography–tandem mass spectrometry analysis in hospital effluent wastewaters. J Chromatogr A 1114:224–233
Gouvei TAI, Silva AMT, Ribeiro AR, Alves A, Santos MSF (2020) Liquid-liquid extraction as a simple tool to quickly quantify fourteen cytostatics in urban wastewaters and access their impact in aquatic biota. Sci Total Environ 740:139995
Gros M, Petrović M, Ginebreda A, Barceló D (2010) Removal of pharmaceuticals during wastewater treatment and environmental risk assessment using hazard indexes. Environ Int 36:15–26
Hawkshead J (2008) Hospital wastewater containing pharmaceutically active compounds and drug resistant organisms: a source of environmental toxicity and increased antibiotic resistance. J Residuals Sci Technol 5(2):51–60
Hena S, Gutierrez L, Croué J-P (2021) Review. Removal of pharmaceutical and personal care products (PPCPs) from wastewater using microalgae: a review. J Hazard Mater 403:124041
Hernando MD, Mezcua M, Fernandez-Alba AR, Barcelo D (2006) Environmental risk assessment of pharmaceutical residues in wastewater effluents, surface waters and sediments. Talanta 69:334–342
Isidori M, Lavorgna M, Russo C, Kundi M, Zegura B, Novak M, Filipic M, Misík M, Knasmueller S, Lopez de Alda M, Barcelo D, Zonja B, Cesen M, Scanar J, Kosjek T, Heath E (2016) Chemical and toxicological characterisation of anticancer drugs in hospital and municipal wastewaters from Slovenia and Spain. Environ Pollut 219:275–287
Kasprzyk-Hordern B, Dinsdale RM, Guwy AJ (2009) The removal of pharmaceuticals, personal care products, endocrine disruptors and illicit drugs during wastewater treatment and its impact on the quality of receiving waters. Water Res 43:363–380
Khasawneh OFS, Palaniandy P (2021) Occurrence and removal of pharmaceuticals in wastewater treatment plants. Process Saf Environ Prot 150:532–556
Khan NA, Vambol V, Vambol S, Bolibrukh B, Sillanpaa M, Changani F, Esrafili Yousefi M (2021) Hospital effluent guidelines and legislation scenario around the globe: A critical review. J Environ Chem Eng 9(5). https://doi.org/10.1016/j.jece.2021.105874
Kim I, Yamashita N, Tanaka H (2009) Performance of UV and UV/H2O2 processes for the removal of pharmaceuticals detected in secondary effluent of a sewage treatment plant in Japan. J Hazard Mater 166:1134–1140
Kosma CI, Lambropoulou DA, Albanis TA (2014) Investigation of PPCPs in wastewater treatment plants in Greece: occurrence, removal and environmental risk assessment. Sci Total Environ 466:421–438
Kosma CI, Nannou CI, Boti VI, Albanis TA (2019) Psychiatrics and selected metabolites in hospital and urban wastewaters: occurrence, removal, mass loading, seasonal influence and risk assessment. Sci Total Environ 659:1473–1483
Kovalova L, Siegrist H, Singer H, Wittmer A, McArdell CS (2012) Hospital wastewater treatment by membrane bioreactor: performance and efficiency for organic micropollutant elimination. Environ Sci Technol 46:1536–1545
Kumar R, Sarmah AK, Padhye LP (2019) Fate of pharmaceuticals and personal care products in a wastewater treatment plant with parallel secondary wastewater treatment train. J Environ Manag 233:649–659
Kuroda K, Li C, Dhangar K, Kumar M (2021) Predicted occurrence, ecotoxicological risk and environmentally acquired resistance of antiviral drugs associated with COVID-19 in environmental waters. Sci Total Environ 776(1). https://doi.org/10.1016/j.scitotenv.2021.145740
Lajeunesse A, Smyth SA, Barclay K, Sauve S, Gagnon C (2012) Distribution of antidepressant residues in wastewater and biosolids following different treatment processes by municipal wastewater treatment plants in Canada. Water Res 46:5600–5612
Langford KH, Thomas KV (2009) Determination of pharmaceutical compounds in hospital effluents and their contribution to wastewater treatment works. Environ Int 35(5):766–770
Li W, Nanaboina V, Zhou Q, Korshin GV (2012) Effects of Fenton treatment on the properties of effluent organic matter and their relationships with the degradation of pharmaceuticals and personal care products. Water Res 46(2):403–412
Lin AY-C, Tsai Y-T (2009) Occurrence of pharmaceuticals in Taiwan’s surface waters: impact of waste streams from hospitals and pharmaceutical production facilities. Sci Total Environ 407:3793–3802
Ma C, Yu S, Shia W, Heijman SGJ, Rietvel LC (2013) Effect of different temperatures on performance and membrane fouling in high concentration PAC–MBR system treating micro-polluted surface water. Bioresour Technol 141:19–24
Ma L, Liu Y, Zhang J, Yang Q, Li G, Zhang D (2018) Impacts of irrigation water sources and geochemical conditions on vertical distribution of pharmaceutical and personal care products (PPCPs) in the vadose zone soils. Sci Total Environ 626:1148–1156
Majumder A, Gupta B, Gupta AK (2019) Pharmaceutically active compounds in aqueous environment: a status, toxicity and insights of remediation. Environ Res 176:108542
Maniakova G, Kowalska K, Murgolo S, Mascolo GG, Libralato G, Lofrano G, Sacco O, Guida M, Rizzo L (2020) Comparison between heterogeneous and homogeneous solar driven advanced oxidation processes for urban wastewater treatment: pharmaceuticals removal and toxicity. Sep Purif Technol 236:116249
Martínez-Alcala I, Guillén-Navarro JM, Lahora A (2021) Occurrence and fate of pharmaceuticals in a wastewater treatment plant from southeast of Spain and risk assessment. J Environ Manag 279:111565
Melchor-Martínez EM, Jiménez-Rodríguez MG, Martínez-Ruiz M, Peña-Benavides SA, Iqbal HMN, Parra-Saldívar R, Sosa-Hernández JE (2021) Antidepressants surveillance in wastewater: overview extraction and detection. CSCEE 3:100074
Mendoza A, Aceña J, Pérez S, López de Alda M, Barceló D, Gil A, Valcárce Y (2015) Pharmaceuticals and iodinated contrast media in a hospital wastewater: a case study to analyse their presence and characterise their environmental risk and hazard. Environ Res 140:225–241
Metcalf & Eddy, Inc (2003) In: Burton FL (ed) Wastewater engineering: treatment and reuse. George Tchobanoglous G. McGraw-Hill, New York
Mohapatra D, Brar S, Tyagi R, Picard P, Surampalli R (2013) A comparative study of ultrasonication, Fenton’s oxidation and ferro-sonication treatment for degradation of carbamazepine from wastewater and toxicity test by Yeast Estrogen Screen (YES) assay. Sci Total Environ 447:280–285
Negreira N, Alda ML, Barcelo D (2014) Cytostatic drugs and metabolites in municipal and hospital wastewaters in Spain: filtration, occurrence, and environmental risk. Sci Total Environ 497-498:68–77
Negreira N, Regueiro J, López de Alda M, Damià Barceló D (2015) Transformation of tamoxifen and its major metabolites during water chlorination: identification and in silico toxicity assessment of their disinfection byproducts. Water Res 85:199–207
Nielsen U, Hastrup C, Klausen MM, Pedersen BM, Kristensen GH, Jansen JLC, Bak SN, Tuerk J (2013) Removal of APIs and bacteria from hospital wastewater by MBR plus O3, O3 + H2O2, PAC or ClO2. Water Sci Technol 67(4):854–862
Ockene IS, Chiriboga DE, Stanek EJ, Harmatz MG, Nicolosi R, Saperia G, Well AD, Freedson P, Merriam PA, Reed G, Ma Y, Matthews CE, Hebert JR (2004) 2004, Seasonal variation in serum cholesterol levels: treatment implications and possible mechanisms. Arch Intern Med 164(8):863–870
Oliveira Klein MD, Serrano SV, Santos-Neto A, Cruz CD, Brunetti IA, Lebre D, Gimenez MP, Reis RM, Silveira HSC (2021) Detection of anti-cancer drugs and metabolites in the effluents from a large Brazilian cancer hospital and an evaluation of ecotoxicology. Environ Pollut 268(Part A):115857
Oliveira TS, Murphy M, Mendola N, Wong V, Carlson D, Waring L (2015) Characterization of pharmaceuticals and personal care products in hospital effluent and wastewater influent/effluent by direct-injection LC-MS-MS. Sci Total Environ 518-519:459–478
Ort C, Lawrence MG, Reungoat J, Eaglesham G, Carter S, Keller J (2010) Determining the fraction of pharmaceutical residues in wastewater originating from a hospital. Water Res 44(2):605–615
Paíga P, Correia M, Fernandes MJ, Silva A, Carvalho M, Vieira J, Jorge S, Silva JG, Freire C, Delerue-Matos C (2019) Assessment of 83 pharmaceuticals in WWTP influent and effluent samples by UHPLC-MS/MS: hourly variation. Sci Total Environ 648:582–600
Papageorgiou M, Kosma C, Lambropoulou D (2016) Seasonal occurrence, removal, mass loading and environmental risk assessment of 55 pharmaceuticals and personal care products in a municipal wastewater treatment plant in Central Greece. Sci Total Environ 543(Part A):547–569
Perez-Alvarez I, Islas-Flores H, Gomez-Olivan LM, Barcelo D, Lopez De Alda M, Solsona SP, Sanchez-Aceves L, SanJuan-Reyes N, Galar-Martínez M (2018) Determination of metals and pharmaceutical compounds released in hospital wastewater from Toluca, Mexico, and evaluation of their toxic impact. Environ Pollut 240:330–341
Perrodin Y, Christine B, Sylvie B, Alain D, Jean-Luc B-K, Cécile C-O, Audrey R, Elodie B (2013) A priori assessment of ecotoxicological risks linked to building a hospital. Chemosphere 90:1037–1046
Ramil M, El Aref T, Fink G, Scheurer M, Ternes TA (2010) Fate of beta blockers in aquatic-sediment systems: sorption and biotransformation. Environ Sci Technol 44:962–970
Santana-Viera S, Hernández-Arencibia P, Sosa-Ferrera Z, Santana-Rodríguez JJ (2019) Simultaneous and systematic analysis of cytostatic drugs in wastewater samples by ultra-high performance liquid chromatography tandem mass spectrometry. J Chromatogr A B 1110–1111:124–132
Santos L, Gros M, Rodriguez-Mozaz S, Delerue-Matos C, Pena A, Barceló D, Montenegro MC (2013) Contribution of hospital effluents to the load of pharmaceuticals in urban wastewaters: identification of ecologically relevant pharmaceuticals. Sci Total Environ 461:302–316
Semerjian L, Shanableh A, Semreen MH, Samaraie M (2018) Human health risk assessment of pharmaceuticals in treated wastewater reused for non-potable applications in Sharjah, United Arab Emirates. Environ Int 121(Part 1):325–331
Sui Q, Huang J, Deng SB, Chen WW, Yu G (2011) Seasonal variation in the occurrence and removal of pharmaceuticals and personal care products in different biological wastewater treatment processes. Environ Sci Technol 45:3341–3348
Sun Q, Lv M, Anyi HA, Yang X, Yu C-P (2014) Seasonal variation in the occurrence and removal of pharmaceuticals and personal care products in a wastewater treatment plant in Xiamen, China. J Hazard Mater 277:69–75
Ternes AT, Giger W, Joss A (2006) Introduction. In: Ternes AT, Joss A (eds) Human pharmaceuticals, hormones and fragrances, the challenges of micropollutants in urban water management, 453rd edn. IWA Publishing, London, pp 1–13
Thomas KV, Dye C, Schlabach M, Langford KH (2007) Source to sink tracking of selected human pharmaceuticals from two Oslo city hospitals and a wastewater treatment works. J Environ Monit 9(12):1410–1418
Tormo-Budowski R, Cambronero-Heinrichs JC, JEJ D, Masís-Mora M, Ramírez-Morales D, Quirós-Fournier JP, Rodríguez-Rodríguez CE (2021) Removal of pharmaceuticals and ecotoxicological changes in wastewater using Trametes versicolor: a comparison of fungal stirred tank and trickle-bed bioreactors. Chem Eng Sci 410(15):128210
Trovo AG, Melo SAS, Nogueira RFP (2008) Photodegradation of the pharmaceuticals amoxicillin, bezafibrate and paracetamol by the photo-Fenton process - application to sewage treatment plant effluent. J Photochem Photobiol A Chem 198(2):215–220
Valcarcel Y, Alonso SG, Rodriguez-Gil JL, Castano A, Montero JC, Criado-Alvarez JJ, Miron IJ, Catala M (2013) Seasonal variation of pharmaceutically active compounds in surface (Tagus River) and tap water (Central Spain). Environ Sci Pollut Res 20(3):1396–1412
Vaudreuil M-A, Duy SV, Munoz G, Furtos A, Sauvé S (2020) A framework for the analysis of polar anticancer drugs in wastewater: on-line extraction coupled to HILIC or reverse phase LC-MS/MS. Talanta. 220:121407
Verlicchi P, Al Aukidy M, Galletti A, Petrovic M, Barceló D (2012a) Hospital effluent: investigation of the concentrations and distribution of pharmaceuticals and environmental risk assessment. Sci Total Environ 430:109–118
Verlicchi P, Al Aukidy M, Zambello E (2012b) Occurrence of pharmaceutical compounds in urban wastewater: removal, mass load and environmental risk after a secondary treatment-a review. Sci Total Environ 429:123–155
Vieno NM, Tuhkanen T, Kronberg L (2005) Seasonal variation in the occurrence of pharmaceuticals in effluents from a sewage treatment plant and in the recipient water. Environ Sci Technol 39:8220–8226
Vieno N, Tuhkanen T, Kronberg L (2007) Elimination of pharmaceuticals in sewage treatment plants in Finland. Water Res 41:1001–1012
Villar-Navarro E, Baena-Nogueras RM, Paniw M, Perales JA, Lara-Martín PA (2018) Removal of pharmaceuticals in urban wastewater: high rate algae pond (HRAP) based technologies as an alternative to activated sludge based processes. Water Res 139:19–29
Wang J, Wang S (2016) Removal of pharmaceuticals and personal care products (PPCPs) from wastewater: a review. J Environ Manag 182:620–640
Wang L, Fang J, Zhang X, Xu X, Kong X, Wu Z, Hua Z, Ren Z, Guo K (2019) Feasibility of the solar/chlorine treatment for lipid regulator degradation in simulated and real waters: the oxidation chemistry and affecting factors. Chemosphere 226:123–131
Wang H, Xi H, Xu L, Jin M, Zhao W, Liu H (2021) Ecotoxicological effects, environmental fate and risks of pharmaceutical and personal care products in the water environment: a review. Sci Total Environ 788:147819
Wilde ML, Mahmoud WM, Kümmerer K, Martins AF (2013) Oxidation-coagulation of β-blockers by K2FeVIO4 in hospital wastewater: assessment of degradation products and biodegradability. Sci Total Environ 452-453:137–147
Wu M, Xiang J, Que C, Chen F, Xu G (2015) Occurrence and fate of psychiatric pharmaceuticals in the urban water system of Shanghai, China. Chemosphere 138:486–493
Yi M, Sheng Q, Sui Q, Lu H (2020) β-blockers in the environment: distribution, transformation, and ecotoxicity. Environ Pollut 266(Part 2):115269
Yu Y, Wu LS, Chang AC (2013) Seasonal variation of endocrine disrupting compounds, pharmaceuticals and personal care products in wastewater treatment plants. Sci Total Environ 442:310–316
Yuan S, Jiang X, Xia X, Zhang H, Zheng S (2013) Detection, occurrence and fate of 22 psychiatric pharmaceuticals in psychiatric hospital and municipal wastewater treatment plants in Beijing, China. Chemosphere 90:2520–2525
Zuccato E, Calamari D, Natangelo M, Fanelli R (2000) Presence of therapeutic drugs in the environment. Lancet 355:1789–1790
Data availability
Not applicable.
Funding
This work was supported by the Turkish Academia of Sciences Awards for Outstanding Young Scientists (TÜBA-GEBIP) and Scientific Research Projects Coordination Unit of Necmettin Erbakan University, Project No.: 151419001.
Author information
Authors and Affiliations
Contributions
Senar Aydin: methodology, sampling and analyzing, and writing and reviewing
Arzu Ulvi: methodology, sampling and analyzing, and writing and reviewing
Mehmet Emin Aydin: methodology, sampling and analyzing, and writing including reviewing and editing
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Roland Peter Kallenborn
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 35 kb)
Rights and permissions
About this article

Cite this article
Ulvi, A., Aydın, S. & Aydın, M.E. Fate of selected pharmaceuticals in hospital and municipal wastewater effluent: occurrence, removal, and environmental risk assessment. Environ Sci Pollut Res 29, 75609–75625 (2022). https://doi.org/10.1007/s11356-022-21131-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-022-21131-y