
Abstract
Purpose
This study aimed to investigate the effectiveness of a 5-week virtual reality training protocol on static and dynamic balance and flexibility compared to a traditional training protocol in healthy adult females.
Methods
Twenty-one healthy female adults (age, 49.81 ± 2.99 years) were randomly assigned into three groups: Virtual Reality (VR; n = 7) that performed a 5-week exergame training protocol; Traditional Training (TR; n = 7) that performed a specific training protocol on balance, and lower limbs and abdominal strength; and waitlist control group (CG; n = 7) that continued their daily activities without any type of structured physical activity. Static balance was assessed by the ellipse area and statokinesigram parameters (Romberg test, in the open-eye (OE) and closed-eye (CE)), dynamic balance by the star excursion balance test on the right and left leg, and flexibility by the sit and reach test.
Results
After the intervention, VR and TR groups showed a significant improvement in static and dynamic balance and flexibility (all p < 0.001) compared to the CG. Compared to TR, the VR training protocol showed greater effect sizes and was more effective in percentage terms on all measured variables, particularly for Sit and Reach (82% vs. 35%), except the OE Area (42% vs. 49%).
Conclusions
Findings suggest that both a 5-week VR training protocol and a 5-week TR protocol may significantly improve static and dynamic balance and flexibility in healthy female adults. The VR training protocol showed a greater effect size compared to the TR training protocol, although it was not statistically significant. Future randomized controlled studies with a larger sample size and longer training protocols are needed to confirm this finding.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
To date, due to significant advances in medical knowledge and public health, there has been a significant increase in life expectancy with an increase in the elderly population. The World Health Organization (WHO) has predicted that the elderly will exceed 780 million people by 2025 [1]. This phenomenon has led to an increased focus on the lifestyle of the elderly. Maintaining balance and functional mobility understood as the ability to move from place to place, overcome obstacles and participate in activities of daily living is a fundamental requirement for maintaining a good quality of life [2]. Advancing age and related diseases can alter balance and the ability to perform activities of daily living and increase the risk of falls [3]. Although multiple factors and co-morbidities are related to falls in the elderly, balance and gait disorders are among the most common causes [4]. Reduced flexibility may affect stability while decreased balance may increase the risk of falls [5], particularly in women for whom there appears to be a higher incidence than in men [6]. In contrast to studies on the elderly population, subjects over the age of 65, little attention is given to fall risk factors in young and middle-aged adults [7]. The same authors suggest that falls defined as accidental can occur in people of all ages and is not exclusively limited to the elderly population. Traditional training that stimulates the vestibular system and motor control through monopodalic and bipodalic exercises on both flat surfaces and unstable platforms appears to be an excellent option for improving balance and preventing falls [8, 9].
Recently, the use of virtual reality and related exergames has emerged as a viable alternative to traditional training [10,11,12,13]. Exergames are interactive games that take advantage of virtual reality technology through three-dimensional camera systems combined with human skeletal tracking software, such as the Microsoft Kinect [10], which observes and reproduces users’ body movement live, providing users with the ability to correct and improve motor control [11]. These interactive games include both exercises whose main task is eye-hand coordination such as moving or grasping objects, and exercises with basic motor patterns such as jumping or sliding, but also sports games such as skiing, tennis, dancing or boxing, making these activities more enjoyable and motivating [12]. The field of use of virtual reality is wide-ranging; in fact, the scientific literature is studded with studies in which exergames are implicated both in rehabilitation strategies for cognitive-motor impairments such as Parkinson’s and stroke [13,14,15,16], both to promote psycho-physical wellbeing in the elderly by promoting the development of a healthy and active lifestyle [11, 17,18,19,20] but also to improve motor learning in young people of developmental age [21, 22]. Babadi and Daneshmandi [23] showed that a virtual reality training protocol using exergames was effective in improving balance compared to the control group but was not significantly more efficient than traditional training. In contrast, Sadeghi et al. [24] stated that an 8-week virtual training protocol was more effective in improving balance than the traditional protocol. Furthermore, they suggest that a combined training protocol is more efficient in improving balance than virtual and traditional training administered individually.
Ren et al. [25] in a meta-analysis suggest that virtual reality-based intervention was more effective than traditional interventions in improving physical function, balance, and reducing the risk of falling in the elderly with balance problems. Chen et al. [26] evidence that simplified and personalized Tai-Chi training conducted through of reality induced greater improvement in balance control and functional mobility than traditional Tai-Chi exercises. Moreira et al. [27] in a study designed to compare an exergame (EG) training program with a 12-week traditional multicomponent (MG) training program on a group of prefragile elderly, showed that EG might be a better alternative for improving cognition, while MG might be a better option for providing physical function gains. However, more recently Maranesi et al. [28] suggest that exergames can effectively train cognitive and physical domains as effectively as traditional exercises in individuals with Parkinson's disease.
Although a small number of studies investigated the effects of virtual training and confirmed its effectiveness in improving balance and flexibility, the authors did not always define the intensity, progressions, and structure of the protocols. Therefore, to date, it is not clear whether there is a significant difference between virtual training and traditional training based on structured protocols for improving balance and flexibility. Finally, the studies performed almost always used elderly subjects with associated co-morbidity, and considering the preventive value of exercise, it might be useful to evaluate healthy adult subjects. Therefore, this study aimed to investigate the effectiveness of a 5-week virtual training protocol on balance and flexibility compared to a traditional training protocol in healthy adult females.
Hypotheses
We hypothesized that: (1) a virtual training protocol would increase static and dynamic balance and flexibility in healthy adult females; (2) a virtual training protocol would more effectively increase static and dynamic balance and flexibility than a traditional training protocol.
Materials and methods
Study design and participants
This study used a prospective longitudinal randomized controlled study design. Test data were collected before and after five weeks of the experimental intervention to analyze the effects of a training protocol through virtual reality on balance and flexibility and compare it with a traditional training protocol. The data collection, pre- and post-treatment tests and training protocols were performed at an amateur sports association in the province of Bari (Italy).
To establish the sample size needed for the study, an a priori power analysis [29] with an assumed type I error (α) of 0.05 and a type II error rate (β) of 0.20 (80% statistical power) was calculated and revealed that 21 participants in total would be sufficient to observe moderate “time × group” interaction effects.
Twenty-one healthy adult females (mean age 49.81 ± 2.99 years) were recruited and randomly assigned to 3 groups: virtual reality training (VR; n = 7, age = 49.86 ± 3.18 years, body height = 161.14 ± 8.55 cm, body mass = 65.57 ± 9.59 kg, BMI = 25.24 ± 3.09 kg/m2); traditional training (TR; n = 7, age = 50.14 ± 2.67 years, body height = 165.00 ± 7.19 cm, body mass = 72.93 ± 14.86 kg, BMI = 26.78 ± 5.10 kg/m2); and waitlist control group (CG; n = 7, age = 49.43 ± 3.50 years, body height = 159.71 ± 5.79 cm, body mass = 60.43 ± 6.63 kg, BMI = 23.70 ± 2.47 kg/m2). Simple randomization was carried out through software available online (www.randomizer.org) and this allowed participants to be randomly assigned to groups preventing any selection bias since the influence of external factors or researcher biases in the distribution of participants was eliminated. In addition, the randomization list was kept hidden in the PC of one of the two researchers who then administered the treatments during the study. Body mass and body height were measured using the C201 Wunder medical scale. Body mass index (BMI) was calculated according to the formula: body mass in kg/body height in m2.
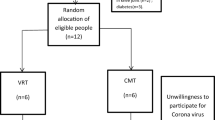
Forty adult females were contacted through e-mail invitations and word of mouth, without offering them any financial compensation. Before the start of the intervention, all participants signed an informed consent and self-reported their health status as healthy and all resided in the same city, with a roughly similar socio-economic background. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Bari University (protocol code 0015637|16/02/23). Firstly, we recognized several potential risks associated with the study. Physical risks were inherent in the training activities, whether virtual reality or traditional, as there was always a possibility of injury. Psychological risks also needed to be considered, as engaging in new activities could potentially cause anxiety or stress. To mitigate these risks, we implemented key strategies. One of the most important steps was obtaining informed consent from all participants. This process ensured that they were fully aware of the study's potential benefits, and risks. They were also assured that participation was voluntary and that they could withdraw from the study at any time without any repercussions. Eligibility screening process helped to reduce the likelihood of physical harm. During the training sessions, supervision by trained professionals was provided to address any immediate physical discomfort or injuries. Participants were also given a thorough orientation before the start of the study, which included detailed instructions on the training protocols, proper use of equipment, and safety measures. Monitoring the participants' health and well-being throughout the intervention was an ongoing process. In case of adverse events, we had a clear protocol for immediate response, including providing first aid and arranging professional support. Participants would have received ongoing support and referrals if needed to ensure full recovery. However, no adverse events were observed, likely due to our rigorous risk mitigation strategies and careful monitoring. All participants were informed in advance about the procedure, benefits, risks, and purpose of the study. Inclusion criteria were: (1) no training protocols aimed at improving the variables under analysis either through exergames or traditional training protocols in the last 6 months; (2) age between 45 and 55 years; (3) no history of injuries or fractures that would conflict with the study; (4) no intake of drugs that could affect postural control; (4) no alcohol intake for at least 12 h before the procedure. Participants were excluded in the presence of (1) pregnancy; (2) neurological diseases; (3) musculoskeletal pain; and (4) uncorrectable hearing and/or vision problems. A sample of healthy adult women, aged 45–50 years, made it possible to evaluate the effects of training protocols in the absence of confounders due to pre-existing conditions. An older sample would have brought with it a greater decline in physical and cognitive functions physiological to ageing. This aspect, in line with the primary objective of our study, allowed a more accurate comparison of the two training protocols. The flow chart of the study design is shown in Fig. 1.

Flow diagram of study design
Procedures and measures
Measurements were taken at baseline (pre-test) and after 5 weeks of intervention (post-test). Both pre- and post-intervention data were collected on 2 separate days; the post-test was performed 72 h after the training protocol. On the first day, flexibility and dynamic balance were assessed, and on the second day, static balance was assessed. All measurements were performed in the same order and by the same qualified operator blinded to the purposes of the study and groups allocation. In our study, we employed several strategies to ensure blinding and minimize bias. Firstly, the participants were unaware of the objective of the experimentation. Secondly, who administered the treatments were not involved in the collection or analysis of outcome data. This prevented them from potentially influencing the outcome assessments. The key to reducing bias in outcome assessments was blinding the outcome assessors. The outcome assessors were completely blind to the participants' treatment conditions. To achieve this, assessments were conducted using anonymous codes for participants, ensuring that the assessors did not know to which group the participants belonged. Additionally, measurement tools and data collection procedures were standardized to minimize the possibility of unconscious bias by the assessors. We verified the success of our blinding procedures by asking outcome assessors to guess the group allocation of participants at the end of the study. This allowed us to analyze whether their guesses were significantly better than chance, thereby confirming the effectiveness of the blinding. Additionally, all personnel involved in the study received a periodic monitoring and audits to ensure that blinding procedures were strictly adhered to throughout the study. These measures helped to minimize the risk of bias and ensure that the outcome assessors remained unaware of the participants' treatment conditions. The participants were unaware of the study hypotheses, but inevitably knew what type of training they were following, which could represent, even indirectly, a limitation to the blinding procedure.
Sit and reach test
The Sit and Reach test is a test widely used as a flexibility test of the lower back and posterior thigh muscles [30]. The test was performed using the Sit and Reach Box Metal. The participants performed the test without shoes and with their palms facing downwards. The examiner recorded the test after two seconds of maintaining maximum torso flexion. Each participant performed three trials, and the best score between the trials was recorded. The test–retest reliability reported high reliability for the sit and reach (ICC = 0.97).
Star excursion balance test
The Star Excursion Balance Test (SEBT) is a widely used field test to assess dynamic balance [31, 32] that is expressed as the maximum distance participants can reach with their foot in 8 directions while maintaining a one-legged stance. Participants performed the test without footwear and to be assessed they performed 2 familiarization tests. Each participant performed three trials, and the best score between the trials was recorded. The score was obtained by averaging the scores of the eight directions. The test–retest reliability reported high reliability for SEBT on the right (R) and left (L) leg (ICC = 0.94).
Romberg test
The Romberg test is widely used to assess static balance [33]. The stabilometric analysis consists of detecting body oscillations while the subject maintains the orthostatic position. The test was performed on the 6-cell stabilometric platform in the D-Wall (Tecnobody Srl, Dalmine, Italy), all participants performed the test without shoes in the open-eye (OE) and closed-eye (CE) variants for 30″. For the assessment of static balance, center of pressure (COP) parameters were considered, including ellipse of area and perimeter.
Intervention protocol
The intervention lasted five weeks. After data collection, the subjects of the VR and TR groups performed balance and flexibility training twice a week for a total of 10 sessions each lasted 60’, divided into three parts: (1) 10 min warm-up with aerobic warm-up and joint mobility; (2) 40 min training session; (3) 10 min cool down with stretching exercises and self-massage with a foam roller. The duration of the intervention was 5 weeks because it was based on the actual time availability and management skills of the participants. In addition, other studies have shown significant improvements in balance and flexibility with a frequency of two sessions per week [34, 35].
The CG were asked to continue their daily activities such as walking, hiking and outdoor outings but to avoid initiating any type of motor activity and structured exercise during the intervention period in order not to interfere with the trial. After completion of the study, they were invited to voluntarily participate in the program for 5 weeks by choosing the protocol to follow.
Virtual training
The VR group, training through virtual reality, performed training sessions using D-Wall (Tecnobody Srl, Dalmine, Italy) and Postural Bench. The D-Wall includes a 3D camera, a 65″ LCD screen, a 15.6″ touch screen tablet, a strength platform and a configuration software divided into Rehab, Health Fitness and Sport. The full HD infrared camera can detect the joints and body segments, position, and movements of the player. The immersive virtual reality on the screen of this system reproduces the player’s movements in virtual environments and provides visual and auditory biofeedback necessary to immediately correct the performance. For the intervention, the participants were positioned on the force platform 1.5–2 m from the camera. For physical conditioning and balance, the Sports package was used in the Move section, which includes games in a virtual environment such as skiing, football, basketball, tennis, and boxing. For motor control and cognitive conditioning, participants played 2 games from the Exergames package, which includes a total of 8 interactive games with different characteristics. Specifically, the games Equilibrium and Fly were proposed, in which movement control and COP control in both the anteroposterior and mid-lateral directions were required with precision. The executions dictated by the tasks of the different games were interspersed with 60″ of passive recovery. In addition, the interactive game implemented in the Postural Bench software was used for flexibility training. The intensity was progressively increased in relation to the levels of difficulty proposed in the various games. Every 4 training sessions the intensity was measured through the OMNI-Resistance Exercise of Perceived Exertion 0–10 scale, aiming for a perceived intensity between 7 and 8 [36] (Suppl.1).
Traditional training
The TR group performed traditional training sessions through free-body and counter-resistance muscle strengthening exercises, abdominal strengthening exercises and balance exercises in both monopodalic and bipodalic. Specifically, the participants performed timed standing, toe and heel exercises in both bipodalic and monopodalic, with open and closed eyes. In addition, they performed squats and lunges, farmer walks, calf raises, planks and lateral planks. Initially, both timed and repetition exercises were structured in 1–2 sets for 15″-20″ or 6–8 repetitions. The sets were interspersed with a 60″ passive recovery. As the participants progressed, the sets, running time, repetitions and loads were increased where appropriate up to 3 sets for 60″ or 12 repetitions for a perceived intensity of 70/80% of 1RM. Again, intensity was measured every 4 training sessions via the OMNI-Resistance Exercise of Perceived Exertion 0–10 scale, aiming for a perceived intensity between 7 and 8 [36].
Adherence and intervention fidelity
Training sessions were facilitated by a certified trainer and supervised by a researcher not involved in testing. The trainers monitored the rate of adherence with the use of logbooks. The mean number of sessions attended out of a total of 10 sessions were calculated.
Statistical analyses
Statistical analyses were conducted using the JASP software v. 0.17.2.1 (JASP Team, 2023; jasp-stats.org). Data were presented as group mean values ± standard deviations (SD) and were checked for assumptions of homogeneity of variances via Levene’s test. The Shapiro–Wilk test was used to test the normality of all variables. A two-way ANOVA [group (virtual training/traditional training/control group) × time (pre/post-intervention)] with repeated measures was performed to analyze the effect of the training on all dependent variables. Subsequently, when “group × time” interactions showed significance, Tukey's post-hoc test was conducted to identify significant comparisons within groups. Percentage changes were calculated as [(post-training value – pre-training value)/pre-training value] × 100.
Partial eta squared (\(\eta_{{\text{p}}}^{2}\)) was used to estimate the magnitude of the difference within each group and defined as follows: small: \(\eta_{{\text{p}}}^{2}\) < 0.06, moderate: 0.06 ≤ \(\eta_{{\text{p}}}^{2}\) < 0.14, and large effect size (ES): \(\eta_{{\text{p}}}^{2}\) ≥ 0.14. In addition, Cohen’s d was calculated for the post hoc tests. The criteria to interpret the magnitude of Cohen’s d were as follows: small: 0.20 ≤ d < 0.50, moderate: 0.50 ≤ d < 0.79, and large ES: d ≥ 0.80 [37]. Statistical significance was set a priori at p ≤ 0.05.
Results
Participant characteristics, adherence, and adverse events
Participant characteristics and anthropometric data measured at baseline are shown in Table 1. All participants completed the protocol, without drop-outs. A good adherence to the intervention protocols was reported, as all participants attended at least 85% of the exercise sessions. During the 5-week intervention period, no adverse events or health problems were observed in the participants. The participants were satisfied with the results of the intervention and stated that they intended to continue physical activity on their own.
Outcome measures
After the 5-week intervention, all the variables showed a significant Time × Group interaction (p < 0.001) that indicated the effectiveness of the experimental intervention. Tukey’s post-hoc test was then performed to investigate the differences within groups. Table 2 shows that for all variables considered, both virtual reality and traditional training protocols resulted in statistically significant improvements (p < 0.001), compared to the control group (p > 0.05).
The analysis showed that, for the OE Area (Fig. 2), the VR group (Δpre/post = − 85.40 ± 18.93 mm2; 95% CI 67.28–103.51) improved by 42% compared to the TR group (Δpre/post = − 85.50 ± 14.65 mm2; 95% CI 67.38–103.61), which improved by 49%.

Pre- and post-test changes for Open-Eye (OE) Area. Traditional and Virtual reality training groups showed large effect sizes
For the CE Area (Fig. 3), the VR group (Δpre/post = −108.48 ± 58.55 mm2; 95% CI 63.83–153.12) showed a 50% improvement over the TR group (Δpre/post = −82.13 ± 15.22 mm2; 95% CI 37.48–126.77), which improved by 43%.

Pre- and post-test changes for Closed-Eye (CE) Area. Traditional and Virtual reality training groups showed large effect sizes
For the OE Perimeter (Fig. 4), the VR group (Δpre/post = −90.36 ± 36.76 mm; 95% CI, 61.06 to 119.66) improved by 17% compared to the TR group (Δpre/post = −82.99 ± 12.04 mm; 95% CI 53.69–112.29), which improved by 16%.

Pre- and post-test changes for Open-Eye (OE) Perimeter. Traditional and Virtual reality training groups showed large effect sizes
For the CE Perimeter (Fig. 5), the VR group (Δpre/post = −107.43 ± 38.47 mm; 95% CI, 70.93 to 143.91) improved by 19% compared to the TR group (Δpre/post = −88.64 ± 30.61 mm; 95% CI 52.14–125.12), which improved by 17%.

Pre- and post-test changes for Closed-Eye (CE) Perimeter. Traditional and Virtual reality training groups showed large effect sizes
For the SEBT-R (Fig. 6), the VR group (Δpre/post = 4.84 ± 1.26 cm; 95% CI −6.03 to −3.64) improved by 8% compared to the TR group (Δpre/post = 3.80 ± 0.78 cm; 95% CI −5.00 to −2.61), which improved by 6%.

Pre- and post-test changes for Star Excursion Balance Test on the right leg (SEBT-R). Traditional training group showed small effect size. Virtual reality training group showed moderate effect size
For the SEBT-L (Fig. 7), the VR group (Δpre/post = 4.40 ± 1.23 cm; 95% CI −5.92 to −2.88) improved by 7% compared to the TR group (Δpre/post = 3.24 ± 1.44 cm; 95% CI −4.76 to −1.72), which improved by 5%.

Pre- and post-test changes for Star Excursion Balance Test on the left leg (SEBT-L). Traditional and Virtual reality training groups showed small effect sizes
For the Sit and Reach (Fig. 8), the VR group (Δpre/post = 3.33 ± 0.67 cm; 95% CI −4.06 to −2.59) improved by 82% compared to the TR group (Δpre/post = 2.10 ± 0.63 cm; 95% CI −2.83 to −1.36), which improved by 35%.

Pre- and post-test changes for Sit and Reach (S&R). Traditional training group showed moderate effect size. Virtual reality training group showed large effect size
Discussion
This study aimed to investigate the effectiveness of a 5-week virtual reality training protocol on balance and flexibility compared to a traditional training protocol in healthy adult females. It was hypothesized that: (1) a virtual training protocol would increase static and dynamic balance and flexibility in healthy adult females; (2) a virtual training protocol would more effectively increase static and dynamic balance and flexibility than a traditional training protocol.
After 5 weeks, we found a significant improvement in all measured variables in both the VR and TR groups. Therefore, the first hypothesis was confirmed. The results obtained agree with many other studies that have shown the effectiveness of virtual reality in improving balance and flexibility [5, 23, 38, 39]. Although both training protocols showed significant effectiveness between pre- and post-intervention, the virtual training protocol showed greater effect sizes and was more effective, albeit not significantly, in percentage terms on all measured variables, in particular for Sit and Reach, but except the OE Area. Therefore, the second hypothesis can be confirmed only partially.
The effectiveness of traditional training in preventing falls in the elderly is well documented [40, 41]. Concorde, Filipovi et al. [42] showed that a 12 week intervention can improve the performance of the Time Up and Go test and the One Leg Stance test in postmenopausal women. However, it is also known that traditional training may be monotonous, leading to low compliance and a high drop-out rate [11, 43]. In contrast, performing physical activity using exergames, besides being safe for the safety of the participants, is considered a hobby, which is why the training protocol is more fun [44] leading not only to stress reduction [45] but also improving the promotion and continuation of physical activity [12, 46]. This concept is highlighted in the review conducted by Costa et al. [38], in which they found that subjects undergoing an intervention through virtual reality showed significant improvement in concentration, challenge, skill development, sense of control, improved goal setting, feedback, immersion and opportunities for social interaction.
These effects could be explained by the fact that VR training protocol has a dual nature, requiring not only physical but also cognitive work at the same time. The cognitive stimulation promoted by interaction with the virtual environment would increase the efficiency of cognitive processing circuits, in particular executive functions such as working memory, planning and inhibition, to a greater extent than traditional training [47, 48].
The feedback provided by the virtual systems resulted in a series of continuous execution adjustments by shifting body weight from the heel to the toes, repeatedly stimulating the proprioceptors of the trunk, limbs and vestibular apparatus, which may have improved balance [49]. A previous study stated that Wii Fit users showed significantly improved vestibular and visual integration abilities compared with the control group immediately after training and at 1-month follow-up [50]. Furthermore, interaction with an on-screen avatar would promote the activation of mirror neurons, relating the observed to the action performed, which could promote motor learning.
Other studies have compared the effectiveness of virtual training with traditional training, confirming that exergames are an effective tool for achieving benefits in terms of balance, flexibility, and functional mobility in the elderly [3, 11]. However, it is known that accidental falls can occur in people of all ages and is not exclusively limited to the elderly population [7]. Therefore, a strength of our study is that the intervention was conducted on a group of adults, highlighting the importance of physical exercise as a prevention of fall risk factors. Furthermore, the improvements achieved in balance and flexibility allow participants to improve their quality of life, as they will be able to perform daily activities more easily [2]. The virtual reality protocol as well as the traditional one did not cause any adverse effects or health problems in the study participants; moreover, they were satisfied with the results of the study and expressed interest in continuing regular physical activity.
The present study had some limitations that must be considered when extrapolating conclusions based on the results. The study period was short, only 5 weeks. Probably the greater results in terms of percentage and effect size obtained from the virtual training protocol compared with the traditional protocol in all measured variables except OE Area were due to the short duration of the protocol. Thus, longer longitudinal studies are hoped to confirm the findings. Moreover, our subject population consisted exclusively of adult females. Another limitation is that the results therefore cannot be generalized to other populations, including adolescents, men, and the elderly, in addition, there may have been potential biases in self-reported health status.
Conclusions
The results suggest that a 5-week virtual reality training protocol may improve static and dynamic balance and flexibility in healthy adult females as much as a traditional training protocol. Given the benefits of exercise for maintaining stability and preventing falls and the lack of longitudinal studies investigating risk factors for falls in youth and adults, this was the first randomized controlled study that has attempted to fill this gap in the literature. Furthermore, given the promising results, it can be inferred that the use of virtual reality could be implemented in traditional protocols by physiotherapists and kinesiologists to enhance the therapeutic effects on balance and flexibility and fall prevention.
However, future randomized controlled trials with a different population from the one used to generalize the results, a larger size and longer training protocols are needed to confirm these results.
Data availability
The data presented in this study are available on request from the first author.
References
Dias GNF, Couceiro MS (2017) Active ageing and physical activity. Springer International Publishing
Forhan M, Gill SV (2013) Obesity, functional mobility and quality of life. Best Pract Res Clin Endocrinol Metab 27(2):129–137. https://doi.org/10.1016/j.beem.2013.01.003
Liu M, Zhou K, Chen Y, Zhou L, Bao D, Zhou J (2022) Is virtual reality training more effective than traditional physical training on balance and functional mobility in healthy older adults? A systematic review and meta-analysis. Front Hum Neurosci 16:843481. https://doi.org/10.3389/fnhum.2022.843481
Khanuja K, Joki J, Bachmann G, Cuccurullo S (2018) Gait and balance in the aging population: fall prevention using innovation and technology. Maturitas 110:51–56. https://doi.org/10.1016/j.maturitas.2018.01.021
Treml CJ, Kalil Filho FA, Ciccarino RFL, Wegner RS, Saita CYDS, Corrêa AG (2013) O uso da plataforma Balance board como recurso fisioterápico em idosos. Rev Bras Geriatr E Gerontol 16(4):759–768. https://doi.org/10.1590/S1809-98232013000400010
Stevens JA, Ballesteros MF, Mack KA, Rudd RA, DeCaro E, Adler G (2012) Gender differences in seeking care for falls in the aged medicare population. Am J Prev Med 43(1):59–62. https://doi.org/10.1016/j.amepre.2012.03.008
Talbot LA, Musiol RJ, Witham EK, Metter EJ (2005) Falls in young, middle-aged and older community dwelling adults: perceived cause, environmental factors and injury. BMC Public Health 5(1):86. https://doi.org/10.1186/1471-2458-5-86
El-Khoury F, Cassou B, Latouche A, Aegerter P, Charles MA, Dargent-Molina P (2015) Effectiveness of two year balance training programme on prevention of fall induced injuries in at risk women aged 75–85 living in community: ossébo randomised controlled trial. BMJ. https://doi.org/10.1136/bmj.h3830
Papalia GF, Papalia R, Diaz Balzani LA et al (2020) The effects of physical exercise on balance and prevention of falls in older people: a systematic review and meta-analysis. J Clin Med 9(8):2595. https://doi.org/10.3390/jcm9082595
Clark RA, Mentiplay BF, Hough E, Pua YH (2019) Three-dimensional cameras and skeleton pose tracking for physical function assessment: a review of uses, validity, current developments and kinect alternatives. Gait Posture 68:193–200. https://doi.org/10.1016/j.gaitpost.2018.11.029
Chen Y, Zhang Y, Guo Z, Bao D, Zhou J (2021) Comparison between the effects of exergame intervention and traditional physical training on improving balance and fall prevention in healthy older adults: a systematic review and meta-analysis. J NeuroEngineering Rehabil 18(1):164. https://doi.org/10.1186/s12984-021-00917-0
Buckinx F, Bruyère O, Lengelé L et al (2020) The effects of GAMotion (a giant exercising board game) on physical capacity, motivation and quality of life among nursing home residents: a pilot interventional study. Exp Gerontol 138:110983. https://doi.org/10.1016/j.exger.2020.110983
Harris DM, Rantalainen T, Muthalib M, Johnson L, Teo WP (2015) Exergaming as a viable therapeutic tool to improve static and dynamic balance among older adults and people with idiopathic parkinson’s disease: a systematic review and meta-analysis. Front Aging Neurosci. https://doi.org/10.3389/fnagi.2015.00167
Liao YY, Yang YR, Cheng SJ, Wu YR, Fuh JL, Wang RY (2015) Virtual reality-based training to improve obstacle-crossing performance and dynamic balance in patients with parkinson’s disease. Neurorehabil Neural Repair 29(7):658–667. https://doi.org/10.1177/1545968314562111
Ribas CG, Alves Da Silva L, Corrêa MR, Teive HG, Valderramas S (2017) Effectiveness of exergaming in improving functional balance, fatigue and quality of life in Parkinson’s disease: a pilot randomized controlled trial. Parkinsonism Relat Disord. 38:13–18. https://doi.org/10.1016/j.parkreldis.2017.02.006
Cikajlo I, Rudolf M, Mainetti R, Borghese NA (2020) Multi-exergames to set targets and supplement the intensified conventional balance training in patients with stroke: a randomized pilot trial. Front Psychol 11:572. https://doi.org/10.3389/fpsyg.2020.00572
Monteiro-Junior R, Vaghetti CO, Nascimento OJ, Laks J, Deslandes A (2016) Exergames: neuroplastic hypothesis about cognitive improvement and biological effects on physical function of institutionalized older persons. Neural Regen Res 11(2):201. https://doi.org/10.4103/1673-5374.177709
Van Diest M, Stegenga J, Wörtche HJ, Verkerke GJ, Postema K, Lamoth CJC (2016) Exergames for unsupervised balance training at home: a pilot study in healthy older adults. Gait Posture 44:161–167. https://doi.org/10.1016/j.gaitpost.2015.11.019
Street TD, Lacey SJ, Langdon RR (2017) Gaming your way to health: a systematic review of exergaming programs to increase health and exercise behaviors in adults. Games Health J 6(3):136–146. https://doi.org/10.1089/g4h.2016.0102
Htut TZC, Hiengkaew V, Jalayondeja C, Vongsirinavarat M (2018) Effects of physical, virtual reality-based, and brain exercise on physical, cognition, and preference in older persons: a randomized controlled trial. Eur Rev Aging Phys Act 15(1):10. https://doi.org/10.1186/s11556-018-0199-5
Graf DL, Pratt LV, Hester CN, Short KR (2009) Playing active video games increases energy expenditure in children. Pediatrics 124(2):534–540. https://doi.org/10.1542/peds.2008-2851
Sheehan D, Katz L (2010) Using interactive fitness and exergames to develop physical literacy. Phys Health Educ J 76(1):12–19
Yousefi Babadi S, Daneshmandi H (2021) Effects of virtual reality versus conventional balance training on balance of the elderly. Exp Gerontol 153:111498. https://doi.org/10.1016/j.exger.2021.111498
Sadeghi H, Jehu DA, Daneshjoo A et al (2021) Effects of 8 weeks of balance training, virtual reality training, and combined exercise on lower limb muscle strength, balance, and functional mobility among older men: a randomized controlled trial. Sports Health Multidiscip Approach 13(6):606–612. https://doi.org/10.1177/1941738120986803
Ren Y, Lin C, Zhou Q, Yingyuan Z, Wang G, Lu A (2023) Effectiveness of virtual reality games in improving physical function, balance and reducing falls in balance-impaired older adults: a systematic review and meta-analysis. Arch Gerontol Geriatr 108:104924. https://doi.org/10.1016/j.archger.2023.104924
Chen PJ, Penn IW, Wei SH, Chuang LR, Sung WH (2020) Augmented reality-assisted training with selected Tai-Chi movements improves balance control and increases lower limb muscle strength in older adults: a prospective randomized trial. J Exerc Sci Fit 18(3):142–147. https://doi.org/10.1016/j.jesf.2020.05.003
Moreira NB, Rodacki ALF, Costa SN, Pitta A, Bento PCB (2021) Perceptive-cognitive and physical function in prefrail older adults: exergaming versus traditional multicomponent training. Rejuvenation Res 24(1):28–36. https://doi.org/10.1089/rej.2020.2302
Maranesi E, Casoni E, Baldoni R et al (2022) The effect of non-immersive virtual reality exergames versus traditional physiotherapy in parkinson’s disease older patients: preliminary results from a randomized-controlled trial. Int J Environ Res Public Health 19(22):14818. https://doi.org/10.3390/ijerph192214818
Faul F, Erdfelder E, Lang AG, Buchner A (2007) G*power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 39(2):175–191. https://doi.org/10.3758/BF03193146
American College of Sports Medicine (2021) In: Liguori G, Feito Y, Fountaine C, Roy B (eds) ACSM's guidelines for exercise testing and prescription, 11th edn. Wolters Kluwer
Munro AG, Herrington LC (2010) Between-session reliability of the star excursion balance test. Phys Ther Sport 11(4):128–132. https://doi.org/10.1016/j.ptsp.2010.07.002
Hyong IH, Kim JH (2014) Test of intrarater and interrater reliability for the star excursion balance test. J Phys Ther Sci 26(8):1139–1141. https://doi.org/10.1589/jpts.26.1139
Lanska DJ, Goetz CG (2000) Romberg’s sign: development, adoption, and adaptation in the 19th century. Neurology 55(8):1201–1206. https://doi.org/10.1212/WNL.55.8.1201
Phu S, Vogrin S, Al Saedi A, Duque G (2019) Balance training using virtual reality improves balance and physical performance in older adults at high risk of falls. Clin Interv Aging 14:1567–1577. https://doi.org/10.2147/CIA.S220890
Cordes T, Bischoff LL, Schoene D et al (2019) A multicomponent exercise intervention to improve physical functioning, cognition and psychosocial well-being in elderly nursing home residents: a study protocol of a randomized controlled trial in the PROCARE (prevention and occupational health in long-term care) project. BMC Geriatr 19(1):369. https://doi.org/10.1186/s12877-019-1386-6
Robertson RJ, Goss FL, Rutkowski J et al (2003) Concurrent validation of the OMNI perceived exertion scale for resistance exercise. Med Sci Sports Exerc 35(2):333–341. https://doi.org/10.1249/01.MSS.0000048831.15016.2A
Cohen J (1992) A power primer. Psychol Bull 112(1):155–159. https://doi.org/10.1037/0033-2909.112.1.155
Costa MTS, Vieira LP, Barbosa EDO et al (2019) Virtual reality-based exercise with exergames as medicine in different contexts: a short review. Clin Pract Epidemiol Ment Health 15(1):15–20. https://doi.org/10.2174/1745017901915010015
Pacheco TBF, De Medeiros CSP, De Oliveira VHB, Vieira ER, De Cavalcanti FAC (2020) Effectiveness of exergames for improving mobility and balance in older adults: a systematic review and meta-analysis. Syst Rev 9(1):163. https://doi.org/10.1186/s13643-020-01421-7
Sherrington C, Michaleff ZA, Fairhall N et al (2017) Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med 51(24):1750–1758. https://doi.org/10.1136/bjsports-2016-096547
Patti A, Zangla D, Sahin FN et al (2021) Physical exercise and prevention of falls. Effects of a pilates training method compared with a general physical activity program: a randomized controlled trial. Medicine (Baltimore) 100(13):e25289. https://doi.org/10.1097/MD.0000000000025289
Filipović TN, Lazović MP, Backović AN et al (2021) A 12-week exercise program improves functional status in postmenopausal osteoporotic women: randomized controlled study. Eur J Phys Rehabil Med. https://doi.org/10.23736/S1973-9087.20.06149-3
Jorgensen MG, Laessoe U, Hendriksen C, Nielsen OBF, Aagaard P (2013) Efficacy of Nintendo Wii training on mechanical leg muscle function and postural balance in community-dwelling older adults: a randomized controlled trial. J Gerontol A Biol Sci Med Sci 68(7):845–852. https://doi.org/10.1093/gerona/gls222
Hall CD, Clevenger CK, Wolf RA, Lin JS, Johnson TM, Wolf SL (2016) Feasibility of a low-cost, interactive gaming system to assess balance in older women. J Aging Phys Act 24(1):111–118. https://doi.org/10.1123/japa.2014-0184
Kappen DL, Mirza-Babaei P, Nacke LE (2019) Older adults’ physical activity and exergames: a systematic review. Int J Hum Comput Interact 35(2):140–167. https://doi.org/10.1080/10447318.2018.1441253
Molina K, Ricci N, De Moraes S, Perracini M (2014) Virtual reality using games for improving physical functioning in older adults: a systematic review. J Neuroeng Rehabil 11(1):156. https://doi.org/10.1186/1743-0003-11-156
Fischetti F, Pepe I, Greco G et al (2024) Ten-minute physical activity breaks improve attention and executive functions in healthcare workers. J Funct Morphol Kinesiol 9(2):102. https://doi.org/10.3390/jfmk9020102
Anderson-Hanley C, Arciero PJ, Brickman AM et al (2012) Exergaming and older adult cognition. Am J Prev Med 42(2):109–119. https://doi.org/10.1016/j.amepre.2011.10.016
Nicholson VP, McKean M, Lowe J, Fawcett C, Burkett B (2015) Six weeks of unsupervised Nintendo Wii fit gaming is effective at improving balance in independent older adults. J Aging Phys Act 23(1):153–158. https://doi.org/10.1123/JAPA.2013-0148
Liao YY, Yang YR, Wu YR, Wang RY (2015) Virtual Reality-based wii fit training in improving muscle strength, sensory integration ability, and walking abilities in patients with parkinson’s disease: a randomized control trial. Int J Gerontol 9(4):190–195. https://doi.org/10.1016/j.ijge.2014.06.007
Funding
Open access funding provided by Università degli Studi di Bari Aldo Moro within the CRUI-CARE Agreement. This research received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, G.G., L.P. and F.F.; methodology, G.G., L.P and F.F.; software, L.P.; validation, G.G. and M.G.; formal analysis, M.G. and F.J.A.; investigation, L.P. and M.G.; resources, M.G. and F.J.A.; data curation, G.G. and L.P.; writing—original draft preparation, G.G., L.P. and M.G.; writing—review and editing, G.G., F.F., A.P. and S.C.; visualization, L.P. and M.G.; supervision, G.G., F.F., A.P., and S.C. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Bari University (protocol code 0015637|16/02/23).
Informed consent
Informed consent was obtained from all study participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Greco, G., Poli, L., Gabriele, M. et al. Effectiveness of a 5-week virtual reality versus traditional training on balance and flexibility in healthy adult females. Sport Sci Health (2024). https://doi.org/10.1007/s11332-024-01259-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11332-024-01259-9