
Abstract
Background
The SARS-CoV virus is a precursor to the SARS-CoV-2 virus (COVID-19) and has caused millions of deaths worldwide. Although exercise can be a non-pharmacological means for the prevention and treatment of various diseases, the effects on COVID-19 patients are not yet completely clear.
Aims
The aim of this study was to investigate the relationship between physical exercise and symptoms caused by COVID-19.
Methods
The present systematic review was sent for evaluation and received the PROSPERO registration protocol-CRD42021257475. The search for studies related to health and physical exercise was carried out in the following databases; the “National Library in Medicine MEDLINE–Ovid”, “Embase”, “Web of Science”, “SportDiscus-Ebsco”, and “Scopus”.
Results
Ten articles were included in the systematic review and the findings demonstrated the protective effects of physical exercise in patients with COVID-19. These effects were observed both in symptoms and in the period of hospitalization. In addition, the results show that the benefits of physical exercise seem to collaborate both in an individual manner and as an alternative to drug therapy. Finally, it was possible to verify the effect of physical exercise on variables, such as quality of life, cardiorespiratory capacity, and immunological biomarkers, and on the symptoms of the new Coronavirus.
Conclusions
It is possible to conclude that physical exercise can be a component for the treatment of COVID-19. In addition, it could help to reduce the symptoms and severity of COVID-19, and may be considered as an adjunct to drug therapy in patients contaminated with SARS-CoV-2.
Similar content being viewed by others


Introduction
The SARS-CoV virus is responsible for cases of severe acute respiratory syndrome (SARS) [1]. Until 2002, this virus posed a relatively low risk of contamination and death [2]. However, some variations in the SARS-CoV virus, which cause Severe Acute Respiratory Syndrome (SARS) have been observed in the last decade, resulting in concern from health institutions and government agencies [1, 2]. Among these variations are MERS-CoV, SARS-CoV, and SARS-CoV-2. The latter, which presents distinct characteristics from the SARS-CoV virus, is the cause of COVID-19, also known as the “new coronavirus”, and arose in 2019 [1].
SARS-CoV-2 affects the airways and compromises the lungs [1, 3]. Inflammation of the bronchi causes the individual to lose the ability to absorb oxygen, leading to shortness of breath and compromised airways [4], which can be determinant for the drop in performance in the sports environment. Although it presents symptoms mainly in the lungs, SARS-CoV-2 can cause several clinical manifestations and affect other organs of the human body [1]. Thus, by mitigating the development of disease and contributing to strengthening of the immune system, it is expected that physical exercise can alleviate the symptoms caused by COVID-19.
As it is a relatively new disease, COVID-19 has challenged researchers and health professionals with regard to prevention and treatment [5]. Although there are no pharmacological treatments that demonstrate proven efficiency against the disease, the use of Antipyretics, Analgesics, and Antibiotics represents some of the treatments used to reduce symptoms [6]. In addition, it is speculated that non-pharmacological measures, such as physical exercise, may help to in the treatment against the disease, such as in the reduction in symptoms and reversal of sequelae caused by COVID-19 [2, 7].
Exercise is used as a non-pharmacological means for the prevention and treatment of various diseases [8]. Among the most common are non-communicable or chronic degenerative diseases, such as obesity, systemic arterial hypertension, type II diabetes mellitus, osteoporosis, and certain types of cancer [9,10,11,12,13].
Some studies have confirmed cardiorespiratory adaptations caused by physical exercise [14, 15]. These adaptations range from increased oxygen uptake by the pulmonary alveoli to improved transport by hemoglobin and utilization in mitochondria [16]. In addition, some findings describe improvement in the immune system after performing exercise protocols [17,18,19].
However, despite some findings regarding the improvement in physical and respiratory capacities caused by physical exercise, there is a lack of clarity about the effects in individuals infected with SARS-CoV-2. Thus, the aim of this study was to investigate the relationship between physical exercise and cases of COVID-19.
Method
Registration protocol
Before the start of activities, this systematic review was sent for evaluation and registration at the International Prospective Registry of Systematic Reviews–PROSPERO (https://www.crd.york.ac.uk/prospero/) and received registration protocol CRD42021257475 on 15/09/2021.
Databases
To carry out this systematic review, databases that include studies related to health and physical exercise were searched, as follows: “the National Library of Medicine MEDLINE–Ovid”, “Embase”, “Web of Science”, “SportDiscus-Ebsco”, and “Scopus”.
The search was performed using terms related to health and physical exercise in the English language “MeSH Terms” (Appendix I), without restrictions regarding the period of publication of the articles. The period for carrying out the searches was determined between the months of February and March 2022.
PICOS
With the intention of answering the question “Can physical exercise be an efficient way to reduce the symptoms of COVID-19?”, the acronym “PICOS” was used based on the Population, Intervention, Comparator, Outcomes, and Studies criteria (Fig. 1).

Determination of the criteria established in the study–PICOS
Secondary outcomes: Secondary outcomes were determined to aid interpretation of the main outcomes. Alterations were observed in Cardiorespiratory Capacity; VO2MAX; Lung Capacity; Inflammatory Biomarkers; and Quality of Life of individuals infected with COVID-19 who performed a physical exercise protocol.
Descriptors
To identify the published articles, the following descriptors were used together with their respective search terms (Table 1):
COVID-19 (SARS-CoV-2); 2—aerobic exercise or resistance exercise; 3—physical exercise; 4—physical activity; 5—randomized Clinical Trial (Table 1). These descriptors were applied in the different databases described above.
Eligibility criteria
Eligibility criteria were established from studies that sought to investigate the effects of physical exercise in patients infected with COVID-19, according to the inclusion and exclusion criteria shown below.
Inclusion criteria
-
1.
Adult or older patients diagnosed with COVID-19;
-
2.
Studies that used physical exercise as a complementary form of treatment;
-
3.
Studies that observed physically active individuals contaminated with COVID-19;
-
4.
Adult or older individuals;
Criteria for non-inclusion
-
1.
Studies that did not perform physical exercise as an adjunct to treatment;
-
2.
Studies that did not evaluate patients with COVID-19.
-
3.
Studies that included children as the sample.
Extracted data
Eligibility was assessed by at least two researchers independently and with previous experience in review studies. In cases where there was no common agreement on the inclusion or exclusion of a particular work, a third researcher was consulted.
In this case, the main interest was the search for articles that investigated the effects of the performance of physical exercises on the symptoms of COVID-19.
Variables of interest
The variables of interest were determined by the variation in disease symptoms, length of hospital stay, effects on physical abilities, and alterations in the immune system or quality of life.
Risk of bias
To reduce the risk of bias, interactions that could influence the results obtained were studied. In this sense, the following factors were considered:
-
1.
Drug treatment (use of drugs)
-
2.
Variation in the way of performing physical exercises: Aerobic, Resistance, Continuous, Interval, Exercises in Telerehabilitation Programs (TERECO), Yoga, Qigong exercise, and Ayurveda.
-
3.
Reported Physical Activity Level: Questionnaires, Former Athletes, or Amateur Athletes.
-
4.
Patients with comorbidities contaminated by COVID-19.
Form of presentation of results
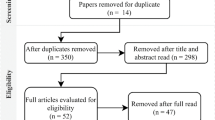
After the inclusion of scientific articles, we evaluated the possibility of carrying out the meta-analysis based on the results found in the studies. However, the included studies had different outcomes, in addition to which, only three articles were conducted from randomized clinical trials, while the others were prepared from epidemiological studies, cross-sectional studies, a cohort study, and a case study. Therefore, it was decided to carry out the systematic review without meta-analysis (Fig. 2).

Flowchart showing the selection and inclusion/exclusion of the articles
Results
Articles found
In total, 205 articles were found in the different databases. Four articles were duplicates from other databases, 150 articles were excluded after reading the title, and 38 after reading the abstract. Thus, following the selection process, 13 studies were identified that met the previously established criteria. Of these, 03 articles were review articles and were later excluded, leaving 10 articles for the systematic review.
Classification of the works
Considering the included works, only three (03) articles were prepared from randomized clinical trials, two (02) from cross-sectional studies, four (04) were characterized as Cohort articles, and one (01) as a case study.
Physical exercise and effects on cardiorespiratory capacity of patients with COVID-19
It was observed that physical exercise improved lung function (blood oxygen saturation), as well as the occurrence of dyspnea (modified Borg dyspnea scale) and cough (days of occurrence), in patients with severe cases, after performing a qigong exercise and acupressure rehabilitation program [20]. In addition, exercise protocols carried out using a telerehabilitation program (TERECO) led to an increase in cardiorespiratory capacity in the 6-min walking test (6MWT) and an improvement in the quality of life of the evaluated patients assessed by the Short Form Health Survey-12 (SF-12) [21].
Physical activity and COVID: protection factor?
It was found that physical exercise did not increase the risk of contamination in street runners, or show an association with symptoms caused by COVID-19 [22]. In addition, a 2-week exercise protocol, at moderate intensity, led to an improvement in the immune response (leukocytes, lymphocytes, and immunoglobulin A) [23] in 30 patients from 24 to 45 years old (15 males and 15 females), in addition to decreased progression of the disease, from the score obtained by the Wisconsin upper respiratory symptom survey. Finally, the findings showed that physical exercise was negatively associated with cases of death caused by COVID-19, in addition to a lower risk of contamination by the disease (Table 2).
Discussion
Main findings
The aim of the present study was to observe the possible relation of physical exercise in individuals infected with COVID-19. It was observed that physical exercise could be a protection factor against the disease in the majority of studies. This protective factor was related to cases of death, improved lung function, and reduced symptoms of the disease. In addition, the practice of street running does not seem to demonstrate a risk for the development of symptoms.
The findings of the present study corroborate the pre-established idea in the literature of the potential protective effects of physical exercise in patients with COVID-19 [23, 30]. Previous studies have suggested the idea of potential beneficial effects of physical exercise on the immune system and on the reduction in symptoms caused by SARS-CoV-2 [23, 31].
Physical exercise and cases of death due to COVID-19
The study of Wang et al. [24] observed an association between cases of deaths due to COVID-19 and lack of physical activity. The authors investigated individuals aged over 65 years, living in 186 countries and reported that lifestyle, as well as sedentary habits, are related to the increase in cases of death from SARS-CoV-2.
Life habits seem to be related to the reduction in symptoms caused by the new coronavirus. The study of Christensen et al. [27] investigated 2690 adults aged between 40 and 69 years and found that patients with high values of cardiorespiratory capacity had a lower risk of death from COVID-19.
In this case, patients classified as having low aerobic capacity (< 20th percentile) were twice as likely to die from COVID-19, when compared with patients classified as having moderate (20th to < 80th percentile) and high cardiorespiratory capacity (> 80th percentile) [27]. This is one of the factors responsible for the increase in oxygen transport and gas exchange, a mechanism that in most cases is affected by the development of the disease.
Physical exercise and effects on cardiorespiratory capacity of patients with COVID-19
This finding corroborates previously published studies. A study carried out in patients with severe symptoms of COVID-19 found that participants presented lower cardiorespiratory capacity, and a higher body mass index (BMI) and associated comorbidities, in addition to daily smoking habits [32]. The study by Brawner et al. [33] found that cardiorespiratory capacity improved the risk profile of patients infected with COVID-19.
In this case, it appears that physically active individuals are, apparently, less susceptible to the risk of death. This fact is especially relevant in the older population who, during the Pandemic caused by the new Coronavirus, showed a greater propensity to develop the disease, due to the aging process and associated comorbidities [29].
Physical activity and COVID: protection factor?
A study of older people living in 3,142 counties in the United States found a negative association between COVID-19 and physical activity [25]. In this case, it was found that the lower the practice of physical activity outside the work environment, the stronger the relationship with cases of death.
In a study carried out with 500,000 participants, aged between 40 and 69 years, it was found that physically active people were less likely to be diagnosed with COVID-19 [26]. The authors verified that participants who self-reported the practice of moderate and vigorous physical activities demonstrated an odds ratio of 0.80 (CI 95%) as a protective factor in cases of death.
According to the authors, physical activity may benefit respiratory viral infections by increasing the resistance of respiratory muscles or by improving the immune response to respiratory viral antigens [26]. These findings reinforce the idea of a protective factor caused by physical exercise.
In the study of Malisoux et al. [28], the effect of possible protection from the previous practice of physical activity was verified in patients contaminated with COVID-19. It was observed that patients who practiced physical activities recreationally or as a means of transportation (walking, cycling, home, and sports activities) before the occurrence of the disease demonstrated a reduction in disease severity, especially in moderate cases.
In addition, there was a reduction in symptoms, such as a feeling of fatigue, dry cough, and chest pain [28]. In this way, the regular practice of physical exercises seems to be an effective way to prevent serious cases of COVID-19 according to the Symptom severity classification scheme of the Luxembourg National Institute of Health.
COVID-19 cases and outdoor exercise
It was also verified that the practice of physical exercise outdoors was not associated with cases of COVID-19. The study by Cloosterman et al. [22] found that although 10 of the 2586 participants tested positive for the new Coronavirus, there was no association between symptoms of the disease and the habit of practicing physical activity in street runners.
Studies show that there is a greater risk of contamination with COVID-19 in closed environments, with a higher concentration of people and little air circulation [34,35,36]. This fact may have contributed to the lower occurrence of the new Coronavirus in runners. Added to this, aerobic exercise seems to reduce the symptoms caused by SARS-CoV-2 [23, 27].
Physical exercise and COVID in randomized clinical trials
A randomized controlled trial sought to investigate the possible effects of a telerehabilitation program (TERECO) on the physical capacity of patients infected with COVID-19. In total, 120 patients were investigated, COVID-19 survivors with a dyspnea complaint, 18–75 years old, of both sexes, who had been discharged from hospital after being contaminated, and who participated in an exercise program at home for a period of 6 weeks. It was found that after the TERECO, there was an increase in cardiorespiratory capacity (6-min walking distance—Control: 499.98 ± 93.41, Intervention: 514.52 ± 82.87), as well as an improvement in the quality of life of the study participants (SF-12 Questionnaire, Control: 3.84 ± 7.60, Intervention: 7.81 ± 7.02) [21].
The literature demonstrates that physical exercise is able to attenuate the emergence and development of several diseases, especially chronic degenerative diseases [37,38,39]. In addition, it is observed that physically active individuals may present better levels of quality of life [30], as well as increased physical capabilities [11, 40,41,42].
Another randomized controlled study investigated the effect of a protocol of moderate intensity physical exercises, performed three times a week, for a period of 2 weeks. A reduction in the symptoms of COVID-19 was found, as well as an increase in the number of immunological markers, such as leukocytes and lymphocytes.
In this case, an increase from 5.44 ± 1.32 to 7.34 ± 1.40 in leukocytes (leucocytes, × 109/L) and from 0.98 ± 0.19 to 2.09 ± 0.18 in lymphocytes was observed (lymphocytes, × 109/L) in the intervention group, after 2 weeks [23]. Furthermore, there was an improvement in the quality of life and a decrease in the severity of the disease [23].
Leukocytes and lymphocytes are found in human blood and play an important role in the defense system against invading elements, such as several types of viruses [23]. These elements are fundamental in protecting against infections caused by diseases and, in certain cases, also by reinfections. This applies to cases of COVID-19, as it is possible to observe recurrent cases of infections by the disease.
According to Mohamed and Alawna [23], patients with COVID-19 present a severe reduction in serum T cells, CD4þ, CD8þ T cells, and B cells, particularly those who need an intensive-care unit. In this case, physical exercise, especially aerobic, seems to be a modality with the potential to increase the immune system and thus collaborate to increase the defense cells of the human body [43].
A third randomized controlled trial aimed to investigate the effects on the respiratory system of a Qigong exercise program (breathing exercise program), combined with drug therapy, in 120 participants, aged between 20 and 80 years, diagnosed with COVID-19. At the end of the study, the participants showed improvement in lung function and a significant increase in vital signs [20].
A case study of physical exercise and COVID
Finally, a case study, carried out with a 55-year-old man, infected with COVID-19, demonstrated that a protocol of Yoga and Ayurveda exercises, combined with drug therapy, was able to attenuate the symptoms in a period of 2–5 days, and provoke complete improvement in the clinical framework in 9 to 12 days [29].
This research demonstrates the idea that physical exercise can prevent or alleviate the symptoms caused by COVID-19. Therefore, the present study collaborates with the literature by identifying possible benefits of physical exercise to patients and symptoms caused by the new Coronavirus.
However, some limitations should be highlighted, such as the lack of randomized controlled trials that sought to investigate similar outcomes. In addition, it was observed that the studies presented different characteristics, such as case studies, observational studies, and cross-sectional studies. In this way, future studies using meta-analysis are needed to collaborate the results presented in the current study.
Conclusion
It is possible to conclude that physical exercise can collaborate with the reduction in the symptoms and severity of COVID-19. In addition, the findings suggest that exercise can be used in conjunction with drug therapies in the treatment of patients contaminated with SARS-CoV-2.
Data availability
The data obtained in the present study were acquired in the databases “The National Library of Medicine MEDLINE–Ovid”, “Embase”, “Web of Science”, “SportDiscus-Ebsco”, and “Scopus”.
References
Chowdhury MA, Hossain N, Kashem MA et al (2020) Immune response in COVID-19: a review. J Infect Public Health 13:1619–1629. https://doi.org/10.1016/j.jiph.2020.07.001
Yeo TJ (2020) Sport and exercise during and beyond the COVID-19 pandemic. Eur J Prev Cardiol 27:1239–1241. https://doi.org/10.1177/2047487320933260
Gao Z, Xu Y, Sun C et al (2021) A systematic review of asymptomatic infections with COVID-19. J Microbiol Immunol Infect 54:12–16. https://doi.org/10.1016/j.jmii.2020.05.001
Rossato L, Negrão FJ, Simionatto S (2020) Could the COVID-19 pandemic aggravate antimicrobial resistance? Am J Infect Control 48:1129–1130. https://doi.org/10.1016/j.ajic.2020.06.192
Pereira LJ, Pereira CV, Murata RM et al (2020) Biological and social aspects of coronavirus disease 2019 (COVID-19) related to oral health. Braz Oral Res 34:1–11. https://doi.org/10.1590/1807-3107bor-2020.vol34.0041
Stasi C, Fallani S, Voller F, Silvestri C (2020) Treatment for COVID-19: an overview. Eur J Pharmacol 889:173644
Leandro CG, Ferreira S, Lima-Silva AE (2020) Covid-19 and exercise-induced immunomodulation. NeuroImmunoModulation 27:75–78. https://doi.org/10.1159/000508951
de Val FF, Okubo R, Falcai MJ et al (2013) Effects of high-impact exercise training on bone mechanical proprieties-An experimental study in female wistar rats. Rev Bras Med do Esporte 19:252–255. https://doi.org/10.1590/S1517-86922013000400005
Dos Santos ACA, Papoti M, De Barros M-G et al (2015) The effects induced by swimming training on rats submitted to normal and hypercaloric diets. Motricidade. https://doi.org/10.6063/motricidade.3069
Leme JACA, Silveira RF, Gomes RJ et al (2009) Long-term physical training increases liver IGF-I in diabetic rats. Growth Horm IGF Res 19:262–266. https://doi.org/10.1016/j.ghir.2008.12.004
Castoldi RC, Aleixo PH, Pereira ACJ et al (2017) Effects of concurrent training on muscle fibers of wistar rats submitted to standard and hypercaloric diets. Int J Morphol. https://doi.org/10.4067/S0717-95022017000200041
Nieman DC (2020) Coronavirus disease-2019: a tocsin to our aging, unfit, corpulent, and immunodeficient society. J Sport Heal Sci 9:293–301
Azizi GG, Orsini M, Dortas Júnior SD et al (2020) COVID-19 and physical activity: What is the relation between exercise immunology and the current pandemic situation? Rev Bras Fisiol Exerc 19:20. https://doi.org/10.33233/rbfe.v19i2.4115
Brown MB, Neves E, Long G et al (2017) High-intensity interval training, but not continuous training, reverses right ventricular hypertrophy and dysfunction in a rat model of pulmonary hypertension. Am J Physiol Integr Comp Physiol 312:R197–R210. https://doi.org/10.1152/ajpregu.00358.2016
Carbone S, Del Buono MG, Ozemek C, Lavie CJ (2019) Obesity, risk of diabetes and role of physical activity, exercise training and cardiorespiratory fitness. Prog Cardiovasc Dis 62:327–333. https://doi.org/10.1016/j.pcad.2019.08.004
Stuart CA, Howell MEA, Baker JD et al (2011) Cycle training increased GLUT4 and activation of mTOR in fast Twitch muscle fibers. Kinesiology 42:423–439. https://doi.org/10.1249/MSS.0b013e3181ad7f36.Cycle
Fallon K (2020) Exercise in the time of COVID-19. Aust J Gen Pract. https://doi.org/10.31128/AJGP-COVID-13
Filgueira TO, Castoldi A, Santos LER et al (2021) The relevance of a physical active lifestyle and physical fitness on immune defense: mitigating disease burden, with focus on covid-19 consequences. Front Immunol 12:1–23. https://doi.org/10.3389/fimmu.2021.587146
Wang J, Liu S, Li G, Xiao J (2020) Exercise regulates the immune system. Adv Exp Med Biol 1228:395–408. https://doi.org/10.1007/978-981-15-1792-1_27
Liu S, Zhan C, Ma Y et al (2021) Effect of qigong exercise and acupressure rehabilitation program on pulmonary function and respiratory symptoms in patients hospitalized with severe COVID-19: a randomized controlled trial. Integr Med Res 10:100796. https://doi.org/10.1016/j.imr.2021.100796
Li J, Xia W, Zhan C et al (2021) A telerehabilitation programme in post-discharge COVID-19 patients (TERECO): a randomised controlled trial. Thorax. https://doi.org/10.1136/thoraxjnl-2021-217382
Cloosterman KLA, Middelkoop M Van, Krastman P (2020) Since January 2020 Elsevier has created a COVID-19 resource centre with free information in English and Mandarin on the novel coronavirus COVID- 19 . The COVID-19 resource centre is hosted on Elsevier Connect , the company ’ s public news and information. https://doi.org/10.1016/j.jsams.2020.10.009
Mohamed AA, Alawna M (2021) The effect of aerobic exercise on immune biomarkers and symptoms severity and progression in patients with COVID-19: a randomized control trial. J Bodyw Mov Ther 28:425–432. https://doi.org/10.1016/j.jbmt.2021.07.012
Wang J, Sato T, Sakuraba A (2021) Worldwide association of lifestyle-related factors and COVID-19 mortality. Ann Med 53:1531–1536. https://doi.org/10.1080/07853890.2021.1968029
Cunningham GB (2021) Physical activity and its relationship with COVID-19 cases and deaths: Analysis of US counties. J Sport Heal Sci 10:570–576. https://doi.org/10.1016/j.jshs.2021.03.008
Zhang X, Li X, Sun Z et al (2020) Physical activity and COVID-19: an observational and Mendelian randomisation study. J Glob Health. https://doi.org/10.7189/jogh.10.020514
Christensen RA, Arneja J, Cyr St K et al (2021) The association of estimated cardiorespiratory fitness with COVID-19 incidence and mortality: a cohort study. PLoS ONE 16:e0250508. https://doi.org/10.1371/journal.pone.0250508
Malisoux L, Backes A, Fischer A et al (2022) Associations between physical activity prior to infection and COVID-19 disease severity and symptoms: results from the prospective Predi-COVID cohort study. BMJ Open 12:e057863. https://doi.org/10.1136/bmjopen-2021-057863
Mishra A, Bentur SA, Thakral S et al (2021) The use of integrative therapy based on Yoga and Ayurveda in the treatment of a high-risk case of COVID-19/SARS-CoV-2 with multiple comorbidities: a case report. J Med Case Rep 15:95. https://doi.org/10.1186/s13256-020-02624-1
Gentil P, de Lira CAB, Coswig V et al (2021) Practical recommendations relevant to the use of resistance training for covid-19 survivors. Front Physiol 12:1–11. https://doi.org/10.3389/fphys.2021.637590
Chastin SFM, Abaraogu U, Bourgois JG et al (2021) Effects of regular physical activity on the immune system, vaccination and risk of community-acquired infectious disease in the general population: systematic review and meta-analysis. Sport Med 51:1673–1686. https://doi.org/10.1007/s40279-021-01466-1
Ekblom-Bak E, Väisänen D, Ekblom B et al (2021) Cardiorespiratory fitness and lifestyle on severe COVID-19 risk in 279,455 adults: a case control study. Int J Behav Nutr Phys Act 18:135. https://doi.org/10.1186/s12966-021-01198-5
Brawner CA, Ehrman JK, Bole S et al (2021) Inverse relationship of maximal exercise capacity to hospitalization secondary to coronavirus disease 2019. Mayo Clin Proc 96:32–39. https://doi.org/10.1016/j.mayocp.2020.10.003
Cross TJ, Isautier JMJ, Morris SJ et al (2021) The influence of social distancing behaviors and psychosocial factors on physical activity during the COVID-19 pandemic: cross-sectional survey study. JMIR Public Heal Surveill 7:e31278. https://doi.org/10.2196/31278
Helsingen LM, Løberg M, Refsum E et al (2021) Covid-19 transmission in fitness centers in Norway-a randomized trial. BMC Public Health 21:2103. https://doi.org/10.1186/s12889-021-12073-0
Yoshihara A, Dierickx EE, Brewer GJ et al (2021) Effects of face mask use on objective and subjective measures of thermoregulation during exercise in the heat. Sport Heal 13:463–470. https://doi.org/10.1177/19417381211028212
Hong AR, Kim SW (2018) Effects of resistance exercise on bone health. Endocrinol Metab 33:435. https://doi.org/10.3803/EnM.2018.33.4.435
Marinho R, Moura LP, ereir. de, Rodrigues B de A, et al (2014) Effects of different intensities of physical exercise on insulin sensitivity and protein kinase B/Akt activity in skeletal muscle of obese mice. Einstein (Sao Paulo) 12:82–89. https://doi.org/10.1590/S1679-45082014AO2881
Ghiasi R, Mohammadi M, Ashrafi Helan J et al (2015) Influence of two various durations of resistance exercise on oxidative stress in the male rat’s hearts. J Cardiovasc Thorac Res 7:149–153. https://doi.org/10.15171/jcvtr.2015.32
Rogerio MM, Santos LS, Garcia TA et al (2019) Effects of concurrent training associated with N-acetylcysteine on bone density of spontaneously hypertensive rats. Motriz Rev Educ Fis. https://doi.org/10.1590/s1980-6574201900010020
Koike TE, Watanabe AY, Kodama FY et al (2018) Physical exercise after immobilization of skeletal muscle of adult and aged rats. Rev Bras Med do Esporte. https://doi.org/10.1590/1517-869220182401172423
Castoldi RC, Camargo RCT, Magalhães AJB et al (2013) Concurrent training effect on muscle fibers in Wistar rats. Mot Rev Educ Física 19:717–723. https://doi.org/10.1590/S1980-65742013000400008
Mohamed AA, Alawna M (2020) Role of increasing the aerobic capacity on improving the function of immune and respiratory systems in patients with coronavirus (COVID-19): a review. Diabetes Metab Syndr Clin Res Rev 14:489–496. https://doi.org/10.1016/j.dsx.2020.04.038
Author information
Authors and Affiliations
Contributions
RCC, JCÂ, TTP, FJN: project development. RCC, FJN: manuscript writing. JCÂ, TTP: search in databases JCÂ, RMD: preparation of results. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval and Informed consent
This is a review study and not need ethical approval. But this systematic review was sent for evaluation and registration at the International Prospective Registry of Systematic Reviews–PROSPERO and received registration protocol CRD42021257475 on 15/09/2021.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix
Appendix I: Example of a Database Search and “MeSH Terms”
Medline—Ovid
1. COVID-19/ |
2. SARS-CoV-2/ |
3. Coronavirus/ |
4. 1 or 2 or 3 |
5. randomized controlled trial.pt |
6. controlled clinical trial.pt |
7. placebo.ab |
8. drug therapy.fs |
9. random*.ab,ti |
10. trial.ab |
11. groups.ab |
12. 5 or 6 or 7 or 8 or 9 or 10 or 11 |
13. animals/ |
14. humans/ and animals/ |
15. 13 not 14 |
16. 12 not 15 |
17. physical activity*.ab,ti,kw |
18. physical exercise*.ab,ti,kw |
19. (exercise* or cycling* or treadmill* or walking* or ergometer* or "postexercise" or "sports" or "interval training" or "sports practice" or "yoga" or "fitness" or "resistance exercise" or "tennis" or "horse riding" or "gymnastics" or "weight lifting" or "weight training" or "strength training" or "endurance training" or "speed training" or "circuit training" or "training frequency" or "training intensity" or "anaerobic training" or "aerobic training" or "HIIT" or "combination training" or "combined training" or "concurrent training" or "training duration" or "swimming" or "survey and questionnaire" or "supervised exercise" or "Military Personnel" or "cross-training" or "Exercise Therapy" or "Muscle Strength" or "Pilates" or "Dance").ab,ti,kw |
20. 17 or 18 or 19 |
Embase
('coronavirus disease 2019'/exp OR 'coronavirus disease 2019' OR 'severe acute respiratory syndrome coronavirus 2'/exp OR 'severe acute respiratory syndrome coronavirus 2' OR 'coronavirus infection'/exp OR 'coronavirus infection') AND ('randomized controlled trial' OR 'controlled clinical trial') AND ('exercise' OR 'cycling' OR 'physical activity' OR 'walking' OR 'treadmill' OR 'ergometer' OR 'interval training' OR 'sport' OR 'yoga' OR 'fitness' OR 'resistance training' OR 'tennis' OR 'horseback riding' OR 'gymnastics' OR 'weight lifting' OR 'weight training' OR 'endurance training' OR 'circuit training' OR 'aerobic training' OR 'high intensity interval training' OR 'concurrent training' OR 'swimming' OR 'questionnaire' OR 'supervised exercise' OR 'military personnel' OR 'cross training (sport)' OR 'muscle strength' OR 'pilates' OR 'dancing').
Web of Science
((ALL = (COVID-19)) OR (ALL = (Coronavirus)) OR (ALL = (SARS-CoV-2))) AND ((ALL = (randomized controlled trial)) OR (ALL = (controlled clinical trial)) OR (ALL = (random))) AND ((ALL = (physical activity)) OR (ALL = (physical exercise)) OR (ALL = (walking)) OR (ALL = (treadmill)) OR (ALL = (ergometer)) OR (ALL = (interval training)) OR (ALL = (sport)) OR (ALL = (yoga)) OR (ALL = (fitness)) OR (ALL = (resistance training)) OR (ALL = (tennis)) OR (ALL = (horseback riding)) OR (ALL = (gymnastics)) OR (ALL = (weight lifting)) OR (ALL = (weight training)) OR (ALL = (endurance training)) OR (ALL = (circuit training)) OR (ALL = (aerobic training)) OR (ALL = (high intensity interval training)) OR (ALL = (concurrent training)) OR (ALL = (swimming)) OR (ALL = (questionnaire)) OR (ALL = (supervised exercise)) OR (ALL = (military personnel)) OR (ALL = (cross training)) OR (ALL = (muscle strength)) OR (ALL = (pilates)) OR (ALL = (dancing))).
Scopus–Elsevier
COVID-19 OR Coronavirus OR SARS-CoV-2 AND randomized controlled trial OR controlled clinical trial OR random AND physical activity OR physical exercise OR walking OR treadmill OR ergometer OR interval training OR sport OR yoga OR fitness OR resistance training OR tennis OR horseback riding OR gymnastics OR weight lifting OR weight training OR endurance training OR circuit training OR aerobic training OR high intensity interval training OR concurrent training OR swimming OR questionnaire OR supervised exercise OR military personnel OR cross training OR muscle strength OR pilates OR dancing.
EBSCO–SPORTDiscus
(TX covid-19 OR TX coronavirus OR TX sars-cov-2).
AND
(TX randomized controlled trials OR TX controlled clinical trial OR TX random).
AND
(TX physical activity OR TX physical exercise OR TX physical training OR TX walking OR TX treadmill OR TX ergometer OR TX interval training OR TX sport OR TX yoga OR TX fitness OR TX resistance training OR TX tennis OR TX horseback riding OR TX gymnastics OR TX weight lifting OR TX weight training OR TX endurance training OR TX circuit training OR TX aerobic training OR TX high intensity interval training OR TX concurrent training OR TX swimming OR TX questionnaire OR TX supervised exercise OR TX military personnel OR TX cross training OR TX muscle strength OR TX pilates OR TX dancing).
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Castoldi, R.C., de Ângelo, J.C., Pereira, T.T. et al. Relationship between physical exercise and COVID-19 (SARS-CoV-2): systematic review. Sport Sci Health 19, 55–67 (2023). https://doi.org/10.1007/s11332-022-01028-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-022-01028-6