
Abstract
Purpose
Energy availability (EA) is considered an important measure for athletes, particularly due to the possible health and performance outcomes defined under the RED-S. Low EA is reported to have far-reaching health consequences among female athletes, especially in weight-sensitive sport. However, it is less explored among male athletes, particularly in the traditional Indian tag sport called Kho-Kho. This cross-sectional observational study aimed to determine the prevalence of LEA and associated RED-S health and performance outcomes among Kho-Kho players.
Methods
Fifty-two male national-level Kho-Kho players aged 16–31 years were assessed for energy availability, bone mineral density (BMD), sleep quality, disordered eating, selected metabolic (hemoglobin, blood glucose, etc.) and performance outcomes (agility, speed, and power) as per RED-S risk assessment tool. Differences across the low EA (≤ 25 kcal/ kg fat-free mass) and Optimal EA (> 25 kcal/ kg fat-free mass) groups were evaluated using the Independent Samples t test and the chi-square test.
Results
Low EA among athletes was associated with lower z-scores for BMD, sleep quality and agility, compared to athletes with optimal EA. At least one moderate-to-high RED-S risk outcome was prevalent among 98% of the Kho-Kho players, irrespective of EA. Most athletes exhibited a lower EAT score and disordered eating outcomes, with no significant differences across groups.
Conclusion
The male Kho-Kho players showed a prevalence of low EA that can be due to higher training loads and unintentional under-eating, not related to an eating disorder. The players also exhibited higher RED-S risk outcomes; however, it was irrespective of low EA.
Similar content being viewed by others


Introduction
Energy intake required for maintaining life processes once exercise energy expenditure is subtracted, expressed as energy availability, has gained significance for its role in maintaining athlete health [1]. Low energy availability (LEA) may lead to a myriad of health and performance outcomes known as Relative Energy Deficiency in Sport (RED-S). The predominantly reported RED-S outcomes are related to disruption of the hypothalamic–pituitary–gonadal axis, and which is independent of the influence of training on the axis [2]. Apart from this, eating disorders, bone stress injuries, and other hormonal disruptions were also related to LEA [2]. A higher prevalence of LEA is reported among female athletes, participating in weight-sensitive sports, which includes esthetic, endurance, or contact sports [2, 3]. However, recent studies have identified certain RED-S risks, including lower bone mineral density, and lower testosterone levels among male endurance athletes [4, 5]. Such exploration in traditional contact sports, particularly among the Asian non-white population has not been carried out.
Kho-Kho is a traditional tag sport of India, played with a chasing team trying to tag their opponents to score points. The sport is played on a rectangular field (30/26 m × 19/17 m) with two poles on either end. An inning includes chasing and defending in 9 min, with nine players on the field and 3 extras. The nine players of a chasing team will be seated on a straight line between poles, and at a time one of them will look to tag three raiders of the defending team. The word “Kho” is used as a signal to make a shift between different chasers. Thus, it is not merely a game of running, but it involves chasing movements, such as controlled sprinting, dodging, diving, taping, covering, and post-turning [6]. This requires higher explosive strength, with increased agility, stamina, and anaerobic power [7, 8].
Athletes in such sports undergo a myriad of changes in their activity pattern, from spontaneous high-intensity sprints to sudden rests within a match and across a playing season. This pattern of movement follows closely to other contact events like Kabbadi, Rugby, Gaelic football, and Australian rules football. They rely heavily on aerobic energy, as well as shorter bouts of anaerobic power, with Indian kabaddi players, a popular tag game in India recognized worldwide, reporting up to 43.5–70.5% of VO2max during a match [9]. The Kho-Kho players were reported to have higher ectomorphic components and muscle mass compared to age-matched controls [10]. They were also reported to have higher explosive strength and lower agility, compared to kabaddi players [8]. Kho-Kho gained popularity, after the Khelo India scheme included Kho-Kho in their competitions, to encourage this sport at the grass-root level. Considering the intensity of the game, there is the possibility of energy deficits and RED-S risk, which has not been explored so far. Therefore, the present study aimed to determine LEA among Indian national male Kho-Kho players, and its association with their health and performance related to RED-S.
Methods
Participant selection
This observational study included participants were male Kho-Kho players aged 16–31 years and were selected based on the criteria that athletes were training for over 2 years in the sport, and were apparently healthy, not suffering from any injury or deformity. The study was approved by institutional ethical committee and conducted according to the guidelines laid down in the declaration of Helsinki and STROBE. The athletes who met the criteria were briefed about the various tests, including the discomforts, and written consent was obtained. The recruited athletes were training within their bio-bubbles and were tested for COVID-19 before initiating data collection.
Energy availability
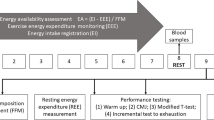
Energy availability (EA) was calculated by subtracting training energy expenditure from energy intake and expressed as kcal per kg fat-free mass (FFM). In general, energy availability less than 30 kcal per kg FFM is considered as low and greater than or equal to 30 kcal per kg FFM as optimal or adequate [11, 12], although these cut-offs were developed on female athletes, it is suggested to hold good for male athletes as well [5]. However, a recent study has reported that an EA threshold ranging from 9–25 kcal per kg FFM reduced explosive power and testosterone levels among male endurance athletes and hence for the present study on male Kho-Kho players a cut-off of less than or equal to 25 kcal per kg FFM was used [13]. The training energy expenditure was determined by a 1-day activity record of the athlete, and multiplying the time spent in activities with METs in the compendium of physical activity [14], corrected for basal metabolic rate (BMR). The BMR was predicted using the equation of Cunningham, which was found to be suitable in the Indian context [15] and among Indian athletes [16]. The energy intake was determined using a 1-day direct weighment plus recall method, [17] and the nutritive value was calculated using the Indian Food Data Tables (IFCT) [18].
Physical measurements
The basic measurement of height and weight was carried out using a standard protocol [19]. Height was recorded to the nearest 0.1 cm using a stadiometer with the athlete maintaining the Frankfurt plane. Body mass was recorded with minimal clothing, after voiding the bladder, to the nearest 0.1 kg using a digital weighment. Skinfold measurements (biceps, triceps, subscapular, and supra-iliac) on the right side of the body were taken using Holtain calipers (U.K) with 0.2 mm accuracy. Body density [20] and body-fat percent [21] were accordingly calculated. FFM was obtained by subtracting fat mass from body mass.
Health and performance risk outcomes related to RED-S
The health and performance outcomes were classified as “high” or “moderate” risk groups, based on the RED-S Cumulative Assessment Tool [1, 22] and overall prevalence included the presence of any one risk factor, irrespective of the group, based on IOC recommendations [23] Eating Disorder and extreme weight loss practices were assessed using self-reporting, while the EAT-26 questionnaire was employed to ascertain eating attitudes with a score above 20 considered as a risk for disordered eating [24]. The ECG was also determined as part of the study, and only the dichotomised data are used for the purpose of this study [25].
Bone mineral density
The lumbar spine (L1–L4) measurements were taken using the Hologic Discovery DXA fan-beam scanner (software V.12.1, fast-array mode). The scan was done using the auto low-density option, which uses algorithms to improve the accuracy of edge detection of the bones in individuals with low bone mineral density (BMD). BMD was calculated using the geometric assumptions made by Carter et al. [26].
Sleep quality
Sleep quality was assessed by the Pittsburgh Sleep Quality Index (PSQI) questionnaire [27], consisting of seven component scores related to subjective sleep quality, sleep onset latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of medication, and daytime dysfunction.
Biochemical estimation
A fasting blood sample (10 mL) was collected via vein puncture and was transferred from the syringe into plain bottles and centrifuged at 4000 rpm for 10 min to separate the serum. The serum samples were kept in the freezer (at 18 °C) till further analysis. The tests were performed within 72 h after obtaining the blood sample. Serum calcium, serum vitamin-D3, serum T3. hemoglobin, serum albumin, serum creatinine, SGOT, SGPT, were measured using an automatic clinical chemistry analyser, Erba (Lachema) XL200, Germany.
Performance outcomes
The maximum force generated by lower limb muscles was estimated using the vertical jump test [28]. Agility being one of the most important components of the game, was determined using the Illinois Agility Test [29]. The sprinting ability was assessed using the 30-m sprint test [30].
Statistical analysis
All analyses were carried out using IBM SPSS (Statistics for Macintosh, Version 27.0, Armonk, NY). Descriptive statistics were carried out and data were expressed as mean, SD, and range. The independent sample t test was employed to ascertain differences between low and optimal EA. The data related to energy availability, selected health and performance risk outcomes were dichotomised based on standard cut-offs (presented in Table 4). The chi-square test was employed to determine differences in RED-S risks outcomes across low and optimal EA groups. Significance was considered at a p-value < 0.05.
Results
Age was not significantly different across the low and optimal EA groups, however, body mass, including lean body mass, and height were significantly higher in the low EA group compared to the optimal EA group (presented in Table 1). The basal metabolic rate, total energy expenditure and activity energy expenditure were significantly higher among the LEA group compared to the optimal EA group (presented in Table 1). Physical Activity Level (DEE/BMR) was also higher in the LEA group, indicating a lower BMR in relation to the total energy expended in the LEA group. Thus, explaining lower energy being utilized for the basic life process. In addition, the corresponding energy intake was significantly lower in the LEA group, compared to the optimal EA group.
Among the health-related outcomes assessed (presented in Table 2), the BMD z-scores were significantly lower in the LEA group, compared to the optimal EA group. However, the serum levels of Vitamin D and calcium were not different. The hemoglobin levels were normal and were not significantly different across the groups, and this corroborated with a majority (85%) of the athletes consuming iron in line with the Indian recommendations. The liver function parameters, serum albumin, and creatine were within normal ranges and were not different (p > 0.05) across the groups. The LEA groups also exhibited lower overall sleep quality (low EA: 0.25 ± 0.84 versus Optimal EA:0.00, p < 0.01), compared to the optimal EA group. Among the performance-related outcomes, the LEA group exhibited significantly lower agility as compared to the AEA group, while speed and power outcomes did not differ significantly across groups.
Macronutrient consumption was lower in the LEA group, in both absolute terms and relative to their body mass. However, the percent contribution of macronutrients (Mean Carbohydrate:Protien:Fat was 58.62:15.50:29.83 in LEA versus 56.98:14.11:29.49 in optimal EA group; p > 0.05) towards the overall energy intake was not significantly different across the groups. Since, the overall energy intake was lower, the estimated metabolic water was lower in LEA group (LEA: 360.1 ± 84.20 versus Optimal EA:538.2 ± 89.03, p < 0.001), and this also resulted in lower total fluid intake (presented in Table 3). The LEA group consumed lower Vitamin-A, B-Vitamins, Iron and Zinc compared to the optimal EA group, while no significant differences were noted in intake of Vitamin-C, Calcium, and Carotenoids.
The RED-S risk assessment (depicted in Table 4) indicated an overall prevalence of 45% in any one of the high-risk health outcomes, with most of the athletes resorting to extreme dehydration techniques (34.5%) and showing ECG abnormalities (10.4%), with no significant differences across the LEA and AEA groups. Among moderate risk outcomes, the most prevalent were lower history of any form of injury, reduced Vitamin D levels, and lower BMD levels. The overall prevalence for any one of the moderate or high-risk outcomes was 98.1 percent, though there was no significant difference across the groups.
Discussion
Low energy availability has been attributed to causing many health and performance outcomes among athletes, and this study is unique as it explores the prevalence of low energy availability and associated RED-S risk outcomes among the Kho-Kho players, which is a traditional sport gaining popularity in recent times. The major finding of the study is that low energy availability was associated with lower bone mineral density, agility, and sleep quality, as compared to adequate energy levels. Another significant outcome was that majority of the athletes exhibited moderate-to-high risk for RED-S, albeit the prevalence of risk was not different across the low energy and optimal energy groups.
Energy deficits have been associated with compromised physiological functioning, with a four-day reduced LEA exhibiting reductions in reproductive hormones among female athletes [31]. Further, a 5-day LEA showing a reduction in blood glucose levels and suppression of other metabolic hormones like insulin and leptin, while, increasing the levels of cortisol [32]. Low energy availability was reported among 44% of the male Kho-Kho players in this study. The activity energy expenditure was higher in the low EA group compared to optimal EA group. This could be due to an inadvertent LEA, considering that the players were assessed for one-day while in a training camp, with higher exercise intensities and being away from their hometowns and natural food environment causing unintentional under-eating, irrespective of the group [33]. Nevertheless, the LEA group exhibited reduced bone mineral density z-scores compared to the optimal EA group (Refer Table 2). This was in line with the findings of reduced lumbar spine bone mineral density z-scores and osteopenia in association with LEA among male endurance athletes from the US and UK [34,35,36]. Within 5 days of LEA, Ihle and Loucks [37] reported an increased rate of bone resorption and decreased bone formation among women with studies also reporting increased risk for injuries, particularly, stress fractures and osteoporosis among female athletes [38, 39], however, similar outcomes of stress injury were scanty among male athletes. A higher training volume has also been associated with a reduced lumbar bone mineral density z-scores and LEA, [39] which could be one of the contributing factors for LEA among Kho-Kho players in this study. Therefore, special attention to dietary intake while on travels and training camps can be a useful strategy to avoid within-day and/or short-duration energy deficits.
Lower energy availability has also been conceptualized to cause performance-related decrements and changes in mental health, including disordered eating attitudes classified as intentional energy deficits [1]. In a study, athletes with a high risk of LEA self-reported performance decrements like decreased coordination, decreased training response, concentration, and depression [23]. The male Kho-Kho players with LEA exhibited lower agility as compared to the optimal EA group (Table 2). However, there were no such differences in other performance parameters related to power and speed in this study. Opposing to this, a study reported lower explosive power among male endurance athletes, with no significant difference in agility [40]. Decrease in performance, particularly in endurance activities, have been related to dietary intake restriction, and male athletes often reported to reduce food intake or under-eat during competitions [41,42,43]. Power-related performances were also reduced with dietary restriction among male wrestlers [44, 45]. Considering that the players in this study have exhibited a lower prevalence of disordered eating and there is no difference across groups, it can be suggestive of an unintentional under-eating among players due to deviation from usual menu plans in training camps. Apart from this, the LEA group in this study also showed reduced overall sleep quality (presented Table 2). Long-term calorie restriction through fasting has been found to have an impact on sleep quality, [46] although short-term fasting or reduced calorie intake among non-exercising individuals has shown improved sleep quality scores [47, 48]. However, athletes can respond differently to energy deficits, particularly during high-intensity training. Research is limited to understand the exact mechanisms, and this needs further exploration.
RED-S has been theoretically postulated to be a result of low energy availability. In the present study, though most of the Kho-Kho players exhibited a moderate-to-high RED-S risk, it was not related to a higher prevalence under the LEA group (Table 4). Although self-reporting errors or biases in activity or dietary recall are considered to have an impact on the association of EA and health outcomes, with a study attributing lack of association of LEA and metabolic hormones to self-reporting [49]. However, it is also a reality that the majority of the studies exploring LEA have resorted to self-reporting to estimate energy intake and/or exercise energy expenditure [50,51,52,53,54,55,56], including the present study. The majority of the studies have also explored LEA and RED-S risk independently [2]. Even in a study [23], that attempted to validate LEA with RED-S risk outcomes, does so by making use of questionnaires that predict an LEA risk factor and not including any form of direct measurement of energy availability. Such questionnaires are also subject to reporting bias [57], particularly when administered through an online mode. A short-term LEA may result in suppression of reproductive hormones and reduction in bone mineral density z score, which may or may not be associated with RED-S risk outcomes. Long-term monitoring of athletes with LEA can provide more definitive association with the health and performance outcomes under the RED-S.
Limitations
In the present study, EA was monitored using estimations of energy intake from dietary recall, energy expenditure using activity records, MET values, predicted RMR using FFM measured by skin fold measurements. Thus, relying heavily on self-reporting of the athlete and technician’s skills for FFM measurement, which in itself can result in under-or-over reporting [58, 59]. Further, these estimations were done only for a single day, thus, not capturing a cumulative energy availability, including the variation in energy intake and activities across a weekly schedule. However, even a within-day energy deficiency has been reported to be associated with reduced RMR, lower estrogen and increased cortisol levels [1, 60]. Apart from this, the players were monitored during their training camp, which might be different from their regular training and dietary habits.
Conclusion
Kho-Kho players in this study exhibited a higher prevalence of LEA, with a reduced lumbar bone mineral density among health outcomes and reduced agility among the performance outcomes in the LEA group compared to the adequate/optimal group. The low EA among the players could be due to unintentional under-eating as opposed to disordered eating behavior, added to the higher training loads. Further, there was a higher prevalence of RED-S risk outcomes among Kho-Kho players, with or without LEA. This study also provides leads for future research to focus on sleep quality disturbances due to energy deficits and to understand the association between short and long-term LEA and RED-S outcomes among athletes.
Data availability
It will be shared based on request.
References
Mountjoy M, Sundgot-Borgen J, Burke L et al (2014) The IOC consensus statement: beyond the female athlete triad—relative energy deficiency in sport (RED-S). Br J Sports Med 48:491–497
Logue DM, Madigan SM, Melin A et al (2020) Low energy availability in athletes 2020: an updated narrative review of prevalence, risk, within-day energy balance, knowledge, and impact on sports performance. Nutrients 12:835
Bratland-Sanda S, Sundgot-Borgen J (2013) Eating disorders in athletes: overview of prevalence, risk factors and recommendations for prevention and treatment. Eu J Sport Sci 13:499–508
De Souza MJ, Koltun KJ, Williams NI (2019) What is the evidence for a Triad-like syndrome in exercising men? Curr Opin Physiol 10:27–34
McGuire A, Warrington G, Doyle L (2020) Low energy availability in male athletes: a systematic review of incidence, associations, and effects. Transl Sports Med 3:173–187
Khelo India, SAI, Ministry of Youth Affairs and Sports, Govt. of India. Kho-Kho Offical Rule Book.: Accessed from https://web.kheloindia.gov.in/kho-kho
Ashwani D, Dhingra M, Kandpal G (2019) Road map to Olympics 2024 & 2028 and intervening competitions: an insight to sports schemes for selection and development of potential athletes. Int J Yogic Hum Mov Sports Sci 4(1):384–389
Rathore VS, Singh AB (2014) Analysis of physical and physiological parameters of kabaddi and kho-kho inter-varsity players. Am J Sports Sci Med 2:13–16
Khanna G, Majumdar P, Malik V et al (1996) A study of physiological responses during match play in Indian national kabaddi players. Br J Sports Med 30:232–235
Jaiswal A (2014) Anthropometric and somatotyping study among the female kho-kho players of pondicherry: a comparative analysis. J Glob Econ 2:1–3
Burke L, Deakin V, Deakin V (2015) Clinical sports nutrition. McGraw-Hill, Boston
Loucks AB, Kiens B, Wright HH (2013) Energy availability in athletes. Food Nutr Sports Perform 3:15–24
Jurov I, Keay N, Rauter S (2022) Reducing energy availability in male endurance athletes: a randomized trial with a three-step energy reduction. J Int Soc Sports Nutr 19(1):179–195
Ainsworth BE, Haskell WL, Whitt MC et al (2000) Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exer 32:S498–S504
Soares MJ, Piers LS, O’dea K et al (1998) No evidence for an ethnic influence on basal metabolism: an examination of data from India and Australia. Br J Nutr 79:333–341
Cherian KS, Shahkar F, Sainoji A et al (2018) Resting metabolic rate of Indian junior soccer players: testing agreement between measured versus selected predictive equations. Am J Hum Biol 30:e23066
Thimmayamma B, Raju P (1987) Food consumption pattern of rural families by weighment and expenditure pattern methods of diet survey. Indian J Nut Diete 24:34–39
Longvah T, An̲antan̲ I, Bhaskarachary K et al (2017) Indian food composition tables: National Institute of Nutrition, Indian Council of Medical Research Hyderabad, pp 1–535
Marfell-Jones MJ, Stewart A, De Ridder J (2012) International standards for anthropometric assessment. International Society for the Advancement of Kinanthropometry, Wellington, New Zealand
Durnin J, Rahaman MM (1967) The assessment of the amount of fat in the human body from measurements of skinfold thickness. Br J Nut 21:681–689
Siri WE (1956) The gross composition of the body. advances in biological and medical physics. Elsevier 4:239–280
Mountjoy M, Sundgot-Borgen J, Burke L et al (2015) The IOC relative energy deficiency in sport clinical assessment tool (RED-S CAT). Br Assoc Sport Exerc Med 49(21):1354
Ackerman KE, Holtzman B, Cooper KM et al (2019) Low energy availability surrogates correlate with health and performance consequences of relative energy deficiency in sport. Br J Sports Med 53:628–633
Garner DM, Olmsted MP, Bohr Y, Garfinkel PE (1982) The eating attitudes test: psychometric features and clinical correlates. Psychol Med 12(4):871–878. https://doi.org/10.1017/S0033291700049163
Surawicz B, Childers R, Deal BJ, Gettes LS et al (2009) AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram. J Am Coll Cardiol 53(11):976–981
Carter DR, Bouxsein ML, Marcus R (1992) New approaches for interpreting projected bone densitometry data. J Bone Miner Res 7:137–145
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ (1989) The pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psy Res 28:193–213
Amaral Vasconcellos FV, Fonseca RT, Dantas EH (2012) Validity and reproducibility of the sargent jump test in the assessment of explosive strength in soccer players. J Hum Kinet 33:115
Roozen M (2004) Illinois agility test. NSCA’s Perform Train J 3:5–6
Furlong LA, Harrison AJ, Jensen RL (2019) Measures of strength and jump performance can predict 30-m sprint time in rugby union players. J Strength Cond Res. https://doi.org/10.1519/JSC.0000000000003170
Loucks A, Verdun M, Heath E (1998) Low energy availability, not stress of exercise, alters LH pulsatility in exercising women. J Appl Physiol 84:37–46
Loucks AB, Thuma JR (2003) Luteinizing hormone pulsatility is disrupted at a threshold of energy availability in regularly menstruating women. J Clin End Metab 88:297–311
Wasserfurth P, Palmowski J, Hahn A et al (2020) Reasons for and consequences of low energy availability in female and male athletes: social environment, adaptations, and prevention. Sports Med-Open 6:1–14
Hooper DR, Kraemer WJ, Saenz C et al (2017) The presence of symptoms of testosterone deficiency in the exercise-hypogonadal male condition and the role of nutrition. Eu J Appl Physiol 117:1349–1357
Keay N, Francis G, Hind K (2018) Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists. BMJ Open Sport Exer Med 4:e000424
Taguchi M, Moto K, Lee S et al (2020) Energy intake deficiency promotes bone resorption and energy metabolism suppression in Japanese male endurance runners: a pilot study. Am J Men’s health 14:1557988320905251
Ihle R, Loucks AB (2004) Dose-response relationships between energy availability and bone turnover in young exercising women. J Bone Mineral Res 19:1231–1240
Rauh MJ, Macera CA, Trone DW et al (2006) Epidemiology of stress fracture and lower extremity overuse injury in female recruits. Nav Health Res Cent San Diego Ca 39(9):1571–1577
Wentz L, Liu P-Y, Ilich JZ et al (2012) Dietary and training predictors of stress fractures in female runners. Int J Sport Nut Exer Metab 22:374–382
Jurov I, Keay N, Spudić D, Rauter S (2022) Inducing low energy availability in trained endurance male athletes results in poorer explosive power. Eur J Appl Physiol 122(2):503–513
Pollock N, Grogan C, Perry M et al (2010) Bone-mineral density and other features of the female athlete triad in elite endurance runners: a longitudinal and cross-sectional observational study. Int J Sport Nut Exer Metab 20:418–426
Eden BD, Abernethy PJ (1994) Nutritional intake during an ultra-endurance running race. Int J Sport Nut Exer Metab 4:166–174
Pfeiffer B, Stellingwerff T, Hodgson AB et al (2012) Nutritional intake and gastrointestinal problems during competitive endurance events. Med Sci Sports Exerc 44:344–351
Tenforde AS, Barrack MT, Nattiv A et al (2016) Parallels with the female athlete triad in male athletes. Sports Med 46:171–182
Ratamess NA, Hoffman JR, Kraemer WJ et al (2013) Effects of a competitive wrestling season on body composition, endocrine markers, and anaerobic exercise performance in NCAA collegiate wrestlers. Eu J Appl Physiol 113:1157–1168
Roemmich JN, Sinning WE (1997) Weight loss and wrestling training: effects on nutrition, growth, maturation, body composition, and strength. J Appl Physiol 82:1751–1759
Karacan I, Rosenbloom AL, Londono JH et al (1973) The effect of acute fasting on sleep and the sleep-growth hormone response. Psychosom J Consult Liaison Psychiatry 14(1):33–37
Martin CK, Bhapkar M, Pittas AG et al (2016) Effect of calorie restriction on mood, quality of life, sleep, and sexual function in healthy nonobese adults: the CALERIE 2 randomized clinical trial. JAMA Internal Med 176:743–752
St-Onge M-P, Mikic A, Pietrolungo CE (2016) Effects of diet on sleep quality. Adv Nutr 7:938–949
Koehler K, Achtzehn S, Braun H et al (2013) Comparison of self-reported energy availability and metabolic hormones to assess adequacy of dietary energy intake in young elite athletes. Appl Physiol Nutr Metab 38:725–733
Heikura IA, Uusitalo AL, Stellingwerff T et al (2018) Low energy availability is difficult to assess but outcomes have large impact on bone injury rates in elite distance athletes. Int J Sport Nutr Exer Metab 28:403–411
Costa PB, Richmond SR, Smith CR et al (2019) Physiologic, metabolic, and nutritional attributes of collegiate synchronized swimmers. Int J Sports Physiol Perform 14:658–664
Lane AR, Hackney AC, Smith-Ryan A et al (2019) Prevalence of low energy availability in competitively trained male endurance athletes. Medicina 55:665
Moss SL, Randell RK, Burgess D et al (2020) Assessment of energy availability and associated risk factors in professional female soccer players. Eu J Sport Sci 21(6):861–870
Muia EN, Wright HH, Onywera VO et al (2016) Adolescent elite kenyan runners are at risk for energy deficiency, menstrual dysfunction and disordered eating. J Sports Sci 34:598–606
McCormack WP, Shoepe TC, LaBrie J et al (2019) Bone mineral density, energy availability, and dietary restraint in collegiate cross-country runners and non-running controls. Eu J Appl Physiol 119:1747–1756
Sim A, Burns SF (2021) Questionnaires as measures for low energy availability (LEA) and relative energy deficiency in sport (RED-S) in athletes. J Eating Disord 9:1–13
Magkos F, Yannakoulia M (2003) Methodology of dietary assessment in athletes: concepts and pitfalls. Curr Opin Clin Nutr Metab Care 6(5):539–549
Ainsworth BE, Ekelund U, Freedson PS et al (2013) Guide to the assessment of physical activity: clinical and research applications. Circulation 128:2259–2279
Fahrenholtz IL, Sjödin A, Benardot D et al (2018) Within-day energy deficiency and reproductive function in female endurance athletes. Scand J Med Sci Sports 28:1139–1146
Acknowledgements
The authors would like to thank Kho-Kho Federation of India for the financial support. We are also thankful to the faculty members of Dept of Nutrition and Dietetics, Faculty of allied Health Sciences and Faculty of Physiotherapy, SGT University for helping us in the data collection.
Author information
Authors and Affiliations
Contributions
Conceptualization: KK, GLK; Data collection and extraction: KK, data analysis and interpretation: KK, KSC; manuscript writing: KSC, KK; review of manuscript: KK, GLK. Finalization of manuscript: KK, KSC, GLK.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Conflict of interest
None declared.
Ethical approval
This study was approved by the Institutional Ethical Committee of Shri Guru Gobind Singh Tricentenary (SGT) University, Gurgaon, Haryana, India (SGTU/FPHY/2021/432 dated 23/07/2020).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kalpana, K., Cherian, K.S. & Khanna, G.L. Energy availability and RED-S risk assessment among Kho-Kho players in India. Sport Sci Health 19, 1101–1108 (2023). https://doi.org/10.1007/s11332-022-00996-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-022-00996-z