
Abstract
Purpose
Occlusal changes are common during long-term treatment with oral appliances (OAs) for sleep apnea. The aim of the present study was to compare subjectively reported bite changes with objective findings.
Methods
Consecutive adherent treated patients were asked to participate in this study. The patients responded to two questionnaires using numeric visual analogue scales (VAS), ranging from 0 (not at all) to 10 (very much). The first questionnaire included open questions and the second questionnaire comprised specific questions about side effects. Measurements of overjet, overbite, and space for the teeth were made on plaster casts taken before treatment start and at follow-up.
Results
Thirty-eight (12 women) patients with a median age of 64 years (interquartile range (IQR) 57 to 69 years) and a median treatment time of 9.5 years (IQR 5.8 to 14.3 years) were included. Overjet, overbite, the molar relationship, and the irregularity of the lower front teeth had changed significantly during treatment. There were no associations between any of the patients’ responses and the objectively measured bite changes. Younger patients, those with a small baseline overjet or overbite and those who developed an anterior crossbite were more likely to report bite changes.
Conclusions
Patients who choose to continue long-term treatment with oral appliances for sleep apnea are unaware of various types of bite changes. Such changes will, however, progressively increase in magnitude and be more difficult to take care of, if needed. It is therefore important continuously to follow up patients in regard to bite changes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Occlusal changes are common during long-term treatment with oral appliances (OAs) for sleep apnea [1, 2], but patients more seldom complain of any dental side effects [3,4,5,6,7,8,9,10,11,12].
The nightly anterior repositioning of the lower jaw with an oral appliance will produce distally directed forces on the upper teeth and anteriorly directed ones on the lower teeth [13]. The molars in the posterior parts of the dentition will reposition into a more class III relationship, and the changed inclinations of the front teeth will decrease the overjet and the overbite (Fig. 1) [1, 2]. The teeth may have more space [14,15,16,17] or become more crowded [18].

Illustration of overjet, overbite, and molar relationship measurements and expected bite change
Patients less frequently report occlusal changes than objective findings reveal according to studies that have included both objective and subjective assessments [3,4,5,6,7,8,9,10,11,12]. Between 2% and 45% of patients report occlusal changes after 1 to 6 years, despite the fact that all the studies have found significant reductions in overjet and overbite [3,4,5,6,7,8,9,10,11,12]. Up to 86% of the patients have been seen to develop objectively measured occlusal changes after 5 years’ treatment, according to another study [14]. It is, however, unknown whether patients’ reports of bite changes are the same as the objectively measured findings.
The aim of the present study was to compare subjectively reported bite changes with objective findings in patients who choose to continue long-term oral appliance therapy.
Methods
Study design
Consecutively followed up patients from a retrospective sample answered questionnaires in order to evaluate whether patients were able to detect bite changes of various types. Patients’ reports of bite changes were compared with objective measurements on study casts. The study protocol was approved by the ethics review board at Umea University, EPN-2015/291-31, and all the patients gave their written informed consent. The sample size was estimated at least 14 patients in each group of patients who had experienced subjective bite changes and those who had not, in order to detect a difference in overjet reduction of ≥ 1 mm with a power of 0.8 and a p value of less than 0.05.
Study sample
Consecutive patients who came for a follow-up and appliance replacement after at least 3 years’ treatment were asked to participate in this study. Exclusion criteria: 50% of the nights or less use of the appliance; dementia or physical illness that prevented participation in the study; insufficient quality of initial study casts; unwillingness to participate. The patients were assessed for eligibility between September and December 2015 and between March and May 2017. The patients had to be included during two time spans of consecutively followed up patients because of time constraints at the clinic.
Of 58 patients who were followed up, 20 patients were excluded. Among the excluded patients, ten reported insufficient adherence to the appliance, two patients were unable to take part because of lack of time, and one patient had no baseline plaster casts. Another seven patients were excluded, because they wanted to discontinue OA therapy and be referred for CPAP therapy; six patients because of insufficient treatment effect from OA and one patient because of increased oral mucosal tenderness when wearing the oral appliance. Thirty-eight patients were included in the study (Table 1). Among the included patients, one had received frontal restorations during the study period and another patient had molar extractions. In these two patients, it was therefore impossible to measure overjet and overbite changes or alterations in molar relationships.
Questionnaires
The patients responded to two questionnaires about adherence and side effects. The first questionnaire included open questions about side effects in order for the patients spontaneously to describe their experiences of the treatment. This questionnaire also included questions about adherence. The second specific questionnaire was distributed after the first questionnaire had been answered and given back to the dental personnel. This second questionnaire included specific questions. The patients were asked whether they had experienced bite changes of various types (Table 2). They were also asked about some other types of frequently reported side effects (Table 2).
Both questionnaires used numeric visual analogue scales (VAS), ranging from 0 (not at all) to 10 (very much). A score of two or more on the scale was regarded as a subjective report of the various side effects.
Measurements on plaster casts
Measurements on the plaster casts taken before treatment start and at follow-up were made regarding changes in overjet, overbite, irregular front teeth, and spacing during the treatment period. Overjet, overbite, and molar relationships were measured with a sliding caliper on the plaster casts oriented according to a wax index in central occlusion (Fig. 1). Frontal irregularity was measured with Little’s Irregularity Index [19]. This index assesses the irregularity of the front teeth. The distances between two contact points or other easily identifiable characteristics on the approximal surfaces of two adjacent front teeth are measured on all contact points between the canines. All distances are then added and described in Little’s Irregularity Index (Fig. 2). An increased value means more irregularity. Spacing between teeth was measured as the distance between two adjacent front teeth. The distances between the canines were added, separately for each jaw. The numbers of occlusal tooth contacts in the premolar-molar area on the wax indices at baseline and follow-up were registered and compared. All measurements were repeated after at least 2 weeks and blinded with respect to the results of the questionnaires. The mean value of the two measurements was used in the analysis.

Illustration of the measurements of Little’s Irregularity Index, where the distances between the contact points (arrows) of the anterior teeth are summarized
Statistical analysis
Data were described in median and interquartile ranges (IQRs). These cut-offs were used to identify patients with various bite changes and baseline characteristics. Differences in measurements before and after treatment were analyzed with Wilcoxon’s test for paired samples. The Mann-Whitney U test was used to compare differences between subgroups of patients. The Fisher’s exact test was used to compare patients who reported bite changes with those who did not report any changes and to identify associated characteristics. The significance level was defined as p < 0.05.
Results
Subjective reports in the questionnaires
In the first open questionnaire that was intended to show spontaneously reported side effects, 5 of the 38 patients (13%) reported occlusal changes. Other spontaneously reported problems included appliance-related problems, such as soreness or difficulty taking the device on or off in five patients (13%), dry mouth in four (11%), jaw tenderness in three (8%), periodontal problems in two (5%), or difficulty sleeping with the appliance in place in one patient (3%).
In the second specific questionnaire, 17 of the 38 patients (45%) reported occlusal changes (Table 2). These 17 patients included all five patients who had spontaneously reported occlusal changes. Only the combined results of questions 1 and 2 were considered in the evaluations, because of the few patients who answered positively on the remaining questions.
Objectively measured changes in dental occlusion and teeth position
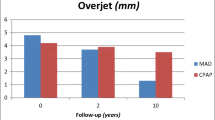
Overjet and overbite decreased, the lower molars repositioned anteriorly in relation to the upper molars, and the irregularity of the lower front teeth increased in the studied sample (Table 3). The median change in overjet was − 1.6 mm (p < 0.001; IQR = − 2.3 mm to − 0.5 mm) and the median change in overbite was − 0.7 mm (p < 0.001; IQR = − 1.6 mm to − 0.1 mm) (Table 3). There was no increase in the spacing between the teeth, but the irregularity of the lower front teeth increased by 0.8 mm (p = 0.001; IQR = − 0.2 mm to 1.3 mm).
Patients’ reports compared with objective findings
Five of the 17 patients who reported occlusal changes defined as 2 or more on VAS (31%) had an objectively measured overjet reduction of the median value (1.6 mm) or more, and 13 of the 21 patients who did not report any occlusal changes (62%) (p = 0.10) had an objective overjet reduction (Table 4). Patients’ reports of bite changes were unrelated also to changes in overbite or in molar relationships (Table 4).
Patients within the largest quartile of overjet reduction (≥ 2.3 mm) reported a median of 0 (IQR = 0 to 7) on VAS, while patients in the smallest quartile of overjet reduction (< 0.5 mm) reported a median of 2 on VAS (IQR = 0 to 6) (p = 0.78). Patients within the largest quartile of overjet reduction had a larger initial overjet of a median of 5.4 mm (IQR = 3.5 to 7.8 mm) at treatment start than the patients within the smallest quartile of overjet reduction with a median of 2.6 mm (IQR = 2.0 to 2.8 mm) (p = 0.002).
Four of the 38 patients had developed a negative overjet at follow-up. Two of these four patients spontaneously reported an occlusal change and three of them reported an occlusal change in the specific questionnaire.
Characteristics of patients reporting occlusal changes
Patients who reported occlusal changes had more frequently a smaller initial overjet or overbite and were younger than those who did not report any such changes (Table 4).
Discussion
Significant bite changes were found in the present sample of patients who had been treated in the long term with oral appliances for sleep apnea. Overjet and overbite decreased, the molars changed their relationship, and the lower front teeth became more irregular. These bite changes were not identified by the patients’ answers in the questionnaires. Patients’ reports of bite changes are therefore uncertain in follow-ups of OA treatment.
Only five patients reported spontaneously about bite changes in the open questionnaire. More patients reported bite changes in the specific questionnaire, although only 31% of these patients had an overjet reduction of 1.6 mm (median value) or more (Table 4). In the remaining group of patients who did not report any bite changes, as many as 62% also had an objectively measured overjet reduction. Consequently, the majority of the patients were unable to identify overjet reductions, despite that change in overjet is fairly easy to detect and that the patients had been informed about the possibility of bite changes developing during OA treatment. The results of the study mean that answers to both open and specific questions are uncertain when it comes to detecting objective bite changes.
Some changes in dental occlusion might be favorable [14]. Patients with a large overjet at baseline can normalize their dental occlusion during long-term treatment with oral appliances for sleep apnea. In addition, those patients with the largest initial overjet have been found to be more likely to receive a more pronounced effect of treatment than those with a smaller initial overjet [20]. This effect was also present in the present sample, since the patients with a large decrease in overjet of ≥ 2.3 mm had a larger initial overjet than those who had the smallest reductions in overjet using the device. This means that patients with the largest baseline overjet who experience the greatest benefit from an overjet reduction will also have the best chance of experiencing an effect of this kind. In summary, some patients might, in fact, be satisfied with the bite changes resulting from oral appliance therapy, since their class II malocclusion will normalize during treatment. It is therefore understandable that these patients are less likely to identify bite changes. Despite that, a large A-P bite change will reduce the advancement of the lower jaw by the appliance and there is a risk for reduced efficacy of the device, if it is left unadjusted.
Unfavorable bite changes may develop in patients who have a normal bite or class III malocclusion at baseline [14]. In these patients, long-term treatment with oral appliances may create or aggravate a malocclusion. A recent meta-analysis has concluded that the more marked the malocclusion, the more likely it is that patients will experience impaired oral health [21] and report this in a questionnaire. Three of the four patients in this study who had developed an anterior crossbite at follow-up had noticed a bite change. In addition, patients with a small baseline overjet or overbite more often reported bite changes. Consequently, the patients’ reports of bite changes are in line with dentists’ view of the severity of bite changes.
Some previous studies have reported that subjective feelings of bite changes decrease over time [6, 9], while the degree of objectively assessed bite changes increases [1,2,3,4,5,6,7,8,9,10,11,12, 16]. The patients included in the present study had used oral appliances for at least 3 years. They had chosen to continue treatment based on subjective benefits and information about effects and side effects from their dentists at earlier follow-ups, usually at intervals of 2 to 3 years. Consequently, some patients who were not included in the present study had discontinued treatment because of lack of treatment effects or dental side effects. The present sample, as well as samples in other long-term studies, might therefore primarily describe patients who are able to acclimatize easily to changes in their teeth positions or those who, in fact, benefit from the treatment. It would be of interest to study also patients who discontinue treatment. The aim of the present study was, however, to evaluate risks for undetected bite changes in patients who are positive to continue treatment.
Previous studies have used questionnaires where patients respond directly on paper [3,4,5,6,7,8,9,10,11,12] or in telephone interviews. It is not known whether the responses to the paper questionnaire were made totally beforehand, without any involvement on the part of the researchers, or were in some way influenced by the professional team. The present study primarily included a first open questionnaire in order for the patients to respond the type of side effects they had spontaneously noticed. After these responses were submitted, the patients responded to more specific questions that were thought to provide some guidance. The first questionnaire constitutes novel information on patients’ spontaneous experiences of bite changes. The very low level of positive answers in the open questionnaire compared with more frequent positive answers in the specific questionnaire in this study indicates that patients who choose to continue treatment do not seem to care significantly about bite changes.
In the question about occlusal changes, combined answers relating to permanent bite changes and temporary ones were included. In a previous study [8],only 4% of the patients had noticed permanent bite changes. This can be compared with the 41% of the patients who reported temporary bite changes, which is more in line with the 25% who had objectively measured bite changes. Fransson et al. [4] report that only 2 of 64 patients report a permanent change in occlusion, despite significant changes in overjet and overbite in the whole sample. Consequently, it might be difficult for patients to subdivide permanent and temporary bite changes and therefore both types of assessments were included.
Conclusions
Patients who choose to continue long-term treatment with oral appliances for sleep apnea are either unaware of or do not care significantly about the various types of bite changes that may develop. These patients might therefore be at risk to suffer from undetected bite changes. It is therefore important to continuously follow up patients with respect to bite changes, since these will progressively increase in magnitude and be less easy to take care of, if needed.
References
Araie T, Okuno K, Ono Minagi H, Sakai T (2018) Dental and skeletal changes associated with long-term oral appliance use for obstructive sleep apnea: a systematic review and meta-analysis. Sleep Med Rev 41:161–172. https://doi.org/10.1016/j.smrv.2018.02.006
Bartolucci ML, Bortolotti F, Martina S, Corazza G, Michelotti A, Alessandri-Bonetti G (2018) Dental and skeletal long-term side effects of mandibular advancement devices in obstructive sleep apnea patients: a systematic review with meta-regression analysis. Eur J Orthod 41:89–100. https://doi.org/10.1093/ejo/cjy036
Battagel JM, Kotecha B (2005) Dental side-effects of mandibular advancement splint wear in patients who snore. Clin Otolaryngol 30:149–156. https://doi.org/10.1111/j.1365-2273.2004.00944.x
Fransson AM, Tegelberg A, Johansson A, Wenneberg B (2004) Influence on the masticatory system in treatment of obstructive sleep apnea and snoring with a mandibular protruding device: a 2-year follow-up. Am J Orthod Dentofac Orthop 126:687–693. https://doi.org/10.1016/S0889540604006614
Fritsch KM, Iseli A, Russi EW, Bloch KE (2001) Side effects of mandibular advancement devices for sleep apnea treatment. Am J Respir Crit Care Med 164:813–818
Gong X, Zhang J, Zhao Y, Gao X (2013) Long-term therapeutic efficacy of oral appliances in treatment of obstructive sleep apnea-hypopnea syndrome. Angle Orthod 83:653–658. https://doi.org/10.2319/060412-463.1
Hammond RJ, Gotsopoulos H, Shen G, Petocz P, Cistulli PA, Darendeliler MA (2007) A follow-up study of dental and skeletal changes associated with mandibular advancement splint use in obstructive sleep apnea. Am J Orthod Dentofac Orthop 132:806–814. https://doi.org/10.1016/j.ajodo.2005.08.047
Marklund M, Franklin KA, Persson M (2001) Orthodontic side-effects of mandibular advancement devices during treatment of snoring and sleep apnoea. Eur J Orthod 23:135–144
Martinez-Gomis J, Willaert E, Nogues L, Pascual M, Somoza M, Monasterio C (2010) Five years of sleep apnea treatment with a mandibular advancement device. Side effects and technical complications. Angle Orthod 80:30–36. https://doi.org/10.2319/030309-122.1
Pantin CC, Hillman DR, Tennant M (1999) Dental side effects of an oral device to treat snoring and obstructive sleep apnea. Sleep 22:237–240
Rose E, Lehner M, Staats R, Jonas IE (2002) Cephalometric analysis in patients with obstructive sleep apnea. Part II: Prognostic value in treatment with a mandibular advancement device. J Orofac Orthop 63:315–324
Wang X, Gong X, Yu Z, Gao X, Zhao Y (2015) Follow-up study of dental and skeletal changes in patients with obstructive sleep apnea and hypopnea syndrome with long-term treatment with the Silensor appliance. Am J Orthod Dentofac Orthop 147:559–565. https://doi.org/10.1016/j.ajodo.2015.01.013
Cohen-Levy J, Petelle B, Pinguet J, Limerat E, Fleury B (2013) Forces created by mandibular advancement devices in OSAS patients: a pilot study during sleep. Sleep Breath 17:781–789. https://doi.org/10.1007/s11325-012-0765-4
Almeida FR, Lowe AA, Otsuka R, Fastlicht S, Farbood M, Tsuiki S (2006) Long-term sequellae of oral appliance therapy in obstructive sleep apnea patients: part 2. Study-model analysis. Am J Orthod Dentofac Orthop 129:205–213. https://doi.org/10.1016/j.ajodo.2005.04.034
Chen H, Lowe AA, de Almeida FR, Fleetham JA, Wang B (2008) Three-dimensional computer-assisted study model analysis of long-term oral-appliance wear. Part 2. Side effects of oral appliances in obstructive sleep apnea patients. Am J Orthod Dentofac Orthop 134:408–417. https://doi.org/10.1016/j.ajodo.2006.10.031
Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR (2014) Obstructive sleep apnea and mandibular advancement splints: occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med 10:1285–1291. https://doi.org/10.5664/jcsm.4278
Rose EC, Staats R, Virchow C Jr, Jonas IE (2002) Occlusal and skeletal effects of an oral appliance in the treatment of obstructive sleep apnea. Chest 122:871–877
Norrhem N, Nemeczek H, Marklund M (2017) Changes in lower incisor irregularity during treatment with oral sleep apnea appliances. Sleep Breath 21:607–613. https://doi.org/10.1007/s11325-016-1456-3
Little RM (1975) The irregularity index: a quantitative score of mandibular anterior alignment. Am J Orthod 68:554–563
Marklund M (2006) Predictors of long-term orthodontic side effects from mandibular advancement devices in patients with snoring and obstructive sleep apnea. Am J Orthod Dentofac Orthop 129:214–221. https://doi.org/10.1016/j.ajodo.2005.10.004
Sun L, Wong HM, McGrath CP (2017) Relationship between the severity of malocclusion and Oral health related quality of life: a systematic review and meta-analysis. Oral Health Prev Dent 15:503–517. https://doi.org/10.3290/j.ohpd.a38994
Funding
The County Council of Västerbotten provided financial support in the form of grant funding. The sponsor played no role in the design or conduct of this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
I, the author, certify that I have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript. Marie Marklund has received a consultancy fee from ResMed.
Ethical approval
All the procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Comment
Dr. Marklund's work on this subject has been indispensable. Her dedication in helping to elucidate these side effects are extremely valuable and appreciated as this field grows in both popularity and application. It is important to see how these side effects present clinically while also understanding how they affect patients in both objective and subjective ways.
Thomas Schell
NH, USA
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Marklund, M. Subjective versus objective dental side effects from oral sleep apnea appliances. Sleep Breath 24, 111–117 (2020). https://doi.org/10.1007/s11325-019-01852-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-019-01852-0