
Abstract
Objectives
This study examined the long-term effects of the Better Start program, an adaptation of Incredible Years parent training enhanced with home visits, for families with mothers being released from incarceration.
Methods
Participants in this quasi-experimental longitudinal study were 224 mothers, of whom 145 (64.7%) received intervention and the other mothers constituted a no intervention group. Official criminal justice records and mother reports of parenting behaviors and child behavior were collected up to 10 years after intervention. Mixed effects models, Cox regression analyses, and latent linear growth models were used to test potential intervention effects on adolescent delinquency, maternal recidivism, parenting behaviors, and disruptive child behaviors.
Results
Outcomes favoring participants in the intervention condition were found for adolescent delinquency, maternal recidivism, and the number of disruptive child behaviors.
Conclusions
Effects on maternal recidivism and delinquency in their children indicate that the Better Start program contributes to preventing the intergenerational transmission of delinquency.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Children of incarcerated parents are at-risk for delinquency and disruptive behavior problems (Murray et al., 2012). This intergenerational transmission of delinquency may be especially strong for children of incarcerated mothers, even compared to incarcerated fathers (Besemer et al., 2017). Maternal incarceration is one of the factors that add to the accumulation of risk factors in these children’s lives, such as financial hardship, maternal depressive symptoms, parenting stress, and suboptimal parenting behaviors (Dallaire, 2007; Loper & Tuerk, 2006; Menting et al., 2017), that may together explain adverse outcomes like delinquency. The stressful, traumatic aspects of incarceration, its consequent negative effects on parent–child bonds and family stability, as well as the detrimental role of stigma and labeling have been highlighted in the literature about parental incarceration (Giordano et al., 2019). Thus, maternal incarceration offers an opportunity to identify vulnerable children and provide an intervention to prevent adverse outcomes (Junger et al., 2013).
Parenting can contribute to the intergenerational transmission of delinquency (Wildeman, 2020). Children of incarcerated mothers may develop delinquent behavior patterns themselves, because their mothers have had fewer opportunities to develop good parenting skills (Menting et al., 2017; Phillips et al., 2004), and parenting is known to play a key role in the development of delinquency and other disruptive behavior problems (Hoeve et al., 2009; Patterson, 2016). Consequently, interventions to support parenting could play a key role in the prevention of delinquency and other disruptive behaviors. Indeed, intervening early in children’s lives is crucial given the early start of antisocial trajectories (Broidy et al., 2003; Shaw et al., 2005), malleability of children’s development at younger ages (Wachs et al., 2014), strong evidence-base for parenting interventions for young children (Comer et al., 2013; Kaminski & Claussen, 2017; McCart et al., 2006), and higher economic return from early intervention compared to later intervention (Heckman, 2006). Accordingly, evidence about life-course-persistent antisocial trajectories, which seem to be affected by risk factors like inadequate parenting, has provided impetus for early-years crime prevention (Moffitt, 2018). Hence, in endeavors to break the cycle of intergenerational transmission of delinquency, delivering an evidence-based parenting intervention to mothers being released from incarceration seems a promising approach.
Theoretically, both the proximal targets of parenting intervention (i.e., parenting behaviors and disruptive child behaviors) and maternal delinquency may explain the at-risk status of children affected by maternal incarceration. The premise that parenting affects the chances that offspring get involved in antisocial behavior is embedded in most theories of delinquent and antisocial behavior (Thornberry et al., 2003). Even static theories, like self-control theory, assume that inadequate parenting is at least partially responsible for unadjusted behaviors including delinquency. More dynamic theories also emphasize the role of parenting by stating that delinquent behaviors are learned in the same ways as other behaviors and that this learning may be strongest in childhood when the bond between parents and their children is strongest (Van der Rakt et al., 2010). In this same line of reasoning, social learning theory emphasizes the role of parenting in the development of disruptive child behaviors and delinquency through operant principles and induction and further specifies that youth may observe and imitate their parents’ criminal behavior (Besemer et al., 2017; Murray & Farrington, 2008). Hence, from a life-course perspective, one would expect more intergenerational transmission when parents show criminal behavior after the traditional peak of offending (Besemer et al., 2016), as there might be more possibilities for social learning and behavior if this happens during the child’s life and behaviors may be considered more deviant (Besemer et al., 2016; Van der Rakt et al., 2010). This influence extends beyond childhood (Van der Rakt et al., 2010). Moreover, maternal delinquency is also assumed to have effects on mothers’ own development, including effectiveness of their parenting (Besemer et al., 2016), which makes parenting one of the most proximate and powerful influences on the development of children’s antisocial behaviors (Thornberry et al., 2003). Therefore, it can be assumed that a parenting intervention aimed at young children affected by maternal incarceration may affect their own delinquency later in adolescence in multiple ways.
Indeed, long-term effects of early prevention programs on offending have been found and tend to be stronger for children who were more at-risk (Deković et al., 2011). This suggests that early prevention programs like parenting intervention can help put children on more positive developmental trajectories. More specifically, it has been suggested based on systematic reviews that family-based interventions are possibly the most effective developmental prevention programs regarding offending outcomes (Weisburd et al., 2016). Moreover, meta-analytic evidence shows that early family/parent training is effective in reducing behavior problems (Piquero et al., 2016), whereas descriptive evidence also suggests effectiveness of such interventions regarding delinquency and crime in later adolescence and adulthood (Piquero et al., 2008). Therefore, empirical evidence also seems to suggest that parenting interventions are a viable strategy for the prevention of delinquency and for building a safer society (Piquero et al., 2016). For families affected by maternal incarceration, such interventions may be most successful (Eddy et al., 2022) and needed (Burraston & Eddy, 2017) in the period when mothers leave prison and reenter community and family life. This is a period when mothers may be highly motivated to strengthen their families (Alsem et al., 2021; Clark et al., 2023) and when new family habits are formed (Adams et al., 2017; Begun et al., 2017).
Better Start (Menting et al., 2014a; Menting & de Castro, 2021) is such a parenting intervention, that is delivered to mothers of 2-to-10-year-old children in the period when mothers leave incarceration. The intervention aims to prevent disruptive behavior problems, including delinquency, in the children, as well as recidivism in their mothers (Menting & de Castro, 2021). It is based on the evidence-based Incredible Years parent training (Menting et al., 2013; Webster-Stratton, 2001) and consists of both group sessions and home visits. The intervention model of Better Start (Menting & de Castro, 2021) builds on the unique motivation that mothers may have after incarceration to invest in their children’s future (Alsem et al., 2021). By emphasizing predictable and consistent parenting interactions and caregiver relationships, sensitivity to children’s cues, and acceptance of emotions, parents learn to give their children a sense of trust in the world and the people in it (Webster-Stratton, 2007b) after separation from their mother. In line with the failure model (Hirschi, 2004), the intervention targets dynamic risk factors (limited skills, limiting cognitions, depressive symptoms, and failure) and protective factors (family bonding, problem solving, and self-efficacy) to increase mothers’ motivation to abstain from crime. This is in line with international human rights conventions as well as United Nations standards and norms that clearly acknowledge the importance of interventions that support the social reintegration of offenders to prevent further crime (United Nations Office on Drugs and Crime (UNODC), 2018).
It can be assumed that parenting intervention during reentry may have an effect on recidivism, as motherhood can both serve as a motivator to remain crime-free and as a stressor that may lead to failed desistance (Rodermond et al., 2016). Indeed, spending time caring for children and feeling influential and effective as a mother seems to contribute to complying with the requirements of supervision and avoiding arrest, but mothers’ intentions may be overwhelmed by the numerous challenges in these mothers’ lives (Adams et al., 2017). This illustrates that being a parent after release involves more than knowing certain pieces of knowledge and types of skills, but involves getting support for using those skills and employing them within family relationships on a day-to-day basis after release (Krysik & Rodriquez, 2022, Chapter 8), and that successful reentry may therefore also depend on addressing vital factors for well-being along parenting skills (Eddy et al., 2022). There is some evidence that this might indeed have an effect on recidivism: For a parent management training program, intervention effects were found on both arrests through 1 year after release from prison and self-reported criminal behavior to 6 months post-release (Eddy et al., 2022). These results are promising given the small effects or inconsistent findings regarding recidivism in the broader literature (e.g., Asscher et al., 2014; de Vries et al., 2018; Landenberger & Lipsey, 2005; Pearson et al., 2002; Verweij et al., 2017) but also ask for a more long-term evaluation.
For Better Start, the short-term effects of the intervention on parenting behavior and disruptive child behavior were shown in a randomized controlled trial (Menting et al., 2014a). Although these results directly after intervention are promising, longer-term outcomes seem even more relevant to the aims of this intervention. Yet, intention-to-treat results of a short-term follow-up eight months after intervention (Alsem et al., 2021) were mixed: There was some evidence for effects on maternal inconsistent discipline, but it was more difficult to demonstrate sustained effects on disruptive child behaviors. However, it should be noted that the participating children had not yet reached ages at which delinquent behavior becomes more likely, and also not enough time has passed to provide an accurate estimate of their mothers’ recidivism. Therefore, a long-term follow-up would be needed to truly evaluate whether the intervention prevents delinquent behavior.
Even though long-term intervention studies are important for informing theory, policy, and practice (Lacourse et al., 2002; Tomlinson et al., 2020), such studies are scarce. This may be especially true for selective prevention interventions (i.e., for children who are considered at high risk due to biological or environmental risk factors). It can be assumed that it is more difficult to maintain effects in these at-risk populations than in clinical populations (Leijten et al., 2013; Tomlinson et al., 2020; Troy et al., 2018), given the smaller initial effects, less parental motivation because of relatively mild child problems, numerous stressors that make it more difficult to maintain changes, and therefore need for ongoing support in these families (Leijten et al., 2013; Scott et al., 2014). Reviewing the evidence, there was indeed no evidence of effects on parenting and disruptive child behavior in a long-term follow-up (5–10 years after intervention) of Incredible Years in a selective prevention sample (Scott et al., 2014). However, more promising results of Incredible Years regarding restoring the family’s ability to care for children were found in a child protection service sample (Leclair Mallette et al., 2021) and on disruptive child behavior in other selective prevention samples at 1- to 1.5-year follow up (Brotman et al., 2008; Gross et al., 2003; Kim et al., 2008; Webster-Stratton, 1998). Hence, few positive results regarding the proximal outcomes of selective preventive parenting interventions have been found in the longer term (i.e., more than a year after intervention), suggesting that positive results may be especially hard to obtain in selective prevention samples.
On the one hand, these mixed findings regarding selective prevention suggest that it may be also difficult to find long-term effects of Better Start. This intervention focuses on a hard-to-retain population of mothers being released from incarceration (Byrne, 2005; Eddy et al., 2001; Goshin & Byrne, 2012), who face many stressors (Arditti & Few, 2008; Menting et al., 2017). Consistent with this, mixed findings at the 8-month follow-up were found for this intervention (Alsem et al., 2021). On the other hand, the intervention effects directly after intervention can be considered relatively large for selective prevention (Menting et al., 2013; Menting et al., 2014a) and the most relevant triggers for delinquent behavior may only become salient once children have become older than in the initial studies.
In sum, despite urgent societal and scientific needs to know the long-term effects of selective prevention programs, there is a paucity of solid empirical data. Therefore, the aim of the current study was to evaluate the long-term preventive effectiveness of the Better Start program. We hypothesized that the intervention would have effects on adolescent delinquency and maternal recidivism, as primary outcomes regarding the intergenerational transmission of delinquency. We further hypothesized that the intervention would have long-term effects on maternal parenting behaviors and disruptive child behaviors, as proximal outcomes of parenting intervention.
Method
Participants
The sample consisted of mothers being released from incarceration who had participated up to 10 years ago in the original study (Menting, et al., 2014a) or in one of the intervention groups that had started after the original study—up to September 2014. Mothers were originally recruited by means of nationwide screening within all penitentiary institutions in the Netherlands. The inclusion criteria were that mothers had to be (a) incarcerated and expected release before the start of the individual home visits (i.e., within 3 or 4 months) or recently released from incarceration (i.e., not exceeding 6 months), (b) caregiver for at least one 2- to 10-year-old child after incarceration, and (c) able to see their children during the period of the group sessions during at least 2 weekends per month (i.e., during weekend leaves for incarcerated mothers). If mothers met the criteria regarding more than one child, they were invited to provide information about three children maximum.
Participants from the original study and later participants mainly differ in that all participants from later groups were invited to participate in the intervention. That is, in the original study, mothers were partly randomized to a control group (n = 26); intervention mothers (n = 55), and mothers who were invited for the intervention but did not attend any sessions in the original study (i.e., opt-out mothers; n = 26) were also included in the current sample. Regarding the later groups, 117 mothers who participated in the intervention as routine care after the original study were included in the current sample, including 90 mothers who had received at least one session. The complete sample therefore consisted of 224 mothers with 328 participating children: 145 intervention mothers (64.7%), 26 control mothers (11.6%), and 53 opt-out mothers (23.7%).
Participant information was available for 213 mothers of 313 participating children (see Table 1). Mothers were on average 32.88 years old (SD = 7.37) at the start of the intervention, and 40.4% were born in the Netherlands. About half of the mothers (48.6%) did not have a partner. Most mothers (59.6%) participated with one child. About half of the mothers (50.2%) were still incarcerated during the intake interview. For most mothers (70.4%), this was their first incarceration, and about half of the mothers (54.3%) reported that they were convicted because of a drug-related offense. The sentence length varied widely (range 0.3–120.0 months). Half of the mothers were low educated, and most mothers (59.1%) had never received another parenting intervention before or only a support program that was offered during incarceration (23.6%). During the intake interview, mothers reported adverse socioeconomical circumstances: e.g., 83.5% reported having debts, of whom 18.0% was in debt restructuring and 40.4% intended to do so.
The child sample was approximately balanced in gender (47.9% boys), and the children were on average 6.56 years old (SD = 2.67) at the start of the intervention. Almost all participating children (97.0%) were the biological children of a participating mother. During their mother’s incarceration, most children had some contact with their mothers: during telephone contact (92.7%), visits (61.1%), and/or weekend leaves (55.7%). A small number of children (n = 7) stayed with their mothers throughout incarceration. Furthermore, mothers reported to have had frequent contact with the caregivers of their children during incarceration (M = 7.48 per week, SD = 7.94).
In this selective prevention sample, most children did not seem to experience serious behavioral difficulties. The Child Behavior Checklist or Adult Behavior Checklist (Achenbach & Rescorla, 2000, 2001, 2003) was used during the long-term follow-up (n = 168). Results showed that the scores were in the average range for internalizing (T = 50.55; 17.9% in [sub]clinical range), Externalizing (T = 50.48; 18.0% in [sub]clinical range), and Total Problems (T = 50.62; 18.5% in [sub]clinical range).
Procedure
Mothers from the original study and intervention mothers from later intervention groups were visited annually, from 2013 to 2020, for individual assessments with a research assistant. In addition, the research assistant attempted to contact each mother once in between assessments to prevent losing track of them. Assessments and telephonic contact stopped earlier if mothers reached 10 years after intervention before 2020. Children were asked to fill out questionnaires from the age of 11. Furthermore, data regarding 43 mothers with 63 children who participated in the original study was assessed once after the follow-up of the original study (Alsem et al., 2021), but before 2013 (M = 2.11 years after intervention, SD = 0.49) to prevent losing track of them.
Informed consent forms were signed by mothers at the start of the original study; consent procedures were repeated before the first assessment of the long-term follow-up and included consent for sending questionnaires to their children’s teachers and requesting official records. At age 12, children also signed a consent form regarding their own participation. Information letters and consent forms for mothers were available in Dutch and Spanish. Participation was voluntary for all participants and they were assured of confidentiality. Participants received monetary compensation (i.e., gift cards) for the time spent completing questionnaires: For each completed assessment during the long-term follow-up, mothers received €15 per child, whereas children received €5. The study was approved by the Ethics Committee of the Utrecht University Faculty of Social and Behavioral Sciences (#20-590).
Intervention
The Better Start intervention included 12 or 14 weekly group sessions of 2 or 2.25 h (depending on the version of the program used) and four individual 1.5-h home visits. The group sessions, which were offered in groups of 7 to 15 mothers, are based on the Incredible Years parent training (Webster-Stratton, 2001)—a manualized, collaborative parenting intervention that uses video vignettes to trigger discussions, problem solving, and practices (e.g., role plays). So, mothers discussed video vignettes and put learned techniques into practice in role plays in collaboration with two group leaders, covering play; praise and rewards; ignoring undesired behavior; limit setting; and logical consequences of behavior. Incredible Years is based on social learning theory and has been used and studied both as a treatment for children with severe conduct problems and as a preventive intervention for improving parenting behaviors and reducing the risk of disruptive child behavior (Menting et al., 2013). The Incredible Years parent training was considered a suitable approach for mothers being released from incarceration, because of its demonstrated effectiveness, tailoring to families’ needs (e.g., by parents setting their own goals), and collaborating and empowering approach (Menting et al., 2014a).
Home visits were added to these group sessions to support mothers to use parenting skills in difficult individual situations and to provide individual practical consultations. These home visits included two topics of the ADVANCE Incredible Years parent training (Webster-Stratton, 2002): communication and problem solving with adults and children (see also Menting et al., 2014a; Menting & de Castro, 2021). Mothers received home visits in the 4 to 6 months after completion of the group sessions and were visited by one or both of the group leaders who had also delivered the group sessions.
The intervention was delivered by nine team members, who had backgrounds in child psychology or within penitentiary institutions for women and were trained during a 3-day workshop. Treatment fidelity was ensured by at least one certified group leader delivering all group sessions, ongoing supervision from accredited Incredible Years trainers, videotaping and reviewing group sessions, and group leaders completing checklists after each group session (see also Menting et al., 2014a; Menting & de Castro, 2021). Checklists were filled out for 185 of the 194 group sessions (95.4%). Overall, group leaders reported that they accomplished 91.0% (SD = 12.9; range = 7.7–100.0) of the activities.
In line with the Incredible Years parent training, participating mothers received the course book (Webster-Stratton, 2007a), handouts, stickers as incentives, and home assignments. Some adjustments for this population were made in line with Incredible Years parent training: more room for discussing additional issues, availability of summaries in simpler language, reward system for maternal engagement, alternatives for buddy calls if necessary, and only capturing group leaders in videotapes of group sessions because of privacy concerns of participants (Menting & de Castro, 2021). To ensure that mothers are able to practice playing with their children, all mothers also received a toy for their children. Furthermore, mothers were assisted to travel from their residence to the location of the group sessions (mostly a community center; a penitentiary institution in the first group), by means of tickets, schedules, and reminders.
Measures
Adolescent delinquency
Adolescent delinquency was assessed using both maternal and self-report from the age of 11. The questionnaire (38 items) was based on the Self-Report of Antisocial Behavior (Loeber et al., 1989). After confidentiality was reassured, participants reported the frequency of 30 delinquent behaviors (1 = never to 5 = more than 10 times), which were dichotomized and summed for analyses—with higher scores reflecting more delinquent behaviors. The internal consistency of this total score was moderate to adequate for 9 out of 11 assessments in the mother report (Cronbach’s α = 0.52 at age 20 to Cronbach’s α = 0.86 at age 17 for these assessments) and 6 out of 10 assessments in self-report (Cronbach’s α = 0.82 at age 16 to Cronbach’s α = 0.96 at age 13 and 17 for these assessments).
Maternal recidivism
Maternal recidivism was based on official criminal records from the Dutch Judicial Information Service of the Ministry of Justice and Security, as requested in 2014, 2016, and 2021. For each of the 224 participating mothers, the original case was identified in these records first; offenses before this original case were defined as previous offenses, whereas offenses after the intervention period were considered recidivism and recorded per year after intervention. Furthermore, to measure the volume of recidivism, the total number of offenses was calculated per participant for the first 5 years after intervention and the first 10 years after intervention—if available for the whole period.
Maternal parenting behavior
The Alabama Parenting Questionnaire (APQ; Shelton et al., 1996; Święcicka et al., 2023) is a self-report questionnaire that measures the most important aspects of parenting behaviors related to disruptive child behavior. Mothers completed the APQ during all assessments, using a 5-point frequency scale (never to always), with higher scores reflecting more frequent use of parenting behavior. Identical to for example Hinshaw and colleagues (Hinshaw et al. 2000), we used three factors assessing parenting behaviors: positive involvement (16 items, e.g., “You praise your child when he/she does something well”); negative/ineffective discipline (11 items, e.g., “You threatened to punish your child an then do not actually punish him/her”); and deficient monitoring (8 items, e.g., “Your child goes out without a set time to be home”). Although reliability and validity of this 3-factor structure were adequate in previous research (Hawes & Dadds, 2006; Hinshaw et al., 2000), we had to remove three items regarding negative/ineffective discipline to optimize the internal consistency of that scale. Therefore, negative/ineffective discipline consisted of eight items in this study. The mean internal consistency was acceptable for the three scales in this study (positive involvement, Cronbach’s α = 0.78; negative/ineffective discipline, Cronbach’s α = 0.62; deficient monitoring, Cronbach’s α = 0.66). Without the data regarding 1 year after intervention (see Analyses), the mean internal consistency was somewhat higher for two out of three scales: α = 0.80 for positive involvement, α = 0.61 for negative/ineffective discipline, and α = 0.70 for deficient monitoring.
Disruptive child behavior
The Eyberg Child Behavior Inventory (ECBI; Eyberg & Pincus, 1999) is a questionnaire designed to measure parental reports of children’s problem behaviors. The ECBI consists of 36 items (e.g., “Sasses adults”) rated on two scales: an intensity scale measuring the intensity or frequency of the problem behavior on a 7-point scale (never to always) and a problem scale that measures the extent to which this behavior is a problem for the parents (yes or no). Mothers completed the ECBI during all assessments. The ECBI’s reliability and validity are good (Abrahamse et al., 2015; Boggs et al., 1990; Rich & Eyberg, 2001), as was the internal consistency in the current study (intensity, M Cronbach’s α = 0.90; problem, M Cronbach’s α = 0.91). At pretest, the mean score on the intensity scale was 103.37 (SD = 31.06; about 50th–75th percentile according to Dutch norm scores [Weeland et al., 2018]) and the mean score on the problem scale 10.07 (SD = 8.25; about 75th–90th percentile according to Dutch norm scores [Weeland et al., 2018]).
Analyses
To examine the potential effect of the intervention on adolescent delinquency, we estimated a mixed effects model using R statistical software. We dichotomized the outcome variable because of a skewed distribution (in 78% of observations no delinquency was reported). As a result, we used logistic regression with family ID and child as cluster variables and gender, age (centered), and time since intervention as control variables. Both condition (0 = no intervention, 1 = intervention) and age × condition interaction were entered as predictors.
To examine the potential effects of the intervention on maternal recidivism, we used Cox regression analyses with intervention (0 = no intervention, 1 = intervention) and three other covariates: maternal age, juvenile delinquency (0 = no, 1 = at least one juvenile offense in official records), and total number of previous offenses (inverse transformation). Kaplan–Meier analyses were used for survival plots. Independent t-tests with bootstrapping (2000 bootstrap samples) were used to test group differences in the volume of recidivism at 5 and 10 years after intervention. These analyses were conducted in SPSS version 24.
To evaluate potential differences in the rates of parenting behaviors and disruptive child behaviors between intervention and non-intervention groups, we used latent linear growth mixture models using the default robust maximum likelihood estimator (ML) with the “knownclasses” and “type = complex” options in Mplus version 8.6 scores. As children were nested within mothers, this method allowed us to account for this clustering by including family ID. A Wald test was used to test between-group differences in slope coefficients. Data collected 1 year after the intervention had to be excluded due to lack of coverage across groups and assessments. Moreover, the high number of missing data pointed the default setting of 10% covariance coverage to a minimum of 2%. Therefore, due to large amounts of missing data and low covariance coverage, care is warranted in generalizing the results.
Results
Participation
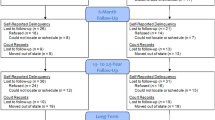
Participants were included in this study from July 2007 to September 2014 in 15 intervention groups. Four of these groups were randomly assigned (see Menting et al., 2014a). The 145 intervention mothers received on average 63.2% (range = 7.1–100.0%; SD = 26.82) of the offered group sessions and 2.45 (SD = 1.77) home visits. For about half of these mothers (50.7%), the intervention started during incarceration. The mean last assessment was 3.65 years after intervention (SD = 3.93; n = 286 children). For the 169 children with long-term follow-up data, this mean last assessment was 6.31 years after intervention (SD = 2.93; 72.2% intervention). For 37 children of 27 mothers, data could be collected up to 10 years after intervention (range 9.51–10.63 years; 62.2% intervention). Figure 1 shows a flow chart outlining sample size and composition. Descriptives per condition are displayed in Table 2, showing group differences in 8 of 22 tests. Only the baseline score regarding negative/ineffective discipline consistently differed between the intervention and no intervention group in both the sample regarding parenting/disruptive child behavior (t(260) = − 2.15, p = 0.03) and the sample regarding adolescent delinquency (t(106) = − 2.25, p = 0.03), with higher scores in the intervention group.

Flow chart participants
Maternal report of adolescent delinquency was available for 116 children (55.2% boys; 74.1% intervention), at ages 11 to 21. On average, for these children, adolescent delinquency data was assessed during 3.03 (SD = 1.77) of the 4.74 (SD = 1.74) possible assessments based on age and follow-up length. In line with the emphasis on intervention mothers in groups after the original study (see procedure), mothers of the included children were more often intervention mothers (χ2(1) = 9.76, p = 0.002) and their children were somewhat older at the start of the intervention than the children that were not included in the analyses (Mincluded = 7.38, Mnot-included = 6.68; t(258) = − 2.20, p = 0.03). However, no differences were found regarding gender and initial severity of disruptive behavior problems. Intervention children were somewhat older than children whose mothers did not receive intervention (Mintervention = 7.64, Mno intervention = 6.60; t(114) = − 2.01, p = 0.047), but groups did not differ regarding gender, initial severity of disruptive behavior problems, age of first adolescent delinquency assessment, age of last adolescent delinquency assessment, and the number of adolescent delinquency assessments. For all ages, except for age 18, delinquent behaviors were reported by mothers, ranging up to eight delinquent behaviors in the past year for a child. Mother report of delinquent behavior correlated positively with adolescent self-report for ages 11 to 14 (r = 0.59 to 0.62), but not for later ages with smaller self-report sample sizes.
Maternal recidivism data was collected for all 224 mothers, with data being available to on average 9.17 years after intervention (SD = 2.80). Data could be collected for the whole observation period in most cases (87.9%). The most common reasons for unavailability were discontinuing (n = 23) and death (n = 2). During the observation period, nearly half of the mothers (46.0%) reoffended, with 10.4% reoffending in the first year after intervention. The total number of re-offenses ranged from 0 to 15 (M = 1.23, SD = 2.17). Independent t-tests revealed no group differences regarding history of delinquency (i.e., juvenile delinquency, adult offenses before the original case, and total number of previous offenses), but the intervention mothers were somewhat older than mothers who did not receive intervention (Mintervention = 33.91, Mno intervention = 30.94; t(191.28) = − 3.64, p < 0.001, equal variances not assumed), and their observation period lasted slightly shorter (Mintervention = 8.83, Mno intervention = 9.77; t(222) = 2.42, p = 0.02).
Effect on adolescent delinquency
A mixed effects model showed that the condition was a significant predictor of mother-reported adolescent delinquency, b = − 0.461, p = 0.04, one-sided, with more beneficial outcomes for the intervention condition (see Fig. 2). Delinquency was reported for 18.9% of the adolescents in the intervention condition compared to 30.6% in the no intervention condition.

Delinquency by age. Note: 0 = no intervention, 1 = intervention
Effect on maternal recidivism
Cox regression analyses revealed a significant effect of intervention on maternal recidivism when controlling for maternal age, juvenile delinquency, and total number of previous offenses, χ2(1) = 4.02, p = 0.02 (one-sided). The hazard ration for intervention (HR = 0.66, 95% CI [0.44, 0.99]) showed that the chance of survival was larger in the intervention group, which means that the chance of recidivism was smaller in the intervention group: 40.69% of the intervention mothers reoffended compared to 55.69% of the mothers who did not receive intervention. The other covariates together also significantly predicted survival (χ2(3) = 21.30, p < 0.001). Figure 3 shows the cumulative proportion of survivors (i.e., mothers without re-offenses) by group. Moreover, independent t-tests with bootstrapping revealed between-group differences regarding the number of re-offenses 5 and 10 years after intervention (5 years, t(207) = 2.07, p = 0.02 (one-sided), d = 0.30; 10 years, t(92.71) = 2.30, p = 0.01 (one-sided), equal variances not assumed, d = 0.42). Both for 5- and 10-year recidivism, fewer re-offenses were reported for the intervention mothers (5 years, M = 0.69, SE = 0.13; 10 years, M = 1.07, SE = 0.22) than for the mothers who did not receive intervention (5 years, M = 1.18, SE = 0.20; 10 years, M = 1.98, SE = 0.34).

Survival plot recidivism (Kaplan–Meier)
Effect on maternal parenting behavior
In latent linear growth mixture models up to 10 years after intervention, no differences in slopes were found regarding parenting behaviors between intervention mothers and mothers who did not receive intervention. For positive involvement, none of the slopes differed from zero (intervention, M = − 0.08, p = 0.45; no intervention, M = 0.31, p = 0.09; Wald = 3.46 (df = 1), p = 0.06). For negative/ineffective discipline, both slopes showed a slight decrease over time (intervention, M = − 0.27, p < 0.001; no intervention, M = − 0.21, p = 0.002), but these slopes did not differ significantly (Wald = 0.68 (df = 1), p = 0.41). For deficient monitoring, a slight increase over time was found in both conditions (intervention, M = 0.33, p < 0.001; no intervention, M = 0.45, p < 0.001), but these slopes did not differ significantly (Wald = 2.05 (df = 1), p = 0.15) (see Fig. 4 for changes per child and condition).

Changes in parenting for individual children and conditions. Note: A Positive involvement. B Negative/ineffective discipline. C Deficient monitoring
Effect on disruptive child behavior
In latent linear growth mixture models, a difference between slopes was found for the number of problems (Wald = 5.52 (df = 1), p = 0.02) but not for the intensity of problems (Wald = 1.47 (df = 1), p = 0.22). The number of problems decreased over time for the children of mothers who had received intervention (M = − 0.44, p < 0.001) but was stable for the children whose mothers did not receive intervention (M = − 0.13, p = 0.20). The intercept also differed between conditions (Wald = 11.81 (df = 1), p < 0.001), with higher initial numbers of problems in the intervention group. The intensity of problems decreased in both conditions intervention, M = − 2.78, p < 0.001; no intervention, M = − 2.18, p < 0.001) (see Fig. 5 for changes per child and condition).

Changes in disruptive child behavior for individual children and conditions. Note: A Intensity of disruptive child behavior. B Number of problems
Discussion
This study aimed to examine the long-term effects (i.e., up to 10 years after intervention) of the preventive Better Start program for families with mothers being released from incarceration. Outcomes favoring the intervention group were found for primary outcomes regarding the intergenerational transmission of delinquency: mother-reported delinquency in adolescents and maternal recidivism based on official records. However, regarding proximal outcomes of parenting intervention (i.e., parenting behaviors and disruptive child behavior), positive results were only found regarding the number of disruptive behavior problems, but not for parenting behaviors and the intensity of disruptive child behavior.
In line with the program’s main intervention goal regarding children affected by maternal incarceration (Menting & de Castro, 2021), children of mothers who participated in the Better Start program showed less delinquent behavior in adolescence than children of mothers who did not receive this preventive intervention. This result is promising and may be considered as the ultimate test of Better Start’s program theory. This study thereby contributes to the relatively scarce literature about the long-term effects of preventive interventions, to the literature on parenting as a mechanism in the intergenerational transmission of delinquency, and to the knowledge of using parenting programs to protect children affected by maternal incarceration from adverse outcomes (Armstrong et al., 2018; Besemer et al., 2017; Murray & Farrington, 2008).
The current findings regarding adolescent delinquency and children’s disruptive behavior problems suggest that an intervention of relatively light intensity may be sufficient to help these families on track. Mothers may use the acquired knowledge and skills after the intervention at least to such an extent that they are able to prevent a relapse of disruptive behavior problems (Van Aar et al., 2017). However, as parental incarceration is known to be associated with poorer child, adolescent, and adult adjustment on a variety of outcomes even when controlling for factors that distinguish these families prior to incarceration (Poehlmann-Tynan & Turney, 2021), broader effects of this intervention should be examined. That is, comparing these children to a control group of children matched on socioeconomic status, for example regarding their school careers and social outcomes, would inform us about the broader developmental effects of this intervention. Notably, comparison to the norm scores revealed that, according to their mothers, this sample initially showed relatively many disruptive behavior problems but did not score very high on internalizing, externalizing, and the overall extent of emotional and behavior problems during long-term assessments (see participants section). This may suggest that, after somewhat elevated levels of disruptive child behaviors, these children’s behaviors were overall not atypical compared to youth of the same gender and similar age, even though higher scores were anticipated because of the children’s at-risk status.
Also in line with the main intervention goals (Menting & de Castro, 2021), our results suggest intervention effects on recidivism: Intervention mothers remained more often crime-free according to official records, and their number of offenses was also smaller—both for 5 and 10 years after intervention—than for mothers who did not receive the intervention. These results add to the literature about motherhood as a motivator to remain crime-free (Rodermond et al., 2016) and suggest that the positive effects of parenting programs on parental recidivism may last longer than the promising results that were already found in previous research (Eddy et al., 2022).
Possibly, the effects on maternal recidivism can be explained by emphasis on modeling and problems solving during the intervention (Menting & de Castro, 2021) as well as spending more time on parenting and feeling more competent as a mother (Adams et al., 2017) after intervention. Successes regarding parenting, awareness of modeling processes, and the wish to provide a better future for their children (Menting et al., 2014b) may not only motivate mothers to desist but might also help them to search for other solutions than criminal activities and encourage this in their children. For example, almost half of the mothers were convicted because of a drug-related offense. Poverty and providing for children are found to be common motivations for women in the drug trade (Fleetwood & Leban, 2023). Awareness of potential negative effects for children, improved skills, feelings of competency, and challenged beliefs may therefore lead to other choices. Being able to work individually with the mothers during home visits may have contributed positively to this.
Although the Better Start parenting intervention seemed to have had long-term effects on disruptive child behavior, adolescent delinquency, and maternal recidivism, no long-term group differences were found for parenting. This result was not in line with our previous studies (Alsem et al., 2021; Menting et al., 2014a), in which effects on inconsistent discipline were found, but seems in line with long-term results of other selective prevention studies, in which initial effects were not sustained (Scott et al., 2014). Besides more methodological explanations (e.g., limited initial effects, regression to the mean, age trends) for not finding sustained differences in the mechanism that we targeted during the intervention, an explanation may be that the intervention also changes mechanisms that were not captured in our measure of parenting behaviors. That is, eventually, the change might be less specific and more related to for example social bonding (Hirschi, 1969). In fact, the idea of optimizing parenting behaviors of mothers being released from incarceration is also based on the idea that this may improve the social bonding of these mothers to others and therefore help to break the vicious circle in the failure model (Hirschi, 2004; Menting & de Castro, 2021), also by teaching the children self-control (Pratt et al., 2011). Alternatively, the intervention targeted the specified mechanism, but this was more difficult to maintain in this at-risk population (Leijten et al., 2013; Tomlinson et al., 2020; Troy et al., 2018).
Although this study contributes to the scarce literature regarding preventive effects of parenting intervention for families affected by maternal incarceration, the study also has a variety of weaknesses. First, we were more dependent on the mother report than we hoped for: We have tried to collect data from other informants as well (see procedure) but were mostly forced to use the mother report because of the small sample sizes for other informants. Fortunately, maternal reports of adolescent delinquency were positively related to self-reports by adolescents (see participation section), whereas mother report of parenting behaviors is known to correspond sufficiently with observation (Hawes & Dadds, 2006; Menting et al., 2013). Nonetheless, especially self-reported delinquency and official records for adolescent delinquency would have been informative as we would assume that this information would be more reliable than mother report only. Second, as may be expected in longitudinal research (Young et al., 2006) in a hard-to-reach and hard-to-retain population (Armstrong et al., 2018; Tremblay & Sutherland, 2017) in which characteristics that are known to be related to dropout tend to cluster (Goshin & Byrne, 2012), we had quite some missing data on a part of the outcome measures. Sometimes this missingness was because of the study design (i.e., opt-out mothers from the groups after the original study were not visited during the long-term follow-up), but mostly due to loss of contact. The smallest sample size can be found in the analyses regarding adolescent delinquency, and therefore, these results should be interpreted with more caution. However, for this sample pretest analyses did not suggest that the study was affected by selective dropout. Nonetheless, in future research, especially a larger no intervention group that consists of mothers who did not opt out themselves would be desirable. A larger control group would also allow for intention-to-treat analyses, which we could not conduct in the current study because of power issues.
The current findings, in combination with findings from our previous studies (Alsem et al., 2021; Menting et al., 2014a), suggest that an evidence-based parenting intervention adjusted to the population of mothers being released from incarceration does have a long-term positive impact on families affected by maternal incarceration. This represents a significant societal benefit. The Better Start program may indeed contribute to the prevention of the intergenerational transmission of delinquency. This seems especially relevant given the high societal costs—besides personal suffering—of criminal careers and concentration of offending in families (Beaver, 2013; Farrington et al., 1996). Notably, these results have been found in the Netherlands—a country with one of the lowest imprisonment rates in Europe, but medium incarceration rates for females (Aebi & Tiago, 2021), a relatively mild penal climate (Subramanian & Shames, 2014), and high prevalence of relatively short sentences (Aebi & Tiago, 2021; Subramanian & Shames, 2014). The generalizability of the results regarding families affected by maternal incarceration in other countries with other penal systems and climates is therefore still unknown. Nonetheless, the current results call for the wider use of effective interventions in vulnerable families that are hard to reach. If these positive ultimate results on delinquency and recidivism are possible for this parenting intervention, it should be feasible to achieve such outcomes in other at-risk populations as well.
Data availability
The datasets analyzed during the current study are not publicly available due to legally binding agreements with the Ministry of Justice and Security but are available from the corresponding author on reasonable request.
References
Abrahamse, M. E., Junger, M., Leijten, P. H. O., Lindeboom, R., Boer, F., & Lindauer, R. J. L. (2015). Psychometric properties of the Dutch Eyberg Child Behavior Inventory (ECBI) in a community sample and a multi-ethnic clinical sample. Journal of Psychopathology and Behavioral Assessment, 37, 679–691. https://doi.org/10.1007/s10862-015-9482-1
Achenbach, T. M., & Rescorla, L. A. (2000). Manual for the ASEBA preschool forms & profiles. University of Vermont, Research Center for Children, Youth, & Families.
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA school-age forms & profiles. University of Vermont, Research Center for Children, Youth, & Families.
Achenbach, T. M., & Rescorla, L. A. (2003). Manual for the ASEBA adult forms & profiles. University of Vermont, Research Center for Children, Youth, & Families.
Adams, E. A., Morash, M., Smith, S. W., & Cobbina, J. E. (2017). Women’s experience of motherhood, violations of supervision requirements and arrests. British Journal of Criminology, 57(6), 1420–1441. https://doi.org/10.1093/bjc/azw092
Aebi, M. F., & Tiago, M. M. (2021). Space I-2020-Council of Europe Annual Penal Statistics: Prison populations (Issue April). https://wp.unil.ch/space/files/2021/04/210330_FinalReport_SPACE_I_2020.pdf. Accessed 25 Oct 2023
Alsem, S. C., Menting, A. T. A., de Castro, B. O., & Matthys, W. (2021). Follow-up effects in a parent-training trial for mothers being released from incarceration and their children. Psychology Public Policy and Law, 27(3), 421–431. https://doi.org/10.1037/law0000305
Arditti, J. A., & Few, A. (2008). Maternal distress and women’s reentry into family and community life. Family Process, 47(3), 303–321. https://doi.org/10.1111/j.1545-5300.2008.00255.x
Armstrong, E., Eggins, E., Reid, N., Harnett, P., & Dawe, S. (2018). Parenting interventions for incarcerated parents to improve parenting knowledge and skills, parent well-being, and quality of the parent–child relationship: A systematic review and meta-analysis. Journal of Experimental Criminology, 14, 279–317. https://doi.org/10.1007/s11292-017-9290-6
Asscher, J. J., Deković, M., Manders, W. A., Van der Laan, P. H., Prins, P. J. M., Van Arum, S., Dutch MST Cost-Effectiveness Group. (2014). Sustainability of the effects of multisystemic therapy for juvenile delinquents in the Netherlands: Effects on delinquency and recidivism. Journal of Experimental Criminology, 10(2), 227–243. https://doi.org/10.1007/s11292-013-9198-8
Beaver, K. M. (2013). The familial concentration and transmission of crime. Criminal Justice and Behavior, 40(2), 139–155. https://doi.org/10.1177/0093854812449405
Begun, A. L., Hodge, A. I., & Early, T. J. (2017). A family systems perspective in prisoner reentry. In S. Stojkovic (Ed.), Prisoner reentry: Critical issues and policy directions (pp. 85–144). Palgrave Macmillan.
Besemer, S., Axelsson, J., & Sarnecki, J. (2016). Intergenerational transmission of trajectories of offending over three generations. Journal of Developmental and Life-Course Criminology, 2(4), 417–441. https://doi.org/10.1007/s40865-016-0037-2
Besemer, S., Ahmad, S. I., Hinshaw, S. P., & Farrington, D. P. (2017). A systematic review and meta-analysis of the intergenerational transmission of criminal behavior. Aggression and Violent Behavior, 37, 161–178. https://doi.org/10.1016/j.avb.2017.10.004
Boggs, S. R., Eyberg, S. M., & Reynolds, L. A. (1990). Concurrent validity of the Eyberg Child Behavior Inventory. Journal of Clinical Child Psychology, 19(1), 75–78. https://doi.org/10.1207/s15374424jccp1901_9
Broidy, L. M., Nagin, D. S., Tremblay, R. E., Bates, J. E., Brame, B., Dodge, K. A., Fergusson, D., Horwood, J. L., Loeber, R., Laird, R., Lynam, D. R., Moffitt, T. E., Pettit, G. S., & Vitaro, F. (2003). Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: A six-site, cross-national study. Developmental Psychology, 39(2), 222–245. https://doi.org/10.1037/0012-1649.39.2.222
Brotman, L. M., Gouley, K. K., Huang, K., Rosenfelt, A., Neal, C. O., Klein, R. G., & Shrout, P. (2008). Preventive intervention for preschoolers at high risk for antisocial behavior: Long-term effects on child physical aggression and parenting practices. Journal of Clinical Child & Adolescent Psychology, 37(2), 386–396. https://doi.org/10.1080/15374410801955813
Burraston, B. O., & Eddy, J. M. (2017). The moderating effect of living with a child before incarceration on postrelease outcomes related to a prison-based parent management training program. Smith College Studies in Social Work, 87(1), 94–111. https://doi.org/10.1080/00377317.2017.1248634
Byrne, M. W. (2005). Conducting research as a visiting scientist in a women’s prison. Journal of Professional Nursing, 21(4), 223–230. https://doi.org/10.1016/j.profnurs.2005.05.001
Clark, M. G., Metcalfe, R. E., Caffery, C. M., Conn, A. D., & Kjellstrand, J. M. (2023). Parenting through re-entry: Ecologically-grounded perspectives of parents returning to the community after incarceration. Journal of Child and Family Studies, 32, 2465–2481. https://doi.org/10.1007/s10826-023-02621-0
Comer, J. S., Chow, C., Chan, P. T., Cooper-Vince, C., & Wilson, L. A. S. (2013). Psychosocial treatment efficacy for disruptive behavior problems in very young children: A meta-analytic examination. Journal of the American Academy of Child and Adolescent Psychiatry, 52(1), 26–36. https://doi.org/10.1016/j.jaac.2012.10.001
Dallaire, D. H. (2007). Children with incarcerated mothers: Developmental outcomes, special challenges and recommendations. Journal of Applied Developmental Psychology, 28(1), 15–24. https://doi.org/10.1016/j.appdev.2006.10.003
de Vries, S. L. A., Hoeve, M., Asscher, J. J., & Stams, G. J. J. M. (2018). The long-term effects of the youth crime prevention program “New Perspectives” on delinquency and recidivism. International Journal of Offender Therapy and Comparative Criminology, 62(12), 3639–3661. https://doi.org/10.1177/0306624X17751161
Deković, M., Slagt, M. I., Asscher, J. J., Boendermaker, L., Eichelsheim, V. I., & Prinzie, P. (2011). Effects of early prevention programs on adult criminal offending: A meta-analysis. Clinical Psychology Review, 31(4), 532–544. https://doi.org/10.1016/j.cpr.2010.12.003
Eddy, B. A., Powell, M. J., Szubka, M. H., McCool, M. L., & Kuntz, S. (2001). Challenges in research with incarcerated parents and importance in violence prevention. American Journal of Preventive Medicine, 20(1, Supplement 1), 56–62. https://doi.org/10.1016/S0749-3797(00)00273-7
Eddy, J. M., Martinez, C. R., Burraston, B., Herrera, D., & Newton, R. M. (2022). A randomized controlled trial of a parent management training program for incarcerated parents: Post-release outcomes. International Journal of Environmental Research and Public Health, 19, 4605. https://doi.org/10.3390/ijerph19084605
Eyberg, S. M., & Pincus, D. (1999). Eyberg Child Behavior Inventory & Sutter-Eyberg Student Behavior Inventory-Revised. Psychological Assessment Resources.
Farrington, D. P., Barnes, G. C., & Lambert, S. (1996). The concentration of offending in families. Legal and Criminological Psychology, 1, 47–63. https://doi.org/10.1111/j.2044-8333.1996.tb00306.x
Fleetwood, J., & Leban, L. (2023). Women’s involvement in the drug trade: Revisiting the emancipation thesis in global perspective. Deviant Behavior, 44(2), 238–258. https://doi.org/10.1080/01639625.2022.2033607
Giordano, P. C., Copp, J. E., Manning, W. D., & Longmore, M. A. (2019). Linking parental incarceration and family dynamics associated with intergenerational transmission: A life-course perspective. Criminology, 57(3), 395–423. https://doi.org/10.1111/1745-9125.12209
Goshin, L. S., & Byrne, M. W. (2012). Predictors of post-release research retention and subsequent reenrollment for women recruited while incarcerated. Research in Nursing and Health, 35(1), 94–104. https://doi.org/10.1002/nur.21451
Gross, D., Fogg, L., Webster-Stratton, C., Garvey, C., Julion, W., & Grady, J. (2003). Parent training of toddlers in day care in low-income urban communities. Journal of Consulting and Clinical Psychology, 71(2), 261–278. https://doi.org/10.1037/0022-006X.71.2.261
Hawes, D. J., & Dadds, M. R. (2006). Assessing parenting practices through parent-report and direct observation during parent-training. Journal of Child and Family Studies, 15(5), 554–567. https://doi.org/10.1007/s10826-006-9029-x
Heckman, J. J. (2006). Skill formation and the economics of investing in disadvantaged children. Science, 312(5782), 1900–1902. https://doi.org/10.1126/science.1128898
Hinshaw, S. P., Owens, E. B., Wells, K. C., Kraemer, H. C., Abikoff, H. B., Arnold, L. E., Conners, C. K., Elliott, G., Greenhill, L. L., Hechtman, L., Hoza, B., Jensen, P. S., March, J. S., Newcorn, J. H., Pelham, W. E., Swanson, J. M., Vitiello, B., & Wigal, T. (2000). Family processes and treatment outcome in the MTA: Negative/ineffective parenting practices in relation to multimodal treatment. Journal of Abnormal Child Psychology, 28(6), 555–568. https://doi.org/10.1023/A:1005183115230
Hirschi, T. (1969). Causes of delinquency. University of California Press.
Hirschi, T. (2004). Self-control and crime. In R. F. Baumeister & K. D. Vohs (Eds.), Handbook of self-regulation: Research, theory, and applications (pp. 537–552). Guilford.
Hoeve, M., Dubas, J. S., Eichelsheim, V. I., Van der Laan, P. H., Smeenk, W., & Gerris, J. R. M. (2009). The relationship between parenting and delinquency: A meta-analysis. Journal of Abnormal Child Psychology, 37(6), 749–775. https://doi.org/10.1007/s10802-009-9310-8
Junger, M., Greene, J., Schipper, R., Hesper, F., & Estourgie, V. (2013). Parental criminality, family violence and intergenerational transmission of crime within a birth cohort. European Journal on Criminal Policy and Research, 19(2), 117–133. https://doi.org/10.1007/s10610-012-9193-z
Kaminski, J. W., & Claussen, A. H. (2017). Evidence base update for psychosocial treatments for disruptive behaviors in children. Journal of Clinical Child & Adolescent Psychology, 46(4), 477–499. https://doi.org/10.1080/15374416.2017.1310044
Kim, E., Cain, K. C., & Webster-Stratton, C. (2008). The preliminary effect of a parenting program for Korean American mothers: A randomized controlled experimental study. International Journal of Nursing Studies, 45, 1261–1273. https://doi.org/10.1016/j.ijnurstu.2007.10.002
Krysik, J., & Rodriquez, N. (Eds.). (2022). Children of incarcerated parents: Integrating research into best practices and policy. Springer. https://doi.org/10.1007/978-3-030-84713-5
Lacourse, E., Côté, S., Nagin, D. S., Vitaro, F., Brendgen, M., & Tremblay, R. E. (2002). A longitudinal-experimental approach to testing theories of antisocial behavior development. Development and Psychopathology, 14(04), 909–924. https://doi.org/10.1017/S0954579402004121
Landenberger, N. A., & Lipsey, M. W. (2005). The positive effects of cognitive-behavioral programs for offenders: A meta-analysis of factors associated with effective treatment. Journal of Experimental Criminology, 1(4), 451–476. https://doi.org/10.1007/s11292-005-3541-7
Leclair Mallette, I. A., Letarte, M. J., Hélie, S., Sicotte, R., & Temcheff, C. E. (2021). Is the Incredible Years parenting programme predictive of case closure in child protection services for neglect? A quasi-experimental study. Child and Family Social Work, 26(4), 687–695. https://doi.org/10.1111/cfs.12849
Leijten, P. H. O., Raaijmakers, M. A. J., de Castro, B. O., & Matthys, W. (2013). Does socioeconomic status matter? A meta-analysis on parent training effectiveness for disruptive child behavior. Journal of Clinical Child and Adolescent Psychology, 42(3), 384–392. https://doi.org/10.1080/15374416.2013.769169
Loeber, R., Stouthamer-Loeber, M., Kammen, W. B., & Farrington, D. P. (1989). Self-Report of Antisocial Behavior. Pittsburgh University.
Loper, A. B., & Tuerk, E. H. (2006). Parenting programs for incarcerated parents: Current research and future directions. Criminal Justice Policy Review, 17(4), 407–427. https://doi.org/10.1177/0887403406292692
McCart, M. R., Priester, P. E., Davies, W. H., & Azen, R. (2006). Differential effectiveness of behavioral parent-training and cognitive-behavioral therapy for antisocial youth: A meta-analysis. Journal of Abnormal Child Psychology, 34(4), 527–543. https://doi.org/10.1007/s10802-006-9031-1
Menting, A. T. A., & de Castro, B. O. (2021). Databank Effectieve Jeugdinterventies: Beschrijving “Betere Start.” [Database effective youth interventions: Description Better Start]. https://www.nji.nl/interventies/betere-start
Menting, A. T. A., de Castro, B. O., & Matthys, W. (2013). Effectiveness of the Incredible Years parent training to modify disruptive and prosocial child behavior: A meta-analytic review. Clinical Psychology Review, 33(8), 901–913. https://doi.org/10.1016/j.cpr.2013.07.006
Menting, A. T. A., de Castro, B. O., Wijngaards-de Meij, L. D. N. V., & Matthys, W. (2014a). A trial of parent training for mothers being released from incarceration and their children. Journal of Clinical Child and Adolescent Psychology, 43(3), 381–396. https://doi.org/10.1080/15374416.2013.817310
Menting, A. T. A., de Castro, B. O., & Matthys, W. (2014b). Engagement in parent training for mothers being released from incarceration [Paper presentation]. 22nd Annual Meeting of the Society for Prevention Research, Washington DC, United States.
Menting, A. T. A., de Castro, B. O., & Matthys, W. (2017). Arrested motherhood: Parenting, cognitive distortions, and depressive symptoms in mothers being released from incarceration. Parenting: Science and Practice, 17(3), 177–186. https://doi.org/10.1080/15295192.2017.1333317
Moffitt, T. E. (2018). Male antisocial behaviour in adolescence and beyond. Nature Human Behaviour, 2(3), 177–186. https://doi.org/10.1038/s41562-018-0309-4
Murray, J., & Farrington, D. P. (2008). The effects of parental imprisonment on children. Crime and Justice, 37(1), 133–206. https://doi.org/10.1086/520070
Murray, J., Farrington, D. P., & Sekol, I. (2012). Children’s antisocial behavior, mental health, drug use, and educational performance after parental incarceration: A systematic review and meta-analysis. Psychological Bulletin, 138(2), 175–210. https://doi.org/10.1037/a0026407
Patterson, G. R. (2016). Coercion theory: The study of change. In T. J. Dishion & J. J. Snyder (Eds.), The Oxford handbook of coercive relationship dynamics (pp. 7–22). Oxford University Press.
Pearson, F. S., Lipton, D. S., Cleland, C. M., & Yee, D. S. (2002). The effects of behavioral/cognitive-behavioral programs on recidivism. Crime and Delinquency, 48(3), 476–496. https://doi.org/10.1177/001112870204800306
Phillips, S. D., Burns, B. J., Wagner, H. R., & Barth, R. P. (2004). Parental arrest and children involved with child welfare agencies. American Journal of Orthopsychiatry, 74(2), 174–186. https://doi.org/10.1037/0002-9432.74.2.174
Piquero, A. R., Jennings, W. G., Farrington, D. P., Diamond, B., & Gonzalez, J. M. R. (2016). A meta-analysis update on the effectiveness of early self-control improvement programs to improve self-control and reduce delinquency. Journal of Experimental Criminology, 12(2), 249–264. https://doi.org/10.1007/s11292-016-9257-z
Piquero, A. R., Farrington, D. P., Welsh, B. C., Tremblay, R., & Jennings, W. G. (2008). Effects of early family/parent training programs on antisocial behavior and delinquency. In Campbell Systematic Reviews (Vol. 11). https://doi.org/10.4073/csr.2008.11
Poehlmann-Tynan, J., & Turney, K. (2021). A developmental perspective on children with incarcerated parents. Child Development Perspectives, 15(1), 3–11. https://doi.org/10.1111/cdep.12392
Pratt, T. C., Gau, J. M., & Franklin, T. W. (2011). Key idea: Hirschi’s social bond/social control theory. In Key Ideas in Criminology and Criminal Justice (pp. 55–69). https://doi.org/10.4135/9781483388045
Rich, B. A., & Eyberg, S. M. (2001). Accuracy of assessment: The discriminative and predictive power of the Eyberg Child Behavior Inventory. Ambulatory Child Health, 7(3–4), 249–257. https://doi.org/10.1046/j.1467-0658.2001.00141.x
Rodermond, E., Kruttschnitt, C., Slotboom, A. M., & Bijleveld, C. C. J. H. (2016). Female desistance: A review of the literature. European Journal of Criminology, 13(1), 3–28. https://doi.org/10.1177/1477370815597251
Scott, S., Briskman, J., & O’Connor, T. G. (2014). Early prevention of antisocial personality: Long-term follow-up of two randomized controlled trials comparing indicated and selective approaches. American Journal of Psychiatry, 171(6), 649–657. https://doi.org/10.1176/appi.ajp.2014.13050697
Shaw, D. S., Lacourse, E., & Nagin, D. S. (2005). Developmental trajectories of conduct problems and hyperactivity from ages 2 to 10. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 46(9), 931–942. https://doi.org/10.1111/j.1469-7610.2004.00390.x
Shelton, K., Frick, P. J., & Wootton, J. (1996). Assessment of parenting practices in families of elementary school-age children. Journal of Clinical Child Psychology, 25(3), 317–329. https://doi.org/10.1207/s15374424jccp2503_8
Subramanian, R., & Shames, A. (2014). Sentencing and prison practices in Germany and the Netherlands. Federal Sentencing Reporter, 27(1), 33–45. https://doi.org/10.1525/fsr.2014.27.1.33
Święcicka, M., Woźniak-Prus, M., Gambin, M., & Stolarski, M. (2023). Confirmation of the five-factor structure of the Parent Global Report version of the Alabama Parenting Questionnaire in a Polish community sample. Current Psychology, 42(19), 15945–15957. https://doi.org/10.1007/s12144-019-00340-8
Thornberry, T. P., Freeman-Gallant, A., Lizotte, A. J., Krohn, M. D., & Smith, C. A. (2003). Linked lives: The intergenerational transmission of antisocial behavior. Journal of Abnormal Child Psychology, 31(2), 171–184. https://doi.org/10.1023/A:1022574208366
Tomlinson, M., Fearon, P., Christodoulou, J., & Rotheram-Borus, M. J. (2020). Editorial perspective: Stop describing and start fixing–The promise of longitudinal intervention cohorts. Journal of Child Psychology and Psychiatry and Allied Disciplines, 61(12), 1388–1390. https://doi.org/10.1111/jcpp.13213
Tremblay, M. D., & Sutherland, J. E. (2017). The effectiveness of parenting programs for incarcerated mothers: A systematic review. Journal of Child and Family Studies, 26, 3247–3265. https://doi.org/10.1007/s10826-017-0900-8
Troy, V., McPherson, K. E., Emslie, C., & Gilchrist, E. (2018). The feasibility, appropriateness, meaningfulness, and effectiveness of parenting and family support programs delivered in the criminal justice system: A systematic review. Journal of Child and Family Studies, 27(6), 1732–1747. https://doi.org/10.1007/s10826-018-1034-3
United Nations Office on Drugs and Crime (UNODC). (2018). Introductory handbook on the prevention of recidivism and the social reintegration of offenders. Criminal Justice Series. United Nations. https://www.unodc.org/documents/justice-and-prison-reform/crimeprevention/Introductory_Handbook_on_the_Prevention_of_Recidivism_and_the_Social_Reintegration_of_Offenders.pdf
Van Aar, J., Leijten, P. H. O., de Castro, B. O., & Overbeek, G. (2017). Sustained, fade-out or sleeper effects? A systematic review and meta-analysis of parenting interventions for disruptive child behavior. Clinical Psychology Review, 51, 153–163. https://doi.org/10.1016/j.cpr.2016.11.006
Van der Rakt, M., Ruiter, S., De Graaf, N. D., & Nieuwbeerta, P. (2010). When does the apple fall from the tree? Static versus dynamic theories predicting intergenerational transmission of convictions. Journal of Quantitative Criminology, 26, 371–389. https://doi.org/10.1007/s10940-009-9089-3
Verweij, S., Wartna, B. S. J., Tollenaar, N., & Beerthuizen, M. G. C. J. (2017). The effectiveness of a cognitive skills training program for adult offenders. Criminal Justice and Behavior, 44(12), 1559–1579. https://doi.org/10.1177/0093854817737338
Wachs, T. D., Georgieff, M., Cusick, S., & Mcewen, B. S. (2014). Issues in the timing of integrated early interventions: Contributions from nutrition, neuroscience, and psychological research. Annals of the New York Academy of Sciences, 1308(1), 89–106. https://doi.org/10.1111/nyas.12314
Webster-Stratton, C. (1998). Preventing conduct problems in Head Start children: Strengthening parenting competencies. Journal of Consulting and Clinical Psychology, 66(5), 715–730.
Webster-Stratton, C. (2001). The Incredible Years: Parents and children videotape series: A parenting course (BASIC). Incredible Years.
Webster-Stratton, C. (2002). The Incredible Years: Parent and children videotape series: A parenting course (ADVANCE). Incredible Years.
Webster-Stratton, C. (2007a). Pittige jaren: Praktische gids bij het opvoeden van jonge kinderen [The Incredible Years-A troubleshooting guide for parents of children aged 3–8 years]. Bohn Stafleu van Loghum.
Webster-Stratton, C. (2007b). Tailoring the Incredible Years parent programs according to children’s developmental needs and family risk factors. In J. M. Briesmeister & C. E. Schaefer (Eds.), Handbook of parent training (pp. 305–344). Wiley.
Weeland, J., Van Aar, J., & Overbeek, G. (2018). Dutch norms for the Eyberg Child Behavior Inventory: Comparisons with other Western countries. Journal of Psychopathology and Behavioral Assessment, 40(2), 224–234. https://doi.org/10.1007/s10862-017-9639-1
Weisburd, D., Farrington, D. P., & Gill, C. (Eds.). (2016). What works in crime prevention and rehabilitation: Lessons from systematic reviews. Springer.
Wildeman, C. (2020). The intergenerational transmission of criminal justice contact. Annual Review of Criminology, 3(1), 217–244. https://doi.org/10.1146/annurev-criminol-011419-041519
Young, A. F., Powers, J. R., & Bell, S. L. (2006). Attrition in longitudinal studies: Who do you lose? Australian and New Zealand Journal of Public Health, 30(4), 353–361. https://doi.org/10.1111/j.1467-842X.2006.tb00849.x
Acknowledgements
We gratefully acknowledge the families, practitioners, and researchers who participated in this study.
Funding
The original research project is funded by the Dutch Ministry of Justice and Security, Directorate-General for Sentences and Protection.
Author information
Authors and Affiliations
Contributions
A. T. A. M., B. O. d. C., and W. M. contributed to the study conception and design. Material preparation and data collection were performed by A. T. A. M. and B. O. d. C. Analyses were performed by A. T. A. M., B. M. G., and J. J. A. D. The first draft of the manuscript was written by A. T. A. M., and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Utrecht University Faculty of Social and Behavioral Sciences (#20–590). Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Menting, A.T.A., de Castro, B.O., Grandfield, E.M. et al. Better start to better future? Long-term follow-up of a parenting intervention for mothers being released from incarceration. J Exp Criminol (2024). https://doi.org/10.1007/s11292-024-09612-1
Accepted:
Published:
DOI: https://doi.org/10.1007/s11292-024-09612-1