
Abstract
Objectives
This study aimed to investigate the distribution patterns and research frontiers of international literature and thus present a holistic bibliometric evaluation of the studies on IgA nephropathy.
Methods
The Web of Science Core Collection database was searched for studies of IgA nephropathy from January 2012 to March 2023. The keywords and references are analyzed by CiteSpace, while the countries and institutions are analyzed by VOSviewer.
Results
A total of 2987 publications on IgA nephropathy were included. The country with the most publications was China (n = 1299), and the institution with the most publications was Peking University (n = 139). The most frequent keywords were IgA nephropathy (n = 2013), Oxford classification (n = 482), and diseases (n = 433). The keywords that continue to burst out at high intensity are multicenter study and gut microbiota. Moreover, the top five references for burst strength were also listed.
Conclusions
IgA nephropathy has attracted widespread research interest, particularly in high-prevalence areas. From 2012 to 2023, publications on IgA nephropathy show a linear increase. China is the country with the highest number of publications and Peking University is the institution with the highest number of publications. Current research hotspots and frontiers are mainly multicenter studies related to IgA nephropathy and its exploration with gut microbiota. Overall, we have provided a comprehensive scientometric analysis of IgA nephropathy that will inform researchers and healthcare practitioners.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
IgA nephropathy (IgAN) is a primary glomerulonephritis characterized by diffuse deposition of IgA or IgA-dominant immunoglobulins in the glomerular mesangial region. IgAN is found in approximately one-third of all primary glomerulonephritis cases worldwide [1]. The clinical presentation of patients with IgAN is highly heterogeneous, and hypertension, hyperproteinuria, hyperlipidemia, and low estimated glomerular filtration rate are reported as independent risk factors for disease progression [2, 3]. Presently, the more recognized pathogenesis of IgAN is the ‘four hits’ theory: the first hit is the production of galactose-deficient IgA1 (Gd-IgA1). The second hit is the production of specific antibodies against Gd-IgA1 in the bloodstream. The third hit is the formation of pathogenic immune complexes that contain Gd-IgA1, and the fourth hit is the deposition of pathogenic immune complexes in the glomerular mesangial region, which causes kidney injury [4].
The Kidney Disease: Improving Global Outcomes Glomerular Diseases Work Group recommends that management of IgAN patients consists of optimizing supportive therapy (with the maximum tolerated doses of angiotensin-converting enzyme inhibitors or angiotensin-receptor blockers), cardiovascular risk assessment, blood pressure management, and lifestyle interventions [5]. Some special IgAN patients, like those with IgA deposition with minimal changes disease, IgAN with acute kidney injury, or IgAN with rapidly progressive glomerulonephritis, have more complicated treatment plans that are often based on the patient’s other health problems and overall situation [5]. Despite the development of new drugs targeting IgAN over recent years, such as Atrasentan, Iptacopan, and Nefecon, specific treatments for IgAN remain scarce and clinical management of patients with confirmed diagnoses remains difficult. In addition, the number of IgAN patients who develop the end-stage renal disease cannot be understated. As the disease worsens, patients have to pay more for treatments like dialysis or kidney transplantation and have a higher risk of dying. Driven by these concerns, many IgAN studies have been published and attracted widespread attention. However, the dramatic increase in publications has made it increasingly difficult for researchers to keep up with research trends and frontiers. Although meta-analyses and reviews can provide researchers with summaries and can save them a lot of time and effort in extracting information from the overwhelming amount of literature, these papers are often not dimensional enough in their assessment of the progress of research.
Bibliometrics was established as an independent discipline in 1969 [6], which provided a quantitative and long-term method for evaluating research advancement [7,8,9]. Hitherto, there has been an extreme lack of bibliometric reporting on IgAN. The present study aims to analyze the current status and hotspots of IgAN research through bibliometric analysis to provide a reference for medical practitioners and researchers.
Methods
Data source
The Web of Science Core Collection (WOSCC) is one of the most comprehensive and authoritative database platforms for accessing global academic information and is also considered the most suitable database for bibliometric analysis [10,11,12]. Here, we conducted a search and literature extraction through WOSCC and further information is shown in Table 1.
Search strategy
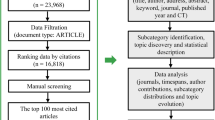
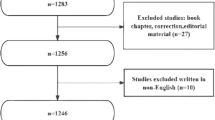
The finalized and integrated retrieval strategy in this paper is [TS = (“IgA nephropathy”) OR TS = (“IgA glomerulonephritis”) OR TS = (“Immunoglobulin A nephropathy”) OR TS = (“IgAN”) OR TS = (“IgA nephritis”) OR TS = (“Berger’s disease”)]. The time is from January 2012 to March 2023, and all searches and data exports were performed on March 4, 2022, to minimize bias due to database updates. After screening and checking for duplicates using CiteSpace, 2987 documents remained. Figure 1A shows how the process went.

Publications screening flowchart and the annual output of IgAN research from 2012–2023
Bibliometric analysis
The most commonly used software for bibliometric analysis is VOSviewer and CiteSpace, which can be complementary.
VOSviewer, developed by Prof. Van Eck and Prof. Waltman, utilizes a probabilistic-based approach to data normalization and features multiple visualizations [13], which are essential tools for researchers to create knowledge maps, evaluate the latest research progress, and identify hotspots [14]. Prof. Chaomei Chen developed CiteSpace, which is based on a set-theoretic approach to data normalization and thus tests the similarity of knowledge units and shows the knowledge evolution in multiple dimensions [15]. Here, the keywords and references were analyzed by CiteSpace 6.1.R6, while VOSviewer 1.6.18 analyzed countries and institutions.
In the network visualization drawn by VOSviewer, the size of the circles indicates the frequency of the elements; the connecting lines indicate the cooperative network, with thicker lines indicating closer cooperation or cross-linking. As a result, network visualization has a unique advantage in analyzing cooperative relationships. In contrast, density visualization uses colors to represent element frequencies, with higher frequencies indicating redder elements. Density visualization is therefore more intuitive when comparing element frequencies.
CiteSpace, on the other hand, has an advantage in evaluating clusters, as reflected in the modularity (Q-score) and silhouette (S-score). The Q-score and S-score indicate the degree to which the network is clustered and the degree to which the data within clusters co-ordinate, respectively. If the Q-score is greater than 0.3 and the S-score is greater than 0.7, this indicates that the clustering is adequate and reliable [16].
Statistics
We have mainly statistics on publications, countries, institutions, keywords and references; other specific research elements are presented in the corresponding tables. Categorical data are expressed as frequencies. All analyses were processed through Word Processing System.
Results
Publication trends
Figure 1B shows the annual and cumulative distribution of IgAN publications from 2012 to 2023. However, 2023 is only counted for 3 months and is not included in the relevant calculations here. It can be seen that the annual publications of IgAN increased steadily from 2012 to 2018. From 2020 to 2022, the annual publications were more than 300, accounting for 10.14%, 12.19% and 12.52% of the total, respectively. In contrast, there is a decrease in annual publications in 2019, which may be related to the COVID-19 outbreak. Finally, the trendline shows a linear trend of increase in cumulative publications from 2012 to 2022 (R2 = 0.9915), suggesting that IgAN has good research sustainability.
Countries
A total of 77 countries have contributed to IgAN publications, of which 73 have collaborative relationships. The network visualization and density visualization, as shown in Fig. 2A–D. The top ten countries in terms of publications are shown in Table 2, with the top three being China (n = 1299), Japan (n = 524), and the USA (n = 409). In terms of average citations per publication, the top three are France (n = 74.57), Germany (n = 66.35), and Turkey (n = 60.08).

A, B The network/density visualization of all 77 countries. C, D The network/density visualization of 73 countries with collaborative relationships. Green circles indicate countries with no cooperation. The visualization to the right of the arrow is a further presentation of the counterpart on the left
Institutions
A total of 3324 institutions have contributed to IgAN publications. 2929 of these have collaborative relationships. The network and density visualization in Fig. 3 shows that institutions without collaborations are scattered like a dial outside the circles in Fig. 3A, B. Seven Chinese institutions were among the top ten institutions in terms of the number of publications, and the top three were Peking University (n = 139), Sun Yat-sen University (n = 97), and Juntendo University (n = 90) (Table 3). In terms of average citations per publication, the top three were the University of Alabama at Birmingham (n = 43.92), Juntendo University (n = 32.89), and Nanjing University (n = 32.02) (Table 3).

A, B The network/density visualization of all 3324 institutions. C, D The network/density visualization of 2929 institutions with collaborative relationships. The majority of institutions without collaborative relationships are outside the circles in A and B. The visualization to the right of the arrow is a further presentation of the counterpart on the left
Keywords
After merging synonyms and removing nonsense words, 604 keyword nodes and 5962 connected lines were presented in the network with a density of 0.0327, as shown in Fig. 4A. All nodes are presented in a tree ring, with colors indicating the time of appearance. Nodes that co-occurred more than 50 times were given labels, with the three most common being IgA nephropathy (n = 2013), Oxford classification (n = 482) and diseases (n = 433).

A Keyword visualization. B Keyword timeline visualization
The clustering results for the keyword network are shown in the Supplementary Material 1, where the Q-score is 0.3538 and the S-score is 0.74, indicating reliable results. 604 keywords were distributed in 5 clusters, #0 Injury, #1 Glomerulonephritis, #2 Proteinuria, #3 Genome-wide association, and #4 Gene polymorphism. The keyword timeline visualization, which reflects the evolutionary trajectory of the study, is shown in Fig. 4B, with cluster #0 Injury, cluster #2 Proteinuria and cluster #3 Genome-wide association running through the entire timeline. As can be seen, the high-frequency keywords tend to appear from the very beginning, around the year 2012. Of course, there are also some keywords that have appeared more recently, such as gut microbiota, machine learning, and COVID-vaccination.
The top 5 keywords in terms of burst strength are presented in Fig. 5, with the top three being multicenter study (strength = 8.89), gut microbiota (strength = 8.16), and diabetic nephropathy (strength = 6.9), while the keywords that consistently burst into 2023 are multicenter study (2020–2023) and gut microbiota (2021–2023).

The top five keywords with the strongest citation bursts
References
The selected IgAN publications cite more than 40,000 references. Figure 6 shows the first author, the publication year, the publication journal, the DOI and the outbreak period for the top 5 references in terms of burst intensity, and Table 4 adds the publication types and the primary research work for these references. The most bursty reference is Oxford Classification of IgA nephropathy 2016: an update from the IgA Nephropathy Classification Working Group (Review, PMID: 28341274, strength = 56.1), and it is also the reference where the bursting continued until recently.

The top five references with the strongest citation bursts
Discussion
Analysis of countries and institutions
Although IgAN was first described by French physicians Jean Berger and Nicole Hinglais [17], it can be seen that there are not as many publications on IgAN in France as expected (ranked ninth), which may be because the pathogenesis of IgAN, the ‘four hits’ theory, was proposed by Japanese academic Hitoshi Suzuki [4], suggesting that Japanese researchers were the first to gain insight into the pathogenesis of IgAN and develop specific therapies. Therefore, there are more IgAN publications in Japan (ranked second). China has more IgAN publications than Japan and ranks first, which may be associated with the distribution of more high-productivity institutions. However, its citations are not yet high enough, indicating that the research quality needs to be improved. This contradiction between quantity and quality may be correlated with the lack of a standardized academic evaluation system and the imbalance of research capabilities among institutions.
Among the high-productivity countries and institutions, there are 4 European countries, 3 East Asian countries, and 7 Chinese institutions. These data suggest that East Asian and European regions shoulder a significant burden of IgAN. It is well known that the pathogenic pathways of IgAN are multifaceted and complicated and that genetic and environmental factors can also influence disease susceptibility, severity, and prognosis across ethnic populations. Epidemiologically, the prevalence of IgAN is highest in populations of East Asian ancestry, followed by Caucasians [18]. Genetically, the frequency of genetic risk alleles for IgAN is higher in the Chinese population [18]. Collectively, our data are in line with the epidemiological and genetic characteristics of IgAN.
Concerning cooperation, 94.80% (73/77) and 88.12% (2929/3324) of countries and institutions, respectively, are involved in collaborative activities. Research collaboration at national level is, therefore, relatively closer. Of course, these collaborations remain robust and stable within the top 10 high-productivity countries/institutions. This implies that multi-institutional collaborations should be further strengthened to address the major scientific questions in IgAN, which requires high-level institutions to make full use of their leadership role in radiating scientific impact, thereby raising the overall academic standard and impact of local institutions.
Analysis of keywords
Keywords with high burst strength reflect the hotspots of research at a given time. The keywords ‘multicenter study’ (2020–2023) and ‘gut microbiota’ (2021–2023) continue to have a sustained burst in 2023, and are both hotspots and frontiers.
IgAN and multicenter study
The importance of well-designed trials in refining treatment strategies for patients cannot be overstated, and this is particularly true of multicenter studies. ClinicalTrials.gov is one of the most comprehensive clinical trials registries in the world. We searched the ClinicalTrials.gov platform for phase II and phase III trials using the search term ‘IgA nephropathy’ on 7 March 2023. Thirty-four multicenter trials were identified by reviewing trial protocol details and tracking publications. Their NCT number, title, status, phase, condition, participant sex, participant age, study type, study design, interventions, and study outcomes were also extracted as shown in the Supplementary Material 2. Of these, the following aspects are worth highlighting.
First, in terms of study type, the 34 multicenter studies were all intervention studies, most of which used randomized allocation and parallel assignment intervention model designs, but only 18 studies used single-, double-, or multi-blind designs. It is important to note that the lack of masking and inadequate randomization often makes it difficult to eliminate reverse causality and patients’ awareness of potential treatments, increasing the likelihood of trials being confounded and biased. Further improvements in trial design and methodology are needed to improve the research quality.
Second, in terms of participants, only seven trials included pediatric patients with IgAN. It is worth noting that children and young adults are both major groups for IgAN [19]. However, the two groups differ in terms of clinical management, dose monitoring, adverse effects, drug tolerability, and metabolic kinetics. Further multicenter trials specific to pediatric patients are warranted.
Third, in terms of interventions, it is mainly divided into supportive therapies, immunosuppressive therapies, novel targeted release corticosteroid therapies, and biologics therapies. Among them, biologics are the most common, including sibeprenlimab [targeting a proliferation-inducing ligand (APRIL)], BION-1301 (targeting APRIL), telitacicept (targeting B-cell-activation factor and APRIL), felzartamab (targeting CD38), AT-1501 (targeting CD40L), CCX168 (targeting C5a receptor), LNP023 (targeting complement factor B), and BCX9930 (targeting complement factor D). The biological agents mentioned above target different subsets of immune cells (B cells, plasma cells, and T–B interactions) and the complement alternative pathway. The following aspects may explain the change in therapeutic strategy. The first is based on the targeting of biologics, which promises to minimize cytotoxic effects on non-target cells; the second is based on the pathogenesis of IgAN, where inhibition of complement activation and differentiation of IgA-producing immune cell subpopulations are important therapeutic ideas; and the third is the advancement of recombinant biotechnology and monoclonal antibody preparation techniques.
A new oral formulation, Nefecon, is also being studied in several multicenter studies in IgAN. In part A of the NefIgArd study, published last month, Nefecon (16 mg/day) was used to treat 199 adult patients with primary IgAN over a period of 9 months [20]. The primary endpoint of this trial was the 24-h urine protein to creatinine ratio (UPCR) after 9 months of treatment. The results showed a 27% reduction in UPCR in the Nefecon group compared to the placebo group and a good advantage of Nefecon in terms of eGFR maintenance and tolerability. Although this is a multicenter study, we are very much looking forward to the results of trials of Nefecon in other regions, as the participants is predominantly Caucasian.
IgAN and gut microbiota
Dysbiosis of gut microbiota ecology suggested as a novel mechanism in the pathogenesis of IgAN [21]. Put simply, dysbiosis affects microbial biochemical and fermentation functions, resulting in altered metabolites that are recognized by pattern recognition receptors in epithelial cells and crosstalk downstream signaling pathways. In addition, the microbial imbalance exposes the host to intestinal inflammation, induces a B-cell classification switch, leads to overproduction of Gd-IgA1 and mediates IgAN development [21].
These mechanisms appear to explain some questions such as the presence of haematuria in IgAN patients following intestinal infection, and differences in microbiota and metabolites in feces and body fluids between IgAN patients and healthy controls. Therefore, restoration of the intestinal microenvironment and re-adjustment of immune homeostasis by probiotics, fecal microbiota transplantation, fecal capsules and dietary modification (gluten-free diet) are feasible for the treatment of IgAN [22,23,24,25,26,27]. Furthermore, at American Society of Nephrology Kidney Week 2022, James Gleeson’s team reported the involvement of gut microbiota in IgA1 deglycosylation [28], highlighting its unique potential and value in IgAN research. Overall, restoring microbial homeostasis and improving intestinal mucosal immune function may be new therapeutic strategies for IgAN, but this needs to be confirmed by extensive long-term laboratory and clinical studies.
Analysis of references
Highly bursty references reflect to some extent the research interests of a given period. References Oxford Classification of IgA nephropathy 2016: an update from the IgA Nephropathy Classification Working Group (2019–2023, Review, PMID: 28341274) and IgA Nephropathy (2021–2023, Review, PMID: 28159829) have received more research attention at present.
Not surprisingly, three of the top five references for burst intensity are related to the Oxford IgAN classification. First, the Oxford classification is extremely significant in guiding/assessing renal biopsy pathology, clinical treatment, and prognosis in IgAN patients. Second, most of the authors involved in these three studies are members of the Working Group of the International IgA Nephropathy Network and the Renal Pathology Society. They have published many high-quality studies in IgAN and enjoy a high academic reputation. In addition, comprehensive and weighty IgAN reviews are also likely to attract the attention of researchers. Finally, it is interesting to note that the two papers whose citations continue to explode until 2023 were published more recently than the other three. This is reasonable, as research is constantly being updated and deepened, and researchers prefer to cite the latest published.
Limitations
First, we ignored other large databases beyond WOSCC, which may have missed some relevant information. Second, we only enrolled English publications, which implies that the role of non-English literature may be underestimated. Third, as the WOS database and the ClinicalTrials.gov platform are constantly updated, this study does not always reflect the real-time situation.
Conclusions
We present global research trends in IgAN. From 2012 to 2023, IgAN publications show a linear increase with good sustainability. China is the country with the highest number of publications and Peking University is the institution with the highest number of publications. Countries and institutions in other high-prevalence regions have also contributed significantly to the development of the IgAN field. Generally speaking, cooperation at national level is generally close, but needs to be further deepened and strengthened at inter-institutional level.
Current research hotspots and frontiers are mainly in IgAN-related multicenter studies and gut microbiota research. Most of these multicenter trials evaluate the efficacy and safety of biological agents in patients with IgAN. However, there is room for improvement in trial design. In addition, there is a need to increase the number of multicenter trials specifically aimed at pediatric patients. Given the prominent burst intensity and burst duration of these two keywords, this research boom is likely to continue and drive new research trends.
Data availability
All original contributions are included in the manuscript.
References
O’Shaughnessy MM, Hogan SL, Thompson BD, Coppo R, Fogo AB, Jennette JC (2018) Glomerular disease frequencies by race, sex and region: results from the International Kidney Biopsy Survey. Nephrol Dial Transpl 33(4):661–669
Maixnerova D, Reily C, Bian Q, Neprasova M, Novak J, Tesar V (2016) Markers for the progression of IgA nephropathy. J Nephrol 29(4):535–541
Floege J, Rauen T, Tang S (2021) Current treatment of IgA nephropathy. Semin Immunopathol 43(5):717–728
Suzuki H, Kiryluk K, Novak J, Moldoveanu Z, Herr AB, Renfrow MB et al (2011) The pathophysiology of IgA nephropathy. J Am Soc Nephrol 22(10):1795–1803
Rovin BH, Adler SG, Barratt J, Bridoux F, Burdge KA, Chan TM et al (2021) Executive summary of the KDIGO 2021 guideline for the management of glomerular diseases. Kidney Int 100(4):753–779
Mou J, Cui Y, Kurcz K (2019) Bibliometric and visualized analysis of research on major e-commerce journals using Citespace. J Electron Commer Re 20(4):219–237
Diem A, Wolter SC (2013) The use of bibliometrics to measure research performance in education sciences. Res High Educ 54(1):86–114
Mayr P, Scharnhorst A (2015) Scientometrics and information retrieval: weak-links revitalized. Scientometrics 102(3):2193–2199
Abramo G, D’Angelo CA, Viel F (2011) The field standardized average impact of national research systems compared to world average: the case of Italy. Scientometrics 88(2):599–615
Wu H, Wang Y, Tong L, Yan H, Sun Z (2021) Global research trends of ferroptosis: a rapidly evolving field with enormous potential. Front Cell Dev Biol 9:646311
Wu H, Li Y, Tong L, Wang Y, Sun Z (2021) Worldwide research tendency and hotspots on hip fracture: a 20-year bibliometric analysis. Arch Osteoporos 16(1):73
Yeung AWK, Tzvetkov NT, Balacheva AA, Georgieva MG, Gan RY, Jozwik AP et al (2020) Lignans: quantitative analysis of the research literature. Front Pharmacol 11:37
Van Eck NJ, Waltman L (2009) Vosviewer, a computer program for bibliometric mapping. In: Proceedings of ISSI 2009—12th international conference of the international society for scientometrics and informetrics, vol 22, pp 886–897
Chen C (2004) Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci USA 101(Suppl 1):5303–5310
Synnestvedt MB, Chen C, Holmes JH (2005) CiteSpace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc 2005:724–728
Sabe M, Pillinger T, Kaiser S et al (2022) Half a century of research on antipsychotics and schizophrenia: a scientometric study of hotspots, nodes, bursts, and trends. Neurosci Biobehav Rev 136:104608
Hsu SI, Ramirez SB, Winn MP, Bonventre JV, Owen WF (2000) Evidence for genetic factors in the development and progression of IgA nephropathy. Kidney Int 57(5):1818–1835
Yeo SC, Goh SM, Barratt J (2019) Is immunoglobulin A nephropathy different in different ethnic populations? Nephrology (Carlton) 24(9):885–895
Wyatt RJ, Julian BA (2013) IgA nephropathy. N Engl J Med 368(25):2402–2414
Barratt J, Lafayette R, Kristensen J et al (2023) Results from part A of the multi-center, double-blind, randomized, placebo-controlled NefIgArd trial, which evaluated targeted-release formulation of budesonide for the treatment of primary immunoglobulin A nephropathy. Kidney Int 103(2):391–402
He JW, Zhou XJ, Lv JC, Zhang H (2020) Perspectives on how mucosal immune responses, infections and gut microbiome shape IgA nephropathy and future therapies. Theranostics 10(25):11462–11478
Tan J, Dong L, Jiang Z et al (2022) Probiotics ameliorate IgA nephropathy by improving gut dysbiosis and blunting NLRP3 signaling. J Transl Med 20(1):382
Lauriero G, Abbad L, Vacca M et al (2021) Fecal microbiota transplantation modulates renal phenotype in the humanized mouse model of IgA nephropathy. Front Immunol 12:694787
Zhao J, Bai M, Yang X, Wang Y, Li R, Sun S (2021) Alleviation of refractory IgA nephropathy by intensive fecal microbiota transplantation: the first case reports. Ren Fail 43(1):928–933
Zhi W, Song W, Abdi Saed Y, Wang Y, Li Y (2022) Fecal capsule as a therapeutic strategy in IgA nephropathy: a brief report. Front Med (Lausanne) 9:914250
Coppo R, Amore A, Roccatello D (1992) Dietary antigens and primary immunoglobulin A nephropathy. J Am Soc Nephrol 2(10 Suppl):S173–S180
Papista C, Lechner S, Ben Mkaddem S et al (2015) Gluten exacerbates IgA nephropathy in humanized mice through gliadin-CD89 interaction. Kidney Int 88(2):276–285
Acknowledgements
Thanks to Dr. Chengliang Wang for his useful suggestions.
Funding
This study did not receive any funding.
Author information
Authors and Affiliations
Contributions
WJ: conceptualization, methodology, visualization, supervision, and revision. WX: original draft preparation. CX: investigation. PD: visualization. All the authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Conflict of interest
The study was conducted without any business or financial relationships that could be interpreted as potential conflicts of interest.
Ethical approval
This study did not involve animal or human experimentation. Therefore, ethical approval from an institutional review board was not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
: The keyword network visualization. (TIF 2534 KB)
Supplementary Material 2
: Details of the IgAN multicenter study. (XLSX 14 KB)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wang, J., Wang, X., Cai, X. et al. Global trends and hotspots in IgA nephropathy: a bibliometric analysis and knowledge map visualization from 2012 to 2023. Int Urol Nephrol 55, 3197–3207 (2023). https://doi.org/10.1007/s11255-023-03598-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-023-03598-x