
Abstract
This study examines spatial disparities and associations between the social deprivation index (SDI) and Type 2 Diabetes, Dementia, and Heart Failure in Italy’s Lazio Region. The primary goal is to assess how social deprivation impacts health inequalities by analysing SDI-disease correlations. This retrospective study uses 2020 socioeconomic data and 2021 epidemiological indicators in Lazio Region, Italy. The SDI, constructed following established guidelines, measures social deprivation. Statistical tools, including regression models, Moran’s I test, and LISA techniques, are used to analyse spatial patterns. Utilizing a retrospective approach, we merge 2020 socioeconomic and 2021 epidemiological data for analysis. The SDI is computed using established methods. Spatial disparities are explored through regression models, Moran’s I test, and LISA techniques. The study reveals significant disparities in disease incidence. District V in Rome exhibits high Type 2 Diabetes (113.75/1000) and Heart Failure (37.98/1000) rates, while Marcetelli has elevated Dementia incidence (19.74). Southern municipalities face high unemployment (up to 25%), whereas bordering areas have higher education levels (30–60%). Disease hotspots emerge in Rome and centre-north municipalities, aligning with social deprivation patterns. Regression models confirm the link between disease incidence and socioeconomic indicators. SDI ranges from − 1.31 to + 10.01. This study underscores a correlation between social deprivation and disease incidence. Further national-level research is essential to deepen our understanding of how social deprivation influences health outcomes, with potential implications for addressing health disparities both regionally and nationally.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Social deprivation refers to an individual’s or a group of individuals’ inability to access material and social resources, as well as to the fragility of social networks ranging from family to community (Lamnisos et al., 2019; Townsend et al., 1988).
In other words, it can be defined as follows: “A state of observable and demonstrable disadvantage relative to the local community or the wider society or nation to which an individual, family or group belongs” (Paterson & Gregory, 2019). The most useful tool for evaluating social deprivation and its relationship to health outcomes, are Social Deprivation Indices, which provide a comprehensive and nuanced understanding of social deprivation than traditional measures such as income or education (Minichilli et al., 2017).
Deprivation indices are multidimensional measures of material and social resources developed since the 1980s (Carstairs & Morris, 1989) already widely applied to understand health inequalities. From the Robert Graham Center (https://www.graham-center.org/maps-data-tools/social-deprivation-index.html) the policy institute affiliated with the American Academy of Family Physicians, the social deprivation index (SDI) instead takes into account information related to social factors that influence health outcomes and healthcare utilization. It employs this data to develop a predictive model and assess its consistency across various geographic areas. (Phillips et al., 2016). The SDI is a tool commonly used tool that assesses geographic areas' deprivation levels by combining various indicators into a composite measure. Like other composite indicators, the SDI is valuable in evaluating relative positions, aiding policy analysis, trend identification, and performance monitoring of area-level deprivation to quantify, for example, the socio-economic variation in health outcomes (Butler et al., 2013). It summarizes multidimensional concepts, aiding decision-makers and public communication, yet may lead to misleading conclusions if poorly constructed or misinterpreted. While advantageous in simplifying complex data, composite indicators could mask deficiencies and lead to inappropriate policies if construction lacks transparency or ignores challenging-to-measure dimensions (OECD et al., 2008). Literature indicates that the most useful parameters to investigate social deprivation belong to demographic, social, and economic domains. In particular, many studies focused on socio-economic domains, including income, education, house ownership, employment status, and social class in terms of occupation (Jarman, 1983; Kawachi & Subramanian, 2007; Rosano et al., 2020). Reducing the significant health gaps between different socio-economic groups, which are determined by factors like education, occupation, and income, poses a major challenge for public health efforts.According to literature, a higher socioeconomic deprivation has a negative impact on a wide variety of health outcomes (Dunn, 2014), demonstrating how health disparities are linked to systematic differences in social or socioeconomic position (Coyte et al., 1995).
Lazio is the second most inhabited region in Italy, (the ninth in terms of geographical dimension) with a population density unevenly distributed over the regional territory, varying between 115 in the municipality of Micigliano inh/km2 and 2969 inh/km2 in the municipality of Ciampino. Hosting Roma, the Capital City of Italy, its territory is vastly variable in both geographical and social terms, with the second highest number of foreign residents among all Italian regions. Its 378 municipalities are variously engaged in economic activities related to all three economic sectors (ISTAT, 2022). Therefore, its heterogeneous socio-economic development reflects both in the educational and business-related contexts. Following the definition included in Healthy People 2010 (United States D of H & HS, 2000), differences that occur in gender, race or ethnicity, education or income, disability, geographic location, or sexual orientation can all be considered various forms of inequalities. As a matter of fact, although universal healthcare represents the health system model in Italy, the renowned right to public healthcare does not always materialize. While entitlement to access healthcare is important, it is crucial to recognize that it does not automatically guarantee the achievement of horizontal equity in healthcare utilization. Horizontal equity refers to a situation where individuals with the same level of healthcare needs receive an equal amount of healthcare services, regardless of non-need-related individual characteristics. These characteristics may include factors like the ability to afford co-payments for healthcare or the option to purchase private healthcare services, thus bypassing the potential delays associated with public queues. (Tavares & Zantomio, 2017). Literature extensively explores the correlation between social deprivation and the occurrence of commonly documented pathologies, both at the national and international levels. A significant link exists between socio-economic factors and health outcomes in Italy, associating status with diabetes prevalence, particularly impacting women (Fano et al., 2013) and escalating risks of mortality and hospitalization. This trend extends nationwide, emphasizing the need for tailored prevention in vulnerable groups (Gnavi et al., 2008). Examining diabetes-related mortality and dietary trends, a consistent rise is noted, indicating poorer dietary habits among socially deprived individuals (Altamirano & Sapienza, 2018). Similarly, analysis of coronary events underscores job status as a pivotal socio-economic factor influencing incidence and mortality, highlighting broader social determinants on heart health (Alicandro et al., 2018). Cardiovascular risk factor prevention shows socio-economic disparities, with higher education correlating with increased cholesterol monitoring and better weight control (Damiani et al., 2011). Finally, Italy’s global dementia plan underscores the need to address socio-economic factors for comprehensive care, stressing the profound impact of social inequities on health outcomes and advocating for focused interventions (Ricci, 2019). Existing literature reinforces a higher dementia prevalence in individuals with limited education, particularly pronounced in younger age groups (Ronchi et al., 1998). Persistent socioeconomic disparities in diabetes prevalence highlight the imperative for comprehensive research into the underlying mechanisms of this relationship (Tapager et al., 2023). Studies found regional disparities in self-rated health linked to factors like poor living conditions and private healthcare expenditure, suggesting that Italian regions might address health inequalities through targeted policies and interventions (Franzini & Giannoni, 2010). An 11 European countries study reports lower education correlating with higher type 2 diabetes mellitus, particularly impacting women (Espelt et al., 2013). Social disparities consistently affect diabetes care in OECD countries, revealing a two-way relationship between social deprivation and diabetes development, with a socioeconomic gradient in complications, particularly in retinopathy and cardiopathy (Tatulashvili et al., 2020). Poor lifestyle choices associated with social factors, like inadequate sleep and lack of exercise, amplify insulin resistance (Ricci-Cabello et al., 2010; Tatulashvili et al., 2020). The global congestive heart failure (G-CHF) registry global examination of heart failure across 40 countries shows economic factors significantly influence HF characteristics and outcomes as well, with lower socio-economic status correlating with increased HF incidence and poorer outcomes (Vergallo & Patrono, 2023). Smoking substantially contributes to a 40% explanation of social disparities in coronary heart disease, emphasizing the need for urgent efforts, particularly targeting the most deprived (Hawkins et al., 2012). Additionally, in the UK, research on individuals with dementia revealed consistent life expectancy and mortality patterns across socio-economic groups, highlighting the impact of social deprivation (Vestergaard et al., 2020). A European scoping review on dementia care highlighted issues like fragmented pathways, cultural hurdles, and inadequate skills in acute hospital settings. The study called for policy changes emphasizing person-centered care, integrated pathways, and healthcare workforce development to address these gaps, with a focus on overcoming stigma, particularly in Western societies and minority groups, to improve care access and health behaviors, affirming the insights gleaned from the national literature (Martin et al., 2020).
Supported by official data from the main Italian institutional databases, we calculated the SDI of the 378 Lazio municipalities and the sub-municipalities of Roma Capitale. That being stated, in order to manage, analyze and visualize spatial data we relied on a Geographic information system (GIS). Several research studies already considered the spatial analysis of the SDI. The utilization of GIS and related spatial analysis methods presents an invaluable toolkit for examining and comprehending the evolving spatial structure of healthcare. By leveraging these tools, researchers can delve into the intricate relationship between healthcare provision, health outcomes, and accessibility, thereby uncovering opportunities for enhancing the delivery of healthcare services. This enables a deeper understanding of the spatial dynamics at play within the healthcare system, allowing for informed decision-making and targeted interventions to optimize healthcare outcomes (McLafferty, 2003; Porter & Howell, 2012). Understanding spatial inequality goes beyond just a simple mapping of the inequality of interest. Comparative analysis using related spatial statistics allows to find results undetectable with a one-method analysis, potentially assisting in the identification of the underlying distributive, or generating forces.
A set of spatial analysis techniques was applied to analyze the deprivation situation in the Lazio Region. Understanding spatial inequality entails more than just mapping out the inequality of interest.
Understanding why these inequalities exist and how policy can address them should be a primary focus of spatial inequality research (Cascini et al., 2019; Lobao et al., 2007). The aim of the present paper is twofold. First, a tailored SDI for the various municipalities of the Lazio region was estimated. Secondly, we will determine whether correlations between the SDI and the incidence of three of the most frequently diagnosed community diseases, namely: Type 2 Diabetes, Dementia, and Heart failure, exist.
2 Materials and Methods
2.1 Study Design and Data Sources
This is a retrospective, longitudinal study conducted on the population of Lazio region in Italy. Socio-economic data referred to 2020 was retrieved from Italian Statistical Institute (ISTAT) and Roma Capitale datasets. Secondly, epidemiological indicators describing the incidence of three of the most frequent diseases in the general population, namely type 2 diabetes, heart failure and dementia, were retrieved from the Department of Epidemiology of Lazio Regional Health (Cascini et al., 2019) for the year 2021.
2.2 SDI Development
The development of our Social Deprivation Index followed Butler et al. (2013) guidelines for the creation of small area deprivation indices uncovered a series of five crucial stages, namely the process of identifying appropriate data and geographic boundaries, the careful selection of specific indicators for measuring deprivation, the development of an index by amalgamating and assigning weights to these indicators, the rigorous validation and sensitivity analysis of the index, and finally, addressing and accounting for any uncertainties encountered throughout the study. A geocode shapefile of the municipalities of Lazio region and metropolitan city of Rome was used to identify our area of interest. Areas were normalized for one thousand inhabitants. For a better reading, the municipalities were grouped into two parts: population with less than one thousand inhabitants per square kilometer and municipalities with more than one thousand inhabitants per square kilometer. Secondly, a literature review was conducted investigating the existing national and international literature approaching the topic (Malmström et al., 1998; Wang et al., 2021; Croudace et al., 2000; Pampalon et al., 2009, 2012; Myck et al., 2015; Knighton et al., 2016; Gonthier et al., 2017; Châtelet et al., 2018; Bevan et al., 2021). The selection of indicator variables was based on available scientific evidence. Single items, derived from the evaluated indexes correlation with health outcomes, were then studied through Pearson (r). From the statistical analysis of evaluated items, the most suitable index resulted to be the one validated in Rosano et al. (2020). Several changes were made to tailor the index to the study aim by updating variables with the latest available data. Considering rental housing as mostly allocated by means of market contracts between landlords and tenants rather than population economic conditions (Dewilde, 2021), we substituted this item with the percentage of people living in crowded houses to evaluate housing conditions. Once selected the most suitable sub indicators, standardization was conducted following the z-scores approach (Anselin, 2016) weighting for persons resident. During the validation and sensitivity analysis phase of the indicator, a preliminary examination of the pairwise correlations among the various sub-indicators. In the process of selecting the most suitable methodology, we compared two approaches: (1) weighted summation of z-scores for individual variables and a (2) Weighting method based on Factor Analysis (Vidoli et al., 2015). The latter aimed to estimate a composite indicator that captures the maximum information common to individual indicators. Surprisingly, our analysis revealed a highly correlated and significant positive relationship (Spearman correlation method) between the Weighting method and the summation of z-scores for individual variables. As a result, the rankings derived from this Spearman correlation were exceptionally close, rendering them almost indistinguishable. Consequently, we made the decision to exclude the Weighting method for the final definition of the indicator to avoid redundancy and complexity, opting instead for the simplicity and transparency afforded by the summation of z-scores. SDI construction allowed us to detect the most influential item on the total score.
2.3 Statistical Analysis
Prior to the empirical analysis, all data were standardized (Minichilli et al., 2017). Applying the Z-scores, we initially estimated a linear regression model explaining the correlation among disease incidence and SDI. Given the spatial nature of the considered variable, which are likely to display smooth variations in space, we fitted a spatial linear regression model as well. Multiple linear regressions and spatial regression analyses were also conducted to quantify the relationship between the dependent variables (i.e., epidemiological indicators) and the set of explanatory variables (i.e., social variables at the municipality level). Furthermore, in order to test the presence of spatial autocorrelation in the observed variables, Moran’s I test was also calculated together with the associated local indicator of spatial association (LISA) techniques (Anselin, 1995). The empirical data examined allow to reveal the presence of spatial heterogeneity in the form of local clusters (Weeks, 2001; Wei, 2015). Given this, the Moran scatter plot (Ivaldi, 2016) was drafted to categorize spatial association into four typologies, i.e., High values surrounded by High values (High–High = HH), Low values surrounded by Low values (Low–Low = LL), Low values surrounded by High values (Low–High = LH) and High values surrounded by Low values (High–Low = HL). In particular, areas labeled HL (or hotspot) and LH (or cold spot) highlight the presence of spatial outliers.
3 Results
3.1 Descriptive Statistics of Social and Health Variables
Our sample was constituted by the 378 municipalities of Lazio region in Italy. For each municipality, we considered the data on the three diseases (i.e., diabetes, heart failure and dementia). Table S1 shows all social variables considered in the analysis and Table S2 shows the descriptive statistical summary of them. Overall, diabetes was the most frequently reported disease. Table S3 shows all social variables considered in the analysis and in Table S4(supplementary materials) shows the descriptive statistical summary of them. The first social variable included in the SDI is the percentage of unemployed individuals aged 16–64 years. Related to this variable, the highest percentages are in the southern municipalities of Lazio (in the provinces of Latina and Frosinone) reaching 25% of the population. In the metropolitan city it reaches a maximum of 5%, whereas values between 10–15% were registered in the north of the region (province of Viterbo).
As for the percentage of people under 12 years of education, the highest percentages refer to the municipalities that are at the border with other Italian regions, with values ranging between thirty and over 60% of the population.
The percentage of people renting fluctuates between just over 1% and over 20%. The largest portion of this percentage can be observed in the metropolitan city of Rome, with high values also recorded in the municipalities of the coastal area of Lazio. The lowest values are observed in the provinces of Rieti and Frosinone. As for the percentage of families with single parents, peaks were detected in the municipalities of the north-east of the region, namely those included in the province of Rieti.
Figure S1a in the supplementary materials presents the map and Violin plot illustrating every social variable that determines the social development index (SDI). The figure allows for the identification of peaks in the data as well as the visualization of their distribution. The last social variable is the population density, which peaks up in the municipalities near Rome and along the Tyrrhenian coast (Figure S1b).
Figure S2 depicts the incidences of the most common diseases per one thousand inhabitants in the year 2021. As illustrated, a higher concentration of diseases regards the central and urban municipalities of Rome if compared with the other areas of the region.
3.2 Correlation Analyses
3.2.1 Sub-indicators
Regarding the preliminary analysis conducted among the five sub-indicators, none of the correlations are significant (results in Figure S3). The highest correlation was found between “population density” and “population in crowded houses” (0.39, p value: 0.17), whereas the lowest correlation was recorded between “populations in crowded houses” and “education < than 12 years” (− 0,41, p value: 0.13). Both the Moran scatter plots, and the LISA maps (Fig. 1a, b) show significant spatial clusters.

a Moran Plot of incidence of community diseases for 1000 inhabitants in 2021. b LISA Map of incidence of community diseases for 1000 inhabitants in 2021. As a result, there are five potential outcomes that could arise: (LL) areas that exhibit high values and have neighboring areas with similar values; (HH) areas that exhibit low values and have neighboring areas with similar values; (HL) areas that exhibit high values but have neighboring areas with low values; (LH) areas that exhibit low values but have neighboring areas with high values; and (NA) areas that do not show any notable local spatial correlation
The combination of Moran scatterplot and the LISA maps for each disease allowed to understand which locations are contributing most strongly to the primary outcome.
For all the three diseases, the hotspot appears concentrated in in the metropolitan city of Rome and in the municipalities in the center-north of the region (Fig. 1a, b).
Particularly, for type 2 Diabetes, we observed the presence of cold spots and outliers of both types (LH and HL) in the Rieti province municipalities. An analogous situation was observed for Heath failure, but with the presence of only LH outliers. Dementia displays LH values only in the northern area of the province of Rieti.
To investigate the relationship between the incidence of the diseases (dependent variable) and the socio-economic indicators (predictors), three multiple regressions models were estimated.
Table 1 shows the main results of the statistical tests conducted on the three regression models. In the two upper sections of the table, we reported the main tests, while the lower section is related to the regression diagnostics on the model hypotheses. In all three regressions, the overall model is significant (p value < 0.001), but not all regressors are significant. In particular:
-
% Unemployed is not significant in regressions related to the incidence of type 2 diabetes (p value = 0.08) and dementia (p value = 0.33).
-
% Education years < 12 is significant for all regressions.
-
% Population in Crowded House is not significant in the regression related to the incidence of Type 2 diabetes (p value = 0.87) and relative to Heart failure (p value = 0.69).
-
% Single Parents is not significant in the regression related to the incidence of Type 2 diabetes (p value = 0.52).
-
Population density is significant for all regressions.
The third section of the table shows the results of the tests related to the hypothesis of heteroskedasticity (Bresh–Pagan test; p value always < 0.001) and normality (Jarque Bera test; p value always < 0.001).
Furthermore, Moran’s I test is positive and significant for all three regressions. This result confirmed the adequate use of spatial regression models.
Table 2 shows the comparison between the multiple linear regression coefficients estimated above (OLS) and two spatial regression models, namely: the spatial lag formulation (SLM) and the spatial error specification (SEM). All Lagrange multiplier (LM) tests reject the OLS model in favor of a spatial alternative, while the robust LM tests (RLM) indicate a preference towards spatial lag structure. We can see how the signs of the coefficients remain the same, whereas some variables do not keep the significance reached in the linear model without spatial components.
3.3 SDI Results/Estimates
The SDI score was categorized into five ranks (i.e., very deprived, deprived, not deprived, rich, very rich) using the resident population quintiles (Table S5), to group the evaluated population into categories based on their characteristics.
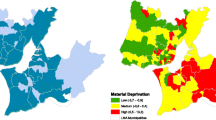
The Social Deprivation Index ranged between − 1.31 to + 10.01. A positive SDI related poor health outcomes, whereas a negative SDI linked with high health outcomes (see Fig. 2). Table S6 in supplementary materials displays spatial outliers of community disease incidence. The table highlights the most frequent clusters associated with high disease incidence values, encompassing all diseases.

Social deprivation index: left map SDI scale (min − 1.31; max: + 10.01); right map subdivision of municipalities in relation to the quintiles of its own SDI
Tables S7 in supplementary materials shows the percentage of municipalities, divided accordingly to provinces, allocated in each quintile. A positive index was recorded in the municipality V of the metropolitan city of Rome as well as in the municipalities along the borders of the region. A Negative SDIs were mostly recorded in the central municipalities of the region.
3.4 Final Regression Model: Association Between Social Deprivation Index and Income and Health Outcomes
The main results of this analysis are reported in Table S8.
All regression models were significant. As for the baseline simple linear regression, SDI has a positive impact on the incidence of the evaluated diseases. Residuals Moran’s I is positive and significant, supporting the idea that contiguous municipalities tend to assume similar values.
All LM tests reject the baseline OLS model in favor of spatial alternative specifications, while the robust version (RLM) indicates a preference towards the spatial lag structure (Table S9).
The estimated value of the spatial parameter (rho), positive and highly significant for all 3 regressions, indicates the presence of a positive spatial dependence SDI and income on the increase in the incidence of the investigated diseases, confirming previous findings (Barry et al., 2022; Hossain et al., 2012; Jarman, 1983; Merrild et al., 2022).
4 Discussion
This study aim was to evaluate whether deprived populations might be considered more susceptible to the incidence of three of the most frequently reported community diseases. Lazio region resulted particularly suitable for this scope, due to its socio-economically heterogenous population. Social inequality is a very actual and already studied topic, both for its consequences on health outcomes and access to services (McCartney et al., 2019). In order to quantify the effective burden of the deprived population, we adopted a Social Deprivation Index. The meticulous selection of the social deprivation index (SDI) is pivotal, influencing outcomes in heart failure, diabetes, and transplant contexts, as reported in existing literature (Deo et al., 2023; Park et al., 2023). SDI plays a critical role in public health planning, guiding resource allocation, and highlighting a positive association with compromised access (Goyal et al., 2023). This underscores its substantial impact on methodological approaches and interventions within diverse health domains (Pampalon et al., 2012). In broader public health planning, SDI serves as a crucial tool in identifying disparities and indicating a positive correlation with constrained access, pinpointing areas requiring targeted assistance and informing federal resource allocation (Butler et al., 2013). Additionally, in the broader context of socioeconomic development, SDI correlates with per capita GNP, influencing the formulation of strategies and policy instruments (Khan, 1991). Over the past three decades, various measures of deprivation have been suggested in areas such as health, quality of life, and development research. These measures have been linked to issues of inequality and poverty. Researchers face a significant barrier when attempting to construct these indices, primarily due to the arduous nature of accessing and compiling information on health indicators, environmental factors, and their classification. Our study, through the adoption of the most accurate and updated available data, tries to solve this issue, relating to a heterogeneous population as a single study group. At the same time, its subdivision into quintiles ensured a characterization of the individual subpopulations based on their socio-economic characteristics. A confirmation of this heterogeneity can be seen into the social variables’ trends, which widely differed among municipalities. As a matter of fact, despite being the second wealthiest region in Italy in terms of income (www.statista.com/statistics/976967/highest-gross-domestic-product-gdp-by-region-in-italy/), Lazio exhibits significant disparities in overall SDI. The registered SDIs, ranging between − 1.31 and 10.01, reflects the existing socio-economic and cultural gap among municipalities, following Townsend et al. (1979) definition of deprivation as “a state of observable and demonstrable disadvantage relative to the local community or the wider society or nation to which an individual, family or group belongs”. The highest SDIs refer to Rome Municipio V and central areas of the region, whereas the lowest SDIs are the ones of border municipalities, especially in the southern areas of the region. As for the health outcomes, investigations on the single diseases’ incidences were already carried out, demonstrating, as previously stated by literature, a correlation among the lowest quintiles and the number of registered cases of diabetes (Zuijdwijk et al., 2013), dementia (Hofbauer & Rodriguez, 2023) and heart failure (Hawkins et al., 2012). Data from the Department of Epidemiology (DEP) in Rome, allowed a rigorous analysis of incidences and their association with deprived communities. Specifically, since the deep interconnection among the investigated diseases, especially considering the higher risk for cognitive impairment when cardiovascular diseases or diabetes (Kochhann et al., 2023) pre-exist, living in socioeconomically deprived realities is consistently reported as a risk factor for all three of them (Kind & Buckingham, 2018). Our statistical analysis encountered diabetes to be the most prevalent between the three investigated diseases, confirming regional data on the matter (Istituto Superiore di Sanità, 2023). Overall, for all the three diseases, Rome municipalities and northern areas of the region presented the highest concentration of spatial clusters. Rieti was the only province to present both cold spots and outlines. As for cold spots, factors as lower population density compared to other provinces in the region, a more diverse economy based mostly on agriculture but with a growing tourism industry, as well as a number of small businesses and industries and a strong community cohesion might have an influence on the data. When it comes to disease incidence, Rieti may also present some differences compared to other areas in the Lazio region. As for the “outlines” in the incidence of disease such as diabetes, heart failure, and dementia, it must be considered that Rieti is also an aging town (https://www.tuttitalia.it/lazio/provincia-di-rieti/statistiche/indici-demografici-struttura-popolazione/#), which could potentially lead to a higher incidence of dementia as the population ages. Access to healthcare may also be a factor in the prevalence of these diseases. The application of Moran I. test allowed to assume the presence of functional relationships between neighboring regional areas, which confirmed how the economic differentiation related to health. Despite the lack of correlation among the five sub-indicators that make up the SDI, the geospatial analyses demonstrate that SDI scores are significantly clustered within the region. The northeastern border towns presented three clusters of the lowest deprivation areas, while central municipalities in the region exhibit clusters of low SDIs compared to neighboring municipalities with higher SDI. The most deprived areas were found in the north-eastern area of the region, where type 2 diabetes found its higher incidence peak. The spatial correlation between neighboring areas may suggest that environmental factors play a role in the development of diseases, as suggested by previous research (Crespo et al., 2020). This underscores the need for further investigation to better understand the relationship between social factors and diseases.
The results shed light on how social determinants play a crucial role in understanding the spatial distribution of material deprivation and its association with health outcomes. Additionally, the plotted distribution of evaluated municipalities highlights those that are furthest from the general tendency of the Lazio urban centers mean values, indicating that these areas may require targeted interventions to address social deprivation and improve access to healthcare services. The obtained results confirm the positive impact of SDI on the investigated disease, with a higher spatial association among SDI and income, as already reported in the scientific literature (Aggarwal et al., 2010; Clark et al., 2009; Connolly et al., 2000; Zoellner et al., 2011).
Evidence already exist in literature, both regarding the definition of SDI and their application to assess deprivation consequences on health (Zoellner et al., 2011). Moreover, previous researchers have already established an inverse association between socioeconomic status and the incidence of the most common diseases (Clark et al., 2009; Connolly et al., 2000). In the Lazio region, the SDI is a commonly used evaluation instrument, as reported from the Istituto Superiore di Sanità (ISS) (Marsili, 2009). The novelty of this study resides in its updated data, with information up to 2022, which provides a more current evaluation of the correlation between social deprivation and chronic diseases in the Lazio region. The provided evidence makes this paper a powerful instrument to inform policymakers and healthcare providers about the need to prioritize the provision of adequate health services based on people needs. Additionally, the plotted distribution of evaluated municipalities highlights which areas are the furthest from the general tendency of the Lazio urban centers mean values, indicating that these areas may require targeted interventions to address social deprivation and improve access to healthcare services. Consequently, it is imperative for policy makers to strategically invest resources in these areas, focusing on targeted interventions to alleviate social deprivation and enhance access to healthcare services.
Moreover, it is crucial to extend the scope of interventions beyond the immediate areas of high social deprivation. By also directing investments towards the neighboring municipalities, policy makers can address the potential spillover effects and minimize the influences of deprivation. Recognizing the interconnectivity and interdependencies between communities is essential for ensuring a comprehensive and effective approach to social development. Additionally, by extending their efforts to the surrounding municipalities, policy makers can foster regional cohesion and prevent the further exacerbation of disparities.
The findings of this study should be considered in light of its main limitations and strengths.
The first limitation is the potential presence of ecological bias. While we may observe certain trends or patterns at the population level, these may not necessarily hold true at the individual level. This problem might lead to inaccurate conclusions or recommendations based on data that is not representative of the experiences of all individuals involved. Moreover, the functional relationships between neighboring municipality areas might suggest a context influence on the development of diseases that was not considered and might require further evaluations of the underlying factors contributing to social deprivation. Also, the lack of literature defining the single provinces realities did not allow a comprehensive-enough correlation with past evidence. The use of composite indicators presents various advantages and challenges, as highlighted by multiple sources (OECD et al., 2008) and insights from Saisana and Tarantola (2002), Rosen (1991), Sharpe (2004). They enable effective communication of country performance and facilitate comparisons across dimensions. However, pitfalls exist. Poor construction or interpretation might lead to misleading policy implications and oversimplified conclusions. Transparency and robust principles are crucial to prevent misrepresentation or misuse. Debate persists on the meaningfulness of summary statistics versus the arbitrariness in the weighting process. Despite criticisms, the allure of summarizing complex data into a single benchmark figure for policy remains, though it may oversimplify complex realities. The utility of composite indicators hinges on their suitability and acceptance within specific contexts.
The main strength of this study is the rigorous applied methodology on official data, which guaranteed up-to-date evidence of the actual Lazio reality. Moreover, the application of a validated SDI guaranteed the efficacious standards necessary to gather the needed data. Finally, the intervention of both statistical and medical professionals involved in the production of this paper allowed an adequate synthesis of both epidemiological and statistical data.
Further research is needed to investigate the same issues on a nation-wide scale to obtain a more comprehensive overview on SDI and relevant health outcomes.
5 Conclusions
Social Deprivation index confirmed its efficacy in mapping populations needs, defining the most critical areas and their spatial distribution. Moreover, a correlation with the incidence of diabetes, heart failure and dementia confirmed the effective association of deprivation with a higher health risk. This study empowers this tool and provides important evidence to decision makers, whilst stimulating researchers to ensure its development in view of its limitations and potentialities.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Aggarwal, R., Mytton, O. T., Derbrew, M., Hananel, D., Heydenburg, M., Issenberg, B., et al. (2010). Training and simulation for patient safety. Quality & Safety in Health Care, 19(Suppl 2), i34-43.
Alicandro, G., Sebastiani, G., Bertuccio, P., Zengarini, N., Costa, G., La Vecchia, C., et al. (2018). The main causes of death contributing to absolute and relative socio-economic inequality in Italy. Public Health, 164, 39–48.
Altamirano, L. M., & Sapienza, E. (2018). Food patterns, diabetes and overweight/obesity and some socio-economic indicators in the Italy regions. Journal of Nutrition & Food Sciences, 08(02), 1000679.
Anselin, L. (1995). Local indicators of spatial association—LISA. Geographical Analysis, 27(2), 93–115. https://doi.org/10.1111/j.1538-4632.1995.tb00338.x
Anselin, L. (2016). Local spatial autocorrelation clusters.
Barry, Y., Le Strat, Y., Azria, E., Gorza, M., Pilkington, H., Vandentorren, S., et al. (2022). Ability of municipality-level deprivation indices to capture social inequalities in perinatal health in France: A nationwide study using preterm birth and small for gestational age to illustrate their relevance. BMC Public Health, 22, 919.
Bevan, G. H., Freedman, D. A., Lee, E. K., Rajagopalan, S., & Al-Kindi, S. G. (2021). Association between ambient air pollution and county-level cardiovascular mortality in the United States by social deprivation index. American Heart Journal, 235, 125–131.
Butler, D. C., Petterson, S., Phillips, R. L., & Bazemore, A. W. (2013). Measures of social deprivation that predict health care access and need within a rational area of primary care service delivery. Health Services Research, 48(2 Pt 1), 539–559.
Carstairs, V., & Morris, R. (1989). Deprivation: Explaining differences in mortality between Scotland and England and Wales. BMJ, 299(6704), 886–889.
Cascini, S., Di Domenicantonio, R., Marino, C., Cappai, G., Bargagli, A. M., Agabiti, N., & Davoli, M. (2019). Identificazione di popolazioni affette da patologie e stime di occorrenza nella popolazione residente e assistita del Lazio. Dip di Epidemiol del Serv Sanit Reg del Lazio.
Châtelet, V., Bayat-Makoei, S., Vigneau, C., Launoy, G., & Lobbedez, T. (2018). Renal transplantation outcome and social deprivation in the French healthcare system: A cohort study using the European Deprivation Index. Transplant International is the Official Journal of the European Society for Organ Transplantation, 31(10), 1089–1098.
Clark, A. M., DesMeules, M., Luo, W., Duncan, A. S., & Wielgosz, A. (2009). Socioeconomic status and cardiovascular disease: Risks and implications for care. Nature Reviews Cardiology, 6(11), 712–722.
Connolly, V., Unwin, N., Sherriff, P., Bilous, R., & Kelly, W. (2000). Diabetes prevalence and socioeconomic status: A population based study showing increased prevalence of type 2 diabetes mellitus in deprived areas. Journal of Epidemiology and Community Health, 54(3), 173–177.
Coyte, P., Evans, R., Barer, M., & Marmor, T. (1995). Why are some people healthy and others not? The determinants of health of populations. Canadian Journal of Economics, 28, 982.
Crespo, R., Alvarez, C., Hernandez, I., & García, C. (2020). A spatially explicit analysis of chronic diseases in small areas: A case study of diabetes in Santiago, Chile. International Journal of Health Geographics, 19(1), 24. https://doi.org/10.1186/s12942-020-00217-1
Croudace, T. J., Kayne, R., Jones, P. B., & Harrison, G. L. (2000). Non-linear relationship between an index of social deprivation, psychiatric admission prevalence and the incidence of psychosis. Psychological Medicine, 30(1), 177–185.
Damiani, G., Federico, B., Bianchi, C. B. N. A., Ronconi, A., Basso, D., Fiorenza, S., et al. (2011). Socio-economic status and prevention of cardiovascular disease in Italy: Evidence from a national health survey. European Journal of Public Health, 21(5), 591–596.
De Ronchi, D., Fratiglioni, L., Rucci, P., Paternicò, A., Graziani, S., & Dalmonte, E. (1998). The effect of education on dementia occurrence in an Italian population with middle to high socioeconomic status. Neurology, 50(5), 1231–1238.
Deo, S. V., Al-Kindi, S., Motairek, I., Elgudin, Y. E., Gorodeski, E., Nasir, K., et al. (2023). Neighbourhood-level social deprivation and the risk of recurrent heart failure hospitalizations in type 2 diabetes. Diabetes, Obesity & Metabolism, 25(10), 2846–2852.
Dewilde, C. (2021). How housing affects the association between low income and living conditions-deprivation across Europe. Socio-Economic Review, 20(1), 373–400. https://doi.org/10.1093/ser/mwab003
Dunn, J. R. (2014). Housing and inequalities in health: A study of socioeconomic dimensions of housing and self reported health from a survey of Vancouver residents.
Espelt, A., Borrell, C., Palència, L., Goday, A., Spadea, T., Gnavi, R., et al. (2013). Socioeconomic inequalities in the incidence and prevalence of type 2 diabetes mellitus in Europe. Gaceta Sanitaria, 27(6), 494–501.
Fano, V., Pezzotti, P., Gnavi, R., Bontempi, K., Miceli, M., Pagnozzi, E., et al. (2013). The role of socio-economic factors on prevalence and health outcomes of persons with diabetes in Rome, Italy. European Journal of Public Health, 23(6), 991–997.
Franzini, L., & Giannoni, M. (2010). Determinants of health disparities between Italian regions. BMC Public Health, 10(1), 296. https://doi.org/10.1186/1471-2458-10-296
Gnavi, R., Karaghiosoff, L., Costa, G., Merletti, F., & Bruno, G. (2008). Socio-economic differences in the prevalence of diabetes in Italy: The population-based Turin study. Nutrition, Metabolism, and Cardiovascular Diseases, 18(10), 678–682.
Gonthier, C., Estellat, C., Deneux-Tharaux, C., Blondel, B., Alfaiate, T., Schmitz, T., et al. (2017). Association between maternal social deprivation and prenatal care utilization: The PreCARE cohort study. BMC Pregnancy and Childbirth, 17(1), 126. https://doi.org/10.1186/s12884-017-1310-z
Goyal, P., Schenck, E., Wu, Y., Zhang, Y., Visaria, A., Orlander, D., et al. (2023). Influence of social deprivation index on in-hospital outcomes of COVID-19. Science and Reports, 13(1), 1746. https://doi.org/10.1038/s41598-023-28362-0
Hawkins, N. M., Jhund, P. S., McMurray, J. J. V., & Capewell, S. (2012). Heart failure and socioeconomic status: Accumulating evidence of inequality. European Journal of Heart Failure, 14(2), 138–146.
Hofbauer, L. M., & Rodriguez, F. S. (2023). The role of social deprivation and depression in dementia risk: Findings from the longitudinal survey of health, ageing and retirement in Europe. Epidemiology and Psychiatric Sciences, 32, e10.
Hossain, M. P., Palmer, D., Goyder, E., & El Nahas, A. M. (2012). Social deprivation and prevalence of chronic kidney disease in the UK: Workload implications for primary care. QJM, 105(2), 167–175.
ISTAT. (2002). Censimenti permanenti Data Warehouse, Censimento della popolazione e delle abitazioni. http://dati-censimentipermanenti.istat.it/.oTitle
Istituto Superiore di Sanità. Le patologie croniche più frequentemente osservate nella popolazione adulta residente in Italia—PASSI—Dati. Retrieved March 30, 2023, from https://www.epicentro.iss.it/passi/dati/croniche
Ivaldi, E. (2016). Material and social deprivation in Italy: An analysis on a regional basis. Business and Economics Journal, 2, 248–268.
Jarman, B. (1983). Identification of underprivileged areas. British Medical Journal (clinical Research Edition), 287, 130–131.
Kawachi, I., & Subramanian, S. V. (2007). Neighbourhood influences on health. Journal of Epidemiology and Community Health, 61, 3–4.
Khan, H. (1991). Measurement and determinants of socioeconomic development: A critical conspectus. Social Indicators Research, 24(2), 153–175. https://doi.org/10.1007/BF00300358
Kind, A. J. H., & Buckingham, W. R. (2018). Making neighborhood-disadvantage metrics accessible—The neighborhood atlas. New England Journal of Medicine, 378(26), 2456–2458.
Knighton, A. J., Savitz, L., Belnap, T., Stephenson, B., & VanDerslice, J. (2016). Introduction of an area deprivation index measuring patient socioeconomic status in an integrated health system: Implications for population health. EGEMS (washington, DC)., 4(3), 1238.
Kochhann, R., Bartrés-Faz, D., Fonseca, R., & Stern, Y. (2023). Editorial: Cognitive reserve and resilience in aging. Frontiers in Psychology, 13, 1120379.
Lamnisos, D., Lambrianidou, G., & Middleton, N. (2019). Small-area socioeconomic deprivation indices in Cyprus: Development and association with premature mortality. BMC Public Health, 19(1), 627. https://doi.org/10.1186/s12889-019-6973-0
Lobao, L. M., Hooks, G., & Tickamyer, A. R. (2007). The sociology of spatial inequality. In Sociology of spatial inequality (pp. 1–274). The State University of New York Press.
Malmström, M., Sundquist, J., Bajekal, M., & Johansson, S. E. (1998). Indices of need and social deprivation for primary health care. Scandinavian Journal of Social Medicine, 26(2), 124–130.
Marsili, D. (2009). Environmental health and the multidimensional concept of development: The role of environmental epidemiology within international cooperation initiatives. Annali Dell’istituto Superiore Di Sanità, 45, 76–82.
Martin, A., O’Connor, S., & Jackson, C. (2020). A scoping review of gaps and priorities in dementia care in Europe. Dementia, 19(7), 2135–2151.
McCartney, G., Popham, F., McMaster, R., & Cumbers, A. (2019). Defining health and health inequalities. Public Health, 172, 22–30.
McLafferty, S. L. (2003). GIS and health care. Annual Review of Public Health, 24, 25–42.
Merrild, C. H., Jønsson, A. B. R., Rasmussen, S., & Sandbæk, A. (2022). Social inequality in health. Ugeskrift for Laeger, 184(16), V09210725.
Minichilli, F., Santoro, M., Bianchi, F., Caranci, N., De Santis, M., & Pasetto, R. (2017). Evaluation of the use of the socioeconomic deprivation index at area level in ecological studies on environment and health. Epidemiologia e Prevenzione, 41(3–4), 187–196.
Myck, M., Najsztub, M., & Oczkowska, M. (2015). Measuring social deprivation and social exclusion. In A. Börsch-Supan, T. Kneip, H. Litwin, M. Myck, & G. Weber (Eds.), Ageing in Europe—Supporting policies for an inclusive society (pp. 67–78). Berlin: De Gruyter. https://doi.org/10.1515/9783110444414-008
OECD, Union E, Commission JRC-E. (2008). Handbook on Constructing Composite Indicators: Methodology and User Guide (p. 162). https://www.oecd-ilibrary.org/content/publication/9789264043466-en
Pampalon, R., Hamel, D., Gamache, P., Philibert, M. D., Raymond, G., & Simpson, A. (2012). An area-based material and social deprivation index for public health in Québec and Canada. Canadian Journal of Public Health, 103(8 Suppl 2), S17-22.
Pampalon, R., Hamel, D., Gamache, P., & Raymond, G. (2009). A deprivation index for health planning in Canada. Chronic Diseases in Canada, 29, 178–191.
Park, C., Schappe, T., Peskoe, S., Mohottige, D., Chan, N. W., Bhavsar, N. A., et al. (2023). A comparison of deprivation indices and application to transplant populations. American Journal of Transplantation: Official Journal of the American Society of Transplantation and the American Society of Transplant Surgeons, 23(3), 377–386.
Paterson, L., & Gregory I. (2019). Defining and Measuring Poverty: Using Geographical Text Analysis to Understand Discourse (pp. 1–18).
Phillips, R. L., Liaw, W., Crampton, P., Exeter, D. J., Bazemore, A., Vickery, K. D., et al. (2016). How other countries use deprivation indices—And why the united states desperately needs one. Health Affairs (millwood)., 35(11), 1991–1998.
Porter, J. R., & Howell, F. M. (2012). Geo-sociology. GeoJournal Library, 105, 1–9.
Ranking of the Italian regions with the highest GDP in 2020 (in billion euros). (2022). Statista. www.statista.com/statistics/976967/highest-gross-domestic-product-gdp-by-region-in-italy/
Ricci, G. (2019). Social aspects of dementia prevention from a worldwide to national perspective: A review on the international situation and the example of Italy. Behavioural Neurology, 2019, 8720904.
Ricci-Cabello, I., Ruiz-Pérez, I., Olry de Labry-Lima, A., & Márquez-Calderón, S. (2010). Do social inequalities exist in terms of the prevention, diagnosis, treatment, control and monitoring of diabetes? A systematic review. Health & Social Care Community., 18(6), 572–587.
Rosano, A., Pacelli, B., Zengarini, N., Costa, G., Cislaghi, C., & Caranci, N. (2020). Update and review of the 2011 Italian deprivation index calculated at the census section level. Epidemiologia e Prevenzione, 44(2–3), 162–170.
Rosen, R. (1991). Life itself: A comprehensive inquiry into the nature, origin, and fabrication of life (Vol. 13, p. 180). New York: Columbia University Press. https://doi.org/10.1177/027046769301300389
Saisana, M., & Tarantola, S. (2002). State-of-the-art report on current methodologies and practices for composite indicator development. The Joint Research Centre Italy European Commission, 214, 1–72.
Sharpe, A. (2004). Literature review of frameworks for macro-indicators (Vol. 3). Ottawa: Centre for the study of Living Standards.
Social Deprivation Index (SDI) | Robert Graham Center. https://www.graham-center.org/maps-data-tools/social-deprivation-index.html
Tapager, I., Bender, A. M., & Andersen, I. (2023). A decade of socioeconomic inequality in type 2 diabetes area-level prevalence: An unshakeable status quo? Scandinavian Journal of Public Health, 51(2), 268–274.
Tatulashvili, S., Fagherazzi, G., Dow, C., Cohen, R., Fosse, S., & Bihan, H. (2020). Socioeconomic inequalities and type 2 diabetes complications: A systematic review. Diabetes & Metabolism, 46(2), 89–99.
Tavares, L. P., & Zantomio, F. (2017). Inequity in healthcare use among older people after 2008: The case of southern European countries. Health Policy, 121(10), 1063–1071.
Townsend, P. (1979). Poverty in the United Kingdom a survey of household resources and standards of living.
Townsend, P., Phillimore, P., & Beattie, A. (1988). Health and Deprivation: Inequality and the North (1st ed.). London: Routledge. https://doi.org/10.4324/9781003368885
Tuttitalia.it. Indici demografici: Struttura della popolazione [Demographic indices: Population structure]. Retrieved April 3, 2023, from https://www.tuttitalia.it/lazio/provincia-di-rieti/statistiche/indici-demografici-struttura-popolazione/#
United States D of H and HS. (2000). Healthy people 2010: Understanding and improving health (p. 63). http://www.health.gov/healthypeople/.Guides-Non-Classroom
Vergallo, R., & Patrono, C. (2023). Heart failure and socioeconomic status: Global differences and inequalities. European Heart Journal, 44(32), 3038–3039.
Vestergaard, A. H. S., Sampson, E. L., Johnsen, S. P., & Petersen, I. (2020). Social inequalities in life expectancy and mortality in people with dementia in the United Kingdom. Alzheimer Disease and Associated Disorders, 34(3), 254–261.
Vidoli, F., Fusco, E., & Mazziotta, C. (2015). Non-compensability in composite indicators: A robust directional frontier method. Social Indicators Research, 122, 635–652.
Wang, K., Law, C.-K., Zhao, J., Hui, A.Y.-K., Yip, B.H.-K., Yeoh, E. K., et al. (2021). Measuring health-related social deprivation in small areas: development of an index and examination of its association with cancer mortality. International Journal for Equity in Health., 20(1), 216. https://doi.org/10.1186/s12939-021-01545-9
Weeks, J. (2001). The role of spatial analysis in demographic research. 4493(August).
Wei, Y. D. (2015). Spatiality of regional inequality. Applied Geography, 61(1), 1–10.
Zoellner, J. M., Connell, C. C., Madson, M. B., Wang, B., Reed, V. B., Molaison, E. F., et al. (2011). H.U.B. city steps: methods and early findings from a community-based participatory research trial to reduce blood pressure among African Americans. International Journal of Behavioral Nutrition and Physical Activity, 8(1), 59. https://doi.org/10.1186/1479-5868-8-59
Zuijdwijk, C. S., Cuerden, M., & Mahmud, F. H. (2013). Social determinants of health on glycemic control in pediatric type 1 diabetes. Journal of Pediatrics, 162(4), 730–735.
Funding
Open access funding provided by Università Cattolica del Sacro Cuore within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Contributions
Ilaria Valentini: Conceptualization, Methodology, Formal Analysis, Investigation, Resources, Data Curation, Writing—Original Draft Preparation, Writing—Reviewing And Editing, Visualization, Project Administration. Mario Cesare Nurchis: Methodology, Resources, Data Curation, Writing—Reviewing And Editing, Visualization. Gerardo Altamura: Methodology, Formal Analysis, Investigation, Writing -Reviewing And Editing. Americo Cicchetti: Conceptualization, Validation, Reviewing, Visualization, Supervision, Project Administration. Giuseppe Arbia: Conceptualization, Methodology, Investigation, Writing—Reviewing And Editing, Visualization, Supervision, Project Administration. Gianfranco Damiani: Conceptualization, Validation, Writing—Reviewing And Editing, Visualization, Supervision, Project Administration.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Valentini, I., Nurchis, M.C., Altamura, G. et al. The Impact of Socio-Economic Conditions on Individuals’ Health: Development of an Index and Examination of its Association with Three of the Most Frequently Registered Diseases in Lazio Region of Italy. Soc Indic Res (2024). https://doi.org/10.1007/s11205-024-03354-3
Accepted:
Published:
DOI: https://doi.org/10.1007/s11205-024-03354-3