
Abstract
This study explores how attitudes toward talking about sex and sexual matters influence practices regarding sexuality, sexual rights, and sexual abuse in residential institutions for people with disabilities in Greenland. 16 residents aged 17–62 and 29 managers and staff from 8 residential institutions have been interviewed about the ways sexual needs and rights are treated and discussed as well as how sexual harassment and violations are prevented or handled. The results of the study show that there are great variations between the residential institutions regarding meeting residents’ sexual needs, talking about sex, sex education, and knowledge of rules and policies in the area. While some managers and staff are quite comfortable talking to residents and each other about sex, boundaries, and the body, others find it extremely difficult and some even reject the thought of sex as a relevant topic for the residents. Regardless of the level of openness about sexual matters in the residential institutions, staff and managers express a need for more sex education with a focus on how they can best help, guide, and protect residents, but guidance about sex is much more available for residents when staff feel comfortable talking about sex. Sexual violations and illegal sexual contact might take place in residential institutions regardless of the local practices regarding sex and sex education. However, openness about sexual matters might help detect overstepped sexual boundaries and stop sexual harassment and violations earlier.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
How does a person who is paralysed and uses a wheelchair have sex? Do people with disabilities (PWD) have different sexual needs and desires than people without disabilities? These are only some of the questions that many people without disabilities ask about the sexuality of PWD [1].
PWD all over the world often face obstacles to maximising their potential as fully sexual human beings [2]. For most people, with or without disabilities, sexuality and its expression are a natural and important component of self-concept, emotional well-being, and overall quality of life [3]. Intellectual and developmental disabilities may significantly alter functioning but do not eliminate basic drives or the desire for love, affection, and intimacy [3].
Prior to the 1970s, the clinical and empirical literature was silent on the issue of sexuality and disability, which reflects a general failure of the social and behavioural sciences to recognize sexuality as a relevant issue for PWD. Historically, the topic of sexuality was either avoided or considered unnecessary in the training of professionals, as it was assumed that disabled people were asexual and had no interest in sexual activity [4].
A central question in the modern history of disability is why social attitudes toward disabled people became dramatically more negative around the turn of the twentieth century. In many industrialised countries, many PWD were segregated into institutions, involuntaryly sterilised, or prohibited from marrying under state eugenics laws. Some nations passed a series of restrictive laws to prevent the entry of ‘undesirable defectives’ into society [2, 5]. The involuntary sterilisation of PWD is not just a phenomenon of the past—it is still practiced today, but more likely in cases where the person has an intellectual disability (ID), rather than a physical disability (PD) [1]. In society, there are strongly held opinions about whether PWD can and should have children, and so they may be viewed as asexual, not just because they are assumed as incapable of having sex, but because some PWD feel that they should not have sex, because they cannot or should not have children [6, 7].
However, in recent decades things have improved for PWD; some research suggests that attitudes toward the sexuality of PWD are nuanced and many may be positive too [8]. Likewise, international policies and guidelines, like the United Nations Convention on the Rights of People with Disabilities have ensured that the rights of PWD are brought to attention [9]. Furthermore, in popular culture, PWD appear more often in television programmes and movies in a broader array of roles and are not only depicted narrowly as they were in the past [4, 10].
Sexual Health of People with Disabilities
The invisibility and oppression of disabled people’s sexual lives in public spaces contribute to disabled young people’s low levels of sexual knowledge and inadequate sex education compared to their non-disabled peers. Consequently, they are more vulnerable to “bad sex” [11], ranging from areas such as prostitution and pornography to sexual violence, unplanned pregnancies, and sexually transmitted diseases [10, 12]. A study from Israel compared 50 school students with mild ID and other disabilities with 50 non-disabled students. The results showed that 40% of students with disabilities reported having experienced sexual harassment, compared to 16% among non-disabled students [13]. In a report from The Danish Institute for Human Rights, it was found that PWD had more than double the risk of becoming a victim of a reported violent or sexual crime in 2017 compared to non-disabled people and the most severe sexual crimes were committed against PWD living in assisted housing; this group had a five times higher risk of becoming the victim of a reported sexual offense [14]. The perpetrators are usually people in their environment: peers, staff members, or family members [12, 15, 16]. Women and girls with disabilities are at greater risk of being exposed to sexual abuse than boys and men [17,18,19]. Furthermore, indigenous people are at an even greater risk of being exposed to sexual abuse [19] and the assaults typically happen in an unequal power relationship [18].
One major issue in relation to the sexuality of PWD, especially ID, regards their capability to consent to sexual contact. This capability is related to sexual knowledge scores, level of ID, adaptive behaviour, completion of a sex education program and capacity to consent to other issues [20].
Some of the common barriers to PWD’s sexual health relates to systemic barriers including lack of privacy, reduced access to sexual health information and health care, and decreased access to sexual partners. Other crucial barriers to sexual health are increased vulnerability to HIV/AIDS, increased vulnerability to sexual exploitation and abuse, and the consistent lack of sex education [2].
Sex Education
For PWD to be able to express their sexuality successfully, they require the opportunity for social and sexual education [21, 22]. Typically, this can be achieved through sex education in schools and community agencies. However, much of what is learned about sex and sexuality is derived from mass media and formal classes that are either sensationalised or not tailored to PWD [22]. PWD experience disproportionate barriers to obtaining comprehensive, accessible, and inclusive sex education due to sexually ableist ideologies [23].
Parents, educationalists, and health professionals often feel uncomfortable or unprepared to discuss issues around sexuality with disabled young people [12, 24]. This could be attributed to the exclusion of PWD from normative definitions of sexuality together with the pervasive societal devaluation of disability and the cultural scripts that portray disabled people as asexual beings [25].
In WHO’s guidance note from 2009; ‘Promoting sexual and reproductive health for persons with disabilities’ the importance of sex education is emphasized: “Like everyone else, persons with disabilities need knowledge about sexual and reproductive health, and they have the right to make reproductive decisions for themselves.”[26].
In this paper we will examine sexual health and rights for institutionalised PWD in Greenland. We will do this by exploring in which ways attitudes toward talking about sex and sexual matters influence practices regarding sexuality, sexual rights, and sexual abuse in residential institutions for PWD in Greenland.
The Greenlandic Context
Greenland is the largest island in the world and is located in the Arctic with a population of 56,000, the vast majority being Inuit (90%) [27]. There are 17 cities spread over the east and west coast with Nuuk as the largest city with over 19,000 inhabitants [28]. In addition, there are more than 60 settlements with 10–500 inhabitants. In the larger cities, there is access to education, good housing conditions, business opportunities and social and health services, while access in the smaller cities and settlements is limited [27].
Since 1979, Greenland (Kalaallit Nunaat) has been governed by Greenlanders within the framework of the Kingdom of Denmark [29].
In Greenland, Naalakkersuisut—the Government of Greenland (the National Board of Health and Welfare) coordinates disability policy and services, but since 2011, the municipalities have had the responsibility of the finances and the referring of citizens to the institutions [30]. In June 2019, Naalakkersuisut adopted an act on support for PWD; Inatsisartutlov no. 13, which is meant to reflect the UN Convention on the Rights of Persons with Disabilities [31].
In 2019, the conditions of PWD in Greenland were reported by Tilioq [32]—a politically independent national advocacy organisation established by Nalaakersuisut (the Greenlandic government) in 2017 [33]. The report concludes that there was a significant lack of knowledge about rights and legislation for PWD and that many were living under conditions that “do not belong in a welfare society” (p. 5). The challenges exist on many levels, encompassing structural factors such as infrastructure, accessibility, and difficulties in cooperation among various public authorities in the field, physical conditions such as unsuitable buildings and facilities and problems with recruiting personnel with the right qualifications and skills to handle and meet the diverse needs of the target group [32].
The challenges of implementing the Convention on the Rights of Persons with Disabilities in Greenland are extensive and complex. This is, among other factors, due to Greenland’s geography and infrastructure, which create unique challenges for all the population particularly for PWD. This underscores the importance of focusing on accessibility, particularly concerning information technology and transportation. Organisational challenges within the public administration also contribute to these complexities [34].
Over the years, PWD have been sent from Greenland to Denmark to receive appropriate support and assistance, as the Greenlandic health and social system could not meet their specific needs [35]. In recent decades, more PWD have had the opportunity to remain in their own country. This means that seeing PWD in local communities is a relatively new phenomenon in Greenland. Thus, the conversation about how people relate to PWD in Greenland and the attitudes towards this group are relatively new. This is important, as attitudes towards PWD can affect their access to participation in society, including education, labour market, and cultural life [36].
Sexuality in Greenland—Taboo or Not Taboo?
In the last century, cultural values and beliefs about sexuality have changed considerably in Greenland. The small settlements were undisturbed communities with a liberal attitude, where sex and sexuality were informal and concerned with reproduction, hereby the survival of the community. In recent decades, the Westernisation of Greenland has resulted in a dilemma regarding private love life versus sexual liberation [37, 38].
Traditionally, in Inuit culture people have been open and straightforward about sex [39]. Traditions such as ‘wife-swap’ and ‘lamp-switch-off-celebrations’ have been described by missionaries and repeated for centuries without any firsthand sources or witnesses [40]. Historical sources from the eighteenth and nineteenth centuries show that the colonial administration in Greenland was particularly occupied with marriages between Danish/Norwegian colonial clergy and Greenlandic or mixed women. Allowing mixed marriages was a way to prevent extramarital sexual relations as well as to control the colonial population [41]. The Christian missionaries imposed Christian morality on Inuit communities affecting marital practices and gender roles [42]. A study of syphilis from the mid-twentieth century estimated that 90% of young women and men had premarital sex, while extramarital sex was regarded as rather uncommon. This was explained by a comparably high age at marriage [43]. Descriptions and narratives about Greenlandic sexuality have been used for centuries to othering Greenlanders and give a picture of them as different and backward as well as morally and culturally inferior to Danes [40, 44].
Recent studies from Greenland have found that many Greenlanders are very open about having sex [45] and that especially many young people often have several sex partners within a three-month period [46]. However, another study focusing on how adults feel about talking to their teenage kids about sex, birth control and prevention, and sexually transmitted infections shows that many parents feel that they lack the knowledge and education to do so [47]. This means that many young people experience their sexual debut with little knowledge and that several adults wish to have help from public institutions such as municipal health workers, schools, and the health care system to talk to young people about sexual health and rights (ibid.)
Methodology
This paper is based on data from a recent study of residential institutions (RI) for PWD [48, 49] conducted at request of the Greenlandic Department for Children, Youth and Families. Residents, staff, and managers were interviewed about quality of life, relational conditions and circumstances regarding sexuality and sexual rights. A qualitative study was considered the most appropriate way to develop an understanding of the unique experiences of PWD based on their own stories, together with the experiences of staff working in the RIs.
16 residents aged 17–62 years participated in the study. Out of the 16 residents who participated, eight were males and eight were females. One woman and two men had such difficulties understanding and answering the questions that their interviews were excluded from the study. Employees and managers helped identify residents who had a verbal language and thus could be interviewed.
Considering the small population of Greenland and the even smaller number of people living in RIs, to ensure the residents’ anonymity, we will not describe any further characteristics of the residents participating in the study.
29 managers and staff members participated in the study. Their job titles and functions varied and ranged from managers, social workers, health assistants and pedagogues to carpenters, hunters, and fishermen. Thus, half or over half of the employees at the RIs were in general uneducated or had professional training in fields other than education, care, and social work.
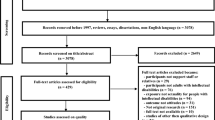
The 10 RIs that exist in Greenland—7 RIs and 3 satellites—have been invited to participate in the study of which two RIs never responded, and one RI agreed to participate, but several attempts of travelling there failed because of weather conditions and challenges with the flights. The RI was invited to participate by answering the questions by email, which they chose not to do. Thus, data were generated face-to-face in seven RIs in the following towns in Greenland: Ilulissat (1), Sisimiut (1), Maniitsoq (1), Nuuk (2), Paamiut (1) and Tasiilaq (1) (Fig. 1).

Overview of data collection in Greenland
The RIs have different specialisations and target groups ranging from RIs with only children and adolescents and RIs with only adults. Some RIs only have residents with mental disabilities such as ADHD and schizophrenia, while others have residents with mental, developmental, and physical disabilities.
The empirical data consists of qualitative semi-structured interviews as well as observations in the RIs. The interviews allowed participants to provide comprehensive answers to open-ended questions and to identify and explore issues of relevance to their experiences [50]. An interview guide covering quality of life, activities, collaboration and communication with relatives, sexuality, sexual rights, prevention of sexual assaults, and action plans in case of assault was developed. The questions were adjusted to the residents, the staff, and the managers, respectively. In this paper, we focus on the data concerning sexuality, sexual rights, and prevention of sexual assaults.
Examples of questions to the staff are: “Are you aware of sexual acts that should not take place between residents and employees?”, “Are there guidelines and action plans for what to do in the event of suspected sexual abuse and, if so, are these followed?”, and “Do you talk with the residents about sex?”.
Examples of questions to the residents are: “Do you know your rights regarding what others may and may not do with your body?”, “Do you sometimes talk to someone about sex?” and “Have you ever been touched on your body where you did not like it?”.
Interviews were carried out individually and took between 30 and 45 min with managers and employees while interviews with residents took 5–20 min.
Interviews were conducted in Danish or Greenlandic depending on the wishes of the interviewee. The residents chose whether an employee should be present during the interview. Most of the residents chose that. In some of the interviews, an employee helped the resident answer the questions, by helping them recall different situations of relevance to the question.
All interviews were audio-recorded to allow full transcripts of the interviews to be prepared for translation (from Greenlandic to Danish) and comprehensive data analysis. The participants were asked permission to make audio recordings, stating that the recordings would only be used for the purpose of the transcription. Participation was voluntary, and all participants were informed about the questions ahead of the interview, and how the answers would be used. They all signed a consent form.
In addition to the interviews, observations were conducted in the RIs. The observations were conducted by researchers over several days at different time slots. The focus of the observations was the general atmosphere, the physical surroundings (e.g., indoor climate), the interior design, facilities, and visible informative materials. Furthermore, interactions between; employees and residents, among employees and among residents were observed. An example of field notes is describing residents setting tables and employees cooking in the open kitchen. To the extent it was possible, field notes were written during the observations. If this was not possible, notes were written as soon as possible afterward.
When analysing the data, collaborative data analysis and thematic analysis was used [51, 52]. Collaborative analysis is a process in which there is a joint focus and dialogue among two or more researchers regarding a shared body of data, to produce an agreed understanding and interpretation, which brings a diversity of perspectives to the analysis [51]. Thematic analysis were used to identify, analyse and report patterns (themes) within the data related to the research question [52].Footnote 1
Findings
Sexuality as an Element of Daily Life
Talking About Sex
There is a great deal of variation in how managers and employees approach sex as a topic, both in terms of discussing it and in practice. Some employees indicate that they do not know whether residents have sex with each other or with others. At one RI, an interviewed employee does not think it is something they need to address, since according to the employee, the residents have no sexual needs. The employee explains that all residents are like family, and therefore do not think about having sex with each other, nor do they have sex with others:
-
Interviewer: Do staff members discuss residents’ sexual needs, for example?
-
Employee: They don’t. Nobody talks to them about it.
-
Interviewer: Do you have any guidelines regarding residents’ sexual needs and behaviour?
-
Employee: There are no guidelines for that, but they don’t do things like that. They just enjoy themselves.
-
Interviewer: So, none of the residents have relationships with each other?
-
Employee: No, I see them as family. That’s how they see themselves.
An employee from another RI explains:
-
No, we don’t talk so much to residents about sex. I haven’t experienced that much. But when residents talk about it, we can listen to them. I haven’t experienced it.
In RIs with young residents (under 20 years old), there are also varying ways of dealing with residents’ sexuality. One employee believes that the residents do not have a sexuality. An employee from another RI explains that they work to ensure that all sexual behaviour takes place in residents’ rooms and that a small book is read daily where the rule is stated that the resident must not touch other people. At a third RI, all residents have filled out a drawing of a body with colours indicating where the specific resident does not want to be touched and where it is acceptable to be touched in certain situations and always. These drawings are displayed with names, so both staff and residents always know how to respect each individual resident’s boundaries regarding touch. At the same time, staff members talk to residents who exhibit sexual behaviour and show interest in their own and others’ bodies.
In the remaining RIs, discussions and guidance regarding sexuality and sexual needs are more prevalent, although it still varies how much, and how easy or difficult it can be for staff and managers to discuss this topic—both with each other and with residents. An employee says:
-
If residents want to have intercourse for the first time, we tell them how it can be and what one can feel. But they always say that they feel good and have fun. I haven’t experienced anyone yet who didn’t feel good.
Another employee states that residents like to talk about sexuality and boundaries:
-
We’ve been talking about it with the residents for as long as I’ve been here. Unhealthy sexuality and healthy sexuality. The residents are good at talking about it ongoingly. They are open.
Several managers and employees express that it can be difficult for them to talk to both staff and residents about sex. Some managers explain that they try, but both they and the staff lack education on how to talk about sex and guide residents on how to experience their sexuality. An employee says:
-
The staff, for example, me, find it difficult to teach or explore possibilities for how to do it. It’s difficult for me.
A manager explains that they discuss sexuality and residents’ sexual needs during staff meetings, but both the manager and the employee lack the knowledge and tools to approach the topic:
-
It used to be a big taboo. But now it’s a bit more open. The residents must go into their own rooms, and they have their privacy in there. But we should get a bit more sex education within our field, I think. There are some points that are a bit too much for the staff. We also talk a lot about that. We train the residents in which areas of the body they are allowed to touch. But we should have more education about it. The residents sometimes need stimulation. They can’t say it, and they can’t signal it properly, but it comes naturally, with reactions and all sorts.
Another manager also mentions that both managers and staff lack knowledge about and education in sexuality and boundaries:
-
When we had a meeting here about a week ago, I could tell that the staff lack knowledge. It’s also been a long time since we had a course on sexuality. I mentioned that a couple of days ago, that we need it because of the boundaries and everything, we don’t know much about that.
Some of the interviewed residents had a bit of difficulty or didn’t want to talk about sexuality. Others gave very short answers, while a few used the interview to express thoughts and wishes regarding their sexual needs and wishes.
Residents’ Sexual Needs and Rights
A manager explains how they talk to residents about sex and practical and hygienic measures such as condoms and cleaning up after sex. However, there is still a strong emphasis on respecting residents’ privacy:
-
Some residents are couples, and some visit each other, even though they’re not couples. So we don’t know what they’re doing in the rooms, but the staff must constantly offer them: ‘Do you have enough condoms in your room? Do you have the things you need when you have intercourse?’ And then we talk to them about cleaning: where they should dispose of what they have used. But not the (act, ed.).
An employee says that residents often let them know when they visit each other to have sex. The openness among the residents helps the staff to be attentive that it is voluntary and pleasant for the involved residents:
-
It happens a lot on the weekends that residents visit each other in the units. If they want to have intercourse, they say that they close the door to their room so they can have a cozy time and enjoy themselves. We don’t really have problems with them overstepping each other’s boundaries, as they tell us all the time. They’re very open about what they’ve been doing.
A manager explains how a specific resident’s sexual behaviour has spurred the staff’s attention and action in relation to residents’ sexuality:
-
When the resident wakes up in the morning, he has an erection. So, we say, ‘Let us know when you’re ready,’ and leave him alone for a little while to get dressed. This resident made us more alert to sexuality. The staff discusses action plans at staff meetings. For example, we’ve put up mirrors in the rooms so residents can examine their bodies. And when they shower, we give them 5 or 10 more minutes if they need to be alone. Then they can feel their bodies.
On several RIs, some residents have sex toys that they occasionally use. Several managers and employees thus explain how residents can express when they want to use their sex toys or aids. What is typically mentioned includes dildos, sex dolls, or silicone vaginas. An employee talks about a resident who doesn’t have explicit verbal language. The staff can sense when the resident wants to use their sex doll, and then they place the doll next to the resident’s bed at bedtime. A few mention that some residents watch pornography and other sexually related material on their private phones or tablets.
In some residential facilities, some residents who have sex with people from the town. Some have a steady sex partner, while others have different sex partners. At a few residential facilities, employees mention that residents can have visits from external sex partners in their rooms on the residential facility.
The residents were asked if they knew the rules about what they and others are allowed to do with their bodies. Not all residents could answer this question. One resident responded that they don’t talk to the staff about sex and don’t know if there are rules about what is allowed or not. They also don’t know how to say no if something they don’t want is happening, but they’ve never experienced being touched in ways they didn’t like. Another resident knew that there are rules but had difficulty answering how to set boundaries if they were to experience something they didn’t like. This same resident also mentioned not talking to anyone about sex and not wanting to discuss it.
Some of the interviewed residents have a clear sense of how to set boundaries. A resident clearly indicated knowing how to set boundaries by saying "no." Another resident referred to the staff when asked about rules and rights related to their body:
-
Interviewer: Do you know if there are rules here about how people can touch each other?
-
Resident: The staff knows the rules better.
One resident received assistance from the present caregiver to remember what is discussed at the institution:
-
Interviewer: Do you know if there are rules here about how people can touch each other?
-
Resident: No.
-
Employee: Can’t you remember these (points to drawing)?
-
Resident: I’ve seen it, but I don’t do it.
-
Resident: Yes. There are drawings on the board.
While most of the interviewed residents find it somewhat difficult to talk about sex, rights to their own body, and boundaries, some don’t find it as difficult. One resident, for example, is willing to talk about sex but also seeks assistance from the present staff member:
-
Interviewer: Do you know your rights about what others are allowed to do with your body?
-
Resident: We talk about using condoms if we’re going to have intercourse.
-
Interviewer: Do you know if there are rules about how people can touch each other?
-
Staff to resident: What is it you’re not allowed to do there? It can be intercourse or… Can you set boundaries for how you’re touched?
-
Interviewer: Have you ever been touched in a way you didn’t like?
-
Resident: No.
Most of the residents don’t talk about their sexual needs during the interview, and most of them, as mentioned, don’t have a strong desire to discuss sex and sexuality. However, the interview situation leads some residents to express needs they don’t usually talk about. An example is a resident who wants to say something more after the interview is over:
-
Interviewer: I don’t have any more questions. Is there anything else you’d like to tell me?
-
Resident: I’d like to have an inflatable doll, but I don’t know where to get one.
-
Interviewer: Can you talk to the staff about wanting such a doll?
-
Resident: I don’t know where to get one, but I’d like to have one.
-
Employee: It’s only now you’re voicing it. Now that we know, we can address it. The staff can help you, like they do with someone else. You’ll get assistance with it.
Another resident wants to have a sexual partner:
-
Resident: Sometimes I feel like it. I’d like to try it, but I don’t have anyone to do it with. I don’t have anyone to visit (for sex).
Sexual Abuse and Violations
Knowledge and Suspicion of Sexual Abuse and Violations
Except for one RI, managers and/or staff members are aware of instances or suspicions of sexual harassment and abuse against residents at some point. Some of these incidents occurred a long time ago, while others have happened within the past year. Some known cases involve incidents at other RIs, while others are specific to the facility where the interviewees work. In some cases, staff members have been involved, while in others, individuals from the local community are implicated.
All interviewees were asked whether they know how to respond if they suspect that something of a sexual nature is occurring that shouldn’t be. Some participants outline a process of notifying those involved to cease the activity and, if necessary, involving the police.
There have been cases where individuals in positions like janitors have caused problems due to attracting residents. One facility has decided to eliminate such positions to avoid similar issues.
In some situations, individuals from outside the facility have been implicated in sexual harassment or abuse cases involving residents. There are cases where these external individuals have been reported to the police at the request of the residents.
When incidents have occurred, they are reported to relevant authorities, and actions are taken to address the situation. This may include involving the police, firing staff members involved, and ensuring the safety of the residents.
Residents occasionally meet individuals from the local community, especially through online platforms, which can sometimes lead to risky situations involving sexual harassment. In such cases, the RI staff intervenes, educates the residents about safe online behaviour, and involves the police if necessary.
A single resident participating in the study has experienced abuse in the past. This doesn’t come up as a direct response to the questions but is mentioned right after when the resident mentions preferring help from a female staff member when taking a bath because of experiences with sexual abuse when the resident lived in another town before moving to the RI.
Prevention
Prevention of sexual offenses in the RIs is carried out through various measures. As mentioned above, in some places, there is significant openness among the residents when it comes to discussing sex and sexuality with the staff. This provides the staff with a good opportunity to understand the individual resident’s needs, as well as whether they require assistance in setting boundaries with others or in recognizing and respecting others’ boundaries.
Several employees and managers explain how they discuss these matters with the residents:
-
There was a resident who touched all the ladies. We talked to the person and helped them realize that it’s not allowed. Some female residents who might find male staff members attractive. We discuss boundaries with these residents and what is not allowed. And we also let the residents know that staff members are not allowed to do that either.
One of the newer preventative measures that have been adopted and implemented in all the RIs is that there should be at least two staff members on the night shift, and there should be two staff members present during bathing and, for example, changing diapers. In many situations, it can be overwhelming and uncomfortable for the resident if only one staff member is needed to assist them in bathing. For pedagogical and ethical reasons, several RIs have chosen an indirect way to implement this measure. One employee explains:
-
One should be present and assist, while the other staff member should simply be able to see and hear what’s happening in the background. We must also respect the residents. The person should not feel attacked or anything like that. The staff have also learned not to touch the resident directly during bathing, but to place the resident’s hand underneath (demonstrates how they assist the residents in washing themselves in the genital area, ed.).
A manager at a residential facility where many residents wear diapers, which are changed by staff, explains that employees should inform each other when they need to change a resident’s diaper:
-
We’ve talked a lot in the staff group about how to do in diaper-changing situations. It should be private, like in a bathroom, and of course, consider the resident. But the other employees need to know that we’re changing a diaper. We’ve tried the thing where two people need to be present when changing a diaper, but sometimes we’ve noticed that the resident reacts. Well, that’s not very good. We need to think about that too.
Another manager mentions that due to staff shortages, it is not always possible to have as many employees at work at the same time as would be ideal. If there are only two staff members at work, and one of them needs to attend to a specific resident or handle something practical, the other staff member might find themselves in a situation where they must help a resident with tasks like using the toilet or bathing without their colleague being able to assist. Another manager explains that it can be difficult to find substitutes when someone is sick, and occasionally, a staff member might be alone at work during the night.
Some residents may initiate attempts to establish sexual contact with other individuals, including staff members. Several managers and employees describe how they can reject residents’ sexual advances in ways that convey that such behaviour is unacceptable without scolding or shaming them. One manager is particularly aware that residents might be attracted to staff members, but staff members might also be attracted to residents. Addressing this issue openly is crucial for preventing sexual offenses and interactions between residents and staff:
-
We need to protect the residents. The residents are good at attracting adult sexual attention. It’s not only the staff that can be attractive; the residents are also good at attracting the staff. So, we discuss continuously what the staff should do if they sense that something is going on. They should talk to department managers or colleagues: "I feel this way." We’d like to have a sexologist visit to discuss various matters with the residents and staff.
Another manager explains that certain female residents can be boundary-pushing when it comes to male staff members, who must be adept at setting boundaries regarding advances:
-
The first time I experienced it was with two residents making sexual advances towards staff members. One must control their attraction to male workers. Their sexual mindset is quite expansive. Staff members must be able to set boundaries for the residents. But sometimes—even though residents know it’s prohibited—they keep trying.
In certain cases, staff members need to protect and guide residents who initiate situations where they might be exposed to offenses and abuse. An employee talks about a resident who posts naked pictures of herself on social media:
-
We have a resident who posts pictures. Then she gets in touch with people we don’t know from town. So, we got in touch with her parents to collaborate on addressing it so that she doesn’t send pictures out, even though she still has her mobile. It’s our duty to protect the residents.
Another employee talks about a resident who sometimes has negative experiences with sex with a man in town:
-
When the resident comes home, she says she had a nice day and visited the man she sees. Very rarely does she come home upset, saying, "He had rough intercourse with me, he did it roughly." We tell the resident to say that she doesn’t like it and to stop visiting him. The resident’s daily life and mood fluctuate greatly. From one day to the next, she’s no longer angry with him and goes back to him. It’s a constant cycle.
A manager explains that residents who are developing and discovering their sexuality or who have previously been subjected to abuse can, in some cases, exhibit boundary-pushing behaviour toward other residents. When asked whether the manager has experienced residents being boundary-pushing towards each other at the RI, the manager responds:
-
Yes, especially the young ones when they start developing and experimenting a bit with themselves. We have plenty of that. We tell the residents that such behaviour is not acceptable. They can’t do that. Well, most of them are very behind in their development for their age. Some residents have also been abused before. If we notice that residents might be about to cross other residents’ or staff members’ boundaries, we ask them to go to their rooms for a moment. Then we talk about how the staff should handle it. Establish some boundaries: "You can’t do this." In a healthy way, of course. It’s an acknowledging pedagogy.
Rules, Policies and Guidelines
There is a significant variation across different RIs in terms of their familiarity with rules and guidelines, as well as whether there are specific local guidelines concerning residents’ sexual rights and protection against abuse and sexual misconduct. Some staff members are uncertain about the presence of guidelines, while others are aware of specific policies and protocols for handling sexual behaviour and suspicions of abuse. Different RIs have varying levels of local policies and guidelines in place. Some have established their own policies and procedures, while others rely on government guidelines. These policies may include reporting procedures, documentation, and measures for dealing with incidents or concerns related to sexual behaviour.
All participants, including managers and staff members, are aware of the new guidelines regarding the number of staff members during night shifts and situations involving diaper changes and bathing. Regarding guidelines for how staff and management should handle residents’ sexuality and sexual needs more broadly, there is a significant variation in terms of existing guidelines and whether sexuality is even addressed in daily routines.
Discussion
The Connection Between Openness, Taboo, and Sexual Rights
The literature on sexuality and attitudes towards sex in Greenland does not give us any clear answers to whether it is taboo or not. While foreigners’ historic accounts of Greenlanders emphasise otherness, difference, and exoticism with references to sexuality [40, 44], it is hard to find evidence of how Greenlanders themselves felt about the topic and the practices around sex in historic times. Not surprisingly, newer studies of the topic show great variations in attitudes towards talking about sex as well as sexual education and guidance within family and community [47].
This study conducted in RIs for PWD shows the same spectrum of variations as is seen in research on parents’ ability and willingness to talk to their youth about sex and sexual health and rights [47]. Thus, many employees in RIs talk to residents about sex while some RI residents are not talked to about sexuality at all. In some RIs, the staff mainly focus on what is not allowed for the resident to do or for others to do to the resident. In a few RIs residents are guided more openly and educated on personal boundaries as well as on how to live out their sexuality and fulfil their sexual needs.
There is great variation in whether residents express their sexuality and whether they do it alone with aids or with sex partners. In most residential facilities, some residents have sex toys, and staff help provide access to or give guidance on using them. The study shows no indication of a relationship between residents’ access to sex toys and staff’s openness or comfortability with talking about sex and sexuality.
The study shows that the lack of knowledge about how to guide and talk to residents about sexuality and sexual rights is a widespread problem and many managers and employees request more education in this area. In this way, employees in RIs reflect research on parents and their ability to talk to youth about sex. They too ask for more education and for help to learn how to talk to and educate the residents about sex and sexual matters.
The Connection Between Openness, Taboo, and Prevention of Sexual Abuse
The widespread knowledge of both past and recent incidents involving sexual harassment and abuse against residents in these facilities highlights the prevalence of such issues. Residents in these settings are particularly vulnerable to experiencing sexual harassment and abuse, emphasising the importance of addressing this concern and implementing measures to protect their rights and safety.
In many residential facilities, managers and staff members find that certain residents can be sexually assertive towards the staff and need to be shown and informed that a sexual relationship between residents and staff members is not allowed. A couple of managers emphasize that staff members might also need reminders about this. Some residents seek out sexual experiences with people in town, which could potentially become offensive and boundary-pushing for the residents.
In relation to guidelines about what residents are allowed and not allowed to do regarding sexual behaviour, many responses focus on what residents are not allowed to do. They are not allowed to exhibit sexual behaviour in common areas, touch themselves, each other, or others in sexual ways, say certain things, etc. In some RIs, there are pictograms in common areas showing what is not allowed.
Overall, the knowledge and implementation of rules and guidelines regarding residents’ sexual behaviour and protection from abuse vary widely among the interviewees and residential facilities. The presence and effectiveness of such guidelines seem to depend on factors such as facility managership, training, collaboration with authorities, and the overall organizational culture.
We do not have evidence of a direct relationship between the openness of staff to talk to residents and each other about sex and the risk of sexual harassment and abuse. However, it seems likely that there is a better chance of preventing or stopping sexual harassment and abuse of residents when there is an institutional culture of openness about these matters. If it is normalised to talk about sex, sexual likes and dislikes and sexual experiences it must be easier for residents to express if they are experiencing something that is pushing their boundaries. Sometimes residents might get sexual attention from an employee that they enjoy, but which is not allowed. In such cases, colleagues must know what is right or wrong and dare to interfere to stop what is going on. Knowing and daring this requires knowledge as well as trust and an institutional culture of talking about it.
Conclusion
We set out to explore in which ways attitudes towards talking about sex and sexual matters influence practices regarding sexuality, sexual rights, and sexual abuse in RIs for PWD in Greenland. Our study shows that in some RIs, residents’ sexual needs and rights are suppressed by staff’s perception of the residents as not having a sexuality. We also found that residents receive much more guidance regarding sex and sexual rights when staff are not too uncomfortable talking about sex as a normal part of daily life and of being human. Sexual harassment and abuse as well as inappropriate and illegal contact—yet appreciated by residents—occur at times regardless of the local institutional culture. However, it seems to be easier to detect and stop such actions and violations in RIs with an openness to talk about sex and sexual health and rights.
References
Braathen, S.H., Carew, M.T., Chiwaula, M., Rohleder, P.: Physical Disability and Sexuality, Some History and Some Findings. In: Hunt, X., Braathen, S.H., Chiwaula, M., Carew, M.T., Rohleder, P., Swartz, L. (eds.) Physical Disability and Sexuality, pp. 27–51. Palgrave Macmillan, Cham. (2021). https://doi.org/10.1007/978-3-030-55567-2_2
Giulio, G.D.: Sexuality and people living with physical or developmental disabilities: a review of key issues. Can. J. Hum. Sex. 12, 53–68 (2003)
Tilley, C.M.: Sexuality in women with physical disabilities: a social justice or health issue? Sex. Disabil.Disabil. 14, 139–151 (1996)
Milligan, M.S., Neufeldt, A.H.: The myth of asexuality: a survey of social and empirical evidence. Sex. Disabil.Disabil. 19, 91–109 (2001)
Baynton, D.C.: ‘These pushful days’: time and disability in the age of eugenics. Health Hist. 13, 43–64 (2011)
Cuskelly, M., Gilmore, L.: Attitudes to sexuality questionnaire (individuals with an intellectual disability): scale development and community norms. J. Intellect. Dev. Disabil.Disabil. 32, 214–221 (2007)
Gilmore, L., Chambers, B.: Intellectual disability and sexuality: attitudes of disability support staff and leisure industry employees. J. Intellect. Dev. Disabil.Disabil. 35, 22–28 (2010)
Hunt, X., et al.: Withdrawn, strong, kind, but de-gendered: non-disabled South Africans’ stereotypes concerning persons with physical disabilities. Disabil. Soc. 33(10), 1579–1600 (2018)
United Nations: United Nations Convention on the Rights of Persons with Disabilities. United Nations (2006)
Shah, S.: “Disabled people are sexual citizens too”: supporting sexual identity, well-being, and safety for disabled young people. Front. Educ. 2, 46 (2017)
Shakespeare, T., Gillespie-Sells, K., Davies, D.: The Sexual Politics of Disability: Untold Desires (1996)
McCabe, M.P., Cummins, R.A., Reid, S.B.: An empirical study of the sexual abuse of people with intellectual disability. Sex. Disabil.Disabil. 12, 297–306 (1994)
Reiter, S., Bryen, D.N., Shachar, I.: Adolescents with intellectual disabilities as victims of abuse. J. Intellect. Disabil.Disabil. 11(4), 371–387 (2007)
Steffensen, T., Nielsen, N.: Voldsofre med Psykiske og Kognitive Handicap—En Undersøgelse af Barrierer i Straffesager. Institut for Menneskerettigheder (2020)
Lesseliers, J.: A right to sexuality? Br. J. Learn. Disabil.Disabil. 27, 137–140 (1999)
United Nations: Standard Rules on the Equalization of Opportunities for Persons with Disabilities (1993)
Cunningham, M., Sena, P.K.: Study on the Situation of Indigenous Persons with Disabilities, with a Particular Focus on Challenges Faced with Regard to the Full Enjoyment of Human Rights and Inclusion in Development. United Nations. Economic and Social Council (2013).
Engen, M., Ibsen, D.L.: Litteraturstudie: Overgreb Mod Piger og Kvinder med Udviklingshandicap (2022)
United Nations: Report of the Office of the United Nations High Commissioner for Human Rights. Thematic Study on the Issue of Violence Against Women and Girls and Disability (2012)
Niederbuhl, J.M., Morris, C.D.: Sexual knowledge and the capability of persons with dual diagnoses to consent to sexual contact. Sex. Disabil.Disabil. 11, 295–307 (1993)
Held, K.R.: Ethical aspects of sexuality of persons with mental retardation. Sex. Disabil.Disabil. 4, 237–243 (1992)
Watson, S., et al.: Sex education. In: Griffiths, D.M. (ed.) Ethical Dilemmas: Sexuality and Developmental Disability, pp. 175–225. NADD Press, New York (2002)
Avci, Ö.H.: It’s a taboo: women with disabilities applying for psychological counseling due to romantic relationship and sexual problems. Sex. Disabil.Disabil. 41, 335–355 (2023)
East, L.J., Orchard, T.R.: Somebody else’s job: experiences of sex education among health professionals, parents and adolescents with physical disabilities in Southwestern Ontario. Sex. Disabil.Disabil. 32, 335–350 (2014)
Payne, D.A., et al.: Physically disabled women and sexual identity: a PhotoVoice study. Disabil. Soc. 31(8), 1030–1049 (2016)
WHO/UNFPA: Promoting sexual and reproductive health for persons with disabilities: WHO/UNFPA guidance note. World Health Organization, UNFPA, Geneva (2009)
Ahlmark, N., et al.: Sundhedsprofil for Socialt Udsatte Grønlændere i Danmark. SUSY UDSAT. [Health Profile for Socially VULNERABLE GREENLANDERS in Denmark. SUSU UDSAT]. Statens Institut for Folkesundhed [National Institute of Public Health], SDU: København (2019)
Statistics Greenland: Grønland i Tal [Greenland in numbers] 2023, Grønlands Statistik [Statistics Greenland] (2023)
Senftleber, N.K., et al.: Diet and physical activity in Greenland: genetic interactions and associations with obesity and diabetes. Appl. Physiol. Nutr. Metab.Nutr. Metab. 46(8), 849–855 (2021)
BDO: Evaluering af Opgaveoverdragelse på Handicapområdet [Evaluation of Task Delegation on the Disability Area]. Binder Dijker Otte & Co, Zaventem (2014)
Naalakkersuisut: Inatsisartutlov nr. 13 af 12. Juni 2019 om Støtte Til Personer med Handicap, Grønlands Selvstyre, Editor (2019)
Tilioq: Tilioq Aallaannaqaaq Kommune Kujallermut Angalanermik Nalunaarut 2019. Tilioq Søsætter Kajakken—Rejserapport Kommune Kujalleq 2019. [Tilioq Launches the Kayak—Travel Report Kujalleq Municipality 2019]. Tilioq (2019)
Tilioq: The Spokesperson for People with Disabilities in Greenland. 30-08-2023; Available from: https://tilioq.gl/en/
Disability—Status in Grønland: Institut for Menneskerettigheder & Grønlands Råd for Menneskerettigheder (2019)
Knigge, M., Grønbæk, J.S.: Forvist Til Forsorg: Grønlændere Med Handicap Nedsendt Til Danmark [Exiled to Welfare: Greenlanders with Disabilities Sent to Denmark] (2008)
Arnfjord, S., Jonsson, A.I.H., Daverkosen, D.: Holdninger Til Handicap 2020—En Undersøgelse af Befolkningens Holdninger Til Personer med Handicap i Samfundet og på Arbejdsmarkedet [ATTITUDES TOWARDS DISABILITY 2020—A Study of the Population’s Attitudes Towards Individuals with Disabilities in Society and in the Labour Market]. Tilioq og Ilisimatusarfik (2020)
Homøe, A., et al.: Sexual and reproductive health in Greenland: evaluation of implementing sexual peer-to-peer education in Greenland (the SexInuk project). Int. J. Circumpolar Health J Circumpolar Health 74(1), 27941 (2015)
Riel, J.: Myter og Sagn fra Grønland. Første og Anden Samling (Myths and Legends from Greenland. First and Second Edition). Nørhaven Book, Viborg (2004)
Arnfred, S., Pedersen, K.B.: From female shamans to Danish housewives: colonial constructions of gender in Greenland, 1721 to ca. 1970. NORA Nord. J. Fem. Gend. Res. 3(4), 282–302 (2015)
Maegaard, M., Mortensen, K.M.: Meeting the Greenlandic people: mediated intersections of colonial power, race and sexuality. Tilburg Pap. Cult. Stud. 218, 1–9 (2018)
Seiding, I.: Colonial categories of rule—mixed marriages and families in Greenland around 1800. Kontur Tidsskr. Kulturstudier 22, 56–65 (2011)
Rink, E., et al.: An ecological approach to understanding women’s reproductive health and pregnancy decision making in Greenland. Health Place 77, 102868 (2022)
Marcussen, P.V., Rendal, J.: A study of syphilis and sexual habits in Greenland. Am. J. Syph. Gonorrhea Vener. Dis.Syph. Gonorrhea Vener. Dis. 34, 144–152 (1950)
Vanek, S.B., Rygaard, J.: To “lure on the gentle reader” approaching historical representations of gender and sexuality in the Arctic through Rockwell Kent’s Salamina. Sibirica 22(1), 56–81 (2023)
Gesink, D., et al.: Developing a culturally competent and socially relevant sexual health survey with an urban arctic community. Int. J. Circumpolar Health 69, 1 (2010)
Gesink, D.C., et al.: Mycoplasma genitalium presence, resistance and epidemiology in Greenland. Int. J. Circumpolar Health 71(1), 18203 (2012)
Rink, E., Montgomery-Andersen, R., Anastario, M.: “Today we are not good at talking about these things”: a mixed methods study of Inuit parent/guardian-youth sexual health communication in Greenland. Int. J. Indig. Health 10(1), 84–99 (2014)
Nørtoft, K., et al.: Beboerperspektiver på Døgntilbud Til Mennesker med Handicap. Statens Institut for Folkesundhed, SDU, København (2023)
Nørtoft, K., et al.: Forhold Omkring Seksualitet og Seksuelle Overgreb på Døgntilbud Til Mennesker med Handicap. Statens Institut for Folkesundhed, SDU, København (2023)
Kvale, S., Brinkmann, S.: Interview—Det Kvalitative Forskningsinterview som Håndværk, vol. 3. Gyldendal (2015)
Cornish, F., Gillespie, A., Zittoun, T.: Collaborative analysis of qualitative data. In: Flick, U. (ed.) The SAGE Handbook of Qualitative Data Analysis, pp. 79–93. SAGE Publications Ltd., Thousand Oaks (2014)
Braun, V., Clarke, V.: Using thematic analysis inpsychology. Qual. Res. Psychol. 3, 77–101 (2006)
Acknowledgements
We wish to thank all the residents, staff members and managers of the RIs for participating in the study and share their reflections and experiences with us. We also wish to thank our colleagues in the project, Sonja Sørensen, Bonnie Jensen, Ivalu Olsen, Else Jensen and Steven Arnfjord.
Funding
Open access funding provided by University of Southern Denmark. The study was funded by The Greenlandic Department of children, youth, and families.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Ethical Approval
All procedures performed in the study involving human participants were in accordance with the ethical standards of the national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Ethical approval was provided by the Science Ethics Committee of Greenland (2023-21528).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nørtoft, K., Rubin, S.E. Let’s Talk About Sex! Perspectives from People with Intellectual and Developmental Disabilities and Caregivers in Residential Institutions in Greenland. Sex Disabil 42, 225–242 (2024). https://doi.org/10.1007/s11195-023-09828-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11195-023-09828-5