
Abstract
Background
The number of published articles on Patient-Reported Outcomes Measures (PROMs) in Coronary Heart Disease (CHD), a leading cause of disability-adjusted life years lost worldwide, has been growing in the last decades. The aim of this study was to identify all the disease-specific PROMs developed for or used in CHD and summarize their characteristics (regardless of the construct), to facilitate the selection of the most adequate one for each purpose.
Methods
A systematic review of reviews was conducted in MEDLINE, Scopus, and the Cochrane Database of Systematic Reviews. PROQOLID and BiblioPRO libraries were also checked. PROMs were classified by construct and information was extracted from different sources regarding their main characteristics such as aim, number of items, specific dimensions, original language, and metric properties that have been assessed.
Results
After title and abstract screening of 1224 articles, 114 publications were included for full text review. Finally, we identified 56 PROMs: 12 symptoms scales, 3 measuring functional status, 21 measuring Health-Related Quality of Life (HRQL), and 20 focused on other constructs. Three of the symptoms scales were specifically designed for a study (no metric properties evaluated), and only five have been included in a published study in the last decade. Regarding functional status, reliability and validity have been assessed for Duke Activity Index and Seattle Angina Questionnaire, which present multiple language versions. For HRQL, most of the PROMs included physical, emotional, and social domains. Responsiveness has only been evaluated for 10 out the 21 HRQL PROMs identified. Other constructs included psychological aspects, self-efficacy, attitudes, perceptions, threats and expectations about the treatment, knowledge, adjustment, or limitation for work, social support, or self-care.
Conclusions
There is a wide variety of instruments to assess the patients’ perspective in CHD, covering several constructs. This is the first systematic review of specific PROMs for CHD including all constructs. It has practical significance, as it summarizes relevant information that may help clinicians, researchers, and other healthcare stakeholders to choose the most adequate instrument for promoting shared decision making in a trend towards value-based healthcare.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Different initiatives have converged on the importance of the patients’ perspective in the improvement of healthcare. The Institute of Medicine (2001) [1] identified patient-centered care as one of the six domains of high-quality healthcare, wherein patient-centered care supports clinicians in “attending to their patients’ physical and emotional needs and maintaining or improving their quality of life.” The Patient-Centered Outcomes Research Institute [2] emphasizes the goal of “focusing on outcomes that people notice and care about such as survival, function, symptoms, and health-related quality of life.” The American Heart Association (AHA, 2013) [3] states that Patient-Reported Outcome Measures (PROMs) implementation in clinical settings has “the potential to support clinical care, evaluate healthcare quality, quantify an important component of procedural appropriateness, identify patients for prognostic discussions and serve as a foundation for shared medical decision making.”
A patient-reported outcome has been defined [4] as “a measurement based on a report that comes directly from the patient (i.e., study subject) about the status of a patient’s health condition without amendment or interpretation of the patient’s response by a clinician or anyone else.” PROMS are standardized questionnaires that collect information on health outcomes directly from patients and cover a wide variety of constructs, including symptoms, functional status, and Health-Related Quality of Life (HRQL) among others [5]. HRQL is one of the constructs most commonly associated with PROMs, and it is a term referring to the health aspects of quality of life, generally considered to reflect the impact of disease and treatment on disability and daily functioning; it has also been considered to reflect the impact of perceived health on an individual's ability to live a fulfilling life [6]. PROMs should ideally undergo psychometric validation to ensure that they accurately reflect the outcomes they purport to cover, and that they are reliable and can assess changes over time.
Coronary Heart Disease (CHD) has been the leading cause of disability-adjusted life years lost worldwide since 1990 in people over 50 years old [7]. For patients with CHD, the principal treatment goals are to reduce cardiac events, eradicate angina, and optimize quality of life [8]. In recent decades, the number of published articles reporting the use of PROMs in CHD has been growing, following the global tendency in most chronic pathologies [9]. The proportion of cardiovascular trials evaluating quality of life has increased over time: from 0.34% in 1980 to 3.6% in 1997 [10], to 14% in 2009 [11]; whereas patient-centered outcomes were reported in 29% of cardiac surgery trials performed between 2010 and 2014 [12].
Broadly, PROMs fall into two main categories: condition-specific and generic. The latter measures health concepts that are relevant to a wide range of patient groups, enabling aggregation and comparisons across varied conditions and settings. Condition-specific PROMs capture elements of health relevant to a particular group of patients [13], which in the case of the present review will be CHD patients. Given the growing interest in these instruments, there are several reviews of the main characteristics of some of the most widely used PROMs for CHD, but none have examined all the available instruments [12, 14,15,16,17,18,19,20].
These reviews have focused on heart disease in general, on specific heart conditions or on particular constructs (such as symptoms or HRQL) [16]. A review of instruments for patients undergoing elective coronary revascularization identified 26 cardiovascular-specific PROMs [18]. Reviews for specific constructs in CHD have been mainly centered on HRQL [10,11,12,13,14], showing that mostly generic instruments, such as the SF-36 or the EQ-5D, have been used in this pathology. A review centered on symptom scales [20] found 36 different instruments (both generic and specific measures) for all types of cardiovascular populations, including 15 for CHD and angina pectoris. A recent scoping review of validated PROMs including more than one domain, either developed or specifically modified for patients with heart disease, found 9 specific instruments for ischemic heart disease and 5 more applied to all types of heart disease [18].
These numerous reviews result in a kind of puzzle, with partial information and overlaps which make it difficult to obtain the global picture. Therefore, the aim of this study was to identify all the disease-specific PROMs (regardless of the construct) developed for or used in CHD and to describe their main characteristics by conducting a systematic review of reviews. The review protocol is registered in the International Prospective Register of Systematic Reviews database (PROSPERO CRD42021248504).
Methods
A systematic review of reviews was conducted following the same process as systematic reviews of primary research, but where the units of analysis were reviews rather than individual studies. Following Cochrane recommendations of selecting a minimum of two databases, searches were performed in three electronic databases: MEDLINE, Scopus, and the Cochrane Database of Systematic Reviews. We selected MEDLINE because most of the publications on PROMs are in the field of medical journals and Scopus because it is multidisciplinary and covers other areas. Additionally, we searched in two specialized libraries: PROQOLID (Patient-Reported Outcomes and Quality of Life Instruments Database), and BiblioPRO (a virtual library of PROMs in Spanish). As recommended by the Cochrane Database of Systematic Reviews, the reference lists of relevant studies were also checked to find other potential eligible studies [21].
We applied a comprehensive search strategy developed by experts in Patient-Reported Outcomes and experts in Systematic Reviews in cardiology, seeking to identify published reviews mentioning disease-specific PROMs for CHD populations. For the electronic databases, we used Boolean search methods to identify relevant papers. The search strategy was limited to “reviews” or “systematic reviews” (see supplementary material).
All the identified review articles were included, since the date of each database's inception until March 2021, regardless of whether they were systematic or not. The search was not restricted to language or timeframe.
The inclusion criteria were (1) systematic review or reviews; and (2) providing information about PROMs specifically designed for CHD or, in the case of being designed for heart diseases in general, having been applied and/or validated in patients with CHD; (3) including any type of construct measured: health-related quality of life, symptoms scales, functional status or activities of daily living, and psychological- or social-related construct; (4) instruments that are domain-specific (such as depression, anxiety, self-efficacy, or social support related to CHD) or treatment-specific (for example, coronary artery bypass grafting—CABS—or percutaneous coronary intervention—PCI).
The following exclusion criteria were applied: (a) review or systematic review reporting on generic PROMs applied to CHD (for example, SF-36 or EQ-5D); and (b) review or systematic review of PROMs specifically developed for children or adolescents (age under 18 years).
Two independent reviewers applied inclusion and exclusion criteria to select titles and abstracts, and a single reviewer performed full text and data extraction. All the PROMs identified were categorized according to the construct measured. In case of discrepancy, consensus was reached with the help of a third expert.
Data extraction and analysis
A data extraction form was developed to collect the PROMs identified, stratified by construct: HRQL, symptoms, functional status, and others.
For each identified PROM, we located the publication reporting the instrument development and we collected information about their general characteristics: author, year, country of publication, and bibliographic reference of the original development; aim (including the characteristics, conditions, or procedure of the population for which the PROM was developed, e.g., coronary artery bypass grafting, congestive heart failure, or myocardial infarction); number of items and dimensions; and the original language and existence of other versions. To identify the linguistic adaptations available, we searched in the PROQOLID and BiblioPRO libraries or the instrument's website. If alternative versions of a PROM were available (for example short forms or pre- and post-treatment forms), they were considered as part of the original. Additionally, we performed a search in PubMed and Scopus databases using the name of the instrument as a search term to find publications of their use within the last 10 years (from March 2011 to March 2021).
For each instrument, we reviewed if there was available information on the main metric properties in patients with CHD: reliability (including reproducibility or test–retest reliability and internal consistency), validity (content, criterion, or construct validity), and sensitivity to change (responsiveness). For information on the metric properties, we considered information on both the original instrument and the linguistic adaptations.
The review was conducted and has been reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [22].
Results
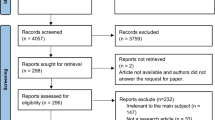
The search strategy yielded 1131 review articles, and 93 more were added from other sources such as manual reference screening (Fig. 1). After the title and abstract screening, 114 publications were included in the full text review. From these reviews, we identified 56 PROMs specifically developed to be applied in patients with CHD: 21 measuring HRQL (1 of them measuring both symptoms and HRQL, the “Speak from the Heart” instrument), 12 symptoms scales, 3 instruments measuring functional status (1 of them measuring both functional status and symptoms, the Cardiovascular Limitations and Symptoms Profile), and 20 focused on other constructs.

Systematic Review Flow Chart. *One instrument (CLASP) could be included in the “Functional status” or “Symptoms scale” constructs
Characteristics of PROMs assessing symptoms and functional status are summarized in Table 1, ordered by the construct measured (symptoms or functional status) and year of publication. Of the 12 symptoms scales identified, three were specifically designed ad hoc for a particular study without any psychometric validation. Only the following 5 instruments have been included in a published study in the last 10 years: Rose Angina Questionnaire (RAQ), Symptoms of Acute Coronary Syndromes Inventory (SACSI), McSweeney Acute and Prodromal Myocardial Infarction Symptom Survey (MAPMISS), Cardiac Symptom Survey (CSS), and Cardiovascular Limitations and Symptoms Profile (CLASP). For these five instruments there is information at least on their reliability and construct validity. However, no sensitivity to change data has been reported. All five instruments have two or more language versions. The RAQ deserves a special mention for being the most widely used in epidemiological surveys since its development in 1962, and being adopted by the WHO [23]. The most common symptom assessed among these symptoms scales is chest pain, followed by dyspnea or fatigue.
Only two of the identified instruments focus on functional status: Seattle Angina Questionnaire (SAQ) and Duke Activity Status Index (DASI). Both were specifically developed for CHD patients, although DASI has nowadays been extended to other conditions. The SAQ, a 19-item questionnaire developed for assessing angina pectoris, has been translated into 54 languages, and a short form is available with seven items. The DASI has 12 items and is available in several languages. Both instruments have evidence on their metric properties: reliability, validity, and responsiveness (Table 1).
Table 2 shows the characteristics of PROMs assessing HRQL, ordered by year of publication between 1988 and 2019. The first ones were developed in Scandinavia for patients with CHD, and most were originally developed in English (11 out of 21 are from UK, USA, Canada, or Australia). Four out of these 21 PROMs were specifically designed for measuring HRQL of patients receiving surgical, percutaneous revascularization or antiarrhythmic medications: Questionnaire for coronary artery bypass grafting, Coronary Revascularization Outcomes Questionnaire (CROQ), Monash University Cardiac Patient-reported Outcome Measure (MC-PROM), and Cardiac Arrhythmia Suppression Trial (CAST). The number of items included in HRQL instruments varies widely, from 14 (HeartQoL), to 70 (Ferrans and Powers QLI-cardiac version). Although the Chronic Heart Failure (CHF) questionnaire was originally designed for heart failure and there are many country-specific versions, we have only included the version that was modified to evaluate HRQL in CHD [24].
Among the questionnaires identified for measuring HRQL in CHD patients, the most used worldwide are Angina Pectoris Quality of Life Questionnaire (APQLQ), QLI-cardiac version, the MacNew, Cardiac Health Profile (CHP), Myocardial Infarction Dimensional Assessment Scale -35 (MIDAS-35), CROQ, and HeartQoL. They all have several linguistic versions and have appeared in published studies in the last ten years (except for the APQLQ). In addition, information on reliability, validity, and responsiveness has been reported for all of them.
The APQLQ was developed in 1988 in Sweden to assess the impact of angina pectoris on patients’ quality of life and has 9 other language versions. The QLI-cardiac version, also known as Ferrans and Powers questionnaire (1993) [24], was developed to measure quality of life in terms of satisfaction with life in patients with heart diseases and has more than 10 country versions. The MacNew was also developed in the early 1990s, initially for myocardial infarction under the name of Quality of Life after Myocardial Infarction (QLMI) and later expanded to evaluate the impact of treatment for patients with myocardial infarction, angina pectoris, and heart failure, and has been adapted to more than 80 languages. The CHP was developed in 1996 with the main aim to assess HRQL in patients with cardiovascular disease and has a specific version for CHD. It has been adapted into 13 languages and is nowadays still applied. The MIDAS-35 was developed approximately one decade later (2002), to be a short measure of health status for individuals with acute myocardial infarction. It was originally created for UK patients, and nowadays there are 7 language versions. The CROQ was specifically designed to evaluate health status in patients undergoing coronary artery disease grafting and percutaneous transluminal coronary angioplasty, and presents different versions according to the moment of administration (pre- or post-intervention) and the type of intervention (coronary artery disease grafting or percutaneous transluminal coronary angioplasty). The HeartQoL (2014) was developed simultaneously in 15 countries and has subsequently been translated into another 16 languages. The original aim was to assess CHD-specific HRQL for making between-diagnosis comparisons following interventions that are routinely used in more than one CHD diagnosis.
Regarding the content of the dimensions, all instruments cover physical and emotional domains, and most of them also include a social dimension (Table 3). Nine of these questionnaires have a specific domain related to disease symptoms, treatments, or their side effects: APQLQ, Angina Impact Questionnaire (AIQ), Questionnaire for coronary artery bypass grafting, CAST, Cardiac Quality of Life Index (CQLI), MIDAS-35, CROQ, Quality of Life Instruments for Chronic Diseases-Coronary Heart Disease (QLICD-CHD), and MC-PROM. Moreover, 13 out of the 21 instruments have a domain covering specific issues such as sleep problems in the APQLQ and Cuestionario de Calidad de Vida de Velasco-del Barrio (CCVPPI), financial aspects in the Questionnaire for coronary artery bypass grafting and Multidimensional Index of Life Quality (MILQ), alertness in the Summary index and CCVPPI, or occupational aspects in the Questionnaire for coronary artery bypass grafting, CAST or MILQ.
Supplementary Table 4 shows 20 specific PROMs for CHD that measured some construct other than symptoms, functional status or HRQL, for example, psychological and behavioral aspects such as depression, anxiety, anger, or distress (measured by 5 instruments), self-efficacy (4 instruments), attitudes, perceptions, threats, and expectations about the treatment (3 instruments), knowledge (2 instruments), adjustment or limitation to work (2 instruments), social support (2 instruments), or self-care (1 instrument). Most of these instruments were developed in the last 20 years and have been used recently, with at least one publication in the last 10 years. Those with the most language versions developed are the CDS and the SC-CHDI, which are available in 9 and 11 languages, respectively. Regarding psychometric properties, for the majority of these instruments only internal consistency and construct or content validity have been assessed, being CDS the exception as its reproducibility and responsiveness have also been assessed.
Deserving a special mention is the RehaCAT-Cardio project for the development and validation of a computer adaptive test (CAT) for cardiac patients undergoing rehabilitation, which has designed different item banks and scales for the assessment of several constructs, such as activities of daily living, anxiety, treatment motivation, and work capacity.
Discussion
Facilitating the selection of the most appropriate PROM for a specific aim is the first step needed to increase patient-centered approaches in CHD, an area where only around 29% of trials report using these measures [12]. The most important characteristic to be considered in this decision process should be what is the construct of interest for the study, program, or initiative implemented.
Reviews of PROMs for CHD have been primarily focused on instruments measuring HRQL or symptoms [12, 14,15,16,17, 20]. Through a systematic review we have identified 56 PROMs to be applied to patients with CHD, covering different constructs: HRQL, symptoms, functional status, or several psychological or behavioral aspects.
A few reviews have included various constructs, but they were not exclusively centered on CHD. There is a scoping review of all existing disease-specific PROMs for patients with heart disease, including heart diseases in general, ischemic heart disease, heart failure, arrhythmia, valve disease, and/or grown-up congenital heart disease [19], which only identified 9 instruments for ischemic heart disease and 5 for heart disease in general. The low number of PROMs identified by this scoping review was probably due to the exclusion criteria of PROMs measuring single symptoms or domains, because its purpose was mapping the items contained in WHO’s International Classification of Functioning, Disability, and Health (ICF). A systematic review of cardiovascular-specific PROMs identified 26 instruments for patients undergoing elective coronary revascularization, although specific PROMs applied to other procedures were not included [18].
Symptoms and functional status were also commonly included in the CHD studies, and 15 PROMs have been developed. A literature review of PROMs assessing symptoms for different cardiovascular diseases found 14 symptoms instruments for various acute coronary syndromes and 10 specifically for patients with angina [20].
Typically, the quantification method of symptoms and functioning in CHD has been the Canadian Cardiovascular Society (CCS) classification system, which is determined by the clinician rather than the patient [25]. Almost 40 years of research have documented substantial limitations in the CCS classification system [26, 27]: the data collectively suggest a need for more consistent, systematic, and accurate means to quantify the frequency and burden of angina from the patient’s perspective. In this sense, 12 symptoms [28,29,30,31,32,33,34,35,36,37,38,39] and 3 functional status instruments [40,41,42] have been developed, but only 5 symptoms and 2 functional status scales have been used in the last 10 years. This is probably the consequence of some of them having been established as “gold standards” and used consistently due to the accumulated evidence of well-established validity, reproducibility, prognostic importance, and sensitivity to clinical change [25]. This would be the case of the RAQ for symptom recognition or the DASI and the SAQ for functional status assessment [9].
The RAQ was constructed in the 1960s for assessing the population burden of angina, and positive screening in RAQ predicts myocardial infarction and cardiovascular disease [43]. The DASI, although initially developed for cardiac patients to assess usual physical activities and cardiopulmonary fitness, has been shown to be useful for non-cardiac disease to improve the identification of patients at an elevated risk for myocardial infarction [44]. The SAQ was endorsed as a performance measure by the AMA/ACC/AHA Physicians’ Consortium for Performance Improvement in the 1990s, and it has been more extensively applied in clinical trials than adopted in clinical practice [27]. The International Consortium for Health Outcomes Measurement (ICHOM), an organization with the mission to unlock the potential of value-based healthcare, recommends the short version of the SAQ in the CHD standard sets of outcome measures.
Instruments focused on HRQL are the largest group with 21 PROMs [24, 33, 45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66], making it difficult to select the most appropriate instrument, yet this is one of the most interesting constructs for clinicians and researchers. HRQL instruments specific for patients with CHD usually include a physical and an emotional domain, quite frequently also a social domain, and the most recent ones add dimensions for measuring self-care, dependency, or satisfaction. Considering the most frequently used instruments in the last 10 years (APQLQ, QLI-cardiac version, MacNew, MIDAS-35, CROQ, and HeartQol), differences among the number of items (22 to 70) and domains are important. Half of them were developed with the aim of evaluating the impact of treatments (MacNew, CROQ, and HeartQol), allowing for comparisons among interventions, a relevant aspect for shared decision making.
In recent decades, there has been a growing interest in patient-centered approaches that open the scope to other constructs like self-care, attitudes, or psychological aspects specifically related to the disease. Our review has found 20 scales [67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91] to measure mood symptoms, perception, expectation regarding the disease (beliefs, attitudes, risk perception, or knowledge) or coping strategies (self-efficacy, self-care, adjustment, or social support). CHD often involves mood symptoms of distress, anxiety, or depression, which, in turn, are risk factors for CHD [92, 93]. However, it should be noted that information on their metric properties has not been reported yet for many of these instruments, with a considerable gap regarding their sensitivity to change. CDS is the only instrument with evidence on reliability, validity, and responsiveness. In the United States, the proportion of depression in patients with acute myocardial infarction is three times higher than in the general population, and anxiety is almost twice [94, 95]. Aware of these data, the American Heart Association (AHA) recommends routine screening for depression, allowing effective treatment for improving health outcomes [96]. Conversely, the assessment of protective factors such as self-care, self-efficacy, or social support, among other constructs related to coping strategies, could help to promote lifestyle changes in patients and increase the level of compliance with medical recommendations.
In general, there is a tendency to develop short versions of the original instrument or to develop a renewed version. Such is the case of the RAQ, which has multiple modified versions, or the MacNew, which was initially developed in 1993 for myocardial infarction (QLMI) and extended its applicability to other conditions in the current version published in 1996. The SAQ, with an original version of 19 items, has a shorter 7-item version developed to reduce its response burden and to provide a single summary score to facilitate its adoption in clinical care [97].
Strengths and limitations
This is the first systematic review of specific PROMs applied in CHD patients, including all the constructs measured, and without restrictions regarding language and year of publication. It was registered at PROSPERO and follows the PRISMA guidelines for the systematic review of reviews, a research procedure nowadays recommended to increase transparency and reproducibility and decrease reporting bias.
The results of the present systematic review should be interpreted in the light of their principal limitation. The authors acknowledge that more PROMs might have been identified if other databases had been searched in addition to MEDLINE, Scopus, and the Cochrane Database. However, additional manual screening of reference lists from relevant articles and targeted searches in PROQOLID and BiblioPRO still yielded a relatively large number of PROMs.
Conclusions and practical implications
A wide variety of instruments has been developed to assess patient-reported outcomes in CHD, covering several constructs which may be of special interest. The first step to increase patient-centered approaches in CHD is to identify, classify, and describe the existing PROMs, including the evidence on their metric properties. The second step on the continuum towards value-based healthcare [98] may be the evaluation of PROMs’ implementation in different settings, to report the usability and utility of these measures for patients, carers, and health professionals.
In conclusion, this review has practical significance, as it summarizes relevant information that may help clinicians, researchers, and other healthcare stakeholders to choose the most adequate instrument for incorporating the patients’ perspective and promote a model of shared decision making in a trend towards value-based healthcare [99].
Data availability
Data and material are available from the corresponding author upon reasonable request.
Code availability
Not applicable.
References
Institute of Medicine (US) Committee on Quality of Health Care in America. (2001). Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press. https://doi.org/10.17226/10027
Patient-Centered Outcomes Research | PCORI. (n.d.). Retrieved July 30, 2021, from https://www.pcori.org/research-results/about-our-research/patient-centered-outcomes-research
Rumsfeld, J. S., Alexander, K. P., Goff, D. C., Jr., Graham, M. M., Ho, P. M., Masoudi, F. A., Moser, D. K., Roger, V. L., Slaughter, M. S., Smolderen, K. G., Spertus, J. A., Sullivan, M. D., Treat-Jacobson, D., Zerwic, J. J., American Heart Association Council on Quality of Care and Outcomes Research, Council on Cardiovascular and Stroke Nursing, Council on Epidemiology and Prevention, Council on Peripheral Vascular Disease, and Stroke Council. (2013). Cardiovascular health: The importance of measuring patient-reported health status a scientific statement from the American Heart Association. Circulation, 127(22), 2233–2249. https://doi.org/10.1161/CIR.0b013e3182949a2e
U.S. Department of Health and Human Services FDA Center for Drug Evaluation and Research; U.S. Department of Health and Human Services FDA Center for Biologics Evaluation and Research; U.S. Department of Health and Human Services FDA Center for Devices and Radiological Health. (2006). Guidance for industry: patient-reported outcome measures: use in medical product development to support labeling claims: draft guidance. Health and Quality of Life Outcomes, 4, 79. https://doi.org/10.1186/1477-7525-4-79
McKenna, S. P. (2011). Measuring patient-reported outcomes: Moving beyond misplaced common sense to hard science. BMC Medicine, 9, 86. https://doi.org/10.1186/1741-7015-9-86
Mayo, N. E. (2015). ISOQOL dictionary of quality of life and health outcomes measurement. International Society for Quality of Life Research.
GBD 2019 Diseases and Injuries Collaborators. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. The Lancet (London, England), 396(10258), 1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
Fihn, S. D., Gardin, J. M., Abrams, J., Berra, K., Blankenship, J. C., Dallas, A. P., Douglas, P. S., Foody, J. M., Gerber, T. C., Hinderliter, A. L., King, M. A., Prager, R. L., Sabik, J. F., Shaw, L. J., Sikkema, J. D., Smith, C. R., Jr., Smith, S. C., Jr., Spertus, J. A., Williams, S. W., & American College Of Cardiology Foundation. (2012). 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: executive summary: a report of the American College of Cardiology Foundation/American Heart Association task force on practice. Circulation, 126(25), 3097–3137. https://doi.org/10.1161/CIR.0b013e3182776f83
Garcia, R. A., & Spertus, J. A. (2021). Using patient-reported outcomes to assess healthcare quality: Toward better measurement of patient-centered care in cardiovascular disease. Methodist DeBakey Cardiovascular Journal, 17(1), e1–e9. https://doi.org/10.14797/VUWD7697
Sanders, C., Egger, M., Donovan, J., Tallon, D., & Frankel, S. (1998). Reporting on quality of life in randomised controlled trials: Bibliographic study. BMJ (Clinical Research Edition), 317(7167), 1191–1194. https://doi.org/10.1136/bmj.317.7167.1191
Rahimi, K., Malhotra, A., Banning, A. P., & Jenkinson, C. (2010). Outcome selection and role of patient reported outcomes in contemporary cardiovascular trials: Systematic review. BMJ (Clinical Research Edition), 341, c5707. https://doi.org/10.1136/bmj.c5707
Mark, D. B. (2016). Assessing quality-of-life outcomes in cardiovascular clinical research. Nature Reviews Cardiology, 13(5), 286–308. https://doi.org/10.1038/nrcardio.2016.10
Churruca, K., Pomare, C., Ellis, L. A., Long, J. C., Henderson, S. B., Murphy, L. E. D., Leahy, C. J., & Braithwaite, J. (2021). Patient-reported outcome measures (PROMs): A review of generic and condition-specific measures and a discussion of trends and issues. Health Expectations, 24(4), 1015–1024. https://doi.org/10.1111/hex.13254
da Silva, S. A., Passos, S. R. L., Carballo, M. T., & Figueiró, M. F. (2011). Quality of life assessment after acute coronary syndrome: Systematic review. Arquivos Brasileiros de Cardiologia, 97(6), 526–540. https://doi.org/10.1590/S0066-782X2011001500013
Cepeda-Valery, B., Cheong, A. P., Lee, A., & Yan, B. P. (2011). Measuring health related quality of life in coronary heart disease: The importance of feeling well. International Journal of Cardiology, 149(1), 4–9. https://doi.org/10.1016/j.ijcard.2010.09.048
Soo Hoo, S. Y., Gallagher, R., & Elliott, D. (2014). Systematic review of health-related quality of life in older people following percutaneous coronary intervention. Nursing and Health Sciences, 16(4), 415–427. https://doi.org/10.1111/nhs.12121
Khoiriyati, A., Kusnanto, & Kurniawati, N. D. (2020). Selecting instruments to measure quality of life after acute coronary syndrome: A literature review. International Journal of Psychosocial Rehabilitation, 24(7), 7744–7751.
Peeters, G., Barker, A. L., Talevski, J., Ackerman, I., Ayton, D. R., Reid, C., Evans, S. M., Stoelwinder, J. U., & McNeil, J. J. (2018). Do patients have a say? A narrative review of the development of patient-reported outcome measures used in elective procedures for coronary revascularisation. Quality of Life Research, 27(5), 1369–1380. https://doi.org/10.1007/s11136-018-1795-6
Algurén, B., Coenen, M., Malm, D., Fridlund, B., Mårtensson, J., & Årestedt, K. (2020). A scoping review and mapping exercise comparing the content of patient-reported outcome measures (PROMs) across heart disease-specific scales. Journal of Patient-Reported Outcomes. https://doi.org/10.1186/s41687-019-0165-7
Zimmerman, L., Pozehl, B., Vuckovic, K., Barnason, S., Schulz, P., Seo, Y., Ryan, C. J., Zerwic, J. J., & DeVon, H. A. (2016). Selecting symptom instruments for cardiovascular populations. Heart and Lung. https://doi.org/10.1016/j.hrtlng.2016.08.012
Horsley, T., Dingwall, O., & Sampson, M. (2011). Checking reference lists to find additional studies for systematic reviews. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.MR000026.pub2
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetziaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonal, S., … Moher, D. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clinical Research Edition). https://doi.org/10.1136/bmj.n71
Cook, D. G., Shaper, A. G., & MacFarlane, P. W. (1989). Using the WHO (Rose) angina questionnaire in cardiovascular epidemiology. International Journal of Epidemiology, 18(3), 607–613. https://doi.org/10.1093/ije/18.3.607
Bliley, A. V., & Ferrans, C. E. (1993). Quality of life after coronary angioplasty. Heart and Lung, 22(3), 193–199.
Thomas, M., Jones, P. G., Arnold, S. V., & Spertus, J. A. (2021). Interpretation of the Seattle Angina Questionnaire as an outcome measure in clinical trials and clinical Care: A review. JAMA Cardiology. https://doi.org/10.1001/jamacardio.2020.7478
Beltrame, J. F., Weekes, A. J., Morgan, C., Tavella, R., & Spertus, J. A. (2009). The prevalence of weekly angina among patients with chronic stable angina in primary care practices: The Coronary Artery Disease in General Practice (CADENCE) Study. Archives of Internal Medicine, 169(16), 1491–1499. https://doi.org/10.1001/archinternmed.2009.295
Shafiq, A., Arnold, S. V., Gosch, K., Kureshi, F., Breeding, T., Jones, P. G., Beltrame, J., & Spertus, J. A. (2016). Patient and physician discordance in reporting symptoms of angina among stable coronary artery disease patients: Insights from the Angina Prevalence and Provider Evaluation of Angina Relief (APPEAR) study. American Heart Journal, 175, 94–100. https://doi.org/10.1016/j.ahj.2016.02.015
Rose, G. A. (1962). The diagnosis of ischaemic heart pain and intermittent claudication in field surveys. Bulletin of the World Health Organization, 27(6), 645–658.
Herlitz, J., Hjalmarson, R., Karlson, B. W., Nyberg, G., Hjalmarson, A., Karlson, B. W., & Nyberg, G. (1988). Long-term morbidity in patients where the initial suspicion of myocardial infarction was not confirmed. Clinical Cardiology, 11(4), 209–214. https://doi.org/10.1002/clc.4960110404
Keresztes, P., Holm, K., Penckofer, S., & Merritt, S. (1993). Measurement of functional ability in patients with coronary artery disease. Journal of Nursing Measurement, 1(1), 19–28.
Artinian, N. T., Duggan, C., & Miller, P. (1993). Age differences in patient recovery patterns following coronary artery bypass surgery. American Journal of Critical Care, 2(6), 453–461.
Plach, S. K., & Heidrich, S. M. (2001). Women’s perceptions of their social roles after heart surgery and coronary angioplasty. Heart and Lung, 30(2), 117–127. https://doi.org/10.1067/mhl.2001.113561
Schroter, S., & Lamping, D. L. (2004). Coronary revascularisation outcome questionnaire (CROQ): Development and validation of a new, patient-based measure of outcome in coronary bypass surgery and angioplasty. Heart, 90(12), 1460–1466. https://doi.org/10.1136/hrt.2003.021899
DeVon, H. A., Ryan, C. J., Ochs, A. L., & Moshe, S. (2008). Symptoms across the continuum of acute coronary syndromes: Differences between women and men. American Journal of Critical Care, 17(1), 14–24.
McSweeney, J. C., O’Sullivan, P., Cody, M., & Crane, P. B. (2004). Development of the McSweeney acute and prodromal myocardial infarction symptom survey. The Journal of Cardiovascular Nursing, 19(1), 58–67. https://doi.org/10.1097/00005082-200401000-00010
Miller, K. H., & Grindel, C. G. (2004). Comparison of symptoms of younger and older patients undergoing coronary artery bypass surgery. Clinical Nursing Research, 13(3), 178–179. https://doi.org/10.1177/1054773804265693
LaPier, T. K. (2006). Psychometric evaluation of the heart surgery symptom inventory in patients recovering from coronary artery bypass surgery. Journal of Cardiopulmonary Rehabilitation, 26(2), 101–106. https://doi.org/10.1097/00008483-200603000-00010
Nieveen, J. L., Zimmerman, L. M., Barnason, S. A., & Yates, B. C. (2008). Development and content validity testing of the Cardiac Symptom Survey in patients after coronary artery bypass grafting. Heart and Lung, 37(1), 17–27. https://doi.org/10.1016/j.hrtlng.2006.12.002
Gilead Sciences. (2012). The speak from the heart chronic angina checklist. http://www.speakfromtheheart.com/anginaassessment.aspx
Lewin, R. J. P., Thompson, D. R., Martin, C. R., Stuckey, N., Devlen, J., Michaelson, S., & Maguire, P. (2002). Validation of the Cardiovascular Limitations and Symptoms Profile (CLASP) in chronic stable angina. Journal of Cardiopulmonary Rehabilitation, 22(3), 184–191. https://doi.org/10.1097/00008483-200205000-00010
Hlatky, M. A., Boineau, R. E., Higginbotham, M. B., Lee, K. L., Mark, D. B., Califf, R. M., Cobb, F. R., & Pryor, D. B. (1989). A brief self-administered questionnaire to determine functional capacity (the Duke Activity Status Index). The American Journal of Cardiology, 64(10), 651–654. https://doi.org/10.1016/0002-9149(89)90496-7
Spertus, J. A., Winder, J. A., Dewhurst, T. A., Deyo, R. A., Prodzinski, J., McDonell, M., & Fihn, S. D. (1995). Development and evaluation of the Seattle Angina Questionnaire: A new functional status measure for coronary artery disease. Journal of the American College of Cardiology, 25(2), 333–341. https://doi.org/10.1016/0735-1097(94)00397-9
Graff-Iversen, S., Wilsgaard, T., Mathiesen, E. B., Njølstad, I., & Løchen, M.-L. (2014). Long-term cardiovascular consequences of Rose angina at age 20–54 years: 29-years’ follow-up of the Tromso Study. Journal of Epidemiology and Community Health, 68(8), 754–759. https://doi.org/10.1136/jech-2013-203642
Wijeysundera, D. N., Beattie, W. S., Hillis, G. S., Abbott, T. E. F., Shulman, M. A., Ackland, G. L., Mazer, C. D., Myles, P. S., Pearse, R. M., Cuthbertson, B. H., Measurement of Exercise Tolerance before Surgery Study Investigators, Myles, P. S., Shulman, M. A., Wallace, S., Farrington, C., Thompson, B., Ellis, M., Borg, B., Kerridge, R K.,… Lifford, R. (2020). Integration of the Duke Activity Status Index into preoperative risk evaluation: a multicentre prospective cohort study. British Journal of Anaesthesia, 124(3), 261–270. https://doi.org/10.1016/j.bja.2019.11.025
Wiklund, I. (1988). Livskvalitet vid kardiovaskulara sjukdomar. Scandinavian Journal of Behavioral Therapy, 17, 87–92.
Wilson, A., Wiklund, I., Lahti, T., & Wahl, M. (1991). A summary index for the assessment of quality of life in angina pectoris. Journal of Clinical Epidemiology, 44(9), 981–988. https://doi.org/10.1016/0895-4356(91)90069-L
Nissinen, A., Wiklund, I., Lahti, T., Akkila, J., Wilson, A., Wahl, M., & Puska, P. (1991). Anti-anginal therapy and quality of life. A comparison of the effects of transdermal nitroglycerin and long-acting oral nitrates. Journal of Clinical Epidemiology, 44(9), 989–997. https://doi.org/10.1016/0895-4356(91)90070-p
Wilson, I. B., & Cleary, P. D. (1995). Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA, 273(1), 59–65.
Caine, N., Harrison, S. C. W., Sharples, L. D., & Wallwork, J. (1991). Prospective study of quality of life before and after coronary artery bypass grafting. British Medical Journal, 302(6775), 511–516. https://doi.org/10.1136/bmj.302.6775.511
Wiklund, I., Gorkin, L., Pawitan, Y., Schron, E., Schoenberger, J., Jared, L. L., & Shumaker, S. (1992). Methods for assessing quality of life in the cardiac arrhythmia suppression trial (CAST). Quality of Life Research, 1(3), 187–201. https://doi.org/10.1007/BF00635618
Velasco, J. A., del Barrio, V., Mestre, M. V., Penas, C., & Ridocci, F. (1993). Validation of a new questionnaire to evaluate the quality of life in patients after myocardial infarction. Revista Espanola de Cardiologia, 46(9), 552–558.
Valenti, L., Lim, L., Heller, R. F., & Knapp, J. (1996). An improved questionnaire for assessing quality of life after acute myocardial infarction. Quality of Life Research, 5(1), 151–161. https://doi.org/10.1007/BF00435980
Lim, L. L. Y., Valenti, L. A., Knapp, J. C., Dobson, A. J., Plotnikoff, R., Higginbotham, N., & Heller, R. F. (1993). A self-administered quality-of-life questionnaire after acute myocardial infarction. Journal of Clinical Epidemiology, 46(11), 1249–1256. https://doi.org/10.1016/0895-4356(93)90089-J
Rukholm, E., & McGirr, M. (1994). A quality-of-life index for clients with ischemic heart disease: Establishing reliability and validity. Rehabilitation Nursing, 19(1), 12–16. https://doi.org/10.1002/j.2048-7940.1994.tb01296.x
Avis, N. E., Smith, K. W., Hambleton, R. K., Feldman, H. A., Selwyn, A., & Jacobs, A. (1996). Development of the multidimensional index of life quality: A quality of life measure for cardiovascular disease. Medical Care, 34(11), 1102–1120. https://doi.org/10.1097/00005650-199611000-00005
Währborg, P., & Emanuelsson, H. (1996). The cardiac health profile: Content, reliability and validity of a new disease-specific quality of life questionnaire. Coronary Artery Disease, 7(11), 823–829.
GISSI-Nursing. (1997). [Evaluation of perception of quality of life and health by patients with myocardial infarction. GISSI-Nursing]. Giornale Italiano di Cardiologia, 27(9), 865–876.
Wolinsky, F. D., Wyrwich, K. W., Nienaber, N. A., & Tierney, W. M. (1998). Generic versus disease-specific health status measures. An example using coronary artery disease and congestive heart failure patients. Evaluation and the Health Professions, 21(2), 216–243. https://doi.org/10.1177/016327879802100205
Martin, A. J., Glasziou, P. P., & Simes, R. J. (1999). A cardiovascular extension of the Health Measurement Questionnaire. Journal of Epidemiology and Community Health, 53(9), 548–557. https://doi.org/10.1136/jech.53.9.548
Buchner, D. A., Graboys, T. B., Johnson, K., Mordin, M. M., Goodman, L., Partsch, D. S., & Goss, T. F. (2001). Development and validation of the ITG Health-Related Quality-of-Life Short-Form measure for use in patients with coronary artery disease. Integrated Therapeutics Group. Clinical Cardiology, 24(8), 556–563. https://doi.org/10.1002/clc.4960240807
Thompson, D. R., Jenkinson, C., Roebuck, A., Lewin, R. J. P., Boyle, R. M., & Chandola, T. (2002). Development and validation of a short measure of health status for individuals with acute myocardial infarction: The myocardial infarction dimensional assessment scale (MIDAS). Quality of Life Research, 11(6), 535–543. https://doi.org/10.1023/A:1016354516168
Oldridge, N., Höfer, S., McGee, H., Conroy, R., Doyle, F., Saner, H. (for the HeartQoL Project Investigators). (2014). The HeartQoL: Part II. Validation of a new core health-related quality of life questionnaire for patients with ischemic heart disease. European Journal of Preventive Cardiology, 21(1), 98–106. . Retrieved from https://journals.sagepub.com/doi/abs/10.1177/2047487312450545
Chuanmeng, Z., Zhiwen, H., Chonghua, W., Zheng, Y., & Chuanzhi, X. (2018). Development and responsiveness of the coronary heart disease scale in the patient reported outcomes instruments system for chronic diseases. Chinese Journal of Modern Nurse, 24(17), 1991–1995.
Wan, C., Li, H., Fan, X., Yang, R., Pan, J., Chen, W., & Zhao, R. (2014). Development and validation of the coronary heart disease scale under the system of quality of life instruments for chronic diseases QLICD-CHD: Combinations of classical test theory and Generalizability theory. Health and Quality of Life Outcomes. https://doi.org/10.1186/1477-7525-12-82
Soh, S.-E., Barker, A. L., Ayton, D. R., Ahern, S., Morello, R., Lefkovits, J., Brennan, A. L., Evans, S., Zalcberg, J. R., Reid, C. M., & McNeil, J. J. (2019). What matters most to patients following percutaneous coronary interventions? A new patient-reported outcome measure developed using Rasch analysis. PLoS ONE, 14(9), e0222185. https://doi.org/10.1371/journal.pone.0222185
Oldridge, N., Höfer, S., McGee, H., Conroy, R., Doyle, F., & Saner, H. (2014). The HeartQoL: Part I. Development of a new core health-related quality of life questionnaire for patients with ischemic heart disease. European Journal of Preventive Cardiology, 21(1), 90–97. https://doi.org/10.1177/2047487312450544
Rumbaugh, D. M., & Knapp, R. R. (1965). Prediction of work potential in heart patients through use of the cardiac adjustment scale. Journal of Consulting Psychology, 29(6), 597. https://doi.org/10.1037/h0022686
Barnason, S. A. (1992). A comparison of cardiac teaching on learning variables among cardiac surgical patients. ETD collection for University of Nebraska - Lincoln. AAI9314388.
Barnason, S., Zimmerman, L., Atwood, J., Nieveen, J., & Schmaderer, M. (2002). Development of a self-efficacy instrument for coronary artery bypass graft patients. Journal of Nursing Measurement, 10(2), 123–133. https://doi.org/10.1891/jnum.10.2.123.52553
Moser, D. K., & Dracup, K. (1995). Psychosocial recovery from a cardiac event: The influence of perceived control. Heart and Lung, 24(4), 273–280. https://doi.org/10.1016/s0147-9563(05)80070-6
Riegel, B., McKinley, S., Moser, D. K., Meischke, H., Doering, L., & Dracup, K. (2007). Psychometric evaluation of the Acute Coronary Syndrome (ACS) response index. Research in Nursing and Health, 30(6), 584–594. https://doi.org/10.1002/nur.20213
Hare, D. L., & Davis, C. R. (1996). Cardiac Depression Scale: Validation of a new depression scale for cardiac patients. Journal of Psychosomatic Research, 40(4), 379–386. https://doi.org/10.1016/0022-3999(95)00612-5
Bennett, S. J., Puntenney, P. J., Walker, N. L., & Ashley, N. D. (1996). Development of an instrument to measure threat related to cardiac events. Nursing Research, 45(5), 266–270. https://doi.org/10.1097/00006199-199609000-00003
Lerner, D. J., Amick, B. C., 3rd., Malspeis, S., Rogers, W. H., Gomes, D. R., & Salem, D. N. (1998). The angina-related limitations at work questionnaire. Quality of life Research, 7(1), 23–32. https://doi.org/10.1023/a:1008880704343
Sullivan, M. D., LaCroix, A. Z., Russo, J., & Katon, W. J. (1998). Self-efficacy and self-reported functional status in coronary heart disease: A six-month prospective study. Psychosomatic Medicine, 60(4), 473–478. https://doi.org/10.1097/00006842-199807000-00014
The ENRICHD investigators. (2000). Enhancing recovery in coronary heart disease patients (ENRICHD): Study design and methods. The ENRICHD investigators. American Heart Journal, 139(1 Pt 1), 1–9. https://doi.org/10.1016/s0002-8703(00)90301-6
Eifert, G. H., Thompson, R. N., Zvolensky, M. J., Edwards, K., Frazer, N. L., Haddad, J. W., & Davig, J. (2000). The Cardiac Anxiety Questionnaire: Development and preliminary validity. Behaviour Research and Therapy. https://doi.org/10.1016/S0005-7967(99)00132-1
di Benedetto, M., & Sheehan, M. (2014). Evaluation of the Cardiac Depression Visual Analogue Scale in a medical and non-medical sample. Psychology, Health and Medicine, 19(1), 93–102. https://doi.org/10.1080/13548506.2013.779728
Young, Q.-R., Ignaszewski, A., Fofonoff, D., & Kaan, A. (2007). Brief screen to identify 5 of the most common forms of psychosocial distress in cardiac patients: Validation of the screening tool for psychological distress. Journal of Cardiovascular Nursing. https://doi.org/10.1097/01.JCN.0000297383.29250.14
Haschke, A., Abberger, B., Wirtz, M., Bengel, J., & Baumeister, H. (2013). Development of short form questionnaires for the assessment of work capacity in cardiovascular rehabilitation patients. International Journal of Occupational and Environmental Health, 26(5), 742–750. https://doi.org/10.2478/s13382-013-0158-3
Schmucker, A., Abberger, B., Boecker, M., & Baumeister, H. (2019). Parallel short forms for the assessment of activities of daily living in cardiovascular rehabilitation patients (PADL-cardio): Development and validation. Disability and Rehabilitation, 41(7), 826–832. https://doi.org/10.1080/09638288.2017.1407967
Abberger, B., Haschke, A., Krense, C., Wirtz, M., Bengel, J., & Baumeister, H. (2013). The calibrated, unidimensional anxiety item bank for cardiovascular patients provided the basis for anxiety assessment in cardiovascular rehabilitation patients. Journal of Clinical Epidemiology. https://doi.org/10.1016/j.jclinepi.2012.08.009
Baumeister, H., Abberger, B., Haschke, A., Boecker, M., Bengel, J., & Wirtz, M. (2013). Development and calibration of an item bank for the assessment of activities of daily living in cardiovascular patients using Rasch analysis. Health and Quality of Life Outcomes. https://doi.org/10.1186/1477-7525-11-133
Abberger, B., Haschke, A., Wirtz, M., Kroehne, U., Bengel, J., & Baumeister, H. (2013). Development and evaluation of a computer adaptive test to assess anxiety in cardiovascular rehabilitation patients. Archives of Physical Medicine and Rehabilitation, 94(12), 2433–2439. https://doi.org/10.1016/j.apmr.2013.07.009
Abberger, B., Haschke, A., Tully, P. J., Forkmann, T., Berger, J., Wirtz, M., Bengel, J., & Baumeister, H. (2017). Development and validation of parallel short forms PaSA-cardio for the assessment of general anxiety in cardiovascular rehabilitation patients using Rasch analysis. Clinical Rehabilitation, 31(1), 104–114. https://doi.org/10.1177/0269215515627288
Chan, C. W. (2014). Perceptions of coronary heart disease: The development and psychometric testing of a measurement scale. Psychology, Health and Medicine, 19(2), 159–168. https://doi.org/10.1080/13548506.2013.802354
Steca, P., Greco, A., Cappelletti, E., D’Addario, M., Monzani, D., Pancani, L., Ferrari, G., Politi, A., Gestra, R., Malfatto, G., & Parati, G. (2015). Cardiovascular management self-efficacy: Psychometric properties of a new scale and its usefulness in a rehabilitation context. Annals of Behavioral Medicine, 49(5), 660–674. https://doi.org/10.1007/s12160-015-9698-z
Odell, A., Bång, A., Andréll, P., Widell, C., Fryklund, H., Kallryd, A., Tygesen, H., & Grip, L. (2017). Patients expectations and fulfilment of expectations before and after treatment for suspected coronary artery disease assessed with a newly developed questionnaire in combination with established health-related quality of life questionnaires. Open Heart, 4(1), e000529. https://doi.org/10.1136/openhrt-2016-000529
Vaughan Dickson, V., Lee, C. S., Yehle, K. S., Mola, A., Faulkner, K. M., & Riegel, B. (2017). Psychometric testing of the Self-Care of Coronary Heart Disease Inventory (SC-CHDI). Research in Nursing and Health. https://doi.org/10.1002/nur.21755
Jackson, A., Rogerson, M., le Grande, M., Thompson, D., Ski, C., Alvarenga, M., Amerena, J., Higgins, R., Raciti, M., & Murphy, B. M. (2020). Protocol for the development and validation of a measure of persistent psychological and emotional distress in cardiac patients: The Cardiac Distress Inventory. British Medical Journal Open, 10(6), e034946. https://doi.org/10.1136/bmjopen-2019-034946
Haschke, A., Abberger, B., Müller, E., Wirtz, M., Bengel, J., & Baumeister, H. (2013). Calibration of an item bank for work capacity in cardiological rehabilitation patients. European Journal of Preventive Cardiology, 20(5), 807–816. https://doi.org/10.1177/2047487312447911
Carney, R. M., & Freedland, K. E. (2017). Depression and coronary heart disease. Nature Reviews. Cardiology, 14(3), 145–155. https://doi.org/10.1038/nrcardio.2016.181
Karlsen, H. R., Matejschek, F., Saksvik-Lehouillier, I., & Langvik, E. (2021). Anxiety as a risk factor for cardiovascular disease independent of depression: A narrative review of current status and conflicting findings. Health Psychology Open, 8(1), 2055102920987462. https://doi.org/10.1177/2055102920987462
Egede, L. E. (2007). Major depression in individuals with chronic medical disorders: Prevalence, correlates and association with health resource utilization, lost productivity and functional disability. General Hospital Psychiatry, 29(5), 409–416. https://doi.org/10.1016/j.genhosppsych.2007.06.002
Lee, C., Lee, S. C., Shin, Y. S., Park, S., Won, K. B., Ann, S. H., & Ko, E. J. (2020). Severity, progress, and related factors of mood disorders in patients with coronary artery disease: A retrospective study. Healthcare. https://doi.org/10.3390/healthcare8040568
Lichtman, J. H., Bigger, J. T. J., Blumenthal, J. A., Frasure-Smith, N., Kaufmann, P. G., Lespérance, F., Mark, D. B., Sheps, D. S., Taylor, C. B., Froelicher, E. S., American Heart Association Prevention Committee of the Council on Cardiovascular Nursing; American Heart Association Council on Clinical Cardiology; American Heart Association Council on Epidemiology and Prevention; American Heart Association Interdisciplinary Council on Quality of Care and Outcomes Research; & American Psychiatric Association. (2008). Depression and coronary heart disease: Recommendations for screening, referral, and treatment: A science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Psychiatric Association. Circulation, 118(17), 1768–1775. https://doi.org/10.1161/CIRCULATIONAHA.108.190769
Chan, P. S., Jones, P. G., Arnold, S. A., & Spertus, J. A. (2014). Development and validation of a short version of the Seattle angina questionnaire. Circulation. Cardiovascular Quality and Outcomes, 7(5), 640–647. https://doi.org/10.1161/CIRCOUTCOMES.114.000967
Porter, M. E. (2010). What is value in health care? The New England Journal of Medicine, 363(26), 2477–2481. https://doi.org/10.1056/NEJMp1011024
Porter, M. E., & Lee, T. H. (2016). From volume to value in health care: The work begins. JAMA, 316(10), 1047–1048. https://doi.org/10.1001/jama.2016.11698
Herlitz, J., Hjalmarson, R., Karlson, B. W., & Nyberg, G. (1988). Long-Term morbidity in patients where the initial suspicion of myocardial infarction was not confirmed. Clinical Cardiology, 11(4), 209–214. https://doi.org/10.1002/CLC.4960110404
Schroeder, S., Baumbach, A., Herdeg, C., Oberhoff, M., Buchholz, O., Kuettner, A., Hanke, H., & Karsch, K. R. (2001). Self-rated health and clinical status after PTCA: Results of a 4-year follow-up in 500 patients. European Journal of Internal Medicine, 12(2), 101–106. https://doi.org/10.1016/S0953-6205(01)00112-1
Acknowledgements
The authors acknowledge the collaboration and contribution of Itxaso Alayo for her assistance in the database management. Moreover, the authors thank Dave Macfarlane and Aurea Martin for their support in English editing, proofreading, and preparing this manuscript for submission.
Funding
This study was supported by grants from the Instituto de Salud Carlos III FEDER: Fondo Europeo de Desarrollo Regional (grant number PI16/00130); Generalitat de Catalunya, Spain (grant number and 2017 SGR 452); and the Centro de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBER of Epidemiology and Public Health). The funders of the study had no role in the study design and conduct, data collection, management, analysis, or interpretation; they also had no role in the preparation, writing, reviewing, and submission of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors have actively participated in the study and have made a substantial contribution to (1) either conception and design, or acquisition of data, or analysis and interpretation of data; as well as (2) the drafting of the article or its critical revision for important intellectual content; and (3) the final approval of the version to be published.
Corresponding author
Ethics declarations
Conflict of interest
The authors declared that they have no conflict of interest.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pardo, Y., Garin, O., Oriol, C. et al. Patient-centered care in Coronary Heart Disease: what do you want to measure? A systematic review of reviews on patient-reported outcome measures. Qual Life Res 32, 1405–1425 (2023). https://doi.org/10.1007/s11136-022-03260-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-022-03260-6