
Abstract
Purpose
The psychometric property of the Dermatology Life Quality Index (DLQI) is underappreciated in public health settings. Our study aimed to assess the reliability, validity, and measurement invariance of DLQI in a homogeneous population with arsenic-related skin lesions and symptoms.
Methods
A cross-sectional study was conducted in communities under lifetime arsenic exposure. The DLQI was measured through a face-to-face interview. Skin examinations were performed by certificated dermatologists. The intensity of itching was measured by a numerical rating scale. Reliability, structural validity, and measurement invariance were determined using classical and modern test theories, including confirmatory factor analysis and item response models.
Results
465 participants with arsenic-related skin lesions and symptoms completed the DLQI assessment. The Cronbach’s alpha was 0.79, and the split-half reliability was 0.77. A two-factor model exhibited the best model fit among models evaluated, but local dependencies among items were identified. The model showed good root mean square error of approximation (0.031) and acceptable Tucker–Lewis index (0.92). Multi-group confirmatory factor analysis showed no measurement invariance across subgroups of age, gender, ethnicity, and intensity of itching.
Conclusions
The DLQI had acceptable psychometric properties, but measurement invariance was not observed across different groups of participants.


Similar content being viewed by others
References
Zheng, Y., & Flanagan, S. V. (2017). The case for universal screening of private well water quality in the U.S. and testing requirements to achieve it: Evidence from arsenic. Environmental Health Perspectives, 125(8), 085002.
Smith, A. H., & Steinmaus, C. M. (2009). Health effects of arsenic and chromium in drinking water: Recent human findings. Annual Review of Public Health, 30, 107–122.
Arikan, I., Namdar, N. D., Kahraman, C., Dagci, M., & Ece, E. (2015). Assessment of arsenic levels in body samples and chronic exposure in people using water with a high concentration of arsenic: A field study in Kutahya. Asian Pacific Journal of Cancer Prevention, 16(8), 3183–3188.
Tondel, M., Rahman, M., Magnuson, A., Chowdhury, I. A., Faruquee, M. H., & Ahmad, S. A. (1999). The relationship of arsenic levels in drinking water and the prevalence rate of skin lesions in Bangladesh. Environmental Health Perspectives, 107(9), 727–729.
Committee on Toxicology. (2001). Arsenic in drinking water: 2001 update. Washington, D.C.: National Academies Press.
Ohnishi, K., Yoshida, H., Shigeno, K., et al. (2002). Arsenic trioxide therapy for relapsed or refractory Japanese patients with acute promyelocytic leukemia: need for careful electrocardiogram monitoring. Leukemia, 16(4), 617–622.
Wang, Z., He, H., Yan, Y., & Wu, C. (1999). Arsenic exposure of residents in areas near Shimen arsenic mine. Journal of Hygiene Research, 28(1), 12–14.
Hu, Y., Zhou, L., Li, X., et al. (2015). Arsenic contamination in Shimen Realgar Mine I: AS spatial distribution, chemical fractionations and leaching. Journal of Agro-Environment Science, 34(8), 1515–1521.
Namdar, N. D., Arikan, I., Kahraman, C., Kocaturk, E., Dagci, M., & Ece, E. (2017) Evaluation of the quality of life in patients with arsenic keratosis. Cutaneous and Ocular Toxicology, 37(2), 1–5.
Finlay, A. Y., & Khan, G. K. (1994). Dermatology Life Quality Index (DLQI)—A simple practical measure for routine clinical use. Journal of Clinical and Experimental Dermatology, 19(3), 210–216.
Both, H., Essink-Bot, M. L., Busschbach, J., & Nijsten, T. (2007). Critical review of generic and dermatology-specific health-related quality of life instruments. Journal of Investigative Dermatology, 127(12), 272639.
Liu, Y. L., Li, T., An, J. G., Zeng, W. H., & Xiao, S. X. (2016). Rasch analysis holds no brief for the use of the Dermatology Life Quality Index (DLQI) in Chinese neurodermatitis patients. Health and Quality of Life Outcomes, 14, 17.
He, Z., Lu, C., Basra, M. K. A., Ou, A., Yan, Y., & Li, L. (2013). Psychometric properties of the Chinese version of Dermatology Life Quality Index (DLQI) in 851 Chinese patients with psoriasis. Journal of the European Academy of Dermatology and Venereology, 27(1), 109–115.
Wang, K. Y., Wang, K. H., & Zhang, Z. P. (2011). Health-related quality of life and marital quality of vitiligo patients in China. Journal of the European Academy of Dermatology and Venereology, 25(4), 429–435.
Wu, Y. Y., Fu, C. W., Zhang, W., Li, C. X., & Zhang, J. (2018). The Dermatology Life Quality Index (DLQI) and the hospital anxiety and depression (HADS) in Chinese rosacea patients. Psychology Health & Medicine, 23(4), 369–374.
Brown, T. A. (2006). Confirmatory factor analysis for applied research. New York: The Guilford Press.
Reise, S. P., & Waller, N. G. (2009). Item response theory and clinical measurement. Annual Review of Clinical Psychology, 5, 27–48.
Shen, M., Cui, Y., Hu, M., & Xu, L. (2017). Quantifying traditional Chinese medicine patterns using modern test theory: an example of functional constipation. BMC Complementary and Alternative Medicine, 17(1), 44.
Du, W., & Xiao, H. (2012). Multidimensional grade response model. Acta Psychologica Sinica, 44(10), 1402–1407.
Nijsten, T., Meads, D. M., de Korte, J., et al. (2007). Cross-cultural inequivalence of dermatology-specific health-related quality of life instruments in psoriasis patients. Journal of Investigative Dermatology, 127(10), 2315–2322.
Acknowledgements
We thank all coordinators and investigators that contributed to the field survey. We thank Dr. Shuiyuan Xiao for his expertise in revising the manuscript.
Funding
This work was supported by The Ministry of Science and Technology of China (2015FY111100).
Author information
Authors and Affiliations
Contributions
YX, XH, DJ, YH, XZ, ZS, ZH, and MS, participated in the field survey. YX, XH, DJ, and YH performed the dermatological examinations. YX and MS analyzed the data and drafted the manuscript. ZH, JS, JL, JZ, MC, XC, and MS designed the study, critically reviewed, and revised the manuscript. XC obtained the funding. All authors gave final approval to the version submitted for publication.
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was conducted according to the guidelines laid down in the Declaration of Helsinki. All procedures involving patients were approved by the institutional research ethics boards of Xiangya Hospital and The Third Xiangya Hospital, Central South University (Changsha, China).
Informed consent
Written informed consent was obtained from all participants.
Electronic supplementary material
Below is the link to the electronic supplementary material.
11136_2018_1969_MOESM1_ESM.tif
Scree plot of the exploratory factor analysis. Two common factors with eigenvalue>1.0 were identified. The third common factor had marginally significant eigenvalue of 0.99 (TIF 106 KB)
11136_2018_1969_MOESM2_ESM.tif
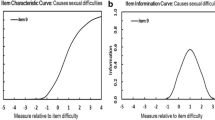
Item characteristic curve and item information function of the unidimensional item response model. The IRT was established for a unidimensional model. Each Item characteristic curve describes the item-specific relationship between the ability level (X-axis) and probability of endorsing a certain response (Y-axis). Black, blue, green, and magenta lines signify 0, 1, 2, and 3, respectively. Ability in the item response theory model practically (though not exclusively) ranged from −3 to +3. The dash lines signify item information functions, which indicate the precision of the items (TIF 253 KB)
11136_2018_1969_MOESM3_ESM.tif
Item characteristic curve and item information function of the bi-dimensional item response model. The IRT was established for a bi-dimensional model. Symbols are identical to Figure S2 (TIF 87 KB)
Rights and permissions
About this article

Cite this article
Xiao, Y., Huang, X., Jing, D. et al. Assessment of the Dermatology Life Quality Index (DLQI) in a homogeneous population under lifetime arsenic exposure. Qual Life Res 27, 3209–3215 (2018). https://doi.org/10.1007/s11136-018-1969-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-018-1969-2