
Abstract
Self-Rated Health (SRH) is currently one of the most popular indicators of population health. Studies show that SRH has a strong association with physical functioning, well-being, and mortality across a variety of populations and ages. Despite its wide use, the different elements that act and interact when an individual assesses their own health are still not clear. To date, only one study has focused on the process of self-assessment of health among the oldest-old individuals. The aim of this paper is to explore direct and indirect effects of socioeconomic status, presence of disease, functional health, and emotional health on the good self-assessment of health among Italian nonagenarians. By applying Structural Equation Modelling (SEM) on Mugello Study data, we find a strong direct effect of both emotional and functional health on SRH, confirming their key roles in the process of self-assessment of health among the oldest-old individuals. Furthermore, we find indirect effects of socioeconomic status, presence of disease, and functional health on SRH. This is in line with existing literature on younger adults and elderly people.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Self-rated health (SRH) is the most commonly used indicator to measure the general (or global) health status of an individual (de Bruin et al. 1996). With a single and simple question: “How is your health in general? Is it excellent, very good, good, fair, or poor?” respondents are asked to assess their own health condition. The aim of this question is to collect information on many dimensions of health (physical, functional, mental, and emotional) summarized in one single answer. There are different variants of the question, the wording could be different depending on the context and of the ratings, that can be skewed towards good health. For this reason, among others, cross national and over time comparisons of SRH could be problematic (Lazarevič and Brandt 2020).
SRH is known to be associated with several objective measures of health as well as to be a valid predictor of health care demand and mortality across populations and ages (Bamia et al. 2017; Luppa et al. 2010; Nybo et al. 2003; Simonsson and Molarius 2020).
Even though it is used extensively, it is still not clear which dimension of health plays an active role in the process of self-evaluation of health, whether the socioeconomic background is also involved in such process, and how all those elements interact with each other. Many researchers, over the last decades, have tried to understand what influences SRH: demographic and socioeconomic characteristics, physical, functional, and physiological health status, and chronic conditions among the others were pointed out as possible determinants (Alonso et al. 2013; Au and Johnston 2014; Fýlkesnes and Førde 1992; Golini and Egidi 2016; Johnson and Wolinsky 1993; Jylhä 2009; Jylhä et al. 1986; Lisko et al. 2020; Stoller 1984). Jylhä (2009) developed a conceptual model for SRH aimed at making explicit which factors could be involved in the cognitive process of self-evaluation of health. The model is composed of two parts: first, it includes health-related factors such as medical diagnoses, current functional status and experienced bodily sensations, and symptoms; second, context-related factors are included such as age, comparison group, culture, and disposition.
To understand the structure of SRH, it is necessary to exploit a model that can evaluate simultaneously direct and indirect effects of observed and latent variables on the designed outcome. Since Structural Equation Modeling (SEM) has such characteristic, it has been chosen by several scholars as the right approach to address this issue (Jylhä et al. 1986; Fýlkesnes and Førde 1992; Golini and Egidi 2016; Lisko et al. 2020; Hirve et al. 2014).
Building up on Jylhä’s model, among the more recent studies, Au and Johnston (2014) highlighted the importance of vitality in the process of self-evaluation of health among Australians, while Golini and Egidi (2016) found that the presence of chronic diseases plays a crucial role in this process for elderly Italians.
As the oldest-old population continues to grow in many high-income countries (Christensen et al. 2009), it becomes increasingly important to understand how they perceive and rate their own health. Until now, assessing the health conditions of the oldest-old individuals was mainly possible through targeted surveys. However, as this population segment expands, it will become more accessible to assess their health through general surveys. Furthermore, the oldest-old population represent a major group in terms of healthcare use (Forma et al. 2017). For those reasons, gaining a deeper understanding of the most important health dimensions among the oldest individuals and the underlying structure of SRH for this population becomes crucial. It would allow to understand the needs of the older individuals and to better plan public health policies targeted to improve their health and functioning in the society. In investigating it, one should take into account that people lower their expectations while getting older (Idler and Cartwright 2018). The first study evaluating the mechanism of self-assessment of health among oldest-old individuals analyzed a sample of Finnish nonagenarians (Lisko et al. 2020). Given the higher prevalence of individuals affected by dementia in the oldest-old population, Lisko and colleagues investigated whether a similar rating mechanism applies to the whole study population and to those who were affected by dementia (Lisko et al. 2020). However, they did not include any information on the socioeconomic status (SES) of the nonagenarians in their model, even though it has been shown that socioeconomic differences in health persist even among the oldest-old individuals (Enroth et al. 2013, 2019; Strozza et al. 2020a; Strozza et al., 2020b).
In this paper, we expand upon the theoretical framework proposed by Golini and Egidi (2016) and Lisko et al. (2020) by incorporating a socioeconomic construct. This extension allows to evaluate the process of self-assessment of health among Italian nonagenarians from Mugello, a rural area in Tuscany (Italy) (Molino-Lova et al. 2013). Our hypothesis is that SES could have both direct and indirect effects on SRH. The direct effect stems from individuals’ understanding of what (good) health is, and how their own health compares to that of their peers. We assume that individuals with higher SES may have a better understanding of both aspects, although this does not necessarily mean that they will rate their health more positively. Additionally, we assume that having higher SES, being associated with better health outcomes, indirectly influences SRH (Enroth et al. 2013, 2019; Strozza et al. 2020a). The notion of this indirect effect of SES on SRH is mentioned by Jylhä (2009) when detailing the theoretical model, but has not been operationalized by the scholars who expanded upon her framework.
By employing a SEM approach, our aim is to evaluate the direct and indirect effect of SES, presence of chronic diseases, and functional and emotional health on good self-rated health among Italian nonagenarians.
2 Methods
2.1 Study population
The study population comes from the Mugello Study, conducted in 2012 in 9 of the 11 municipalities of the Mugello area of Tuscany (Italy). The Mugello study was aimed to evaluate the aging process of individuals aged 90+. Demographic and socioeconomic information, as well as many health aspects, were collected by a trained physician at the patient’s residence. 504 individuals were interviewed, representing about 65% of the whole nonagenarians living in that geographical territory in 2012. The participation rate was 69% after the exclusion of the nonagenarians who died before being interviewed or those who could not be reached. More information about the study design and survey methods are available in Molino-Lova et al. (2013).
2.2 Variables description
The present study uses a binary measure of good SRH as a health outcome. SRH was measured by the question “How is your health in general? Is it excellent, very good, good, fair, or poor?” as part of the Short-Form 12 questionnaire (SF-12) (Ware et al. 1996). Individuals reporting excellent, very good or good health, out of the five possible answers, were considered in “Good SRH” while individuals reporting fair or poor health were considered in “Poor SRH”, reference category in the model. Some study participants could not be tested because of their severely poor health conditions. For this reason, following the approach adopted in (Strozza et al. 2020a), they were considered “Non testable” and added to the “Poor SRH” category, thus representing the counterpart of the “Good SRH”.
All the other observed indicators, were also transformed into binary indicators, as the small number of individuals in analysis would lead to obtaining unrobust estimates. Furthermore, this choice facilitates the interpretation of the results.
In terms of age, individuals were distinguished between those aged 90–94, reference category in the model, and 95 + years, representing younger and older nonagenarians in a standard 5-year age category and an open-age category.
The level of education was assessed by the number of completed years of education. It was dichotomized in order to distinguish between people who had completed at most the first elementary degree (3 years of education or less), reference category in the model, and people who continued to study after the first elementary degree (4 years of education or more). For people aged 90 + in 2012, studying further than the first elementary degree represented an important school achievement. It would allow them to access more skilled types of occupation.
The main occupation performed during the working life was defined according to the Italian National Institute of Statistics (ISTAT) classification of jobs with 9 categories that were reduced to 2, as the resulting categories were found to be suitable for distinguishing people in good or bad health on the same study population (Strozza et al. 2020a). Farmers, housewives and low skilled worker (laborer or unskilled worker) represented the reference category in the model and medium skilled workers (office or, industry or intellectual worker) represent the other one.
The living condition was defined by where the interview was performed (home or institution) and by the question “If home, with whom do you live?” with four possible answers: alone; spouse; other relatives; other non-relatives. It was dichotomized to distinguish between people living alone and with someone or in nursing home, reference category in the model. Living alone is assumed to represent individuals’ economy through homeownership or economic capability. Additionally, it also represents independency to participate in activities within the society.
The functional limitations were evaluated by the ability to perform 5 Activities of Daily Living (ADL): eating, dressing, bathing, toileting, transferring. Individuals who could perform all the ADLs were considered “Autonomous” while individuals who were not able to perform at least one of the five activities were considered “Not autonomous”, reference category in the model (Katz 1963).
The sensory limitations were measured by the ability to hear and see of the nonagenarians. Individuals with no sensory limitations, that is neither blind nor deaf, were considered “Not impaired” while people reporting at least one of these problems were considered “Impaired”, reference category in the model.
The motion limitation of the nonagenarians was assessed by the question: “Is the patient: confined to bed; confined to the wheelchair; walking autonomously; walking leaning on the furniture; walking with help of people; walking with aids?”. Individuals were distinguished between those who could walk autonomously (“Not impaired”) and those who could only walk with help of people, aids or leaning on furniture or who were confined to bed or wheelchair (“Impaired”), reference category in the model.
The questionnaire used in the Mugello Study included the SF-12 questionnaire, which is also intended to evaluate mental and emotional aspects of health with three specific questions (Ware et al. 1996). The three items used to represent the emotional health were assessed by the following questions: “In the last four weeks, how often did you feel calm?” (MH3); “In the last four weeks, how often did you feel sad?” (MH4); “In the last four weeks, how often did you feel full of energy?” (VT2). The possible answers to the three questions were: always; usually; often; sometimes; rarely and never. The items were dichotomized to emphasize the most severe or best condition depending on the question. For this reason, the cut-offs were chosen with reference to the frequency distribution of the observed variables, corresponding to the first or the third quartile of the distribution, depending on the implicit direction of the response range (Golini and Egidi 2016). Therefore, individuals were considered calm when they answered always or usually to MH3, and not calm, reference category in the model, when their answer was often, sometimes, rarely, or never. Furthermore, individuals were considered lively when they answered always, usually, or often to MH4, and not lively, reference category in the model, when their answer was sometimes, rarely, or never. Finally, individuals were considered sad, reference category in the model, when they answered always, usually, often, or sometimes to VT2, and not sad when they answered rarely or never.
2.3 Structural equation modelling
A Structural Equation Model (SEM) is a statistical modelling technique used to analyze relationship among multiple variables. It is particularly suitable for evaluating conceptual frameworks that involve both observed (categorical or continuous) and latent (continuous) variables. Latent variables are integral components of the theoretical framework, representing conceptual constructs that cannot be measured by a single indicator. Therefore, multiple indicators are used to measure and validate these latent variables within the SEM framework, as described below. The main advantage of using SEM over separate regressions (logistic or probit) is that SES simultaneously models all regression equations, allowing for the inclusion of mediating effects and latent confounding variables (Kupek 2006). In short, it allows estimating the direct and indirect effect of predictive variables on an observed or latent outcome (Muthén 1983).
In this study setting, the latent variables are linked to the observed (dichotomous) indicators via probit regression models, as well as the outcome to the latent and observed variables.
SEM is characterized by two components: a measurement model that relates observed to latent variables and a structural model in which relations between outcome and observed or latent variables, as well as relations between latent variables, are expressed via linear regression models. The latent variables hypothesized in the conceptual framework are validated through Confirmatory Factor Analysis (CFA). The strength of the relationship between latent variables and observed indicators is indicated by factor loadings that are expected to be higher than 0.7 in order to provide convergent validity. Moreover, the estimated correlation between latent variables is expected to be lower than 0.9 in order to provide discriminant variability.
As recommended by Hu and Bentler (1998, 1999), we reported some alternative indicators of model fit to the chi-squared statistic that is highly dependent on the sample size. In fact, with a relatively high sample size, it tends to refuse the null hypothesis, indicating that the model represents the reality, too often. The authors suggest including the Standardized Root Mean Square Residual (SRMR), representing the portion of variance and covariance not explained by the model. This indicator is considered the most powerful one to detect the adequacy of the model. They also recommend including at least one of the following indicators: the Root Means Square Error of Approximation (RMSEA), indicating the error made by approximating what we observe with the conceptual model; the Tucker and Lewis Index (TLI) and the Comparative Fit Index (CFI), representing the adequacy of the model compared to the null model where no relations among the variables are hypothesized.
Statistical analysis was performed in R version 4.2.1 (R Core Team 2022), using the lavaan package (Rosseel 2012), excluding the individuals who reported missing values in the variables in analysis. The analysis was also performed excluding the “Non testable” individuals from the study population as a sensitivity check (see Supplementary Materials).
2.3.1 Measurement Model.
The measurement model assessed in this analysis is inspired by the framework proposed by Jylhä (2009). The author defined the process of self-assessment of health as a cognitive process that leads to answering to the SRH question. Building up on Jylhä’s framework and on the work by Golini and Egidi (2016), the self-evaluation of health is assumed to depend on medical conditions (functional status and medical diagnosis) and sensations (feelings related to the status of the individual) but also on their socioeconomic condition. Other personal characteristics as age and sex are also included in the framework, potentially influencing the health perception. The health dimensions included in the model were summarized in two latent variables representing two of the three health dimensions that are assumed to contribute to the self-assessment of health: Functional Health (FH) and Emotional Health (EH). FH represents the functional dimension of health that is assumed to be related to SRH and it was measured by three binary indicators: ADL, motion limitation, and sensory limitation. EH represents the emotional and psychological dimension of health that are supposed to be related to SRH: feeling sad, lively, and calm. The third health component potentially involved and included in the model was directly measured on the patients indicating the presence of at least one Chronic Diseases (CD) among the following: cardiovascular, neurological, pulmonary, connective tissue, gastroenterological, endocrine, renal, oncological, and immunodeficiency syndrome. Furthermore, the model includes a socioeconomic component summarized by the latent variable Socioeconomic Status (SES). SES represents the social and economic latent dimension that is assumed to be related to SRH. This latent variable combines information on individuals’ level of education, main occupation performed during the working life, and living conditions. It therefore measures jointly the economic and intellectual background of the individuals together with their status within the society.
All the observed indicators were categorized as binary variables because of the small sample size of the study population. As the model assumed to represent the structure of SRH was based on assumptions that could not be simplified, the trade-off was to reduce the complexity of the variables. Furthermore, the variables’ dichotomization makes the interpretation of the latent constructs easier and of the model results more straightforward. The indicators are always intended to represent the healthy dimension of each health domain (FH, EH and CD) and the highest socioeconomic status for SES. This choice is coherent with the one of other researchers investigating the structure of SRH among elderly and oldest-old individuals (Golini and Egidi 2016; Lisko et al. 2020). Moreover, it allows to easily compare the results obtained in the present study and in the ones of Golini and Egidi (2016) on elderly Italians.
2.3.2 Structural Model.
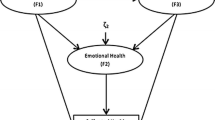
In the conceptual model proposed in this paper, good SRH is expected to be influenced, directly and indirectly, by the socioeconomic status of the individual while presence of chronic diseases, functional and emotional health may have both an independent and mediating role. The model was designed following what Golini and Egidi (2016) proposed but with the introduction of the effect of the socioeconomic status of the individuals as an active latent variable instead of a set of covariates. Socioeconomic variables seem to play a role in determining health in later life, even at very old ages (Enroth et al. 2013; Guilley et al. 2010; Strozza et al. 2020a). The model follows the extension of Nagi’s model (1965) of disabilities causation proposed by Schulz et al. (2000). The causal chain goes from pathology to impairments, to functional limitations, to disability, and finally to anxiety and depression. SRH is placed at the end of this causal chain, with the assumption that it is influenced directly and indirectly by all these factors, as proposed by Jylhä (2009). Moreover, the model proposed in this paper is coherent with the one proposed by Liang et al. (1991), in which the health structure is considered as the result of the interaction of different health factors. No reverse effect can be estimated because of the cross-sectional nature of the data. The model is represented in Fig. 1 that includes the latent constructs and the observed variable, together with the hypothesized relationships.
In addition to the socioeconomic and health factors, age and sex were included in the model as covariates. Their influence on health perception is well known as it is their effect on other health factors that were assumed to influence SRH (Lazarevič and Brandt 2020; Padua et al. 2018). It was not possible to analyze separately women and men because of the small number of the latter included in the dataset.

Hypothesized structural model of Self-Rated Health (SRH)
Note: SRH: Self-Rated Health; EH: Emotional Health; FH: Functional Health; CD: Chronic Diseases; SES: Socioeconomic Status
3 Results
3.1 Descriptive results
About three quarters of the Mugello nonagenarians were women (73.2%), who were on average older than men (respectively 93.3 vs. 92.5 years old, the difference is statistically significant with p < 0.05). More than half of the nonagenarians rated their health as good (54.6%), almost one quarter of them rated their health as bad (23.6%) while the remaining were defined as non-testable (21.8%) because of their poor health condition.
Table 1 shows the distribution of the observed indicators measuring the latent variables. Half of the participants completed 4 or more years of education (51.0%). However, 67.1% of them worked as farmers or were housewives. Despite the old age, half of the study population was autonomous in performing activities of daily living (51.8%) and almost two thirds of them did not have motion limitations (62.1%).
3.2 Model results
The hypothesized model fitted well the data: the value of the SRMR is 0.05, far below the empirical reference threshold of 0.08 suggested by Hu and Bentler (1998, 1999). The RMSEA is 0.05 (90% confidence interval 0.04–0.06). According to the previously mentioned authors, the value should be lower than 0.08 to be considered acceptable and below 0.06 to be considered good. CFI and TLI are greater or equal to the empirical threshold of 0.95: respectively 0.97 and 0.95 (Hu and Bentler 1998, 1999).
CFA verified construct validity of the three latent dimensions (SES, FH and EH) measured by the binary indicators described in Table 1. No factor cross-loadings were allowed: every indicator was assumed to have nonzero loading for the factor that it had to measure and zero factor loadings on all the others. Furthermore, measurement errors (ei) associated with each indicator were assumed to be uncorrelated with measurement errors of the other indicators measuring the same latent variable and the latent variable itself. All the unstandardized factor loadings resulted statistically significant with a value greater than the recommended threshold of 0.7 (convergent validity) with the only exception represented by the sensory limitation. Unstandardized and standardized factor loadings, together with error variances, are presented in Fig. 2. Moreover, the estimated correlations between latent variables were all lower than the recommended threshold of 0.9 (discriminant validity): 0.564 between SES and FH; 0.373 between SES and EH; and 0.520 between FH and EH.

Confirmatory Factor Analysis (CFA) of the latent dimensions of Self-Rated Health (SRH) among nonagenarians from Mugello. Unstandardized (with standard errors in parenthesis) and standardized (in italic) factor loadings
Unstandardized probit and linear regression estimates are presented in Fig. 3. Non-significant estimates are reported in Tables 2 and 3.

Hypothesized relationships between latent and observed health dimensions, socioeconomic status (SES), covariates, and Self-Rated Health (SRH) for the nonagenarians from Mugello
Note. Unstandardized linear and probit regressions are represented respectively by solid and dashed arrows. Only significant values are shown in the figure
The relationships among latent (and observed) health dimensions and between them and covariates are presented in Table 2. Being older (95 or more vs. 90–94 years old) is strongly associated with having a worse socioeconomic status (SES) and worse functional health (FH). Higher SES and not reporting any chronic disease (CD) are positively associated with having a better FH. Finally, having a better FH is positively associated with a better emotional health (EH).
Self-rated health (SRH) is associated with both functional and emotional health with the first one showing a greater magnitude expressed by the standardized estimate, than the second one. No other associations were detected, as reported in Table 3.
4 Discussion
The aim of our paper is to evaluate direct and indirect effects of socioeconomic characteristics and health-related factors on SRH among Italian nonagenarians. Based on the framework proposed by Jylhä (2009) and on the extensions made by Au and Johnston (2014) first, and Golini and Egidi (2016) afterwards, we propose an extra layer of complexity by including SES as a latent construct in the conceptual framework. Socioeconomic disparities in health are well documented among the elderly (Mackenbach et al. 2008) and, in more recent years, evidence suggests that they persist at more advanced ages (Enroth et al. 2013, 2019; Strozza et al. 2020a; Strozza et al. 2020b). Therefore, we hypothesize that SES could have a direct and indirect effect on the process of self-assessment of health among the oldest-old individuals.
To pursue our aim, we exploit a SEM that allows the simultaneous evaluation of direct and indirect associations between latent or observed variables (Muthén 1983). The SRH measure used in our analysis is obtained from the American version of the question: it is characterized by three positive items (excellent, very good, good) and two negative ones (poor, very poor). Comparing results to others obtained with the European SRH requires an appropriate rescaling of the health indicator (Jürges et al. 2008). In our study, we collapsed all the good health categories into one to compare good to poor SRH. Since both versions of SRH have shown to be associated to the same demographic and health indicators, and we only distinguish between good and poor health, it should be possible to indirectly compare our results with the ones of other studies following a similar analytical strategy.
We find a strong direct effect of emotional and functional health on SRH, the latter also having an indirect effect on good self-assessment of health through the emotional component. SES and presence of chronic disease have both an indirect effect on SRH via functional health. Being older has an impact on functional health while sex did not influence any of the construct included in the framework, even if it has been observed that gender differences in health exist among nonagenarians from Mugello (Padua et al. 2018).
The psychological and emotional component has a double role in the process of self-assessment of health. It has a direct effect on SRH, as found by other scholars who analyzed emotional health as a single indicator (Chang-Quan et al. 2010; French et al. 2012; Lisko et al. 2020) or as a latent construct (Au and Johnston 2014; Golini and Egidi 2016). At the same time, it mediates the effect of other health-related measures included in the process, confirming the importance of emotional health in the mechanism of self-assessment health. This result is consistent with what has been found among Finnish oldest-old individuals by Lisko and colleagues (Lisko et al. 2020), who considered depression as a measure of psychological and emotional health. The same double effect of emotional health in the process of self-assessment was also found among Italian elderly people by Golini and Egidi (2016), who measured it with a similar latent construct.
Functional health also plays an important role in the process of self-assessment of health of the oldest-old individuals. The direct effect is stronger than the effect of emotional health, indicating that being able to perform daily activities or not having motion impairments is very important for the oldest-old individuals to positively rate their health. Even though it is not the strongest component of the mechanism, functional health resulted directly associated to SRH among Italian elderly as well as mobility among Finnish nonagenarians (Golini and Egidi 2016; Lisko et al. 2020). In accordance to what has been found by Golini and Egidi (2016), functional health has also an indirect effect on SRH among Italian nonagenarians, confirming its importance in the process of self-assessment of health.
The presence of chronic diseases does not play a main (direct effect) role in the mechanism of self-rating health among Italian nonagenarians. This result is in contrast with what has been observed for elderly Italians, for whom the presence of chronic disease was the main driver of poor SRH (Golini and Egidi 2016). One possible explanation is that younger elderly people are less used to living with chronic diseases than the oldest-old people: the timing of occurrence might be the key factor here. An additional explanation could be that the diseases considered in this study are less strongly related to SRH than the ones analyzed by other scholars. Lisko and colleagues, for instance, included separately many different diseases in their model and found heart disease (directly), arthritis and dementia (indirectly) to be related to SRH (Lisko et al. 2020). They, in particular, considered dementia as a key factor in the process of self-assessment of health. For this reason, they analyzed the subsample of people affected by dementia, finding that dementia weakens both direct and indirect associations of observed and latent variables with SRH (Lisko et al. 2020). In the present study, excluding from the analysis non-testable individuals, those who are in the worst health conditions (mainly cognitive) (Strozza et al. 2020a), did not change the results obtained on the total population (see Supplementary Materials). However, it has not been possible to perform the same analysis on the subsample of non-testable individuals because of the small sample size.
SES does not have a direct effect on SRH, similarly to what has been found by Au and Johnston (2014) among Australian. However, as for the presence of chronic disease, it has an indirect effect on SRH by influencing functional health, confirming that socioeconomic health disparities persist among nonagenarian (Enroth et al. 2013, 2019; Strozza et al. 2020a; Strozza et al., 2020b). This result suggests that SES by itself does not influence the perception of health of the individuals, contrary to what was hypotesized, that highly educated people or people living in a better economic condition perceive their health differently from those who are less educated or wealthy. The association between SES and SRH might be explained through other health factors that are directly influenced by the SES and that are associated to SRH. This was anticipated by Jylhä (2009) when outlying her theoretical model and confirmed by our results. However, these results should be interpreted with caution. Since our study is based on cross-sectional data, it is not possible to exclude the possibility of reverse-causality when analyzing the relationship between SES and health. It is plausible that worse health conditions throughout the lifecourse could lead to worse SES. Additionally, the construction of the latent variable may introduce additional bias, as living conditions are part of the SES construct. It is worth considering that individuals who live alone at very old ages may be self-selected for good health, as only those with sufficiently good health are able to manage independently. This could potentially explain the association between SES and age, as older nonagenarians have lower SES. As health tends to deteriorate with age, it is more common for individuals to reside in nursing homes or live with relatives. Further investigation is necessary to determine whether these findings are consistent among the oldest-old individuals in other populations.
These results suggest that at older ages, oldest-old individuals with the same cultural background (Italian) share a similar mechanism of evaluation of their own health with younger-old individuals. This result is extremely important as it brings new evidence to the discussion of cross-age differences in SRH. It is known that, when growing older, the standards for considering one’s health as good become lower. However, it is not clear whether the importance given to certain aspects of health when rating the own health conditions change. Lazarevič and Brandt (2020) investigated such difference in several countries, finding that between adults and elderly there were quite some differences in terms of health dimensions influencing SRH. However, they could not investigate differences between younger-old and oldest-old individuals as the survey did not include a sufficiently large group of very old people (Lazarevič and Brandt 2020). The results of this paper bring evidence on the cross-age comparison of SRH at older ages that was never explored before. Despite some questioning on the reliability of SRH as overall health measure at very old ages, European and American research shows that it remains a valid measure to capture objective health changes over time and to predict mortality as a consequence of health worsening (Galenkamp et al. 2013; Vogelsang 2014; Vuorisalmi et al. 2012). Our results suggest that even at very old ages, SRH is still sensitive to some objective health measures as functional health and presence of chronic diseases.
The present study has some strengths and limitations. The uniquely rich health data on nonagenarians (Mugello Study) and the use of a powerful statistical method as SEM are the two major strengths of this study. However, the cross-sectional nature of the data does not allow us to tackle the causal relationships between the latent and observed variables included in the model. Furthermore, we do not account for individual heterogeneity in the process of self-rating health. However, Hirve et al. (2014) showed that cultural background and individual-specific reporting behavior do not alter the mechanism of SRH (Hardy et al. 2014).
5 Conclusions
Overall, our study brings new evidence on the process of self-assessment of health among oldest-old individuals. The findings, even though with some differences, are coherent with the only other study on the topic we were able to find in the literature (Lisko et al. 2020). Our result suggests that self-assessment of health has the same structure among younger- and oldest-old people when sharing similar cultural background. To add important pieces to the puzzle, additional studies comparing different cultural contexts and different age groups, including the oldest-old one, are necessary (Lazarevič and Brandt 2020).
Finally, given the broad use of SRH, understanding the mechanism of self-assessment of health is crucial to correctly interpret the results obtained when SRH is used as an indicator of general health. Studies investigating the process of self-assessment of health at different ages, from younger to older ones, and in different countries are present in literature. However, many more studies are necessary to disentangle such mechanism among older individuals. The oldest-old population is the fastest growing segment of the population in many high-income countries (Christensen et al. 2009). As their participation to demographic and social surveys is increasing, and it is expected to increase even more in the coming years, future estimates of the health conditions of the oldest-old population should become more available and reliable. Since SRH is commonly measured in general surveys, extending the knowledge on how long-lived individuals assess their own health becomes crucial. It will help policy makers to better understand the needs of the older individuals populating modern societies.
References
Alonso, J., Vilagut, G., Adroher, N.D., Chatterji, S., He, Y., Andrade, L.H., Bromet, E., Bruffaerts, R., Fayyad, J., Florescu, S., de Girolamo, G., Gureje, O., Haro, J.M., Hinkov, H., Hu, C., Iwata, N., Lee, S., Levinson, D., Lépine, J.P., …, Kessler, R.C.: Disability mediates the impact of common conditions on Perceived Health. PLoS ONE. 8(6) (2013). https://doi.org/10.1371/journal.pone.0065858
Au, N., Johnston, D.W.: Self-assessed health: What does it mean and what does it hide? Soc. Sci. Med. 121, 21–28 (2014). https://doi.org/10.1016/j.socscimed.2014.10.007
Bamia, C., Orfanos, P., Juerges, H., Schöttker, B., Brenner, H., Lorbeer, R., Aadahl, M., Matthews, C.E., Klinaki, E., Katsoulis, M., Lagiou, P., Bueno-de-mesquita, H.B., Eriksson, S., Mons, U., Saum, K.-U., Kubinova, R., Pajak, A., Tamosiunas, A., Malyutina, S., …, Trichopoulos, D.: Self-rated health and all-cause and cause-specific mortality of older adults: Individual data meta-analysis of prospective cohort studies in the CHANCES Consortium. Maturitas. 103, 37–44 (2017). https://doi.org/10.1016/j.maturitas.2017.06.023
Chang-Quan, H., Xue-Mei, Z., Bi-Rong, D., Zhen-Chan, L., Ji-Rong, Y., Qing-Xiu, L.: Health status and risk for depression among the elderly: A meta-analysis of published literature. Age and Ageing. 39(1), 23–30 (2010). https://doi.org/10.1093/ageing/afp187
Christensen, K., Doblhammer, G., Rau, R., Vaupel, J.W.: Ageing populations: The challenges ahead. The Lancet. 374(9696), 1196–1208 (2009). https://doi.org/10.1016/S0140-6736(09)61460-4
R Core Team:. R: A Language and Environment for Statistical Computing. (2022). https://www.r-project.org/
de Bruin, A., Picavet, H.S.J., Nossikov, A. (eds.): Health Interview Surveys: Towards International Harmonization of Methods and Instruments. World Health Organization, Regional Office for Europe (1996)
Enroth, L., Raitanen, J., Hervonen, A., Jylha, M.: Do socioeconomic Health differences persist in Nonagenarians? The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 68(5), 837–847 (2013). https://doi.org/10.1093/geronb/gbt067
Enroth, L., Veenstra, M., Aartsen, M., Kjær, A.A., Nilsson, C.J., Fors, S.: Are there educational disparities in health and functioning among the oldest old? Evidence from the nordic countries. Eur. J. Ageing. 16(4), 415–424 (2019). https://doi.org/10.1007/s10433-019-00517-x
Forma, L., Aaltonen, M., Pulkki, J., Raitanen, J., Rissanen, P., Jylhä, M.: Long-term care is increasingly concentrated in the last years of life: A change from 2000 to 2011. Eur. J. Pub. Health. 27(4), 665–669 (2017). https://doi.org/10.1093/eurpub/ckw260
French, D.J., Sargent-Cox, K., Luszcz, M.A.: Correlates of Subjective Health across the aging lifespan: Understanding self-rated health in the Oldest Old. J. Aging Health. 24(8), 1449–1469 (2012). https://doi.org/10.1177/0898264312461151
Fýlkesnes, K., Førde, O.H.: Determinants and dimensions involved in self-evaluation of health. Soc. Sci. Med. 35(3), 271–279 (1992). https://doi.org/10.1016/0277-9536(92)90023-J
Galenkamp, H., Deeg, D.J.H., Huisman, M., Hervonen, A., Braam, A.W., Jylha, M.: Is self-rated Health still sensitive for changes in Disease and Functioning among Nonagenarians? The Journals of Gerontology Series B: Psychological Sciences and Social Sciences. 68(5), 848–858 (2013). https://doi.org/10.1093/geronb/gbt066
Golini, N., Egidi, V.: The latent dimensions of poor self-rated health: How chronic Diseases, functional and emotional dimensions interact influencing Self-Rated Health in Italian Elderly. Soc. Indic. Res. 128(1), 321–339 (2016). https://doi.org/10.1007/s11205-015-1033-3
Guilley, E., Bopp, M., Faeh, D., Paccaud, F.: Socioeconomic gradients in mortality in the oldest old: A review. Arch. Gerontol. Geriatr. 51(3), e37–e40 (2010). https://doi.org/10.1016/j.archger.2009.12.009
Hardy, M., Acciai, F., Reyes, A.: How Health Conditions translate into Self-Ratings: A comparative study of older adults across Europe. J. Health Soc. Behav. 55(3), 320–341 (2014). https://doi.org/10.1177/0022146514541446
Hirve, S., Oud, J.H.L., Sambhudas, S., Juvekar, S., Blomstedt, Y., Tollman, S., Wall, S., Ng, N.: Unpacking self-rated health and quality of life in older adults and Elderly in India: A structural equation Modelling Approach. Soc. Indic. Res. 117(1), 105–119 (2014). https://doi.org/10.1007/s11205-013-0334-7
Hu, L., Bentler, P.M.: Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychol. Methods. 3(4), 424–453 (1998). https://doi.org/10.1037/1082-989X.3.4.424
Hu, L., Bentler, P.M.: Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 6(1), 1–55 (1999). https://doi.org/10.1080/10705519909540118
Idler, E., Cartwright, K.: What do we rate when we rate our health? Decomposing age-related contributions to self-rated health. J. Health Soc. Behav. 59(1), 74–93 (2018). https://doi.org/10.1177/0022146517750137
Johnson, R.J., Wolinsky, F.D.: The structure of Health Status among older adults: Disease, disability, functional limitation, and Perceived Health. J. Health Soc. Behav. 34(2), 105–121 (1993). https://doi.org/10.2307/2137238 JSTOR
Jürges, H., Avendano, M., Mackenbach, J.P.: Are different measures of self-rated health comparable? An assessment in five european countries. Eur. J. Epidemiol. 23(12), 773–781 (2008). https://doi.org/10.1007/s10654-008-9287-6
Jylhä, M.: What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 69(3), 307–316 (2009). https://doi.org/10.1016/j.socscimed.2009.05.013
Jylhä, M., Leskinen, E., Alanen, E., Leskinen, A.-L., Heikkinen, E.: Self-Rated Health and Associated factors among men of different Ages. J. Gerontol. 41(6), 710–717 (1986). https://doi.org/10.1093/geronj/41.6.710
Katz, S.: Studies of illness in the aged: The Index of ADL: A standardized measure of biological and psychosocial function. JAMA. 185(12), 914 (1963). https://doi.org/10.1001/jama.1963.03060120024016
Kupek, E.: Beyond logistic regression: Structural equations modelling for binary variables and its application to investigating unobserved confounders. BMC Med. Res. Methodol. 6(1) (2006). https://doi.org/10.1186/1471-2288-6-13
Lazarevič, P., Brandt, M.: Diverging ideas of health? Comparing the basis of health ratings across gender, age, and country. Soc. Sci. Med. (2020). https://doi.org/10.1016/j.socscimed.2020.112913
Liang, J., Bennett, J., Whitelaw, N., Maeda, D.: The structure of self-reported Physical Health among the aged in the United States and Japan. Med. Care. 29(12), 1161–1180 (1991)
Lisko, I., Törmäkangas, T., Jylhä, M.: Structure of self-rated health among the oldest old: Analyses in the total population and those living with dementia. SSM - Population Health. 11, 100567 (2020). https://doi.org/10.1016/j.ssmph.2020.100567
Luppa, M., Luck, T., Weyerer, S., Konig, H.-H., Brahler, E., Riedel-Heller, S.G.: Prediction of institutionalization in the elderly. A systematic review. Age and Ageing. 39(1), 31–38 (2010). https://doi.org/10.1093/ageing/afp202
Mackenbach, J.P., Roskam, A.-J.R., Schaap, M.M., Menvielle, G.: Socioeconomic inequalities in Health in 22 european countries. N Engl. j. Med. 14 (2008). https://doi.org/10.1056/NEJMsa0707519
Molino-Lova, R., Sofi, F., Pasquini, G., Gori, A., Vannetti, F., Abbate, R., Gensini, G.F., Macchi, C.: The Mugello Study, a survey of nonagenarians living in Tuscany: Design, methods and participants’ general characteristics. Eur. J. Intern. Med. 24(8), 745–749 (2013). https://doi.org/10.1016/j.ejim.2013.09.008
Muthén, B.: Latent variable structural equation modeling with categorical data. J. Econ. 22(1–2), 43–65 (1983). https://doi.org/10.1016/0304-4076(83)90093-3
Nagi, S.Z.: Some conceptual issues in disability and rehabilitation. https://doi.org/null (1965)
Nybo, H., Petersen, H.C., Gaist, D., Jeune, B., Andersen, K., McGue, M., Vaupel, J.W., Christensen, K.: Predictors of mortality in 2,249 Nonagenarians—The danish 1905-Cohort survey. J. Am. Geriatr. Soc. 51(10), 1365–1373 (2003). https://doi.org/10.1046/j.1532-5415.2003.51453.x
Padua, L., Pasqualetti, P., Coraci, D., Imbimbo, I., Giordani, A., Loreti, C., Marra, C., Molino-Lova, R., Pasquini, G., Simonelli, I., Vannetti, F., Macchi, C.: Gender effect on well-being of the oldest old: A survey of nonagenarians living in Tuscany: The Mugello study. Neurol. Sci. 39(3), 509–517 (2018). https://doi.org/10.1007/s10072-017-3223-z
Rosseel, Y.: lavaan: An R Package for Structural equation modeling. J. Stat. Softw. 48(2) (2012). https://doi.org/10.18637/jss.v048.i02
Schulz, R., Heckhausen, J., O’Brien, A.: Negative affect and the disablement process in late life: A life-span control theory approach. In: Behavior, Health, and Aging, pp. 119–133. Lawrence Erlbaum Associates Publishers (2000)
Simonsson, B., Molarius, A.: Self-rated health and associated factors among the oldest-old: Results from a cross-sectional study in Sweden. Archives of Public Health. 78(1) (2020). https://doi.org/10.1186/s13690-020-0389-2
Stoller, E.P.: Self-assessments of Health by the Elderly: The impact of Informal Assistance. J. Health Soc. Behav. 25(3), 260 (1984). https://doi.org/10.2307/2136424
Strozza, C., Pasqualetti, P., Egidi, V., Loreti, C., Vannetti, F., Macchi, C., Padua, L.: Health profiles and socioeconomic characteristics of nonagenarians residing in Mugello, a rural area in Tuscany (Italy). BMC Geriatr. 20(1) (2020a). https://doi.org/10.1186/s12877-020-01689-3
Strozza, C., Zarulli, V., Egidi, V.: Understanding Health Deterioration and the Dynamic Relationship between Physical Ability and Cognition among a Cohort of Danish Nonagenarians. Journal of Aging Research, 2020b, 1–8. (2020b). https://doi.org/10.1155/2020b/4704305
Vogelsang, E.M.: Self-rated Health Changes and Oldest-Old Mortality. The Journals of Gerontology: Series B. 69(4), 612–621 (2014). https://doi.org/10.1093/geronb/gbu013
Vuorisalmi, M., Sarkeala, T., Hervonen, A., Jylhä, M.: Among nonagenarians, congruence between self-rated and proxy-rated health was low but both predicted mortality. J. Clin. Epidemiol. 65(5), 553–559 (2012). https://doi.org/10.1016/j.jclinepi.2011.11.001
Ware, J.E., Kosinski, M., Keller, S.D.: A 12-Item short-form Health Survey: Construction of Scales and preliminary tests of reliability and validity. Med. Care. 34(3), 220–233 (1996). https://doi.org/10.1097/00005650-199603000-00003
Funding
The Mugello Study was partially supported by the Italian Ministry of Health within the Current Research Program performed at National Research Institutes (IRCCS). Cosmo Strozza’s research is supported by the AXA Research Fund, through funding for the AXA Chair in Longevity Research. The other authors received no financial support for the research, authorship, and/or publication of this article.
Open access funding provided by University Library of Southern Denmark
Author information
Authors and Affiliations
Contributions
CS conceptualized the study. CS, VE, and PP contributed to the design of the study. FV, FC, CM contributed to data acquisition. CS analyzed the data. CS, VE, and PP contributed to the interpretation of the results. CS wrote the first draft of the manuscript. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Strozza, C., Egidi, V., Vannetti, F. et al. Self-assessment of health: how socioeconomic, functional, and emotional dimensions influence self-rated health among Italian nonagenarians. Qual Quant (2023). https://doi.org/10.1007/s11135-023-01724-6
Accepted:
Published:
DOI: https://doi.org/10.1007/s11135-023-01724-6