
Abstract
Sufficient and nourishing foods during the early years of a child’s life are essential for optimal growth and healthy life. The existing disparities among rural-urban populations also affect the dietary pattern as well. Therefore, this study aims to identify the factors that contribute towards the rural-urban disparity in children’s dietary diversity (CDD) and quantify their importance for the reduction of rural-urban disparities in achieving a minimum dietary diversity level. Using Pakistan Demographic and Health Survey (PDHS) data, version 2017-18, a non-linear decomposition analysis was performed. Eighty-one (81%) of the gap in CDD between rural-urban areas is attributed to the differences in the observed factors (endowments) and of these most of the difference is explained by three factors i.e. number of antenatal care visits (45%), maternal education (18%) and type of toilet facility (15%). There is a need to explore maternal education-related interventions to decrease the rural-urban gap regarding CDD as maternal education may affect CDD through different dimensions. Moreover, such programs should be initiated that may be helpful to enhance women’s role in society, such as skilled education, well-paid job opportunities and better health facilities.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Inroduction
Sufficient and nourished foods during the early years of a child’s life are essential for optimal growth and healthy life (Kumera et al. 2018). Also, the poor nutritional status during infancy may cause long lasting severe consequences for learning and future productivity (Victora et al. 2008). A child being stunted, i.e. having low height for age, may be considered to be deprived of required nutrients for linear growth. Therefore, interventions, to improve nutritional level during infancy, have been found to be crucial to later life outcomes in cognitive and physical ability (Asuman et al. 2019). Moreover, under-nutrition is a major cause of child mortality, accounting for about 45% of child deaths (Black et al. 2013) so, the governments have to be committed to mitigate malnutrition among children by 2030, under the sustainable development goals (SGDs), set by United Nations in 2015.
Globally 151 million children were reported to be stunted in 2017, and about 24% children of age less than five years in low- and middle-income countries (LIMCs) had stunted growth (UNICEF, 2018). A recently published report demonstrated that about 135 million people were acutely food insecure and Africa is the major contributor (73 million) of this insecure situation. The Middle-East and Asia are at number second with 43 million people with insecure food (FSIN, 2020). The corona virus also worsens the people’s financial situation, especially daily wage earners, due to unemployment or under-employment which severely reduces their purchasing power and this in turn severely affects their dietary pattern.
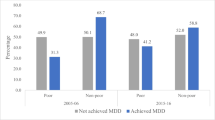
According to the World Health Organization (WHO) guidelines complementary foods may be introduced at the age of six months to meet essential nutritional requirements. In this sense child dietary diversity (a proxy indicator of adequate micronutrient density of complementary foods beside breastfeeding) refers to the consumption of a variety of food groups that may be capable of ensuring adequate intake of essential nutrients (Kumera et al. 2018). Consumption of at least 4 or more food groups out of seven food groups, recommended by WHO, is considered as minimum dietary diversity level for children aged 6–23 months (WHO, 2008). According to recently published document one out of three children of age 6–23 months meets the minimum dietary diversity in the world (FAO 2020) while there exist disparities in achieving minimum dietary diversity level among rural-urban residents (that is 27.4% for rural children and 35.1% for urban children) (Micha et al. 2020).
In Pakistan, being the sixth largest country by population, malnutrition is a predominant public-health challenge which might be due to persistent poverty, non-availability/insufficient quantity of food or unequal and poor purchasing power of the people (Iqbal et al. 2017). About 17.7% of the children are acutely malnourished while 14.2% of the children of age 6–23 months consume the minimum required diet during the past 24 h (FSIN, 2020). Moreover, there exist inequalities in provision of diverse food to children among rural urban areas (NNS, 2019). Evidence showed that 25.8% children of age 6–23 months meet the recommended minimum dietary diversity in urban areas while this goes down to 18.3% in rural areas (PDHS, 2019). Hence, for Pakistan, being a nation of about 207.8 million people with 12.4% of the population living below the poverty line and dietary diversity is poor (Iqbal., 2018), it is necessary to highlight the important factors that may contribute for the improvement in child dietary diversity pattern and effectively reduce this rural- urban gap.
The published literature demonstrated the linkages between environmental factors such as water and sanitation and nutritional outcome of the children (Shreshtha et al., 2020; Bekele et al. 2020), however, there is a need to explore these socio-economic factors in the sense that neat and clean drinking water and improved sanitation may improve the dietary pattern of the children which in turn may result as the children’s better nutritional level. Also, the association between child dietary diversity and different socio-economic factors has been documented in literature for different countries (Kuche et al. 2020; Custodio et al. 2019; Kumera et al. 2018; Sarosh et al., 2017; Amugsi et al. 2016) however, decomposition analysis using recently developed empirical methods is rare (Bauer et al. 2007). Though, few studies have addressed the inequality problem and assessed different factors of health outcomes for Pakistan (Asif, et al., 2020; Raza et al. 2018). However, none has considered the dietary diversity inequality among rural-urban areas and its contributing factors for Pakistan so far. Therefore, this study aims, to identify different socioeconomic factors that contribute towards the rural-urban disparity in CDD and to quantify their relative importance for the reduction of rural-urban gap, using an extended version of Oaxaca-Blinder decomposition method for non-linear response (child’ dietary diversity scores). This analysis may also set some guidelines to identify the sustainable policy measures to achieve universal child dietary patterns for both rural-urban areas in the line of SDGs.
2 Methods
2.1 Data description
Findings of this study are based on the nationally representative Pakistan Demographic and Health Survey (PDHS) data, version 2017-18 (PKKR71FL file of the data). Following two-stage stratified sampling procedure, 580 primary sampling units (PSUs) (295 rural and 285 urban) were selected at first stage and out of these PSUs 16,240 households were selected at second stage. The information of about 12,708 children of age less than 5 years is available in the data. However, 3,443 children of age 6–23 months are included in this analysis subject to the age limits considered for child dietary diversity measurement following WHO’s guidelines. Further details about sampling procedures can be seen elsewhere (PDHS, 2019).
Children’s dietary diversity (CDD) score is the main outcome variable of this analysis and is constructed following WHO’s guidelines (WHO, 2008). In literature, other studies on the topic has also adopted this methodology (Fentahun et al. 2016; Frempong and Annim, 2017; Perkins et al. 2018). Data on twelve food items, which a child consumed during the last 24 h, are used to form seven food groups which comprise of (1) grains/roots/tubers, (2) legumes/nuts, (3) dairy products, (4) flesh foods, (5) eggs, (6) vitamin A rich foods and (7) other vegetables and fruits. A child consuming at least one food item from a specific food group is worth one point and zero otherwise. The scores of all seven groups is then added up to obtain dietary diversity score, ranging from zero to seven (0–7).
Other factors (explanatory variables) incudes parental education in years, child gender (male/female), antenatal care visit (considered 1 if mother has completed at least four antenatal care visits following WHO’s guidelines and zero otherwise), gender of household head (male/female), water source of household (improved/unimproved), type of toilet facility (improved/unimproved), maternal working status (working/not-working) and number of household members.
2.2 Statistical analysis
Statistical analysis was performed in three folds using Stata version 15.0 (Stata Corp, College Station, TX, USA). At first, distribution of the response variable and existence of possible inequality among rural-urban areas regarding CDD was checked through graphical examination. Secondly, mean and standard deviations of the selected covariates and response variable were calculated and difference in their means were tested. Moreover, chi-square test was performed to test the bivariate association among categorical variables and the CDD. At third, the Oaxaca-Blinder (OB) decomposition method, originally developed by Oaxaca (1973) and Blinder (1973), was performed using stata command “mvdcmp” to determine the factors responsible for the disparities in CDD among rural-urban areas. The standard Oaxaca-Blinder decomposition assumes that the outcome variable (CDD in this analysis) is linearly related to the covariates (X), and that the error term (ε) is conditionally independent of X:
CDDgi = βg0 + \(\sum _{k=1}^{K}{\beta }_{gk}{X}_{ki}\) + εgi, g = urban(U), rural(R),
where CDDgi is the diversity scores of \(ith\)child residing in area g and X is the vector of selected covariates. In OB analysis the overall gap regarding CDD among rural-urban areas can be split in to two parts. The first part, the explained part (the part which explains the gap that is due to the differences in selected characteristics between rural and urban areas) and the second part known as unexplained part (the part that is due to differences in the estimated coefficients). Generally, it is hard to interpret the unexplained part (Heady, 2014). Commonly, the OB-decomposition has been applied in the context of linear regression modelling in previous literature (Sharaf et al., 2016), however, non-linear outcomes such as discrete or limited dependent variables, as in our case, needs the estimation of some non-linear models (Bauer et al. 2007). Since, the ordinary least square regression yields inconsistent estimates and in turn decomposition analysis may produce misleading results, therefore, we have adopted an extended version of standard OB decomposition method for discrete outcome variables purposed by Bauer and Sinning (2008) for this analysis.
As the outcome variable in this study is children’s dietary diversity scores (the number of food groups consumed by the child in last 24 h), which takes on only positive integer values ranging from zero to seven (Fig. 1), thus a count data modelling approach is suitable and therefore, we can estimate the parameters (betas) in above equation using count data model (Bauer et al. 2007), under maximum likelihood method, both for rural/urban groups separately. However, possible existence of overdispersion (when the variance of the responses is greater than the mean in a Poisson regression model) should be tested, while modelling count response data because in studying count data, it’s important to be aware of the consequences of overdispersion, as failing to do so leads to inaccurate model parameter interpretations. In this analysis ratio of the Pearson chi-square statistic to its corresponding degrees of freedom (McCullagh and Nelder 1989) was used to determine whether overdispersion is present or not in data set used, and in the line of this ratio we have decided to consider the Poisson modelling as this ratio meets the criteria discussed in literature (Payne et al. 2018).

Non-linear nature of children’s dietary diversity
The contribution of each variable to the overall dietary diversity gap between rural-urban areas is also considered in this analysis. However, results of detailed decomposition, in case of non-linear outcomes, are sensitive to the order in which the factors enter the decomposition equation (Hirvonen, 2016; Bauer et al. 2007). Therefore, weighing methodology purposed by Yun (2004) is used to handle this issue. All statistical tests were two-sided, and differences were considered statistically significant at p < 0.05.
3 Results
Figure 2 demonstrated a significant rural-urban gap in child dietary diversity. Moreover, the existing inequality among rural-urban areas regarding the selected covariates is also presented in Table 1. The ratio of the Pearson chi-square statistic to its corresponding degrees of freedom was found to be approximately equals to one (3484.097/3434 = 1.01) and this demonstrates the absence of over dispersion in the response variable. The descriptive analysis demonstrated that, on the average, one to four groups have been used by children among the studied sample (Table 2). Only a little number of children have consumed al the seven good groups during 24-hours. Interestingly, ANC is more prevalent among urban women (68.1%) as compared to rural. Majority of the households have both improved water and toilet facilities (Table 2). 81% (81%) of the gap in CDD between rural-urban areas is attributed to the differences in the observed factors (endowments) and of these most of the difference is explained by three factors i.e. number of antenatal care visits (45%), maternal education (18%) and type of toilet facility (15%). 6% (6%) of the gap is also due to difference in parental education however, this result remained insignificant (Table 3).

Children’s dietary diversity by age in rural-urban areas and overall
4 Discussions
This analysis contributes to existing literature addressing rural-urban gap regarding child dietary diversity and its contributing factors. It also highlighted the association of maternal and other important factors with child’s likelihood of achieving minimum dietary diversity level, which in turn play important role in child’s nutritional outcome.
This analysis reported, maternal education, number of antenatal care visits during pregnancy and household’s sanitation type, as significant factors among the selected covariates. Of these number of mother’s antenatal care visits is the highest contributing factors (45%) addressing the rural-urban gap regarding CDD. Few pathways, through which mother’s self-care attitude, such as ANC may affect the children’s dietary pattern and healthcare, are might be as follows. First, achieving minimum number of antenatal visits can be considered as an important element of maternal empowerment. Since, the association of different maternal health indicators and women’s empowerment is well documented in literature (Osamor and Grady 2016; Sado et al. 2014). A review of 67 studies in developing countries demonstrated a positive association between maternal empowerment and use of health services, like antenatal visits during pregnancy (Pratley 2016). Another study found that a higher maternal autonomy was associated with more use of maternal health services (Adhikari 2016). Moreover, maternal role in making decision about her own health is among the important factors describing the household’s decision-making autonomy (Asif and Akbar 2020). Second, a mother who had completed the WHO’s recommended (at least four) antenatal visits, during pregnancy period, is considered to be well aware of the importance of health care for herself as well as for her child. Moreover, self-caring mothers also take healthy and diverse diet during pregnancy which is one of the best strategies among pregnant women (Desta et al. 2019) and this may also be considered that self-caring mothers are highly caring regarding breastfeeding and other complementary feedings of her siblings and even mothers reduce their intake to secure those of infants and small children (USAID, 2012). Third, mother’s health seeking behaviour, including ANC visits, also promotes the health behaviours inside the household, including healthy environment, early childhood vaccination and nutritious and diverse diet for family (Lincetto et al. 2006). Thus, mother’s ANC status may be considered as an important factor in household’s well-being and reflect mother’s awareness about her healthcare/diet pattern as well as for her child.
Maternal education is at number second (18%) among the contributing factors of CDD gap among rural-urban areas. Since, the maternal role is well documented in the literature addressing the welfare of children (Asif et al. 2019; Asif and Akbar 2020). Also, UNICEF’s conceptual framework for child nutrition has linked maternal role (at underlying layer) with children’s nutritional outcome through CDD (at immediate layer) (UNICEF, 1990). Education is the most important dimension of maternal empowerment also (Duflo 2012). Since, through better educational level, mother’s would be enlightened and be more conscious; and therefore can make better decisions for herself as well as for her children. Moreover, literate mothers can easily comprehend the benefits of ANC and thus expected to utilize it more effectively (Okedo-Alex et al. 2019). In addition, an educated woman, being more confident, might communicate better with the health service providers to get required healthcare both for herself as well as for her child (Bloom et al. 2001). Also, an educated mother may get well paid jobs and be more financially empowered which positively affect the children’s dietary pattern. Thus, the impact of maternal education may also be channelized, through mother’s better health knowledge, and better feeding practices, as a protective measure of CDD.
Water, sanitation, and hygiene (WASH) is among the important factors affecting the childcare (Asif and Akbar 2020). We have considered water facility and sanitation type in this analysis and of this improved toilet facility contributed a larger part (15%) in the explained portion of the rural-urban gap, while type of water facility remains insignificant. Thus, being an important factor, sanitation type could play important role in assessing the household’s socioeconomic status. As there is greater chance that poor households are more likely to have unimproved sanitation, and thus likely to be categorised as poor. However, with the passage of time, poor household that improve their sanitation type are likely to fall in the middle or wealthier quintile of wealth index in subsequent surveys (Rheingans et al. 2014). Also, due to higher fertility among poor households (Milanovic, 1996), the unimproved sanitation, in terms of health effects, may affect the children’s nutritional level through unbalance and insufficient food.
However, though water source remains insignificant in this analysis, it is important for child’s better nutritional status through sufficient and nutritious dietary pattern (Choudhary et al. 2020). Improved water facility may affect household food diversity, which in turn may affect children’s dietary diversity position and thus, need to be further explored in other studies.
Besides, these other factors such as number of household member and maternal working status, though, did not shown significant contribution in explaining the rural-urban gap in this analysis, yet they are important. A recent study has outlined that an increase in household’s residents may increase the likelihood of being classified as low dietary diversity (Huluka and Wondimagegnhu 2019). The reason behind might be that increase number of children with limited income source may stretch these resources over wider range of competing needs which in turn, may lead to lower dietary diversity specially among children. Also, working mothers may have less time to serve their families. Such as working mothers could not prepare complementary foods. Also, in rural areas mostly women bear many responsibilities such as fetching of water, look-after of animals and household cleanliness which take much time and this results as insufficient time availability for preparing and feedings of complementary foods for their children.
In view of above discussion, we may conclude that improved WASH facilities might be the signal of an improved socio-economic status (SES), which in turn play an important role in reducing rural-urban gap. Also, the role of maternal education is of prominent nature. As all the contributing factors such as ANC and household WASH factors are connected to the mother’s ability to understand these basic requirements for the welfare of her family. Also, a complete ANC may also be attributed to improved SES because mothers of socio-economically better households have better autonomy in the family (Nigatu et al. 2014; Tiruneh et al. 2017; Sebayang et al. 2019) and thus careful about herself as well as for her children. Thus, it may also be stated that mothers with better ANC, having higher educational level and improved WASH facilities have better SES which in turn helps to reduced CDD gap.
Thus, there is need to explore maternal education related interventions to decrease the rural-urban gap regarding CDD. Such programmes should be initiated that may helpful to enhance women’s role in the society, such as skilled education, well paid job opportunities and better health facilities. Moreover, the provision of supplement food on subsidized rate may be useful for eradication of poor dietary diversity. Optimal and equal access to improved water and sanitation can increase the likelihood of reducing inequality in achieving minimum dietary requirements, through better socio-economic status, and therefore, can have potential effect on child’s nutritional level through different pathways separate from WASH. Moreover, the extent CDD is also associated with the consumption of sufficient micronutrient and macronutrients which may have implications for child’s nutritional level which need further research in this area using different empirical methods.
The findings of this study, however, should be considered subject to few limitations. First, cross sectional nature of data limits us to know the casual relationship between the outcome and explanatory variables. Second, this analysis does not consider survey weights due to the following reasons. Firstly, oversampling from some parts of population and then post survey adjustments cause variation in weights across the sample which adversely affects precision of parameters’ estimates (De Leeuw et al. 2012). Secondly, post survey adjustments may increase standard errors of the estimates, which adversely affects statistical modelling (Young and Johnson 2012). Despite the above limitations, secondary analysis of demographic and health surveys data is thought to be a sufficient contribution to public health knowledge in developing countries and we believe that our findings can help in child health related interventions.
References
Adhikari, R.: Effect of Women’s autonomy on maternal health service utilization in Nepal: a cross sectional study. BMC women’s health. 16(1), 26 (2016)
Amugsi, D.A., Dimbuene, Z.T., Bakibinga, P., Kimani-Murage, E.W., Haregu, T.N., Mberu, B. Dietary diversity, socioeconomic status and maternal body mass index (BMI): quantile regression analysis of nationally representative data from Ghana, Namibia and Sao Tome and Principe.BMJ open, 6(9), e012615 (2016)
Asif, A.M., Akbar, M., Tahir, M.R., Arshad, I.A.: Role of Maternal Education and Vaccination Coverage: Evidence from Pakistan Demographic and Health Survey. Asia Pac. J. Public Health. 31(8), 679–688 (2019)
Asif, A.M., Akbar, M.: Inequalities in child health care in Pakistan: measurement and decomposition analysis of maternal educational impact. Pub Heal. 183, 94–101 (2020)
Asuman, D., Ackah, C.G., Fenny, A.P., Agyire-Tettey, F.: Assessing socioeconomic inequalities in the reduction of child stunting in sub-Saharan Africa.J Pub Heal,1–11(2019)
Bauer, T.K., Sinning: An extension of the Blinder–Oaxaca decomposition to nonlinear models. AStA Ad Stat Ana. 92(2), 197–206 (2008)
Bauer, T., Göhlmann, S., Sinning, M.: Gender differences in smoking behavior. Health Econ. 16(9), 895–909 (2007)
Bekele, T., Rawstorne, P., andand Rahman, B.: Effect of water, sanitation and hygiene interventions alone and combined with nutrition on child growth in low and middle income countries: a systematic review and meta-analysis. BMJ open. 10(7), e034812 (2020)
Black, R.E., Alderman, H., Bhutta, Z.A., Gillespie, S., Haddad, L., Horton, S., Walker, S.P.: Maternal and child nutrition: building momentum for impact. The Lancet. 382(9890), 372–375 (2013)
Blinder, A.S.: Wage discrimination: reduced form and structural estimates.Journal of Human resources,436–455(1973)
Bloom, S.S., Wypij, D., Gupta, M.D.: Dimensions of women’s autonomy and the influence on maternal health care utilization in a north Indian city. Demog. 38(1), 67–78 (2001)
Choudhary, N., Schuster, R., Brewis, A., Wutich, A.: Water insecurity potentially undermines dietary diversity of children aged 6–23 months: Evidence from India. Mat. and Child. Nut. 16(2), e12929 (2020)
Custodio, E., Herrador, Z., Nkunzimana, T., Węziak-Białowolska, D., Perez-Hoyos, A., Kayitakire, F.: Children’s dietary diversity and related factors in Rwanda and Burundi: A multilevel analysis using 2010 Demographic and Health Surveys. PloS one. 14(10), e0223237 (2019)
De Leeuw, E.D., Hox, J., Dillman, D.: International handbook of survey methodology. Routledge (2012)
Desta, M., Akibu, M., Tadese, M., Tesfaye, M.: Dietary diversity and associated factors among pregnant women attending antenatal clinic in Shashemane, Oromia, Central Ethiopia: a cross-sectional study.J nut and metab, (2019)
Duflo, E.: Women empowerment and economic development. J. Eco lit. 50(4), 1051–1079 (2012)
FAO, I.: and UNICEF. The State of Food Security and Nutrition in the World 2020. Transforming food systems for affordable healthy diets (2020)
Fentahun, N., Belachew, T., Lachat, C.: Determinants and morbidities of multiple anthropometric deficits in southwest rural Ethiopia. Nutrition. 32(11–12), 1243–1249 (2016). DOI: https://doi.org/10.1016/j.nut.2016.03.023
Frempong, R.B., Annim, S.K.: Dietary diversity and child malnutrition in Ghana. Heliyon. 3(5), e00298 (2017). DOI: https://doi.org/10.1016/j.heliyon.2017.e00298
FSIN (Food Security Information Network). Global Report on Food Crises: Joint Analysis for Better Decisions:, Available at: (2020). https://www.fsinplatform.org/sites/default/files/resources/files/GRFC_2020_ONLINE_200420.pdf as on 1 Nov, 2020
Hirvonen, K.: Rural–urban differences in children’s dietary diversity in Ethiopia: A Poisson decomposition analysis. Eco Let. 147, 12–15 (2016)
Huluka, A.T., Wondimagegnhu, B.A.: Determinants of household dietary diversity in the Yayo biosphere reserve of Ethiopia: An empirical analysis using sustainable livelihood framework. Cog Food and Agri. 5(1), 1690829 (2019)
Iqbal, S., Zakar, R., Zakar, M.Z., Fischer, F.: Factors associated with infants’ and young children’s (6–23 months) dietary diversity in Pakistan: evidence from the demographic and health survey 2012–13. Nut j. 16(1), 78 (2017)
Kuche, D., Moss, C., Eshetu, S., Ayana, G., Salasibew, M., Dangour, A.D., Allen, E.: Factors associated with dietary diversity and length-for‐age z‐score in rural Ethiopian children aged 6–23 months: A novel approach to the analysis of baseline data from the Sustainable Undernutrition Reduction in Ethiopia evaluation. Mat. and chi nut. 16(1), e12852 (2020)
Kumera, G., Tsedal, E., Ayana, M.: Dietary diversity and associated factors among children of Orthodox Christian mothers/caregivers during the fasting season in Dejen District, North West Ethiopia. Nut and metab. 15(1), 16 (2018)
Lincetto, O., Mothebesoane-Anoh, S., Gomez, P., Munjanja, S. Antenatal care. Opportunities for Africa’s newborns: Practical data, policy and programmatic support for newborn care in Africa, 55–62 (2006)
McCullagh, P., Nelder, J.A.: Generalized linear models. Chapman and Hall, London; New York (1989)
Micha, R., Mannar, V., Afshin, A., Allemandi, L., Baker, P., Battersby, J., … and Dolan, C. 2020 Global nutrition report: action on equity to end malnutrition (2020). Available at: (2020). https://globalnutritionreport.org/reports/2020-global-nutrition-report/. as on 1
Milanovic, B. Income, inequality and poverty during the transition: : a survey of the evidence.MOCT-MOST Eco Pol Tran Eco 6,131–147(1996)
Nigatu, D., Gebremariam, A., Abera, M., Setegn, T., Deribe, K.: Factors associated with women’s autonomy regarding maternal and child health care utilization in Bale Zone: a community based cross-sectional study. BMC women’s health. 14(1), 1–9 (2014)
NNS, National Nutrition Survey Key Findings Report:, Available at: (2018). (2018) https://www.unicef.org/pakistan/media/1871/file/KeyFindings-NationalNutritionSurvey2018.pdf. as on 1 Nov 2020
Oaxaca, R. Male-female wage differentials in urban labor markets.Int eco rev,693–709(1973)
Okedo-Alex, I.N., Akamike, I.C., Ezeanosike, O.B., Uneke, C.J.: Determinants of antenatal care utilisation in sub-Saharan Africa: a systematic review. BMJ open. 9(10), e031890 (2019)
Osamor, P.E., Grady, C.: Women’s autonomy in health care decision-making in developing countries: a synthesis of the literature. Int. j. wom heal. 8, 191 (2016)
Payne, E.H., Gebregziabher, M., Hardin, J.W., Ramakrishnan, V., Egede, L.E.: An empirical approach to determine a threshold for assessing overdispersion in Poisson and negative binomial models for count data. Commun. Statistics-Simulation Comput. 47(6), 1722–1738 (2018)
PDHS, Pakistan Demographic and Health Survey 2017-18 main findings report. Available at: https://nips.org.pk/abstract_files/PDHS%20Final%20Report%20 as%20of%20Jan%2022 – 2014.pdf as on 1 Nov, 2020
Perkins, J.M., Jayatissa, R., Subramanian, S.V.: Dietary diversity and anthropometric status and failure among infants and young children in Sri Lanka. Nutrition. 55, 76–83 (2018). DOI: https://doi.org/10.1016/j.nut.2018.03.049
Pratley, P.: Associations between quantitative measures of women’s empowerment and access to care and health status for mothers and their children: a systematic review of evidence from the developing world. Soc. Sci. and Med. 169, 119–131 (2016)
Raza, O., Lodhi, F.S., Morasae, E.K., Majdzadeh, R.: Differential achievements in childhood immunization across geographical regions of Pakistan: analysis of wealth-related inequality. Int. j. equ heal. 17(1), 122 (2018)
Rheingans, R., Anderson, J.D., Luyendijk, R., Cumming, O.: Measuring disparities in sanitation access: does the measure matter? Trop. Med. and Int. Heal. 19(1), 2–13 (2014)
Sado, L., Spaho, A., Hotchkiss, D.R.: The influence of women’s empowerment on maternal health care utilization: evidence from Albania. Soc. Sci. and Med. 114, 169–177 (2014)
Sebayang, S.K., Efendi, F., Astutik, E.: Women’s empowerment and the use of antenatal care services: analysis of demographic health surveys in five Southeast Asian countries. Women & health. 59(10), 1155–1171 (2019)
Sharaf, M.F., Rashad, A.S.: Regional inequalities in child malnutrition in Egypt, Jordan, and Yemen: a Blinder-Oaxaca decomposition analysis. Heal eco rev. 6(1), 23 (2016)
Shrestha, A., Six, J., Dahal, D., Marks, S., Meierhofer, R.: Association of nutrition, water, sanitation and hygiene practices with children’s nutritional status, intestinal parasitic infections and diarrhoea in rural Nepal: a cross-sectional study. BMC pub heal. 20(1), 1–21 (2020)
Tiruneh, F.N., Chuang, K.Y., Chuang, Y.C.: Women’s autonomy and maternal healthcare service utilization in Ethiopia. BMC Health Serv. Res. 17(1), 1–12 (2017)
UNICEF. Levels and trends in child malnutrition. eSocialSciences: : available at: (2018). https://www.who.int/nutgrowthdb/2018-jme-brochure.pdf as on 5 Nov, 2020
UNICEF. Strategy for Improved Nutrition of Children and Women in Developing Countries. A UNICEF Policy Review. ERIC Clearinghouse: (1990)
USAID:. Maternal dietary diversity and the implications for children’s diets in the context of food security.USAID(2012)
Victora, C.G., Adair, L., Fall, C., Hallal, P.C., Martorell, R., Richter, L., et al.: Maternal and child undernutrition: consequences for adult health and human capital. The lancet. 371(9609), 340–357 (2008)
World Health Organization:. Indicators for assessing infant and young child feeding practices: part 1: definitions: conclusions of a consensus meeting held 6–8 November 2007 in Washington DC, USA. World Health Organization (2008). (2008)
Young, R., Johnson, D.R. To weight, or not to weight, that is the question: Survey weights and multivariate analysis. In the American Association for Public Opinion Research (AAPOR) 67th Annual Conference 2012 May 17. (2012)
Yun, M.S.: Decomposing differences in the first moment. Eco let. 82(2), 275–280 (2004)
Acknowledgements
The authors wish to thank measuredhs.com for giving access to Pakistan demographic and health survey data for 2017-18.
Funding
This work was not funded by any source.
Author information
Authors and Affiliations
Contributions
AMA performed the data analysis and wrote the first draft of the manuscript. MA critically revised the manuscript and makes essential corrections. Both authors contributed to and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Ethical Statement
This study did not required ethical approval as a secondary data analysis was performed using Pakistan Demographic and Health Survey (PDHS) data for year 2017-18. Data was obtained from measuredhs.com after permission. PDHS data are collected with due ethical considerations.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Asif, A.M., Akbar, M. A non-linear decomposition analysis of children’s dietary diversity scores: explaining rural-urban inequality. Qual Quant 57, 3273–3284 (2023). https://doi.org/10.1007/s11135-022-01501-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11135-022-01501-x