
Abstract
Background
Medication use in older adults is increasing, therefore, reducing the risk of suboptimal medicine use is imperative in achieving optimal therapeutic outcomes. Research suggests that factors such as personal beliefs and beliefs about medicines may be associated with non-adherence and inappropriate medicine use.
Aim
To systematically review and identify quantitative research on the influence of beliefs about medicines and the relationship with suboptimal medicine use in older adults.
Method
Searches were conducted on PubMed, EMBASE, CINAHL, and PsycINFO for quantitative studies (inception to March 2023). Inclusion criteria: (1) exposure: participants’ beliefs (personal, cultural, and medication-related), (2) outcomes: polypharmacy, potentially inappropriate medicines use, or non-adherence, and (3) participants: community-dwelling adults 65 years or above. Study selection, data extraction and quality appraisal (Joanna Briggs Institute critical appraisal checklist) were completed independently by two investigators. Data were combined in a narrative synthesis and presented in a summary of findings table.
Results
Nineteen articles were included: 15 cross-sectional and four cohort studies. Outcomes of included papers were as follows; adherence (n = 18) and potentially inappropriate medicine use (n = 1). Ten studies found stronger beliefs in the necessity of medicines and/or fewer concerns led to better adherence, with one paper contradicting these findings. Three studies did not find associations between adherence and beliefs. One study confirmed an association between unnecessary drug use and a lack of belief in a "powerful other" (e.g. doctor).
Conclusion
Further investigation is necessary to (1) ascertain the importance of necessity or concern beliefs in fostering adherence and, (2) examine the influence of beliefs on polypharmacy and inappropriate medicine use.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Impact statements
-
The relationship between medication beliefs and adherence is multifaceted and can vary based on patient populations and other contextual factors.
-
Stronger beliefs in the necessity of medications and reduced concerns appear to positively influence medication adherence in older adults, however further investigation is needed to ascertain the relative importance of necessity or concern beliefs in fostering adherence.
-
There is a paucity of research on the influence of beliefs on polypharmacy and inappropriate medication use. Consequently, further research is needed.
Introduction
The number of medicines prescribed and utilised by older adults is increasing [1, 2]. Inappropriate use of medicines can result in treatment failure and can increase the risk of adverse events [3]. As such, inappropriate and suboptimal medicine use are significant safety concerns in this aging population [1, 4, 5]. Therefore, appropriate use of medicines is crucial in achieving optimal therapeutic outcomes.
Suboptimal medicine use can arise from various factors, including polypharmacy, non-adherence and the prescribing of potentially inappropriate medicines (PIMs) [5]. In a tertiary hospital setting, PIM use among older adults was found to be 55%, with 6% of all admissions attributed to PIM use [6]. Current research suggests that beliefs about medicines and personal beliefs may be associated with non-adherence and therefore suboptimal medicine use [3, 7,8,9].
Beliefs can be influenced by an individual’s personal and cultural beliefs, as well as those shaped by personal experiences [10]. Negative experiences can result from instances of adverse drug events, medication-related burden, polypharmacy and dissatisfaction with the healthcare system [11, 12]. Moreover, a 2016 review of qualitative studies explored patients' lived experiences with medications, revealing that medication-related burden significantly influences patients' well-being, beliefs and behaviours toward medicines [13]. The rapport and trust established between patients and their healthcare providers are also pivotal factors known to impact medication use [14]. Patients often develop their own experiences, beliefs, and perceptions of their medications, which can subsequently shape their attitudes towards healthcare and the utilisation of medicines. Research also suggests that patients with a stronger belief in the necessity of their medicines with fewer concerns, demonstrate higher adherence to medicines with beliefs being identified as the most influential predictor of adherence [12, 15].
In this review, the term "beliefs" encompasses a broad spectrum of perspectives, including personal, cultural, and medication-related beliefs. The current literature employs various methods to measure beliefs, including use of validated tools such as the Beliefs About Medicines Questionnaire (BMQ) and the Beliefs and Behaviour Questionnaire (BBQ) [16, 17], with the BMQ being the most commonly utilised tool. The BMQ is an 18-item scale divided into two parts: BMQ-Specific and BMQ-General. The BMQ-Specific includes necessity and concern subscales, while the BMQ-General includes overuse and harm subscales. Each domain is rated on a five-point Likert scale, with higher scores reflecting stronger beliefs in that domain [16]. However, for this review, beliefs were not restricted to assessment solely through validated tools. Use of other methods to evaluate participants' beliefs may also be suitable for inclusion. As for the outcomes—polypharmacy, potentially inappropriate medicines use, and nonadherence—these have been defined in Box 1. By delineating these outcomes, we aim to provide a comprehensive understanding of the relationship between beliefs and various forms of suboptimal medicine use.
While systematic reviews have explored the impact of beliefs on adherence [18,19,20,21,22,23], few delve into its influence in older adults 65 years and above, resulting in their underrepresentation. Although existing research consistently demonstrates that stronger beliefs in the necessity of medicines with fewer concerns lead to better adherence [12, 15, 21, 23], reviews vary in terms of populations, methodologies, and outcomes assessed. For instance, a 2014 review highlighted the profound influence of beliefs on adherence, however it encompassed participants of all ages and was limited to qualitative studies [22]. Similarly, a 2013 review focused solely on beliefs measured through the BMQ necessity-concern framework and did not restrict participants to those aged 65 or older [21]. Nonetheless, while a more quantitative based review has been adopted, whereby medication adherence was higher where necessity beliefs were stronger, the review similarly was not restricted to older adults and only included participants diagnosed with hypertension [23]. Lastly, a 2006 review investigated the influence of beliefs on medication adherence; however, it solely focused on adherence as the single outcome measure and included adults aged 50 or above [20]. Furthermore, existing reviews fail to explore various other forms of suboptimal medicine use and lack a quantitative approach. This review exclusively incorporates quantitative studies. By identifying these beliefs, healthcare professionals may tailor adherence strategies to align with patients' individual beliefs. This personalized approach may hold the potential to enhance medication adherence and overall health outcomes in older adults.
The extent to which beliefs may influence suboptimal medicines use in older adults warrants further research, as highlighted by the reasons above. We present the first systematic review of quantitative studies which investigated the influence of beliefs on multiple forms of suboptimal medicines use (adherence, polypharmacy and inappropriate use of medicines such as PIMs) in community-dwelling older adults 65 years and above.
Aim
To systematically review and identify quantitative research on the influence of beliefs about medicines and the relationship with suboptimal medicine use in older adults.
Method
Protocol and registration
The PEO (Population, Exposure, Outcome) framework was used in the development of this systematic review and reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA) [24, 25]. The protocol was registered on The International Prospective Register of Systematic Reviews (PROSPERO) (Registration number: CRD42023416431).
Sources and search strategy
A full electronic literature search was conducted on PubMed, EMBASE, CINAHL, and PsycINFO from inception to March 2023. The search strategy was developed in consultation with a research librarian and incorporated combinations of keywords and indexed terms (e.g. MeSH, Emtree subheadings and the APA Thesaurus of Psychological Index Terms) related to beliefs, older adults and suboptimal medicine use. Relevant keywords included: ‘health beliefs’, ‘health views’, ‘health attitude’, ‘medicine beliefs’ and ‘polypharmacy’ utilised in conjunction with Boolean operators (e.g., OR, AND) and truncations. The full detailed search strategy is available in Supplementary material 1. Based on each database, a separate strategy was developed to account for variations in indexed terms. Reference lists of included studies were also searched, and relevant journals were manually inspected.
Eligibility criteria
Original, peer-reviewed research studies were included with the exclusion of grey literature, literature reviews, qualitative studies and studies where full articles could not be obtained. Studies were included if (1) the exposure involved participants’ beliefs including personal beliefs, cultural beliefs, health/medication related beliefs and/or attitudes, (2) the main outcome was one of three forms of suboptimal medicine use; polypharmacy, potentially inappropriate medicine use, or non-adherence, (3) participants were considered older adults 65 years or above, (4) participants were community-dwelling, (5) the study was quantitative and (6) full-text articles were available in English. The outcomes and exposures have been defined as presented in Box 1. Where full-text articles could not be obtained, authors of the study were contacted. If full-text articles still could not be obtained, the study was excluded.
Participants and population
The population of interest was community-dwelling older adults aged 65 years and above, defined, for the purpose of this review, as adults aged 65 years or above living independently in the community. Studies were included if (1) the mean age of recruited participants was 65 years or above or (2) where certain studies included older adults, the data from participants aged 65 years or older could be extracted.
Study selection
Following export of studies to Endnote Version 21, deduplication was completed. Titles and abstracts were independently screened by two reviewers (ER, MA) for eligibility and then full-text screened again by two reviewers (ER, MA). Following review of each full-text paper, reasons for exclusion were noted in an Excel spreadsheet for comparison. Any disagreements were resolved through discussion of each paper. Where both reviewers could not come to an agreement, a third reviewer facilitated consensus.
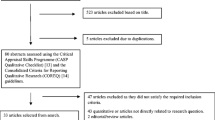
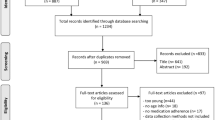
Using the PRISMA guidelines, a flow diagram was generated to illustrate the selection process and the final studies included.
Data extraction and synthesis
Data from papers identified to fit the inclusion criteria were extracted using a standardized data-extraction tool. Data extracted included study design, aim, country, clinical setting, number of participants, measurement of beliefs, participant eligibility criteria, exposure, outcome/s, covariates considered in analysis and the main findings of each study. As such, a narrative synthesis approach was utilised, and a summary of findings table presented. A narrative synthesis has been defined as “an approach to the systematic review and synthesis of findings from multiple studies that relies primarily on the use of words and text to summarise and explain the findings of the synthesis” [26]. Included studies were subsequently analysed and categorised based on their outcome/s; adherence, polypharmacy and/or inappropriate medicine use.
Quality and risk-of-bias assessment
To assess the quality and risk of bias of each study, the Joanna Briggs Institute (JBI) critical appraisal checklist tool was used. This checklist serves as a tool to guide the assessment of the quality and potential inclusion of each study. It includes various appraisal checklists tailored to different types of studies. Hence, depending on the study design being evaluated, a specific checklist from the JBI critical appraisal tool was utilized.
Two reviewers (ER, MA) independently appraised each article, after having set standards for each appraisal standard. Any disagreements among reviewers were resolved through discussion. Where both reviewers could not come to an agreement, a third reviewer would facilitate consensus.
For this systematic review, a high-quality study was defined as a score of ≥ 6 out of 8 for cross-sectional studies and ≥ 8 out of 11 for cohort studies [27].
Results
Study selection
A total of 5,484 entries were identified across four databases (Fig. 1). After eliminating duplicates (n = 360), 5124 articles underwent title and abstract screening. Of these, 94 underwent full-text screening, and 18 studies were included in this systematic review. A hand-search contributed one additional paper, resulting in a total of 19 studies. Of the 19 studies, 15 were cross-sectional [28,29,30,31,32,33,34,35,36,37,38,39,40,41,42] and four were cohort studies [43,44,45,46]. Characteristics of each included study are presented in Table 1 and 2.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of study selection process
Study characteristics
Studies were conducted in The United States (US) (n = 6) [33, 38,39,40, 43, 44], Ireland (n = 3) [28, 32, 45], China (n = 3) [34, 37, 42], Belgium (n = 1) [29], Italy (n = 1)[30], United Kingdom (UK) (n = 1) [46], Netherlands (n = 1) [31], Malaysia (n = 1) [35], Spain (n = 1) [36] and Sweden (n = 1) [41]. Participants were community-dwelling, recruited from a variety of clinical settings including primary care settings, community pharmacies and outpatient clinics.
Participants' beliefs were predominantly assessed using the BMQ (n = 15, 78.9%), either in isolation or in combination with other assessment tools [28,29,30,31,32, 34, 35, 37, 39,40,41, 43,44,45,46]. Of the 19 studies, nine employed the BMQ-Specific in English [29, 31, 32, 37, 40, 43,44,45,46], three utilised both the General and Specific scales of BMQ [28, 39, 41], three employed the Illness Perception Questionnaire–Revised (IPQ-R) [28, 32, 43], two utilised self-made belief questionnaires [33, 36], one used the Brief IPQ [41], one employed the BMQ-Specific in Chinese [34], another in Italian [30], one used the Health Locus of Control Scale with Decisional balance and self-efficacy scales from the Transtheoretical Model [38], and finally, one employed the Aging Perceptions Questionnaire in Chinese [42].
Most studies in the review focused on participants with recognized chronic conditions, but not all had strict criteria. Out of 19 studies, three did not require a formally diagnosed chronic condition [35, 38, 44]. Specific conditions studied included hypertension (n = 2) [32, 43], osteoporosis (n = 2) [42, 46], coronary heart disease (n = 1) [28], type 2 diabetes (n = 1) [31], major depressive disorder (n = 1) [34], and stroke (n = 1) [41].
Among the 18 studies where adherence was the outcome measure, majority of papers (n = 15) recruited participants who were receiving treatment for a chronic health condition [28,29,30,31,32,33,34, 36, 37, 39, 41,42,43, 45, 46].
Quality appraisal
While all studies met the inclusion criteria, their quality varied. Six cross-sectional studies fulfilled all JBI criteria, scoring 8/8 [28, 30, 33, 37, 41, 42], one scored 87.5% (7/8) [29], four scored 75.0% (6/8) [31, 34, 36, 38], and the remaining four were of moderate quality, meeting 62.5% (5/8) of the criteria due to their failure in addressing potential confounding factors, as well as other criteria [32, 35, 39, 40].
Regarding cohort studies, none met all eleven of the JBI Cohort appraisal criteria. Three studies satisfied 45.5% (5/11) of the criteria [43,44,45]. This was due to their failure in identifying confounding factors, lacked strategies to handle such factors, didn't address incomplete follow-up, and certain criteria was deemed "not applicable" to their study. The remaining study fulfilled 27.3% of the criteria (3/11) [46]. Detailed information about the JBI appraisal is outlined in Table 3 and 4. Due to the paucity of papers, no papers were excluded based on their quality.
Outcomes of interest
While the inclusion criteria covered various aspects of suboptimal medicines use (adherence, polypharmacy, PIMs/inappropriate medicine use), most studies in this review focused on adherence as the primary outcome. Of the 19 studies, 18 investigated adherence [28,29,30,31,32,33,34,35,36,37, 39,40,41,42,43,44,45,46], one examined unnecessary medicine use (where patients were using more than one medication receiving an inappropriate rating in terms of indication, effectiveness, or therapeutic duplication) [38], and no studies explored polypharmacy as its primary outcome.
Beliefs and inappropriate medicine use
In a US study, 58.6% of patients were prescribed more than one unnecessary medication, with reasons including ineffectiveness (41.4%), lack of medical indication (39.8%), and therapeutic duplication (8.6%) [38]. Factors including race (white), income, number of prescribed medications, and a lack of belief in a "powerful other" health locus of control were associated with unnecessary medicine use [38]. Interestingly, those with higher unnecessary medicine use were less likely to believe in external factors like physicians influencing their health [38]. While strong health beliefs did not directly lead to unnecessary drug prescribing, the study suggested that patients who have less trust in the healthcare system are more likely to engage in unnecessary medicine use [38]. Overall, patient characteristics and health beliefs were identified as potential contributors to unnecessary medicine use [38].
Beliefs and adherence
Of the 19 studies included in this review, 18 investigated adherence [28,29,30,31,32,33,34,35,36,37, 39,40,41,42,43,44,45,46]. Of these, three studies did not discover any significant associations between patient beliefs and adherence [32, 41, 43]. However, irrespective of the tool used, 15 studies revealed that patient beliefs influenced medication adherence [28,29,30,31, 33,34,35,36,37, 39, 40, 42, 44,45,46]. Among these, 10 studies specified the importance of stronger necessity beliefs in medicine and/or fewer concerns leading to better adherence [28, 29, 33,34,35, 37, 39, 40, 44, 45]. One study highlighted the significant impact of health beliefs on medication adherence, noting distinct variations in these beliefs between adherent and non-adherent individuals [36]. Another revealed an association between beliefs regarding the chronic duration of an illness and decreased adherence [42]. One study presented contradictory findings, indicating that patients with higher necessity beliefs and lower concerns were less inclined to adhere to therapy compared to ambivalent subjects (high necessity and concerns) [30]. Additionally, another study highlighted that low perceived necessity of medicines contributed to non-adherence [46], while a separate study observed no significant differences in necessity beliefs between adherent and non-adherent individuals, however stronger concern beliefs were associated with intentional non-adherence [31].
Using the BMQ, nine studies found stronger beliefs in the necessity of medicine and/or fewer concerns led to better adherence [28, 29, 34, 35, 37, 39, 40, 44, 45]. Likewise, using a 20-item beliefs scale, one study found that perceived medication need and perceived medication affordability were stronger predictors of unintentional non-adherence than medication concerns [33]. While one study did not find significant differences in adherence among four belief groups, self-reported adherence was high and necessity beliefs outweighed concerns for 92.2% of patients [29]. Likewise, one study revealed that adherence was higher when necessity beliefs were high and concern beliefs were low [45]. However, adherence was also higher when both necessity and concern beliefs were high, compared to when both were simultaneously low [45]. Additionally, one study indicated that while both necessity and concern beliefs in medications were significant for intentional non-adherence, only concern beliefs were significant in unintentional non-adherence [44].
Discussion
Statement of key findings
To our knowledge, this is the first systematic review of quantitative studies which assesses beliefs as a contributing factor to multiple forms of suboptimal medicines use such as adherence, potentially inappropriate medicine use (including PIMs), and/or polypharmacy in older adults. Most studies indicated that patient beliefs did indeed influence medication adherence [28,29,30, 33,34,35,36,37, 39, 40, 42, 44,45,46]. In many instances, stronger beliefs in the necessity of medications and/or reduced concerns regarding them were associated with improved adherence. However, one paper presented conflicting results [30], another found no significant differences in necessity beliefs between adherent and non-adherent individuals [31], and others did not find any significant associations between patient beliefs and adherence [32, 41, 43]. Among the studies reviewed, no papers examined the influence of beliefs on polypharmacy, and only one investigated its influence on inappropriate medication use [38]. As such, the influence of beliefs on polypharmacy and the inappropriate use of medicines remains an underexplored area.
Strengths and weaknesses
This systematic review undertook a comprehensive approach by encompassing various outcome measures of suboptimal medication use and did not confine measurement of beliefs to a single validated tool. Qualitative studies were excluded to maintain consistency across findings and to enhance the generalisability of results. To minimise researcher bias, study selection, data extraction and quality assessment were conducted independently by two investigators.
There were certain limitations in this review. Firstly, the review only considered studies written in English, this restricting the pool of available data. Additionally, due to limited existing literature, the review could not draw definitive conclusions regarding the influence of beliefs on polypharmacy or inappropriate medicine use.
Interpretation of findings
Among 18 studies exploring beliefs and adherence, findings suggest that the relationship between medication beliefs and adherence is multifaceted and can vary based on patient populations and other contextual factors. Some US, Swedish, and Irish studies showed no significant association between beliefs and non-adherence [32, 41, 43]. Most studies were conducted on participants who were utilizing medications to manage long-term chronic conditions, this emphasizing the clinical significance of beliefs in managing adherence among patients diagnosed with chronic diseases. However, while most studies emphasized the importance of strong necessity and/or low concern beliefs for higher adherence, there were contradictory studies [30]. Additionally, one study aligned with previous literature, however also found higher adherence when both necessity and concern beliefs were high [45]. Beliefs are an interpersonal factor that can be influenced by individual cultural beliefs and personal experiences.
Due to the complexity of managing multiple chronic conditions and the consequent need for multiple medications, it is argued that polypharmacy in older adults can have a detrimental impact on adherence and increase morbidity [47, 48]. While this assertion holds true, it is important to note that no individual paper was identified to investigate the influence of beliefs on polypharmacy. Therefore, the association between beliefs and polypharmacy remains relatively underexplored.
While PIMs are typically defined as high-risk medicines, as outlined in the Beers or STOPP criteria [49, 50], none of the studies reviewed defined inappropriate medicines as such. One study revealed a significant prevalence (58.6%) of unnecessary medicine use, influenced by factors like the quantity of prescribed medications and patient distrust [38]. Health beliefs were also identified as a potential contributor to unnecessary medicine use [34]. However, despite the known impact of high-risk medications on older adults, the relationship between inappropriate medicine use and patient beliefs remains unclear. Among the 19 studies exploring beliefs, only one investigated their influence on inappropriate medicine use, hence further research is needed.
Current literature, supported by two studies in this review [36, 38], emphasizes the positive impact of a trusting patient–prescriber relationship on medication usage [14]. Research suggests that, (1) receiving medication reviews from doctors may correlate with better adherence [36], and (2) patients who have less trust in their healthcare providers may be more prone to unnecessary medicine use [38]. Therefore, negative experiences and distrust can negatively impact medication-taking behaviour [11]. Considering these findings, coupled with the results of this review, it is evident that patient–prescriber relationships may serve as a critical factor influencing patients' medication beliefs, subsequently affecting their adherence and medication use.
This review places emphasis on the influence of beliefs on adherence, polypharmacy, or inappropriate medicines use, however other influencing factors have been identified. Factors associated with unnecessary medicine use included race (white), income level, and number of prescribed medications [38]. Conversely, factors linked to non-adherence encompassed concerns about side effects, sociodemographic factors, chronic diseases, emotional burden, medication costs, and practical barriers (e.g. dexterity) [30, 33, 39, 40, 42, 46]. Hence, while beliefs may have an impact on suboptimal medicine use, it is crucial to recognise that other barriers may also be contributing to non-adherence.
There were limitations present within the methodology of certain studies. Of the 20 studies, only four did not require participants to have a predefined medical condition, thus narrowing the applicability of findings to specific populations. In addition, where adherence was measured, self-reported questionnaires were employed, potentially introducing bias as participants may overrepresent their adherence.
Further research
There is a need for further research in the understanding of beliefs and its influence on polypharmacy and inappropriate medicines use. More so, additional research is warranted to more comprehensively determine whether necessity or concern beliefs play a pivotal role in adherence. Future studies should explore the benefits in reducing patient concerns and increasing necessity beliefs in improving medication adherence.
Conclusion
Findings suggest that the relationship between medication beliefs and adherence is multifaceted and can vary based on patient populations and other contextual factors. While most studies included in this review supported the finding that stronger beliefs in the necessity of medicines and reduced concerns appear to positively influence adherence in older individuals, further investigation is needed to ascertain the relative importance of necessity or concern beliefs in fostering adherence. Additionally, there is a paucity of research on the influence of beliefs on polypharmacy and inappropriate medicine use, highlighting the need for further research in this area.
References
Barry HE, Hughes CM. An update on medication use in older adults: a narrative review. Curr Epidemiol Rep. 2021;8(3):108–15.
Charlesworth CJ, Smit E, Lee DS, et al. Polypharmacy among adults aged 65 years and older in the United States: 1988–2010. J Gerontol A Biol Sci Med Sci. 2015;70(8):989–95.
Holloway KA. Combating inappropriate use of medicines. Expert Rev Clin Pharmacol. 2011;4(3):335–48.
Espino DV, Bazaldua OV, Palmer RF, et al. Suboptimal medication use and mortality in an older adult community-based cohort: results from the Hispanic EPESE Study. J Gerontol A Biol Sci Med Sci. 2006;61(2):170–5.
Lee GB, Etherton-Beer C, Hosking SM, et al. The patterns and implications of potentially suboptimal medicine regimens among older adults: a narrative review. Ther Adv Drug Saf. 2022;13:20420986221100116.
PSA. Medicine Safety: Take Care Canberra: Pharmaceutical Society of Australia; 2019 [Available from: https://www.psa.org.au/wp-content/uploads/2019/01/PSA-Medicine-Safety-Report.pdf. Accessed 16 Feb 2024.
Wamala S, Merlo J, Bostrom G, et al. Socioeconomic disadvantage and primary non-adherence with medication in Sweden. Int J Qual Health Care. 2007;19(3):134–40.
Andersson Sundell K, Jönsson AK. Beliefs about medicines are strongly associated with medicine-use patterns among the general population. Int J Clin Pract. 2016;70(3):277–85.
Kasahun AE, Sendekie AK, Mekonnen GA, et al. Impact of personal, cultural and religious beliefs on medication adherence among patients with chronic diseases at University Hospital in Northwest Ethiopia. Patient Prefer Adherence. 2022;16:1787–803.
Ibrahim KM, Schommer JC, Morisky DE, et al. The association between medication experiences and beliefs and low medication adherence in patients with chronic disease from two different societies: The USA and the Sultanate of Oman. Pharmacy (Basel). 2021;9(1).
Dolovich L, Nair K, Sellors C, et al. Do patients’ expectations influence their use of medications? Qualitative study. Can Fam Physician. 2008;54(3):384–93.
Park HY, Seo SA, Yoo H, et al. Medication adherence and beliefs about medication in elderly patients living alone with chronic diseases. Patient Prefer Adherence. 2018;12:175–81.
Mohammed MA, Moles RJ, Chen TF. Medication-related burden and patients’ lived experience with medicine: a systematic review and metasynthesis of qualitative studies. BMJ Open. 2016;6(2): e010035.
Martin LR, Williams SL, Haskard KB, et al. The challenge of patient adherence. Ther Clin Risk Manag. 2005;1(3):189–99.
Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–67.
Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24.
George J, Mackinnon A, Kong DCM, et al. Development and validation of the Beliefs and Behaviour Questionnaire (BBQ). Patient Educ Couns. 2006;64(1):50–60.
Shahin W, Kennedy GA, Stupans I. The consequences of general medication beliefs measured by the beliefs about medicine questionnaire on medication adherence: a systematic review. Pharmacy (Basel). 2020;8(3).
Shahin W, Kennedy GA, Stupans I. The impact of personal and cultural beliefs on medication adherence of patients with chronic illnesses: a systematic review. Patient Prefer Adherence. 2019;13:1019–35.
Chia L, Schlenk EA, Dunbar-Jacob J. Effect of personal and cultural beliefs on medication adherence in the elderly. Drugs Aging. 2006;23(3):191–202.
Horne R, Chapman SC, Parham R, et al. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the Necessity-Concerns Framework. PLoS ONE. 2013;8(12): e80633.
Kelly M, McCarthy S, Sahm LJ. Knowledge, attitudes and beliefs of patients and carers regarding medication adherence: a review of qualitative literature. Eur J Clin Pharmacol. 2014;70(12):1423–31.
Al-Noumani H, Wu J-R, Barksdale D, et al. Health beliefs and medication adherence in patients with hypertension: a systematic review of quantitative studies. Patient Educ Couns. 2019;102(6):1045–56.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Munn Z, Stern C, Aromataris E, et al. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Methodol. 2018;18(1):5.
Popay J, Roberts H, Sowden A, et al. Guidance on the conduct of narrative synthesis in systematic reviews: A product from the ESRC Methods Programme (2006).
Wang KN, Bell JS, Chen EYH, et al. Medications and prescribing patterns as factors associated with hospitalizations from long-term care facilities: a systematic review. Drugs Aging. 2018;35(5):423–57.
Byrne M, Walsh J, Murphy AW. Secondary prevention of coronary heart disease: patient beliefs and health-related behaviour. J Psychosom Res. 2005;58(5):403–15.
Capiau A, Mehuys E, Van Tongelen I, et al. Community pharmacy-based study of adherence to non-vitamin K antagonist oral anticoagulants. Heart. 2020;106(22):1740–6.
Cicolini G, Comparcini D, Flacco ME, et al. Self-reported medication adherence and beliefs among elderly in multi-treatment: a cross-sectional study. Appl Nurs Res. 2016;30:131–6.
de Vries ST, Keers JC, Visser R, et al. Medication beliefs, treatment complexity, and non-adherence to different drug classes in patients with type 2 diabetes. J Psychosom Res. 2014;76(2):134–8.
Durand H, Hayes P, Harhen B, et al. Medication adherence for resistant hypertension: assessing theoretical predictors of adherence using direct and indirect adherence measures. Br J Health Psychol. 2018;23(4):949–66.
Gadkari AS, McHorney CA. Unintentional non-adherence to chronic prescription medications: how unintentional is it really? BMC Health Serv Res. 2012;12:98.
Lu Y, Arthur D, Hu L, et al. Beliefs about antidepressant medication and associated adherence among older Chinese patients with major depression: a cross-sectional survey. Int J Ment Health Nurs. 2016;25(1):71–9.
Neoh CF, Long CM, Lim SM, et al. Medication use and adherence among multi-ethnic community-dwelling older adults in Malaysia. Geriatr Gerontol Int. 2017;17(8):1214–20.
Pagès-Puigdemont N, Tuneu L, Masip M, et al. Determinants of medication adherence among chronic patients from an urban area: a cross-sectional study. Eur J Public Health. 2019;29(3):419–24.
Qiao X, Tian X, Liu N, et al. The association between frailty and medication adherence among community-dwelling older adults with chronic diseases: medication beliefs acting as mediators. Patient Educ Couns. 2020;103(12):2548–54.
Rossi MI, Young A, Maher R, et al. Polypharmacy and health beliefs in older outpatients. Am J Geriatr Pharmacother. 2007;5(4):317–23.
Rovner BW, Casten RJ. Health beliefs and medication adherence in black patients with diabetes and mild cognitive impairment. Am J Geriatr Psychiatry. 2018;26(7):812–6.
Sirey JA, Greenfield A, Weinberger MI, et al. Medication beliefs and self-reported adherence among community-dwelling older adults. Clin Ther. 2013;35(2):153–60.
Westberg A, Sjölander M, Glader EL, et al. Primary non-adherence to preventive drugs and associations with beliefs about medicines in stroke survivors. Patient Prefer Adherence. 2022;16:343–52.
Wu X, Wei D, Sun B, et al. Poor medication adherence to bisphosphonates and high self-perception of aging in elderly female patients with osteoporosis. Osteoporos Int. 2016;27(10):3083–90.
Alison Phillips L, Leventhal H, Leventhal EA. Assessing theoretical predictors of long-term medication adherence: patients’ treatment-related beliefs, experiential feedback and habit development. Psychol Health. 2013;28(10):1135–51.
Unni EJ, Farris KB. Unintentional non-adherence and belief in medicines in older adults. Patient Educ Couns. 2011;83(2):265–8.
Foley L, Doherty AS, Wallace E, et al. Exploring the multidimensional relationship between medication beliefs and adherence to medications among older adults living with multimorbidity using polynomial regression: an observational cohort study. Ann Behav Med. 2023;57(7):561–70.
Clark EM, Gould VC, Tobias JH, et al. Natural history, reasons for, and impact of low/non-adherence to medications for osteoporosis in a cohort of community-dwelling older women already established on medication: a 2-year follow-up study. Osteoporos Int. 2016;27(2):579–90.
Rochon PA, Petrovic M, Cherubini A, et al. Polypharmacy, inappropriate prescribing, and deprescribing in older people: through a sex and gender lens. Lancet Healthy Longev. 2021;2(5):e290–300.
Smaje A, Weston-Clark M, Raj R, et al. Factors associated with medication adherence in older patients: a systematic review. Aging Med (Milton). 2018;1(3):254–66.
O’Mahony D, O’Sullivan D, Byrne S, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2015;44(2):213–8.
American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc. 2015;63(11):2227–46.
Hugtenburg JG, Timmers L, Elders PJ, et al. Definitions, variants, and causes of nonadherence with medication: a challenge for tailored interventions. Patient Prefer Adherence. 2013;7:675–82.
Acknowledgements
The authors would like to acknowledge Karen McVean, teaching and research librarian from RMIT University, Melbourne, Australia.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. No specific funding was received.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rafhi, E., Al-Juhaishi, M., Stupans, I. et al. The influence of patients’ beliefs about medicines and the relationship with suboptimal medicine use in community-dwelling older adults: a systematic review of quantitative studies. Int J Clin Pharm (2024). https://doi.org/10.1007/s11096-024-01727-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11096-024-01727-9