
Abstract
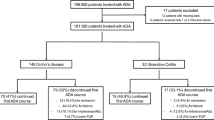
Background Conventional therapy of inflammatory bowel disease with traditional immunosuppressant medication is increasingly being replaced by biological agents. However, the response to these biological agents may be lost over time, with discontinuation being a marker of loss of effectiveness. There are few published reports on the treatment drug survival of infliximab and adalimumab in patients with inflammatory bowel disease. Objective This study compared the drug survival of infliximab versus adalimumab as first- and second-line treatments, identified factors associated with drug survival, and described reasons for treatment withdrawal. Setting A pharmacy department of a university hospital in Spain. Method A retrospective single-centre cohort study of all patients with inflammatory bowel disease treated with biological agents between 2008 and 2017 at a regional referral hospital. The primary outcome was drug survival and associated factors during a follow-up of 52 months. Main outcome measure Drug survival of infliximab versus adalimumab. Results One hundred thirty-four patients with inflammatory bowel disease (73.9% Crohn’s disease and 26.1% ulcerative colitis) were treated with biological therapy. The overall mean drug survival of first-line treatment with an anti-tumour necrosis factor agent was 18.6 months (SD 14.9), with mean values of 20.2 months (SD 16.6) for adalimumab and 17.1 months (SD 13.1) for infliximab. As a second-line treatment, the drug survival of anti-tumour necrosis factor agents was 17.9 months (SD 15.6), with mean values of 22.9 months (SD 17.1) for adalimumab and 12.5 months (SD 11.7) for infliximab. The difference in time to discontinuation at 52 months of follow-up between the infliximab and adalimumab subgroups, as either first- or second-line treatment, was not statistically significant (p = 0.547 and p = 0.676, respectively). Therapeutic drug monitoring was the only factor associated with greater drug survival in first-line treatment (HR 0.27; 95% confidence interval, CI 0.15–0.50) and second-line treatment (HR 0.26; 95% CI 0.10–0.65). Secondary failure to treatment was the most frequent reason for withdrawal. Conclusion Infliximab and adalimumab showed similar drug survival as first- and second-line anti-tumour necrosis factor treatments. Therapeutic drug monitoring was associated with higher drug survival for both first- and second-line anti-tumour necrosis factor treatments.


Similar content being viewed by others


References
Yokoyama K, Yamazaki K, Katafuchi M, Ferchichi S. A retrospective claims database study on drug utilization in Japanese patients with Crohn’s disease treated with adalimumab or infliximab. Adv Ther. 2016;33:1947–63.
Camus M, Seksik P, Bourrier A, Nion-Larmurier I, Sokol H, Baumer P, et al. Long-term outcome of patients with Crohn’s disease who respond to azathioprine. Clin Gastroenterol Hepatol. 2013;11:389–94.
Timmer A, Patton PH, Chande N, Mcdonald JW, Macdonald JK. Azathioprine and 6-mercaptopurine for maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev. 2016;18(5):CD000478.
Quetglas EG, Armuzzi A, Wigge S, Fiorino G, Barnscheid L, Froelich M, et al. Review article: the pharmacokinetics and pharmacodynamics of drugs used in inflammatory bowel disease treatment. Eur J Clin Pharmacol. 2015;71:773–99.
Kotlyar DS, Lewis JD, Beaugerie L, Tierney A, Brensinger CM, Gisbert JP, et al. Risk of lymphoma in patients with inflammatory bowel disease treated with azathioprine and 6-mercaptopurine: a meta-analysis. Clin Gastroenterol Hepatol. 2015;13:847–58.
Khan N, Abbas AM, Lichtenstein GR, Loftus EV, Bazzano LA. Risk of lymphoma in patients with ulcerative colitis treated with thiopurines: a nationwide retrospective cohort study. Gastroenterology. 2013;145:1007–15.
Hanauer SB, Feagan BG, Lichtenstein GR, Mayer LF, Schreiber S, Colombel JF, et al. Maintenance infliximab for Crohn’s disease: the ACCENT I randomised trial. Lancet. 2002;359:1541–9.
Sandborn WJ, Hanauer SB, Rutgeerts P, Fedorak RN, Lukas M, MacIntosh DG, et al. Adalimumab for maintenance treatment of Crohn’s disease: results of the CLASSIC II trial. Gut. 2007;56:1232–9.
Rutgeerts P, Sandborn WJ, Feagan BG, Reinisch W, Olson A, Johanns J, et al. Infliximab for induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2005;353:2462–76.
Sandborn WJ, van Assche G, Reinisch W, Colombel J, D’Haens G, Wolf DC, et al. Adalimumab induces and maintains clinical remission in patients with moderate-to-severe ulcerative colitis. Gastroenterology. 2012;142:257–65.
Doecke JD, Hartnell F, Bampton P, Bell S, Mahy G, Grover Z, et al. Infliximab vs. adalimumab in Crohn’s disease: results from 327 patients in an Australian and New Zealand observational cohort study. Aliment Pharmacol Ther. 2017;45:542–52.
Einarson TR, Bereza BG, Ying Lee X, Lelli F. Dose escalation of biologics in Crohn’s disease: critical review of observational studies. Curr Med Res Opin. 2017;33:1433–49.
Gonczi L, Kurti Z, Rutka M, Vegh Z, Farkas K, Lovasz BD, et al. Drug persistence and need for dose intensification to adalimumab therapy; the importance of therapeutic drug monitoring in inflammatory bowel diseases. BMC GastroenterolBMC Gastroenterol. 2017;17:1–7.
Menter A, Papp KA, Gooderham M, Pariser DM, Augustin M, Kerdel FA, et al. Drug survival of biologic therapy in a large, disease-based registry of patients with psoriasis: results from the psoriasis longitudinal assessment and registry (PSOLAR). J Eur Acad DermatolVenereol. 2016;30:1148–58.
Pouillon L, Baumann C, Rousseau H, Choukour M, Andrianjafy C, Danese S, et al. Treatment persistence of infliximab versus adalimumab in ulcerative colitis: a 16-year single-center experience. Inflamm Bowel Dis. 2019;25:945–54.
Van Der Valk ME, Mangen MJJ, Leenders M, Dijkstra G, Van Bodegraven AA, Fidder HH, et al. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-TNFα therapy: results from the COIN study. Gut. 2014;63:72–9.
Targownik LE, Tennakoon A, Leung S, Lix LM, Nugent Z, Singh H, et al. Factors associated with discontinuation of anti-TNF inhibitors among persons with IBD: a population-based analysis. Inflamm Bowel Dis. 2017;23:409–20.
Olivera P, Thiriet L, Luc A, Baumann C, Danese S, Peyrin-Biroulet L. Treatment persistence for infliximab versus adalimumab in Crohn’s disease: a 14-year single-center experience. Inflamm Bowel Dis. 2017;23:976–85.
Benmassaoud A, Al-Taweel T, Sasson MS, Moza D, Strohl M, Kopylov U, et al. Comparative effectiveness of infliximab versus adalimumab in patients with biologic-Naïve Crohn’s disease. Dig Dis Sci. 2018;63:1302–10.
Cosnes J, Sokol H, Bourrier A, Nion-Larmurier I, Wisniewski A, Landman C, et al. Adalimumab or infliximab as monotherapy, or in combination with an immunomodulator, in the treatment of Crohn’s disease. Aliment Pharmacol Ther. 2016;44:1102–13.
Roblin X, Vérot C, Paul S, Duru G, Williet N, Boschetti G, et al. Is the pharmacokinetic profile of a first anti-TNF predictive of the clinical outcome and pharmacokinetics of a second anti-TNF? Inflamm Bowel Dis. 2018;24:2078–85.
Carbonnel F, Colombel JF, Filippi J, Katsanos KH, Peyrin-Biroulet L, Allez M, et al. Methotrexate Is not superior to placebo for inducing steroid-free remission, but induces steroid-free clinical remission in a larger proportion of patients with ulcerative colitis. Gastroenterology. 2016;150:380–8.
Ungar B, Kopylov U, Engel T, Yavzori M, Fudim E, Picard O, et al. Addition of an immunomodulator can reverse antibody formation and loss of response in patients treated with adalimumab. Aliment Pharmacol Ther. 2017;45:276–82.
Liefferinckx C, Minsart C, Toubeau JF, Cremer A, Amininejad L, Quertinmont E, et al. Infliximab trough levels at induction to predict treatment failure during maintenance. Inflamm Bowel Dis. 2017;23:1371–81.
Mitchell RA, Shuster C, Shahidi N, Galorport C, Demarco ML, Rosenfeld G, et al. The utility of infliximab therapeutic drug monitoring among patients with inflammatory bowel disease and concerns for loss of response: a retrospective analysis of a real-world experience. Can J Gastroenterol Hepatol. 2016;2016:5203898.
Hoseyni H, Xu Y, Zhou H. Therapeutic drug monitoring of biologics for inflammatory bowel disease: an answer to optimized treatment? J Clin Pharmacol. 2018;58:864–76.
Ungar B, Levy I, Yavne Y, Yavzori M, Picard O, Fudim E, et al. Optimizing anti-TNF-α therapy: serum levels of infliximab and adalimumab are associated with mucosal healing in patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol. 2016;14:550–7.
Mitrev N, Vande Casteele N, Seow CH, Andrews JM, Connor SJ, Moore GT, et al. Review article: consensus statements on therapeutic drug monitoring of anti-tumour necrosis factor therapy in inflammatory bowel diseases. Aliment Pharmacol Ther. 2017;46:1037–53.
Frymoyer A, Hoekman DR, Piester TL, De Meij TG, Hummel TZ, Benninga MA, et al. Application of population pharmacokinetic modeling for individualized infliximab dosing strategies in crohn disease. J Pediatr Gastroenterol Nutr. 2017;65:639–45.
Funding
This work was performed as part of the routine work of our organisation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
CIN received speaker fees from Amgen. The other authors have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gil-Candel, M., Gascón-Cánovas, J.J., Urbieta-Sanz, E. et al. Comparison of drug survival between infliximab and adalimumab in inflammatory bowel disease. Int J Clin Pharm 42, 500–507 (2020). https://doi.org/10.1007/s11096-020-00978-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-020-00978-6