
Abstract
A review of patients with brain injury showing personal neglect is presented. The aim is to shed light on this aspect of neglect often unresearched or only indirectly investigated, and to discuss recent findings concerning the methods used to assess personal neglect, its neural correlates and its association with the more often explored aspect of extrapersonal neglect. The review was performed using PubMed and PsychInfo databases to search for papers published in the last 123 years (until January 2018). We reviewed 81 papers describing either single or group studies for a total of 2247 patients. The results of this review showed that various aspects of personal neglect are still controversial and outcomes potentially contradictory. Despite the data reported in the present review suggest that personal neglect is more frequently associated with lesions of the right hemisphere, the left hemisphere may also play an important role. Not surprisingly, personal neglect and extrapersonal neglect seem to co-occur. However double dissociations of these two forms of neglect have been reported, and they seem to dissociate both from a functional and an anatomical perspective. More recent interpretations of personal neglect suggest that it may result from a disrupted body representation. The development of reliable psychometric tools with shared diagnostic criteria is essential to identify different degrees of personal neglect for different body parts and to better refine personal neglect in comparison to extrapersonal neglect and disorders related to distortions of personal domain.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hemispatial neglect is a well-known and relatively common deficit following unilateral brain lesions and it refers to a variety of acquired neuropsychological disorders that affect spatial cognition (see Halligan, Fink, Marshall, & Vallar, 2003; Vallar, 1998 for reviews). The main feature of hemispatial neglect is a general lack of awareness and attention to stimuli located in the contralesional side of space and not due to elementary sensory or motor disorders. Hemispatial neglect can be fractionated into different patterns of impairment according to the specific frame of reference (personal, reaching space and far extrapersonal) that can be selectively affected according to distinct coordinates (Vallar, 1998).
Personal neglect refers to a form of hemi-inattention where brain-injured patients show a “deficit relative to the side of the body contralateral to the lesion” (Guariglia & Antonucci, 1992; p.1001). This definition of ‘personal neglect’ seems to imply a general inattention for the contralesional side of the body. However, different attentional deficits can be related to the contralesional limb. In 1893, Gabriel Anton described the case of a patient who exhibited a deficit of tactile and pain sensation on the left side, as well as proprioceptive impairment of position sense. The loss of both the perception and the “knowledge” of the left side fits with the current definition of personal neglect. However, it is widely accepted in the neuropsychological literature that the first clear observation of personal neglect was made in 1913, by Hermann Zingerle, who referred to Anton’s case. Zingerle described two patients with right brain-injury (cases 2 and 3) both of whom failed to spontaneously attend to the left side of their own body. Referring to case 2, Zingerle noted that the patient “never drew his attention to it [ …] apparently never missed it, and seemed to have completely forgotten about it” (translation as in Benke, Luzzatti, & Vallar, 2004; p. 268). With case 3, Zingerle stated that “the patient did not use his left arm at all for spontaneous movements [ …] it was impossible to obtain comments about his left side or a description of the sensations on that side.” (translation as in Benke et al., 2004; p. 270). Zingerle’s early descriptions seem to reflect different possible deficits associated with neglect in the personal domain: motor and premotor neglect. The term motor neglect (Laplane & Degos, 1983) refers to patients that show a considerable reduction in spontaneous use of their contralesional limbs (as in Zingerle’s case 3), which is not explained by their associated motor impairments (e.g., Punt & Riddoch, 2006; Sampanis & Riddoch, 2013). On the other hand, premotor neglect (Heilman, Bowers, Coslett, Whelan, & Watson, 1985; Bisiach, Vallar, Perani, Papagno, & Berti, 1986b) refers to patients, like Zingerle’s cases 2 and 3, who show a reduced tendency to perform movements with the ipsilesional (unimpaired) limbs toward the contralesional side of their body (Bisiach, Perani, Vallar, & Berti, 1986a) as well as within peripersonal space (Saevarsson, Eger, & Gutierrez-Herrera, 2014).
The relationship between motor and premotor neglect is still unclear and investigation of these two forms of neglect is rarely carried out in the same sample (e.g., Garbarini et al., 2012; Buxbaum et al., 2004). Despite the fact that both motor and premotor neglect within personal space should intuitively fall under the umbrella of ‘personal neglect’, the term personal neglect has often been used to identify the premotor form. As such, we re-direct the reader interested in motor neglect to a review by Punt and Riddoch (2006; see also Sampanis & Riddoch, 2013), as this review will mainly focus on personal neglect defined as a set of spatially asymmetrical symptoms occurring in personal space including: defective awareness of the contralesional side of the body, a lack of awareness of contralesional tactile or proprioceptive stimuli and defective motor programming towards targets in the neglected sector of space (Vallar, 1998). Patients tend to neglect the contralesional side of their body, for example, they may forget to shave the left side of their face or fail to properly dress the left side of their body (e.g. not put the left arm in the left sleeve of a shirt).
The aim of this review is to elucidate different aspects and findings of this specific type of neglect, which is often overlooked or investigated indirectly, by appraising research undertaken since Anton’s first description.
Studies on Personal Neglect: A Systematic Literature Review
The literature on personal neglect is quite fragmented, with inconsistent definitions and assessment methods. This lack of clarity causes difficulties in understanding and defining such an impairment and has implications for both theoretical and clinical or diagnostic purposes. A recent review from Committeri, Piervincenzi and Pizzamiglio (2018) provides a useful re-evaluation of the theoretical accounts and neuro-anatomical correlates of personal neglect, highlighting the association of personal neglect with a variety of body representation disorders. The present review offers a systematic update on relevant research and frames personal neglect in terms of its assessment methods, neural substrates and its relationship with inattention for extrapersonal space.
Method
The review was performed using PubMed and PsychInfo databases to search for papers published before January 2018. Following an initial search with the keywords: personal neglect and stroke; personal neglect and brain damage; personal neglect and lesion; body representation neglect, we identified 62 papers that mentioned personal neglect as part of an empirical study or review paper.
We initially considered English language papers only, though crucial, historical papers in different languages (e.g. Anton, 1893; Zingerle, 1913) were also considered. As part of a second additional search, we scrutinized various papers and reviews on neglect (i.e., Azouvi et al., 2006; List, Brooks, Esterman, & Flevaris, 2008; Rode, Pagliari, Huchon, Rossetti, & Pisella, 2016; Vallar & Ronchi, 2009; Jehkonen, Laihosalo, & Kettunen, 2006) and on associated disorders, such as anosognosia (e.g., Appelros, Karlsson, Seiger, & Nydevik, 2002; Cocchini, Beschin, & Sala, 2002; Buxbaum et al., 2004; Berti, Làdavas, & Della Corte, 1996) to identify further studies about personal neglect, some of which were not published in English. Additionally, for the purpose of the present review, we did not consider forms of neglect which explicitly referred to the clinical description of motor neglect provided by Laplane and Degos (1983) and schematized in the work of Punt and Riddoch (2006).
Results and Discussion
We finally considered a sample of 81 papers (51 reporting single cases and 30 reporting group studies) published in the last 123 years (between 1893 and 2018). The number of patients in the 81 studies ranged from 1 (single case studies) to 282 (group studies). Table 1 reports demographic and clinical information of 51 papers describing 83 single or multiple cases showing personal neglect. Table 2 includes 30 group studies in which personal neglect was assessed as the primary purpose of the studies or as a control variable. The sample size of group studies ranges from eight (Reinhart et al., 2012) to 282 (Guariglia et al., 2014) patients for a total sample size of 2247 patients, of which 755 were reported to have personal neglect (33.6%). Details of these studies are discussed in the sections below considering three aspects that we consider crucial in order to better understand the implications of personal neglect for future research and clinical purposes i) assessment methods, ii) neural correlates of personal neglect and iii) the relationship of personal neglect with extrapersonal neglect.
-
i)
Assessment methods
Tables 1 and 2 report the assessment methods used in each study included in this review, and Table 3 provides a brief description of the most common tests used to assess personal neglect and how extensively they have been used.
Despite a range of diagnostic methods having been developed to assess personal neglect and distortion of personal domain (see Table 3), in the majority (57%; 29/51) of the single case studies reported in Table 1, personal neglect was diagnosed by means of clinical observation. Only 20% (10/51) of the studies used one psychometric test, and as few as 22% (11/51) of the studies used two or three tests to assess personal neglect (seven and four studies respectively). In the group studies (Table 2) personal neglect was assessed more systematically with nearly all studies adopting at least one psychometric test (97%; 29/30). In about a third (30%; 9/30) of the studies personal neglect was investigated by means of two different tests, and only 7% (2/30) of the studies used three different measures to assess personal neglect. This is rather surprising if we consider that other forms of neglect, such as extrapersonal neglect, are usually examined through the use of a wider battery of tests to reflect the complexity of extrapersonal neglect (e.g., Behavioural Inattention Test; Wilson, Cockburn, & Halligan, 1987). Interestingly, when more than one personal neglect assessment method was used, the researchers observed a heterogeneous picture (e.g. Bowen et al., 2005; Azouvi et al., 2006; Glocker et al., 2006; Rousseaux et al., 2013; Caggiano et al., 2014), suggesting that personal neglect may be a term that encompasses disruption of different underlying mechanisms.
A possible reason for the lack of systematic investigations into the literature concerning personal neglect may be due to the fact that personal neglect was not investigated in group studies until 1978 (Cutting, 1978), more than 60 years after its first description. During this period, personal neglect was mainly described in single case studies where the research focused on the clinical evidence for this syndrome (Table 1). One of the first attempts to systematically investigate personal neglect was not until 1986 when Bisiach and colleagues (Bisiach et al., 1986a) devised the One Item Test (Table 3) and reported that 39% of 97 patients showed personal neglect. The One Item test represents a very easy and quick way to assess evidence of personal neglect and has been extensively used for clinical and research purposes in at least 23 studies. This scale has been recently modified to allow evaluation of other body parts such as ear, shoulder, elbow, wrist, waist and knee (Fortis et al., 2010). However, the test also presents some limitations. It usually consists of a single trial assessing a limited area, such as the contralateral arm. More importantly, the command per se (i.e. “With this hand, touch your other hand”) implies the existence of the contralesional limb. This may result in the patient attempting to reach for a limb, otherwise neglected, thus potentially leading to a false negative result. Finally, the search for the contralesional limb is guided by proprioceptive information providing little insight into the patient’s mental representation of their own body (Cocchini et al., 2001).
To respond to some of these limitations, Zoccolotti and Judica (1991) devised the Semistructured Functional Evaluation Scale (SFES), which includes a semi-structured scale assessing difficulties relating to personal space. The ‘Personal sub-scale’ (SFES-P) requires the use of everyday objects, such as a comb, a razor (for males), powder (for women) and glasses, with the examiner assigning a score from 0 (normal performance) to 3 (severe personal neglect). The rating, depending on the examiner’s expertise, provides a general indication of the presence or absence of personal neglect but this rating seems less able to establish different degrees of personal neglect severity, resulting in an underestimation of less severe forms (Beschin & Robertson, 1997).
To improve the objectivity of the assessment of personal neglect, Beschin and Robertson (1997) developed the Comb and Razor/Compact Test where the examiner considers the number of strokes applied by the patient on each side of their own face (when asked to pretend to shave or apply make-up) or on each side of their head (when asked to pretend to comb their hair). Patient’s performance was then compared with normative data and 48% of patients with right-sided brain damage had a pathological performance in the Comb and Razor/Compact Test. Interestingly, in the same study 12 patients showed a double dissociation between extrapersonal neglect and personal neglect. The scoring was later revised by McIntosh and colleagues (McIntosh et al., 2000), who proposed a new formula and cut-off criterion to account for possible biases due to ambiguous response strokes (i.e. responses not clearly assigned on either side).
It must be considered though, that both the Comb and Razor/Compact test and the SFES-P did not extend the investigation to other parts of the body. Such investigation may be crucial as it is widely accepted that personal neglect also refers to lack of exploration of part of the body. To this aim, Cocchini and colleagues (Cocchini et al., 2001) developed the Fluff Test, where blindfolded patients were required to remove 24 circles previously attached on the patient’s clothes in order to cover the contralesional arm, the torso and both legs. Scoring was based on the number of targets removed on each side and the diagnostic cut-off was based on normative group performance. Clinical findings on 38 brain-damaged patients (27 with right and 11 with left unilateral lesions) confirmed a relatively high percentage of personal neglect (44%) following right brain lesion and a lower, though not negligible, percentage (20%) following left-sided brain damage. In Cocchini and colleagues (Cocchini et al., 2001) study the authors also reported six cases of double dissociation between extrapersonal neglect and personal neglect, and a low correlation between these two forms of neglect. These findings seem consistent with previous studies also showing dissociations between the personal and extrapersonal spaces (Guariglia & Antonucci, 1992; Peru & Pinna, 1997; Bisiach et al., 1986a; Beschin & Robertson, 1997; Bailey, Riddoch, & Crome, 2000). However, Glocker and collaborators (Glocker et al., 2006) reported a considerably higher frequency of personal neglect assessed by means of the Vest Test, where patients are asked to search for 24 everyday objects hidden in 24 pockets on a vest, and a modified version of the Fluff test, where targets were attached on a long jacket worn by the patients. In a sample of 25 patients with right-sided brain damage and 25 with left-sided brain damage, up to 80% of the patients with right-sided damage and 48% of those with left-sided damage showed personal neglect on the Vest test, whereas up to 68% of the patients with right-sided damage and 48% of those with left damage showed personal neglect when the modified Fluff test was used. The different findings on frequency may be due to different inclusion criteria used in the studies. However, it should be a matter of careful consideration if relatively small methodological changes, as those between the Vest test and the modified Fluff test, have led to such different diagnostic outcomes in the same sample (e.g. 80% versus 68% of those with right damage). Contradictory results have been observed also in a study by Bowen and collaborators (Bowen et al., 2005) when personal neglect was assessed by means of the Face Washing test, where patients are asked to wipe their face for 20 s with the right hand. In this test, the time spent on the left side of the face is compared with the time spent on the right side. Results of the pilot study did not seem to be in line with other personal neglect tests adopted for the preliminary assessment, such as the One Item Test and the Fluff test. The authors considered the duration of the test as a possible methodological bias. Indeed, 20 s may be an unusually long time to wipe one’s own face and this may have led the patients to clean their face more carefully than they would normally do, spending more time and eventually moving on to the left areas. Unfortunately, the authors only reported data on the total time spent on either the left or right side of the face, not providing information on potential differences between each side of the face during the first few seconds of the task. Focusing on a shorter window of time could have provided valid data about latent personal neglect and a modified version of ths task may represent a further valuable measure to assess personal neglect.
In line with the attempt to maintain some type of ecological validity in assessing personal neglect, methods requiring meta-cognition evaluation, such as the Catherine Bergego Scale (Bergego et al., 1995; Azouvi et al., 2003) have been introduced. The Catherine Bergego Scale is a 10-item questionnaire which takes into account several dimensions of neglect within daily living: personal and motor neglect, extrapersonal, peripersonal and anosognosia. Therapists and patients are asked to rate possible difficulty on a series of situations, such as “Forgets to clean the left side of his or her mouth after eating”. The authors stressed the importance of this particular questionnaire in comparison to conventional tests, which, they argued, fail to consider a patients actual performance in their everyday activities, yet real-life observations may pick up neglect in a way that is missed in “simulated tasks” (Azouvi, 2016).
All the tests described above require actions toward the contralesional body, or an evaluation of these type of actions, but a very different approach to assess possible distortion of personal domain, has been focusing more on the pictorial component of prototypical body representation. At the end of the 1970s, it was proposed that neglect could involve a deficit of internally generated images, namely, the representational hypothesis (Bisiach & Luzzatti, 1978; Bisiach, Luzzatti, & Perani, 1979, Bisiach, Capitani, Luzzatti, & Perani, 1981). Therefore, the impairment may involve a distortion of mental events the occurrence of which is not necessarily linked to the actual stimulation or actions (Bisiach & Luzzatti, 1978). In line with this well-documented approach to neglect, some personal neglect tests (Table 2) have been developed to investigate the mental representation of one’s own body.
These studies raise an interesting question about the extent of personal neglect and its implications for mental representations of one’s own body and represent a valuable source of information for research purposes. However, the relevance of these tasks to diagnose personal neglect is debatable as these methods do not distinguish possible confounding variables related to forms of neglect in other domains (e.g. peripersonal space and arm-reaching space). In this vein, some tests have been developed to investigate body representation and been used as diagnostic tools (Table 3). For example, the Draw-A-Man test (Goodenough, 1926) represents one of the most controversial methods as it has been often used for neuropsychological evaluation in patients with brain-damaged (Andrews, Brocklehurst, Richards, & Laycock, 1980; Cohn, 1953; Colombo, De Renzi, & Faglioni, 1976; Gasparrini, Shealy, & Walters, 1980; Reznikoff & Tomblen, 1956; Riklan, Zahn, & Diller, 1962; Schulman, Kaspar, & Throne, 1965; Ska & Nespoulous, 1987). However, the Draw-A-Man test only recently has been considered as a diagnostic method for personal neglect. Chen-Sea (2000) proposed to validate this test by assessing the presence of personal neglect in right-sided brain damage patients. Patients were asked to draw a human figure on a blank piece of paper and any asymmetry, independently evaluated by two raters, was considered evidence of personal neglect. The results of the study showed the presence of personal neglect in 13 patients out of 51 (25.5%). However, it should be highlighted that the possible bias due to associated representational neglect and extrapersonal neglect remains unclear, and it is difficult to exclude any role of these latter forms of neglect on the test findings. In addition to this, results of the Draw-A-Man test have not been compared with other tests for personal neglect, leaving its specificity unclear. Another interesting assessment tool for personal neglect is the Body Representation test (Daurat-Hmeljiak et al., 1978), which consists of four subtests requiring the patient to name, localize and reconstruct specific body parts. In order to find the correct position of a specific body part, patients with personal neglect cannot consider the relations among body parts separately from their own body (allocentric frame of reference), but they have to use an egocentric reference (their own body). Therefore, Palermo et al. (2014) claimed that this test necessitates the use of an egocentric frame of reference in processing the topological body map. This test has been used in several studies with brain-damaged patients (Canzano, Piccardi, Bureca, & Guariglia, 2011; Guariglia & Antonucci, 1992; Marangolo et al., 2003; Palermo et al., 2014) but validation for clinical assessment of this test has not been undertaken as yet.
Similarly, the Subjective Straight Ahead test evaluates the egocentric frame of reference (Heilman, Bowers, & Watson, 1983; Karnath, Sievering, & Fetter, 1994; Richard, Honoré, & Rousseaux, 2000; Richard, Rousseaux, Saj, & Honoré, 2004; Rousseaux et al., 2015). In this task, patients with neglect tend to show a bias towards the right when asked to point ‘straight ahead’ of their body midline. This bias seems to be closely linked to an alteration of the internal representation of the midsagittal plane of the body, which is the egocentric frame of reference. Richard et al. (2004) devised a test to obtain a direct indication of the Subjective Straight Ahead test, in which participants were asked to adjust the position of a luminous rod straight ahead of the middle part of their trunk in a dark room. Results showed a translation of the egocentric frame of reference towards the right. In a study conducted by Rousseaux et al. (2015), the same Subjective Straight Ahead test procedure developed by Richard and colleagues was used to assess personal neglect together with the One Item Test (Bisiach et al., 1986a). In a sample of 45 patients with right-sided brain damage, the authors reported eight patients as having personal neglect (18%) based on their impaired performance in the One Item Test and that up to 27 (60%) of these patients showed a pathological rightward deviation in the Subjective Straight Ahead test. It must be considered that the tasks assessing distortion of body representation and egocentric reference frames inevitably require a crucial involvement of information arising from extrapersonal space and they tend to address different aspects than premotor personal neglect. Overall, these measures therefore provide valuable research information about some aspects of personal space, but their specificity in assessing personal neglect remains to be clarified.
-
ii)
Neural correlates of Personal Neglect
As discussed above, without a robust diagnostic method for personal neglect, it is difficult to evaluate the neural correlates of personal neglect as, in some studies, its diagnosis is not well defined, leaving unresolved doubts of false negatives or false positives. A further reason for caution is the fact that several studies report limited information on the patient lesions, or the neuroimaging investigation performed is represented by a routine radiological exam. Keeping in mind these limitations, we have reviewed the literature to consider convergence of outcomes and replication of findings.
Considering Table 1, the vast majority of the single and multiple cases (74/83; 89%) suffered from unilateral right-sided brain damage, whereas only 11% of the sample showed personal neglect associated with bilateral (four cases) or unilateral left-sided brain damage (five cases). Similarly, in Tables 2, 72% (1624/2247 patients) of the patients in the 30 group studies reported personal neglect following right-sided brain damage, whereas only 20% (457/2247) following left-sided damage. Therefore, while there is a clear predominance of personal neglect following right-sided brain damage, about one-fifth of patients showed evidence of this form of neglect after left-sided lesions. Traditionally, personal neglect is investigated following right-sided brain damage and assessed following left-sided injury only if the authors have specific research questions or, when it is evident on general assessment (i.e. severe). On the basis of such consideration, we suspect that personal neglect after left-sided brain injury may be more frequent than reported.
To further explore the hemispheric asymmetry of personal neglect, we considered five studies reported in Table 2 where personal neglect was investigated by means of the same method both in patients with left-sided or right-sided brain damage (Cocchini et al., 2001; Appelros et al., 2002; Azouvi et al., 2006; Glocker et al., 2006; Caggiano et al., 2014). These five studies investigated personal neglect in a total sample of 841 patients, of which 485 had right unilateral lesions and 356 had left unilateral lesions. When different tests were used to assess personal neglect in the same sample, resulting in slightly different frequencies of personal neglect, we considered the highest value reported from each sample. Evidence of personal neglect was found in 119 out of 485 patients with right-sided brain damage (24.5%) and 49 out of 356 (14%) patients with left-sided lesions. Personal neglect after right hemisphere lesions was significantly more frequent than after left hemisphere lesions (χ2 = 13.17; p <. 001). However, the frequency of personal neglect in these samples should be interpreted with caution as they are not epidemiological studies, therefore inclusion criteria for right-sided damage vesus left-sided damage may differ. Unintended sampling bias could account, at least in part, for the higher frequency of personal neglect in one group. Interestingly, though personal neglect seems to be more often associated to right-sided brain damage, the presence of personal neglect is highly variable ranging from 2.7% (Appelros et al., 2002) to 48% (Glocker et al., 2006). A recent study by Kesayan and collaborators (Kesayan, Lamb, Williamson, Falchook, & Heilman, 2016) investigated personal pseudoneglect in 24 healthy participants who showed the typical leftward deviation on allocentric neglect tasks, such as line bisection. However, when they were asked to perform egocentric neglect tasks, such as evaluating the strength of tactile stimuli and the arm bisection test, the participants showed a rightward deviation. The authors concluded that the right hemisphere is crucial for modulating allocentric attention, whereas the left hemisphere may be more involved in tasks requiring egocentric attention and attention directed to personal space (Kesayan et al., 2016).
Information about site of lesions within the hemispheres is even less conclusive and it is complicated by the lack of clear information about the lesion site in some studies, as well as the association of other deficits, in particular extrapersonal neglect, making it difficult to understand the selective impact of a lesion on personal neglect. An analysis of single cases, which tend to provide more detailed descriptions, was also rather inconclusive. Considering the single case studies reported in Table 1, the lesion site information was not available for 10 cases (Zingerle, 1913; Kramer, 1915; Barré et al., 1923; Barkman, 1925; Ehrenwald, 1930; Ehrenwald, 1931; Von Hagen & Ives, 1937; Gerstmann, 1942). Three further studies provide limited lesion site information (Paulig et al., 2000; Di Vita et al., 2016; Ronchi et al., 2017) and in one study localization of the brain lesion was deduced through clinical diagnosis (Wortis & Dattner, 1942). Based on the information reported in the other 65 cases, personal neglect seems frequently associated with a widespread range of cortical and subcortical lesion sites, including the thalamus, basal ganglia and internal capsule.
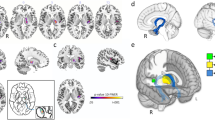
A similar picture appears when we considered group studies reported in Table 2. Lesion site information is not available in 12 studies (Cutting, 1978; Zoccolotti & Judica, 1991, Beschin & Robertson, 1997; McIntosh et al., 2000; Cocchini et al., 2001; Appelros et al., 2002, 2004; Azouvi et al., 2003; Bartolomeo, Sylvie Chokron, & Gainotti, 2001; Bowen et al., 2005; Glocker et al., 2006; Spaccavento et al., 2017) and various papers reported widespread lesions across the four lobes and subcortical structures, including the thalamus, basal ganglia, insula and white matter fibers. However, a few recent group studies start to shed light on the identification of different neural correlates between personal and extrapersonal neglect. Baas et al. (2011), using subtractive analysis to highlight the affected areas in patients with personal neglect, observed that the temporo-parietal junction and the underlying white matter were most affected (about 50% more often) in patients with personal neglect compared to patients without personal neglect. One of the first systematic studies on neural correlates of personal neglect in humans was conducted by Committeri and colleagues (Committeri et al., 2007). The authors observed a significant dissociation between the neural substrates underlying personal versus extrapersonal neglect. In particular, the authors reported that while lesions involving frontal circuits such as the right central premotor cortex, medial frontal gyrus and superior temporal regions are related to extrapersonal neglect, the critical regions related to personal neglect seem to be the postcentral and supramarginal gyri of the parietal lobe and white matter that underlies the two regions. Interestingly, damage to the right inferior posterior-parietal region (supramarginal gyrus), and underlying white matter, has been considered a pathological correlate of asomatognosia (Feinberg, Roane, & Ali, 2000; Feinberg, DeLuca, Giacino, Roane, & Solms, 2005).
The supramarginal gyrus has a considerable hemispheric specialization, the left side is associated with linguistic information processing, while right side is more related to spatial information processing (Kandel, Schwarts, Jessel, Siegelbaum, & Hudspeth, 2012). In detail, the main afferent signals to the supramarginal gyrus come from the somatosensory cortex (post-central gyrus) concerning the positions of the limbs. In addition, it receives information from the vestibular system and the premotor areas about head orientation in space. The supramarginal gyrus sends information to both the associative somatosensory cortex, involved with visual information processing concerning the spatial location, and to the premotor areas, involved in spatial orientation and movement planning. The postcentral gyrus, receives sensory and proprioceptive information from the body surface and tension state of joints. In addition to this, efferent fibers projecting to the primary motor cortex allow the motor system to integrate information about the intention of movement with proprioceptive information. As originally proposed by Committeri and colleagues (Committeri et al., 2007), these observations support the hypothesis that personal neglect is due to a functional disconnection between regions important for coding proprioceptive and somatosensory input, such as the postcentral gyrus, and those which encode more abstract egocentric representation of the body in space, such as the supramarginal gyrus (Coslett, 1998; Galati, Committeri, Sanes, & Pizzamiglio, 2001; Committeri et al., 2018). This type of injury could cause an impairment in creating a mental model of body image, awareness of the configuration and motion of body in space (Galati et al., 2001).
Similar anatomical substrates, with no apparent involvement of the supramarginal gyrus, have been recently reported in a study conducted by Rousseaux et al. (2015). In a sample of 45 neglect patients, Rousseaux and colleagues observed a dissociation between the neural correlates underlying personal neglect and peripersonal neglect. In particular, personal neglect was associated mainly with lesions in somatosensory cortex and motor cortex and, to a lesser degree, in superior temporal gyrus, middle temporal gyrus, intraparietal sulcus and inferior parietal gyrus. On the other hand, peripersonal neglect was associated with much larger lesions involving the superior temporal gyrus and inferior parietal gyrus with extension to the middle temporal gyrus, temporo-occipital junction, somatosensory and motor cortices.
Despite some methodological limitations concerning the assessment of personal neglect (see Assessment methods, above), these data stress the relevance of parietal lesions in personal neglect and partially support the hypothesis that body centered tasks, which require conscious awareness of body representation and an egocentric coding of spatial information, are affected by lesions involving the anterior parietal lobe, superior temporal lobe and the underlying white matter (Galati et al., 2001).
-
iii)
Personal and extrapersonal neglect
Unilateral neglect may affect both personal and extrapersonal spaces and they have often been associated (e.g. Bisiach et al., 1986a; Cocchini et al., 2001; Committeri et al., 2007; Guariglia et al., 2014; Iosa et al., 2016). Unsurprisingly, information provided in Table 1 seems to confirm that personal and extrapersonal neglect frequently co-occur. Indeed, these two forms of neglect were both assessed in 74 cases (Table 1), and up to 63 patients (85%; 63/74) showed personal neglect associated with extrapersonal neglect. Despite this, evidence of selective personal neglect was not infrequent (Bisiach et al., 1986a; Buxbaum et al., 2004). We identified evidence of selective personal neglect in 11 single cases (Table 1; Garcin et al., 1938; Zoccolotti & Judica, 1991; Guariglia & Antonucci, 1992; Beschin et al., 1997; Peru & Pinna, 1997; Marangolo et al., 2003; Ortigue et al., 2006; and four patients in Di Vita et al., 2016) and 10 group studies (see Table 2; Bisiach et al., 1986a; Beschin & Robertson, 1997; McIntosh et al., 2000; Cocchini et al., 2001; Buxbaum et al., 2004; Bowen et al., 2005; Committeri et al., 2007; Guariglia et al., 2014; Rousseaux et al., 2015; Spaccavento et al., 2017). We fully agree with Guariglia and Antonucci (1992) who suggested that the number of patients showing a pure form of personal neglect may be underestimated due to methodological issues, as there is a lack of measures for evaluating impaired processes related to the contralesional body space and, as discussed in the Assessment of personal neglect section, above, the evaluation of personal neglect is still associated with some important limitations. Moreover, there is a small, but growing, body of evidence reporting a pattern of double dissociation between personal versus extrapersonal neglect (mainly peripersonal: Patterson & Zangwill, 1944; Rizzolatti, Matelli, & Pavesi, 1983; Bisiach, Perani, et al., 1986; Zoccolotti & Judica, 1991; Guariglia & Antonucci, 1992; Pizzamiglio et al., 1989; Vallar, Sterzi, Bottini, Cappa, & Rusconi, 1990; Beschin & Robertson, 1997; Cocchini et al., 2001; McIntosh et al., 2000; Bowen et al., 2005; Committeri et al., 2007; Spaccavento et al., 2017). Pizzamiglio and colleagues (Pizzamiglio, Guariglia, Antonucci, & Zoccolotti, 2006) reviewed the effect of rehabilitation methods, such as transcutaneous electrical nervous stimulation and optokinetic stimulation, on different aspects of neglect syndrome. The authors concluded that some of these techniques might lead to a significant recovery of spatial exploration for the extrapersonal space but have little, if any, impact on representational neglect and personal neglect. This research suggests that different underlying mechanisms may underpin these forms of neglect. More recently, Iosa et al. (2016) investigated the recovery of personal and extrapersonal neglect in 49 patients with right-sided brain damage following a combination of physiotherapy and a 6-week neuropsychological rehabilitation training, which involved visual scanning, reading, copying verbal and non-verbal material and verbal description of scenes. On average the extrapersonal neglect improvement was almost 80%, whereas personal neglect recovery was about 58% in patients who initially showed mild personal neglect and up to 72% in those who initially showed severe personal neglect. However, the authors found no correlation between personal and extrapersonal neglect improvement, supporting once more the hypothesis for different mechanisms, at least for recovery.
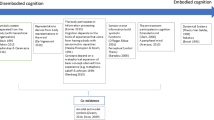
Therefore, the frequent association of personal with extrapersonal neglect seems to indicate a shared attentional deficit which can involve different sectors of the space (Vallar & Bolognini, 2014). However, there is also growing evidence suggesting that, in addition to the inattentional component, personal neglect might also subtend a disorder of multisensory body representation. Coslett, Saffran, and Schwoebel (2002) suggested that personal neglect patients might show a disorder of body representation mainly due to impaired sensorimotor information, that is, impaired perception of body schema. This consideration was based on a previous study where patients were asked to decide whether displayed images of hands (on dorsal and palmar view) were left or right hands (Coslett, 1989). This type of task required participants to form a mental representation of this part of the body in order to make a correct judgment (Parsons, 1987a; b). This result does not seem to be attributed to a loss of information about the representation of the left side of the body but to an impairment in representing the correct relations amongst different parts of the body (Rousseaux et al., 2013). Interestingly, passive limb activation in personal neglect patients, but no general alertness cueing, reduced judgment error rates in discriminating left hand stimuli, suggesting that “bottom-up” interventions in brain-damaged patients displaying personal neglect, modulates the activation of the body schema and can promote a better body representation (Reinhart et al., 2012).
Guariglia and Antonucci (1992) described a patient showing a profound distortion of the left side of his body representation in absence of extrapersonal neglect. The authors argued that personal neglect might be linked to an alteration of bodily spatial relations and other authors (Baas et al., 2011) supported this interpretation, further claiming that body representation is a fundamental mechanism in personal neglect, which could be interpreted as a disorder of the ‘body schema’ and implying that this construct involves mechanisms that go beyond the mere higher order somatosensory representation (Coslett et al., 2002).
Conclusions
Personal neglect represents an important aspect of everyday life (e.g., dressing, washing, eating, and personal care) and can be detrimental to functional rehabilitation (Iosa et al., 2016). However, in the last 123 years, the personal neglect has been relatively ‘neglected’ in research and clinical practice. The number of studies that have systematically investigated this syndrome is vastly smaller compared to those investigating the extrapersonal neglect. The variety of diagnostic measures to assess personal neglect is also limited, with only 7% of the group studies adopting more than two assessment tools. Although some recent studies have adopted a more comprehensive approach, the need for novel and sensitive diagnostic tools to assess various aspects of personal neglect has been emphasized by various authors and echoed in this review. A greater attention to the assessment issue seems to represent the first and crucial step to refine methodological aspects of research on personal neglect. Different aspects of extrapersonal space have been extensively studied and examined by means of standardised test batteries, which have been widely used for decades for research and diagnostic purposes. On the contrary, the lack of uniformity in the assessment methods concerning personal neglect has led to unclear definitions of such impairment, undermining its relevance for clinical and research purposes. A robust assessment method, with batteries of tests evaluating different aspects and body areas will enhance our ability to diagnose different degrees of personal neglect and consequently, it will lead to a better definition of related neuronal substrates and networks. As suggested by Committeri and colleagues (Committeri et al. 2018), the use of the One Item Test (Bisiach et al., 1986a, b) and the SSES-P (Zoccolotti & Judica, 1991) or the Comb and Razor/Compact test (Beschin & Robertson, 1997; McIntosh et al., 2000) should be part of the standard assessment of personal neglect. However, as highlighted in the present review, personal neglect refers to lack of exploration of part of the body. Therefore, we believe that the Fluff test (Cocchini et al., 2001) should not be just desirable (Committeri et al., 2018) but an integral part of the routine assessment, in order to have a triad of tests that target the different body areas providing a more exact clinical picture of personal neglect.
This review also shows that, despite a frequent co-occurrence of personal and extrapersonal neglect, a few cases show a selective form of personal neglect suggesting that these two forms of neglect can be dissociated. Also, the neural bases of personal and extrapersonal space awareness seem to support the hypothesis that these two forms of neglect may, at some point, underlie different neuroanatomical structures and processes. Similarly, based on the body representation literature, it seems that personal neglect may not differ from extrapersonal neglect only because it represents an attentional deficit involving a specific space frame (i.e. the body). On the contrary, the impairment associated with personal neglect may go beyond an attentional deficit and be part of a more complex deficit of body representation (Committeri et al., 2018). The impairment of personal space processing is indeed associated with a perturbation of the mental representation of the patient’s body. In fact, personal space awareness requires the integration of many sources of proprioceptive and somatosensory information pertaining to the body as well as abstract egocentric representations necessary to perceive and to move the body in space (Committeri et al., 2007). Impairments in use of this complex array of information may lead to a significant reduction of awareness for possible impairment related to the neglected side of the body.
In more dramatic cases, the loss of awareness of one body-half can be associated with profoundly disturbed feelings of ownership of contralesional limbs (Dieguez, Staub, & Bogousslavsky, 2007; Pinel, 2009). Patients do not recognise that some parts of their (usually left) body belong to them, as they show asomatognosia (Jenkinson, Moro, & Fotopoulou, in press; Arzy, Overney, Landis, & Blanke, 2006). The relationship between personal neglect and asomatognosia is still controversial, as some studies have described a defective sense of ownership in the absence of a disturbance in body awareness (Hécaen, Ajuriaguerra, Guillant, & Angelergues, 1954; Bisiach, Rusconi, & Vallar, 1991; Halligan, Marshall, & Wade, 1993; Bisiach et al., 1990).
A better understanding of personal neglect will also shed light on syndromes often associated, and sometimes confused, with personal neglect, such as asomatognosia, anosognosia and other syndromes showing disturbances of personal identity.
References
Aglioti, S. M., Smania, N., Manfredi, M., & Berlucchi, G. (1996). Disownership of left hand and objects related to it in a patient with right brain damage. Neuroreport, 8(1), 293–296.
Andrews, K., Brocklehurst, J. C., Richards, B., & Laycock, P. J. (1980). The prognostic value of picture drawings by stroke patients. Rheumatology and Rehabilitation, 19(3), 180–188.
Anton, G. (1893). Beiträge zur klinischen Beurtheilung und zur Localisation der Muskelsinnstörungen im Grosshirne. Z Heilk, 14, 313–348.
Appelros, P., Karlsson, G. M., Seiger, A., & Nydevik, I. (2002). Neglect and anosognosia after first-ever stroke: Incidence and relationship to disability. Journal of Rehabilitation Medicine, 34(5), 215–220.
Appelros, P., Nydevik, I., Karlsson, G. M., Thorwalls, A., &Seiger, Å. (2004). Recovery from unilateral neglect after right-hemisphere stroke. Disability and Rehabilitation, 26(8), 471–477.
Arzy, S., Overney, L. S., Landis, T., & Blanke, O. (2006). Neural mechanism of embodiment: Asomatognosia due to premotor cortex damage. Archives of Neurology, 63(7), 1022–1025.
Assal, G. (1983). Non, je ne suis pas paralysée, c’est la main de mon mari. Schweizer Archiv für Neurologie, Neurochirurgie und Psychiatrie, 133, 151–157.
Azouvi, P. (2016). The ecological assessment of unilateral neglect. Annals of Physical and Rehabilitation Medicine, 60(3), 186–190.
Azouvi, P., Bartolomeo, P., Beis, J. M., Perennou, D., Pradat-Diehl, P., & Rousseaux, M. (2006). A battery of tests for the quantitative assessment of unilateral neglect. Restorative Neurology and Neuroscience, 24(4–6), 273–285.
Azouvi, P., Olivier, S., de Montety, G., Samuel, C., Louis-Dreyfus, A., & Tesio, L. (2003). Behavioral assessment of unilateral neglect: Study of the psychometric properties of the Catherine Bergego scale. Archives of Physical Medicine and Rehabilitation, 84(1), 51–57.
Azouvi, P., Samuel, C., Louis-Dreyfus, A., Bernati, T., Bartolomeo, P., Beis, J. M., … Rousseaux, M. (2002). French collaborative study group on assessment of unilateral neglect (GEREN/GRECO). Sensitivity of clinical and behavioural tests of spatial neglect after right hemisphere stroke. Journal of Neurology, Neurosurgery, and Psychiatry, 73(2), 160–166.
Baas, U., Haan, B., Grässli, T., Karnath, H. O., Mueri, R., Perrig, W. J., … Gutbrod, K. (2011). Personal neglect-a disorder of body representation? Neuropsychologia, 49(5), 898–905.
Bailey, M. J., Riddoch, M. J., & Crome, P. (2000). Evaluation of a test battery for hemineglect in elderly stroke patients for use by therapists in clinical practice. Neurorehabilitation, 14(3), 139–150.
Barkman, A. (1925). De l’anosognosie dans l’hémiplégie cérébrale: contribution clinique a l’étude de ce symptôme. Acta Medica Scandinavica, 52, 235–254.
Barré, J. A., Morin, L., & Kaiser, A. (1923). Etude clinique d’un nouveau cas d’anosognosie. Revue Neurologique, 39, 500–503.
Bartolomeo, P., Sylvie Chokron, S., & Gainotti, G. (2001). Laterally directed arm movements and right unilateral neglect after left hemisphere damage. Neuropsychologia, 39(19), 1013–1021.
Beis, J.-M., Keller, C., Morin, N., Bartolomeo, P., Bernati, T., Chokron, S., & Azouvi, P. (2004). Right spatial neglect after left hemisphere stroke. Qualitative and quantitative study. Neurology, 63(9), 1600–1605.
Benke, T., Luzzatti, C., & Vallar, G. (2004). Hermann Zingerle's "Impaired perception of the own body due to organic brain disorders". 1913. An introductory comment, and an abridged translation. Cortex, 40(2), 265–274.
Bergego, C., Azouvi, P., Samuel, C., Marchal, F., Louis-Dreyfus, A., Jokic, C., … , Renard G. (1995). Validation d’une échelle d’évaluation fonctionnelle de l’héminégligence dans la vie quotidienne: l’échelle CB. Annales de Readaptation et de Medecine Physique, 38, 183–189.
Berthier, M., & Starkstein, S. (1987). Acute atypical psychosis following a right hemisphere stroke. Acta Neurologica Belgica, 87(3), 125–131.
Berti, A., Làdavas, E., & Della Corte, M. (1996). Anosognosia for hemiplegia, neglect dyslexia, and drawing neglect: Clinical findings and theoretical considerations. Journal of the International Neuropsychological Society, 2(5), 426–440.
Beschin, N., Basso, A., & Della Sala, S. (2000). Perceiving left and imagining right: Dissociation in neglect. Cortex, 36(3), 401–414.
Beschin, N., Cocchini, G., Della Sala, S., & Logie, R. H. (1997). What the eyes perceive, the brain ignores: A case of pure unilateral representational neglect. Cortex, 33(1), 3–26.
Beschin, N., & Robertson, I. H. (1997). Personal versus extrapersonal neglect: A group study of their dissociation using a reliable clinical test. Cortex, 33(2), 379–384.
Besharati, S., Forkel, S. J., Kopelman, M., Solms, M., Jenkinson, P. M., & Fotopoulou, A. (2016). Mentalizing the body: Spatial and social cognition in anosognosia for hemiplegia. Brain, 139, 971–985.
Bisiach, E., Capitani, E., Luzzatti, C., & Perani, D. (1981). Brain and conscious representation of outside reality. Neuropsychologia, 19(4), 543–551.
Bisiach, E., & Luzzatti, C. (1978). Unilateral neglect of representational space. Cortex, 14(1), 129–133.
Bisiach, E., Luzzatti, C., & Perani, D. (1979). Unilateral neglect, representational schema and consciousness. Brain, 102(3), 609–618.
Bisiach, E., Meregalli, S., & Berti, A. (1990). Mechanisms of production control and belief fixation in human visuospatial processing: Clinical evidence from hemispatial neglect and misrepresentation. In M. L. Commons, R. J. Herrnstein, S. M. Kosslyn, & D. B. Mumford (Eds.), Quantitative analysis of behavior. Computational and clinical approaches to pattern recognition and concept formation (Vol. IX, pp. 2–21). Hillsdale, New Jersey: Lawrence Erlbaum Associates, Inc.
Bisiach, E., Perani, D., Vallar, G., & Berti, A. (1986a). Unilateral neglect: Personal and extra-personal. Neuropsychologia, 24(6), 759–767.
Bisiach, E., Rusconi, M. L., & Vallar, G. (1991). Remission of somatoparaphrenic delusion through vestibular stimulation. Neuropsychologia, 29(10), 1029–1031.
Bisiach, E., Vallar, G., Perani, D., Papagno, C., & Berti, A. (1986b). Unawareness of disease following lesions of the right hemisphere: Anosognosia for hemiplegia and anosognosia for hemianopia. Neuropsychologia, 24(4), 471–482.
Bottini, G., Bisiach, E., Sterzi, R., & Vallar, G. (2002). Feeling touches in someone else’s hand. Neuroreport, 13(2), 249–252.
Bowen, A., Gardener, E., Cross, S., Tyrrell, P., & Graham, J. (2005). Developing functional outcome measures for unilateral neglect: A pilot study. Neuropsychological Rehabilitation, 15(2), 97–113.
Buxbaum, L., Ferraro, M. K., Veramonti, T., Farne, A., Whyte, J., Ladavas, E., ... Coslett, H. B. (2004). Hemineglect: subtypes, neuroanatomy and disability. Neurology, 62(5), 749–756.
Caggiano, P., Beschin, N., & Cocchini, G. (2014). Personal neglect following unilateral right and left brain damage. Procedia-Social and Behavioral Sciences Journal, 140, 164–167.
Canzano, L., Piccardi, L., Bureca, I., & Guariglia, C. (2011). Mirror writing resulting from an egocentric representation disorder: A case report. Neurocase, 17(5), 447–460.
Chen-Sea, M. J. (2000). Validating the draw-A-man test as a personal neglect test. American Journal of Occupational Therapy, 54(4), 391–397.
Cocchini, G., Beschin, N., & Jehkonen, M. (2001). The fluff test: A simple task to assess body representation neglect. Neuropsychological Rehabilitation, 11(1), 17–31.
Cocchini, G., Beschin, N., & Sala, S. D. (2002). Chronic anosognosia: A case report and theoretical account. Neuropsychologia, 40(12), 2030–2038.
Cohn, R. (1953). Role of “body image concept” in pattern of ipsilateral clinical extinction. Archives of Neurology and Psychiatry, 70(4), 503–509.
Colombo, A., De Renzi, E., & Faglioni, P. (1976). The occurrence of visual neglect in patients with unilateral cerebral disease. Cortex, 12(3), 221–231.
Committeri, G., Pitzalis, S., Galati, G., Patria, F., Pelle, G., Sabatini, U., & Pizzamiglio, L. (2007). Neural bases of personal and extrapersonal neglect in humans. Brain, 130(2), 431–441.
Committeri, G., Piervincenzi, C., & Pizzamiglio, L. (2018). Personal neglect: A comprehensive theoretical and anatomo–clinical review. Neuropsychology, 32(3), 269–279.
Coslett, H. B. (1989). The role of the body image in neglect. Journal of Clinical and Experimental Neuropsychology, 11, 79.
Coslett, H. B. (1998). Evidence for a disturbance of the body schema in neglect. Brain and Cognition, 37(3), 527–544.
Coslett, H. B., Saffran, E. M., & Schwoebel, J. (2002). Knowledge of the human body: A distinct semantic domain. Neurology, 59(3), 357–363.
Cutting, J. (1978). Study of anosognosia. Journal of Neurology, Neurosurgery, and Psychiatry, 41(6), 548–555.
Daurat-Hmeljiak, C., Stambak, M., & Berges, J. (1978). Il test dello schema corporeo. Una prova di conoscenza e costruzione dell’immagine del corpo [the body schema test. A test of knowledge and construction of body image]. Firenze, Italy: Organizzazioni Speciali.
Di Vita, A., Palermo, L., Piccardi, L., & Guariglia, C. (2015). Peculiar body representation alterations in hemineglect: A case report. Neurocase, 21(6), 697–706.
Di Vita, A., Palermo, L., Piccardi, L., Di Tella, J., Propato, F., & Guariglia, C. (2016). Body representation alterations in personal but not in Extrapersonal neglect patients. Applied Neuropsychology: Adult, 24(4), 308–317.
Dieguez, S., Staub, F., & Bogousslavsky, J. (2007). Asomatognosia. In O. Godefroy & J. Bogousslavsky (Eds.), The behavioral and cognitive neurology of stroke (pp. 215–253). Cambridge: Cambridge University Press.
Ehrenwald, H. (1930). Verändertes Erleben des Körperbildes mit konsekutiver Wahnbildung bei linksseitiger Hemiplegie. Monatsschrift Fur Psychiatrie Und Neurologie, 75, 89–97.
Ehrenwald, H. (1931). Anosognosie und Depersonalisation. Nervenarzt, 4, 681–688.
Facchin, A., Beschin, N., & Daini, R. (2016). Rehabilitation of right (personal) neglect by prism adaptation: A case report. Annals of Physical and Rehabilitation Medicine, 60(3), 220–222.
Feinberg, T. E., DeLuca, J., Giacino, J. T., Roane, D. M., & Solms, M. (2005). Right-hemisphere pathology and the self. In T. E. Feinberg & J. P. Keenan (Eds.), The lost self. Pathologies of the brain and identity (pp. 100–130). Oxford: Oxford University Press.
Feinberg, T. E., Roane, D. M., & Ali, J. (2000). Illusory limb movements in anosognosia for hemiplegia. Journal of Neurology, Neurosurgery, and Psychiatry, 68(4), 511–513.
Fortis, P., Maravita, A., Gallucci, M., Ronchi, R., Grassi, E., Senna, I., … Vallar, G. (2010). Rehabilitating patients with left spatial neglect by prism exposure during a visuomotor activity. Neuropsychology, 24(6), 681–697.
Frederiks, J. A. M. (1963). Occurrence and nature of phantom limb phenomena following amputation of body parts and following lesions of the central and peripheral nervous system. Psychiatria, Neurologia, Neurochirurgia, 66, 73–97.
Galati, G., Committeri, G., Sanes, J. N., & Pizzamiglio, L. (2001). Spatial coding of visual and somatic sensory information in body-centered coordinates. European Journal of Neuroscience, 14(4), 737–746.
Garbarini, F., Rabuffetti, M., Piedimonte, A., Pia, L., Ferrarin, M., Frassinetti, F., ..., Berti, A. (2012). ‘Moving’ a paralysed hand: bimanual coupling effect in patients with anosognosia for emiplegia. Brain, 135, 1486–1497.
Garcin, R., Varay, A., & Hadji-Dimo. (1938). Document pour servir à l’étude des troubles du schéma corporel (sur quelques phénomènes moteurs, gnosiques et quelques troubles de l’utilisation des members du côté gauche au cours d’un syndrome temporo-pariétal par tumeur, envisagés dans leurs rapports avec l’anosognosie et les troubles du schéma corporel). Revue Neurologique, 69, 498–510.
Gasparrini, B., Shealy, C., & Walters, D. (1980). Differences in size and spatial placement of drawings of left versus right hemisphere brain-damaged patients. Journal of Consulting and Clinical Psychology, 48(5), 670–672.
Gerstmann, J. (1942). Problem of imperception of disease and of impaired body territories with organic lesions. Archives of Neurology and Psychiatry, 48(6), 890–913.
Glocker, D., Bittl, P., & Kerkhoff, G. (2006). Construction and psychometric properties of a novel test for body representational neglect (vest test). Restorative Neurology and Neuroscience, 24(4–6), 303–317.
Goodenough, F. L. (1926). Measurement of intelligence by drawing. Chicago: World Book.
Groh-Bordin, C., Glocker, D., Bittl, P., Keller, I., Preger, R., Hildebrandt, H., & Kerkhoff, G. (2009). Scanning your body is different from performing body movements: A double dissociation between body representational neglect and apraxia. Neuropsychologia, 47(4), 1187–1192.
Guariglia, C., & Antonucci, G. (1992). Personal and extrapersonal neglect: A case of neglect dissociation. Neuropsychologia, 30(11), 1001–1009.
Guariglia, P., Matano, A., & Piccardi, L. (2014). Bisecting or not bisecting: This is the neglect question. Line bisection performance in the diagnosis of neglect in right brain-damaged patients. PLoS One, 9(6), e99700.
Halligan, P. W., Fink, G. R., Marshall, J. C., & Vallar, G. (2003). Spatial cognition: Evidence from visual neglect. Trends of Cognitive Science, 7(3), 125–133.
Halligan, P. W., Marshall, J. C., & Wade, D. T. (1993). Three arms: A case study of supernumerary phantom limb after right hemisphere stroke. Journal of Neurology, Neurosurgery, and Psychiatry, 56(2), 159–166.
Healton, E. B., Navarro, C., Bressman, S., & Brust, J. C. (1982). Subcortical neglect. Neurology, 32, 776–778.
Hécaen, H., de Ajuriaguerra, J., Le Guillant, L., & Angelergues, R. (1954). Delire centré sur un membre-fantome chez une hemiplegique gauche par lesion vasculaire avec anosognosie. L'Évolution Psychiatrique (Paris), 2, 275–279.
Heilman, K. M., Bowers, D., Coslett, H. B., Whelan, H., & Watson, R. T. (1985). Directional hypokinesia: Prolonged reaction times for leftward movements in patients with right hemisphere lesions and neglect. Neurology, 35(6), 855–859.
Heilman, K. M., Bowers, D., & Watson, R. T. (1983). Performance on hemispatial pointing task by patients with neglect syndrome. Neurology, 33(5), 661–664.
Invernizzi, P., Gandola, M., Romano, D., Zapparoli, L., Bottini, G., & Paulesu, E. (2013). What is mine? Behavioral and anatomical dissociations between somatoparaphrenia and anosognosia for hemiplegia. Behavioural Neurology, 26(1–2), 139–150.
Iosa, M., Guariglia, C., Matano, A., Paolucci, S., & Pizzamiglio, L. (2016). Recovery of personal neglect. European Journal of Physical and Rehabilitation Medicine, 52(6), 791–798.
Jehkonen, M., Laihosalo, M., & Kettunen, J. E. (2006). Impact of neglect on functional outcome after stroke: A review of methodological issues and recent research findings. Restorative Neurology and Neuroscience, 24(4–6), 209–215.
Jenkinson, P., Moro, V., & Fotopoulou, A. (in press) Asomatognosia. Cortex.
Kandel, E. R., Schwarts, J. H., Jessel, M. T., Siegelbaum, S. A., & Hudspeth, T. H. (2012). Principles of neuroscience. London: McGraw-Hill Professional.
Karnath, H. O., Sievering, D., & Fetter, M. (1994). The interactive contribution of neck muscle proprioception and vestibular stimulation to subjective "straight ahead" orientation in man. Experimental Brain Research, 101(1), 140–146.
Kesayan, T., Lamb, D., Williamson, J., Falchook, A., & Heilman, K. (2016). Perceptual pseudoneglect: Laterality and the perception of tactile pressure. Neurology, 86(16) Supplement P4.056.
Kramer. (1915). Alloästhesie und fehlende Wahrnehmung der gelähmten körperhälfte bei subvertikalem Hirnherd. Neurol Centralblatt, 34, 287–288.
Laplane, D., & Degos, J. D. (1983). Motor neglect. Journal of Neurology, Neurosurgery, and Psychiatry, 46(2), 152–158.
Lhermitte, J., & Tchehrazi, E. (1937). L’image du moi corporel et ses deformations pathologiques. Encéphale, 32, 1–24.
Lindell, A. B., Jalas, M. J., Tenovuo, O., Brunila, T., Voeten, M. J., & Hämäläinen, H. (2007). Clinical assessment of hemispatial neglect: Evaluation of different measures and dimensions. The Clinical Neuropsychologist, 21(3), 479–497.
List, A., Brooks, J. L., Esterman, M., & Flevaris, A. V. (2008). Visual hemispatial neglect, re-assessed. Journal of International Neuropsychological Society, 14(2), 243–256.
Maguire, A.M., &. Ogden, J.A. (2002). MRI brain scan analyses and neuropsychological profiles of nine patients with persisting unilateral neglect. Neuropsychologia; 40 (7), 879–887.
Marangolo, P., Piccardi, L., & Rinaldi, M. C. (2003). Dissociation between personal and Extrapersonal neglect in a crossed aphasia study. Neurocase, 9(5), 414–420.
McIntosh, R. D., Brodie, E. E., Beschin, N., & Robertson, I. H. (2000). Improving the clinical diagnosis of personal neglect: A reformulated comb and razor test. Cortex, 36(2), 289–292.
Moro, V., Pernigo, S., Tsakiris, M., Avesani, R., Edelstyn, N. M. J., Jenkinson, P. M., & Fotopoulou, A. (2016). Motor versus body awareness: Voxel-based lesion analysis in anosognosia for hemiplegia and somatoparaphrenia following right hemisphere stroke. Cortex, 83, 62–77.
Moro, V., Zampini, M., & Aglioti, S. M. (2004). Changes in spatial position of hands modify tactile extinction but not disownership of contralesional hand in two right brain-damaged patients. Neurocase, 10(6), 437–443.
Nightingale, S. (1982). Somatoparaphrenia: a case report. Cortex, 18(3), 463–467.
Ortigue, S., Mégevand, P., Perren, F., Landis, T., & Blanke, O. (2006). Double dissociation between representational personal and extrapersonal neglect. Neurology, 66(9), 1414–1417.
Palermo, L., Di Vita, A., Piccardi, L., Traballesi, M., & Guariglia, C. (2014). Bottom-up and top-down processes in body representation: A study of brain-damaged and amputee patients. Neuropsychology, 28(5), 772–781.
Parsons, L. M. (1987a). Imagined spatial transformation of one's body. Journal of Experimental Psychology: General, 116(2), 172–191.
Parsons, L. M. (1987b). Imagined spatial transformations of one’s hands and feet. Cognitive Psychology, 19(2), 178–241.
Patterson, A., & Zangwill, O. L. (1944). Disorder of visual space perception associated with lesion of the right cerebral hemisphere. Brain, 67(4), 331–358.
Paulig, M., Weber, M., & Garbelotto, S. (2000). Somatoparaphrenie. Eine “plusvariante” der Anosognosie für Hemiplegie [Somatoparaphrenia. A positive variant of anosognosia for emiplegia]. Nervenarzt, 71(2), 123–129.
Peru, A., & Pinna, G. (1997). Right personal neglect following a left hemisphere stroke. A case report. Cortex, 33(3), 585–590.
Pinel, J. P. J. (2009). Biopsychology. Harlow, Essex: Pearson Education Limited.
Pizzamiglio, L., Cappa, S., Vallar, G., Zoccolotti, P., Bottini, G., Ciurli, P., Guariglia, C., & Antonucci, G. (1989). Cortex, 25(3), 471–477.
Pizzamiglio, L., Guariglia, C., Antonucci, G., & Zoccolotti, P. (2006). Development of a rehabilitative program for unilateral neglect. Restorative Neurology and Neuroscience, 24(4–6), 337–345.
Punt, T. D., & Riddoch, M. J. (2006). Motor neglect: Implications for movement and rehabilitation following stroke. Disability and Rehabilitation, 28(13–14), 857–864.
Reinhart, S., Schmidt, L., Kuhn, C., Rosenthal, A., Schenk, T., Keller, I., & Kerkhoff, G. (2012). Limb activation ameliorates body-related deficits in spatial neglect. Frontiers in Human Neuroscience, 6, 188.
Reznikoff, M., & Tomblen, D. (1956). The use of human figure drawings in the diagnosis of organic pathology. Journal of Consulting and Clinical Psychology, 20(6), 467–470.
Richard, C., Honoré, J., & Rousseaux, M. (2000). Is there a distortion of body projection in extracorporeal space in neglect patients? Neuroreport, 11(13), 3047–3051.
Richard, C., Rousseaux, M., Saj, A., & Honoré, J. (2004). Straight ahead in spatial neglect: Evidence that space is shifted, not rotated. Neurology, 63(11), 2136–2138.
Riklan, M., Zahn, T. P., & Diller, L. (1962). Human figure before and after chemosurgery of basal ganglion in parkinsonism. Journal of Nervous and Mental Disease, 135, 500–506.
Rizzolatti, G., Matelli, M., & Pavesi, G. (1983). Deficits in attention and movement following the removal of postarcuate (area 6) and prearcuate (area 8) cortex in macaque monkeys. Brain, 106(Pt 3), 655–673.
Rode, G., Charles, N., Perenin, M. T., Vighetto, A., Trillet, M., & Aimard, G. (1992). Partial remission of hemiplegia and somatoparaphrenia through vestibular stimulation in a case of unilateral neglect. Cortex, 28(2), 203–208.
Rode, G., Pagliari, C., Huchon, L., Rossetti, Y., & Pisella, L. (2016). Semiology of neglect: An update. Annals of Physical and Rehabilitation Medicine, 60(3), 177–185.
Ronchi, R., Heydrich, L., Serino, A., & Blanke, O. (2017). Illusory hand ownership in a patient with personal neglect for the upper limb, but no somatoparaphenia. Journal of Neuropsychology. https://doi.org/10.1111/jnp.12123 (published online ahead of print 17 April).
Roth, M. (1949). Disorders of the body image caused by lesions of the right parietal lobe. Brain, 72, 89–111.
Rousseaux, M., Allart, E., Bernati, T., & Saj, A. (2015). Anatomical and psychometric relationships of behavioral neglect in daily living. Neuropsychologia, 70, 64–70.
Rousseaux, M., Sauer, A., Saj, A., Bernati, T., & Honoré, J. (2013). Mislocalization of tactile stimuli applied to the trunk in spatial neglect. Cortex, 49(10), 2607–2615.
Rubinstein, L. H. (1941). Imperception for the position of the eyelids on one side. Journal of Neurology, Neurosurgery, and Psychiatry, 4, 191–205.
Saevarsson, S., Eger, S., & Gutierrez-Herrera, M. (2014). Neglected premotor neglect. Frontiers in Human Neuroscience, 8, 778.
Sambo, C. F., Vallar, G., Fortis, P., Ronchi, R., Posteraro, L., Forster, B., & Maravita, A. (2012). Visual and spatial modulation of tactile extinction: Behavioural and electrophysiological evidence. Frontiers in Human Neuroscience, 6, 217.
Sampanis, D. S., & Riddoch, J. (2013). Motor neglect and future directions for research. Frontiers in Human Neuroscience, 7, 110.
Sandifer, P. H. (1946). Anosognosia and disorders of body scheme. Brain, 69(2), 122–137.
Schiff, N. D., & Pulver, M. (1999). Does vestibular stimulation activate thalamocortical mechanisms that reintegrate impaired cortical regions? Proceeding Biological Science, 266(1417), 421–423.
Schilder, P. (1935). The image and appearance of the human body. New York: International Universities Press.
Schulman, J. C., Kaspar, J. C., & Throne, F. M. (1965). Brain damage and behavior. Springfield, IL: Charles C. Thomas.
Ska, B., & Nespoulous, J. L. (1987). Pantomimes and aging. Journal of Clinical and Experimental Neuropsychology, 9(6), 754–766.
Spaccavento, S., Cellamare, F., Falcone, R., Loverre, A., & Nardulli, R. (2017). Effect of subtypes of neglect on functional outcome in stroke patients. Annals of Physical and Rehabilitation Medicine, 60, 376–381.
Starkstein, S. E., Berthier, M. L., Fedoro, V. P., Price, T. R., & Robinson, R. G. (1990). Anosognosia and major depression in 2 patients with cerebrovascular lesions. Neurology, 40(9), 1380–1382.
Tei, H. (2000). Right ipsilateral hypersensation in a case of anosognosia for hemiplegia an,d personal neglect with the patient’s subjective experience. Journal of Neurology, Neurosurgery, and Psychiatry, 69(2), 274–283.
Vallar, G. (1998). Spatial hemineglect in humans. Trends of Cognitive Science, 2(3), 87–97.
Vallar, G., & Bolognini, N. (2014). Unilateral spatial neglect. In A. C. (. K.). Nobre & S. Kastner (Eds.), The Oxford handbook of attention (pp. 972–1027). Oxford: Oxford University Press.
Vallar, G., & Ronchi, R. (2009). Somatoparaphrenia: A body delusion. A review of the neuropsychological literature. Experimental Brain Research, 192(3), 533–551.
Vallar, G., Sterzi, R., Bottini, G., Cappa, S., & Rusconi, M. L. (1990). Temporary remission of left hemianesthesia after vestibular stimulation. A sensory neglect phenomenon. Cortex, 26(1), 123–131.
Verret, J. M., & Lapresle, J. (1978). Syndrome d’Anton-Babinski avec reconnaissance du membre supérieur gauche lors de sa vision dans un miroir. Revue Neurologique, 134, 709–713.
Von Hagen, K. O., & Ives, E. R. (1937). Anosognosia (Babinski), imperception of hemiplegia. Bulletin of the Los Angeles Neurological Societies, 2, 95–103.
Weinstein, E. A., & Kahn, R. L. (1950). The syndrome of anosognosia. Archives of Neurology and Psychiatry, 64, 772–791.
Weinstein, E. A., Kahn, R. L., Malitz, S., & Rozanski, J. (1954). Delusional reduplication of parts of the body. Brain, 77, 45–60.
Wilson, B., Cockburn, J., & Halligan, P. (1987). Development of a behavioral test of visuospatial neglect. Archives of Physical and Medical Rehabilitation, 68(2), 98–102.
Wortis, H., & Dattner, B. (1942). An analysis of a somatic delusion. A case report. Psychosomatic Medicine, 4, 319–323.
Zingerle, H. (1913). Über Störungen der Wahrnehmung des eigenen Körpers bei organischen Gehirnerkrankungen. Monatschr f Psychiat und Neurol, 34, 13–36.
Zoccolotti, P., & Judica, A. (1991). Functional evaluation of hemineglect by means of a semistructured scale: Personal and extrapersonal differentiation. Neuropsychological Rehabilitation, 1(1), 33–44.
Acknowledgements
The authors thank Dr. Gianna Cocchini for her valuable contribution to the manuscript. The authors also thank Hannah Gregory and Xavier Job for proofreading the manuscript. This study was partly supported by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Caggiano, P., Jehkonen, M. The ‘Neglected’ Personal Neglect. Neuropsychol Rev 28, 417–435 (2018). https://doi.org/10.1007/s11065-018-9394-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11065-018-9394-4