
Abstract
Objectives
To describe demographic characteristics and health-related social needs of families who accessed maternal-infant care through a mobile medical clinic (MMC) during the COVID-19 pandemic and to explore feasibility, acceptability, perceived benefits, and barriers to care.
Methods
In this mixed-methods observational study, chart reviews, telephone surveys, and qualitative interviews in English and Spanish were conducted with caregivers who accessed the MMC between April and November 2020. Qualitative interviews were analyzed with the constant comparative method alongside descriptive chart and survey data analyses.
Results
Of 139 caregiver-infant dyads contacted, 68 (48.9%) completed the survey; 27 also completed the qualitative interview. The survey participants did not differ from the larger sample; most (86.7%) were people of color (52.9% identified as Latino and 33.8% as Black). Health-related social needs were high, including food insecurity (52.9%), diaper insecurity (44.1%), and anxiety (32%). Four women (6.1%) were diagnosed with hypertension requiring urgent evaluation. Nearly all (98.5%) reported being very satisfied with the services. Major themes from qualitative interviews included (1) perceived patient- and family-centered care, (2) perceived safety, and (3) perceived benefits of dyadic mother-infant care.
Conclusions for Practice
In this assessment of caregivers who accessed the MMC—a rapidly-developed COVID-19 pandemic response—insights from caregivers, predominantly people of color, provided considerations for future postpartum/postnatal service delivery. Perceptions that the MMC addressed health-related social needs and barriers to traditional office-based visits and the identification of maternal hypertension requiring urgent intervention suggest that innovative models for postpartum mother-infant care may have long-lasting benefits.
Similar content being viewed by others


Significance
These findings support the need for innovative models for postpartum mother-infant care during and beyond the pandemic to provide dyadic care and material support. Ongoing studies of community outreach efforts like the MMC, which focus on dyadic care, can evaluate comparative effectiveness of maternal and infant outcomes.
Introduction
Postpartum maternal and neonatal health care schedules, endorsed by American College of Gynecology (ACOG) and American Academy of Pediatrics (AAP) guidelines, respectively, promote the health and well-being of birthing persons and the nearly 4 million infants born annually in the US (“ACOG Committee Opinion No. 736,” 2018; Hagan et al., 2017; Martin et al., 2019; McInerny et al., 2016). Assessments of mothers and infants provide critical opportunities to screen for and detect postpartum depression and health-related social needs (HRSN) affecting families (“ACOG Committee Opinion No. 736,” 2018; McInerny et al., 2016).
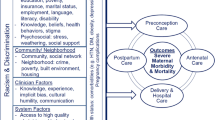
In 2018, the ACOG Committee on Obstetrics Practice substantially shifted its recommendations for maternal postpartum care from a single visit at 4–6 weeks to earlier, frequent, individualized care during the first 12 weeks postpartum—“the fourth trimester”—a period that lays the groundwork for healthier futures for women and families. These recommendations evolved from the United States’ unacceptably high maternal mortality rate, which has more than doubled since 1990 (World Health Organization, 2019). For women with pregnancy complications, short-interval follow-up can mitigate the risk of postpartum pregnancy-related deaths, 35% of which occur between 24 h to 6 weeks postpartum (“ACOG Committee Opinion No. 736,” 2018; Kassebaum et al., 2014) and can address the higher lifetime risk of developing cardiovascular disease associated with adverse pregnancy outcomes (Canoy et al., 2016; Grandi et al., 2019; Parikh et al., 2021; Riise et al., 2019; Theilen et al., 2018).
Despite the public health importance of postpartum care for women and infants, there are substantial and longstanding barriers to and disparities in accessing regular and recommended postpartum care. Even though frequent care is indicated for at-risk women, about 40% do not attend the six-week postpartum visit. Attendance rates are lower among women with limited resources, lack of insurance or underinsurance, or individuals with difficulty communicating with their healthcare providers (“ACOG Committee Opinion No. 736,” 2018; Bennett et al., 2014; Bryant et al., 2006; Danilack et al., 2019; Daw et al., 2020). These disparities extend to stark gaps in maternal and infant health outcomes in the US, with significantly high morbidity and mortality among Non-Latino Black women and infants (CDC Infant Mortality, 2020; CDC Pregnancy Mortality Surveillance System, 2020; Howell & Zeitlin, 2017).
As with other disaster-related events (DeYoung & Mangum, 2021), the COVID-19 pandemic exacerbated existing challenges in postpartum care, including economic challenges and interrupted support structures for perinatal care (Barbosa-Leiker et al., 2021; Kinser et al., 2021). Because of uncertainties about transmission and hospital burdens of caring for COVID-19 patients, postpartum stays were shortened, and other services, such as depression screening and lactation support, were limited (DeYoung & Mangum, 2021; Hendrix et al., 2021).
Mobile medical clinic (MMC) strategies can bridge community and medical systems and decrease barriers to accessing care, especially for patients from racial and ethnic minority groups disproportionately impacted by health inequities (Hendel, 2022; Yu et al., 2017). For women who are pregnant or who have recently given birth, MMCs have been associated with improved hypertension management, decreased emergency care utilization, lower cost, and earlier initiation of prenatal care with fewer preterm births (Edgerley et al., 2007; O’Connell et al., 2010; Song et al., 2013).
In light of the many challenges related to accessing care during the COVID-19 pandemic, primary care clinicians at our institution re-purposed an MMC to provide medical care to newborns and women near or outside their homes. The MMC was deployed to respond to both pandemic concerns (related to community transmission of COVID-19 and heightened transportation barriers) and to provide patient- and family-centered postpartum and neonatal care to narrow pandemic-generated health disparities. In this mixed methods study, we describe demographic characteristics and HRSN of families (caregivers and infants) who accessed maternal-infant care through the MMC and explore intervention feasibility (Lancaster & Thabane, 2019), acceptability, perceived benefits, and barriers to care.
Methods
Setting
New Haven, Connecticut, with a population of 130,000, is disproportionately impacted by poverty, unemployment, an elevated infant mortality rate, substance use, and HIV (Data Haven, 2016). To address the HIV and substance use epidemics, a 40-foot MMC has provided free healthcare since 1993 (Gibson et al., 2014; Morano et al., 2013a, 2013b; Morano et al., 2014a, 2014b). Redeployed in April 2020 for maternal-infant care during the COVID-19 pandemic, the MMC, staffed by a Family Nurse Practitioner and a Medical Assistant, offers clinical assessments of newborns (vital signs, growth, limited physical exam, transcutaneous bilirubin when needed) and women (vital signs, wound healing, mood) in safe, accessible, physically distanced, community settings.
Sample Population
Of the 170 caregivers who attended MMC appointments during this period, eight were excluded because a language other than Spanish or English was listed as their primary language in the electronic health record (Fig. 1). Purposive sampling for the concurrent surveys and interviews preferentially included (1) recent attendees and (2) attendees who listed Spanish as their primary language. The study was exempt by our institution’s Internal Review Board, and all respondents provided verbal informed consent to participate and for collection of deidentified chart data.

Caregivers who received care at the mobile medical clinic and completed surveys/interviews
Study Design
We used a convergent mixed methods design (Curry & Nunez-Smith, 2015; Fetters et al., 2013) to conduct and analyze a telephone survey (all respondents) and interview (until thematic saturation) with caregivers whose preferred language in the electronic health records was English and/or Spanish and who received care at the MMC between April and November 2020. Surveys/interviews occurred one to nine months after the MMC encounter.
Survey and Semi-Structured Interview Development
The survey and semi-structured interview guide (Supplemental Table 1), developed and iteratively refined by our research team, included demographic components modeled from the American Community, National Health and Education, and National Immunization Surveys (National Immunization Surveys | CDC, 2021; NHANES—National Health and Nutrition Examination Survey Homepage, 2021; US Census Bureau, 2021) and previously-validated instruments to assess COVID-19 symptoms and exposures, food insecurity, diaper insecurity, anxiety, and means of transportation (Hager et al., 2010; Nelson et al., 2020; Silver et al., 2012; Smith et al., 2013; Spitzer et al., 2006).
Telephone Interviews and Chart Data Collection
Following recruitment and verbal informed consent, English- and/or Spanish-speaking members of the research team conducted both a structured survey and semi-structured qualitative interview with participants. A three-person coding team of a health services researcher, a primary care pediatrician, and a medical student (JR, LS, MB) independently developed codes and created a codebook by consensus. We recorded survey responses in Qualtrics® (Qualtrics, Provo, Utah) and, separately, we recorded contact information to send participants a $20 gift card. All respondents were provided information about additional services and resources for mental health, nutrition, and medical resources at the conclusion of the survey. Semi-structured interview components were audio-recorded, transcribed with the automatic transcription software Trint®, and manually edited. Once we reached thematic saturation, we continued to administer the structured telephone survey without the semi-structured interview components. Full surveys with semi-structured qualitative interviews ranged from approximately 20 to 40 min in duration, while structured surveys alone ranged approximately 10 to 30 min. For all caregiver-infant dyads who consented to participate in the study, we collected the following infant data via medical chart review: number of MMC visits, bilirubin assessments, COVID-19 test results, and vitamin D prescriptions (Supplemental Table 2). For the 66 of 68 postpartum women who were evaluated on the MMC, maternal blood pressure evaluations, maternal follow-up appointment data, and COVID-19 test results were also collected via chart review. Survey data and chart review data were linked and subsequently de-identified.
Mixed Methods Analyses
Descriptive analyses of survey data and chart review using proportions were analyzed using Stata (StataCorp, 2017). Transcripts were analyzed with grounded theory methodology using the constant comparative method in Dedoose® (Corbin & Strauss, 2008). The coding team analyzed all transcripts (with two coders—JR and MB—analyzing Spanish-language transcripts) and discrepancies were resolved through an iterative process. Codes were then sorted into emerging themes and reviewed and modified with the larger research team. Representative Spanish-language quotations were translated after analysis, and original Spanish-language quotations can be found in the Supplement. We used an intervention mixed methods framework to perform connected integration of qualitative and quantitative results (Curry & Nunez-Smith, 2015; Fetters et al., 2013). We followed the COREQ criteria for reporting qualitative research (Tong et al., 2007).
Results
Of the 162 eligible caregivers, we attempted to reach 139 (97 English-preferred and 42 Spanish-preferred) and successfully completed 68 surveys, 27 of which also included qualitative interviews, of caregivers of 69 children (one set of twins) with a 48.9% response rate (Fig. 1).
Sociodemographic Characteristics
Nearly all caregiver respondents were mothers (91.2%). Over half (52.9%) identified as Latino and 33.8% as Non-Latino Black (Table 1). Nearly half (44.1%) lived in multilingual households, 44.1% had education beyond high school, and just over half (52.9%) were married or living with a partner. Most (89.9%) made one or two visits to the MMC (Table 1). Most women had public insurance (63.3%), and many (22.7%) were uninsured (Table 2).
Infant and Maternal Health Characteristics
Four caregivers (5.9%) reported contact with someone who tested positive for SARS-CoV2, and two mother-infant dyads (2.9%) tested positive after discharge. No women or infants tested positive for SARS–CoV2 during their birth admissions. We found no cases of hyperbilirubinemia requiring phototherapy. Although most (89.9%) reported ever breastfeeding, nearly all (94.2%) had fed formula, and only half (49.3%) were still breastfeeding at the time of the survey (Table 2).
According to chart review, two-thirds of women who were evaluated on the MMC attended an in-person or telehealth postpartum visit, and 16.7% had a documented missed postpartum visit. All women evaluated on the MMC had blood pressure evaluated. Over two-thirds (69.7%) had at least one postpartum blood pressure reading > 120/80 mmHg, and 19.6% had readings elevated enough to require contact with the obstetric provider for further guidance. Follow-up visits with either an outpatient or obstetric provider regarding blood pressure then occurred in 15.2% of mothers, and four (6.1%) required emergent treatment and/or readmission to the hospital for postpartum hypertension detected on the MMC (Table 2).
Health-Related Social Needs (HRSN) of Caregivers
About half of caregivers screened positive for food insecurity (52.9%), diaper insecurity (44.1%), and use of Supplemental Nutritional Assistance Program (SNAP) (55.9%). About one-third of respondents screened positive for mild (16.2%), moderate (8.9%), or severe (1.5%) anxiety. Most respondents were somewhat and/or very worried about contracting COVID-19 and about finances related to COVID-19 (69.1% for both) (Table 3).
One-quarter of respondents reported missing an office appointment because of transportation problems. About one-third (29.4%) reported that they found it “somewhat” or “very” challenging to get to the doctor’s office (Table 3). When asked about transportation, most reported that they typically traveled by driving themselves or obtaining a ride with family and/or friends, while 5.9% reported taking a taxi-like service, 4.4% reported using a bus, and 1.5% reported walking.
Acceptability and Satisfaction
Table 4 demonstrates satisfaction measures from survey responses. Nearly all caregivers reported they were very satisfied and very likely to recommend the MMC to friends (98.5% and 94.1%, respectively), with responses like: “They exceeded my expectations,” and “It was better than expected” (Respondents #4 and #5, respectively). Most (85.3%) had no suggestions for improvement, although some requested additional resources and space (“I'm kind of claustrophobic and it was kind of tight.” –Respondent #2).
About two-thirds (66.2%) preferred the MMC for future visits over the office location, 7.3% preferred the office, and 26.5% expressed no location preference.
As we discussed the acceptability and satisfaction with caregivers, perceived patient- and family-centered care and respectful interactions were common threads through many responses, with many expressing a desire to expand services.
“Even like if they have this when I was pregnant too. It would have been nice to be able to go down and talk to somebody in a in a situation like this instead of having to go all the way down there, you know, nine months pregnant, you know, risking getting sick and everything. So if you guys have a possibility to expand this, I would go for it.” – Respondent #18
Themes from Qualitative Interviews
Major themes from the qualitative analysis of interviews included (1) patient- and family-centered care, (2) perceived safety, and (3) perceived benefits of dyadic mother-infant care (Table 5).
Patient- and Family-Centered Care
Perceived delivery of patient- and family-centered care, in which patient/family goals, values, and preferences guide provision of healthcare, was evident in several subthemes related to the patient experience on the MMC. This included patient- and family-centeredness around aspects of convenience, communication, privacy, continuity of care, acceptability and intervention feasibility, and resources provided to address HRSN.
Related to patient- and family-centered convenience, caregivers discussed transportation, childcare, and scheduling as typical burdens and inconveniences of in-person office visits eased by the MMC. One participant noted the convenience of not needing to coordinate travel or childcare for other children while home schooling during COVID-19:
“Because I have two other kids that are toddlers and they do virtual school, so it's hard to go all out once over there. And then also taking the baby out.” – Respondent #11
Many respondents reflected that, in contrast to prior in-office experiences, they faced fewer barriers to communication with MMC staff and had positive interactions during the scheduling process, appointment confirmations, and discussing care for themselves and their newborns:
“I spoke with a person directly and they would always arrange the arrival time and call a day ahead of time to confirm that they were coming, to see if everything was okay with me, and that I didn’t have COVID symptoms and that everything was good.” – Respondent #24
Privacy was appreciated as a component of patient- and family-centered care for providing respectful, personalized interactions with the MMC staff:
“I mean I just like it because you're by yourself. It's private, you're by yourself. Just you and the staff which is nice.” – Respondent #3
Perceived Safety
Perceived safety from exposure to communicable diseases, especially related to COVID-19, was a major theme that emerged from discussions with many caregivers. There was often overlap with patient- and family-centered care and convenience, as the components of the MMC model which provided convenience for transportation, childcare, privacy, ease of scheduling and communication also allowed many caregivers physical space and reassurance around COVID-19 safety during the height of the pandemic in 2020:
“Honestly, the [MMC] is just better, with no other patients on the [MMC]. So I just you know, I'm just scared because people start coughing, don't cover their mouth. At the clinic, that's what I'm worried about. But the [MMC] is literally just you, so you don't have to worry about much.” – Respondent #3
“I would recommend it, since newborn babies leave the hospital without vaccines and are low in defenses and, well, we can avoid exposure for them.” –Respondent #24
Perceived Benefits of Dyadic Care
The final theme reflected the perceived benefits of dyadic care, in which participants expressed how engaging the mother-infant dyad in care together provided opportunities for improved health for both caregivers and their infants.
One woman discussed how the MMC evaluation provided her confidence as she continued to breastfeed:
“Because I can keep track on his weight because I have mastitis. So I was worried he wasn't getting enough nutrients and enough milk, but everything was all good. That's how I can keep track, with the [MMC].” – Respondent #12
This woman, like many, often mentioned her own health as secondary to the health of her child. Similarly, when asking about care for themselves, caregivers would often respond in the context of caring for their children, especially for women recovering from Caesarean sections who had added barriers to care:
“And I was glad that they had that because I can't drive right now because I had a C-section with the boys…It was like a relief for me. You know, I'm going [to the office] all the time…So I was glad when they told me about the [MMC] doing home visits, I was really glad that they had that service available.” – Respondent #13
Furthermore, as noted above, many women had not yet attended a postpartum visit, and yet the MMC clinicians detected many instances of elevated blood pressure and several instances of hypertension requiring urgent or emergent medical management. For one woman who was admitted, her focus remained on her child, only disclosing her own admission after being explicitly asked about her experience with blood pressure checks:
“Because I thought it was only for [my daughter], they were going to check her up and then I realized it was also for me. So when they checked me, I found out that I was with high blood pressure. So then I went back to the hospital for two days with my magnesium and everything.” – Respondent #15
Discussion
In this mixed methods evaluation of a MMC that was emergently repurposed to provide postpartum/postnatal care for women and neonates during the early COVID-19 pandemic, findings suggest high acceptability especially related to perceived safety and feelings that certain transportation and social needs were addressed. Respondents found services acceptable, feasible, and, importantly, patient- and family-centered. In addition, 15% of women had instances of maternal hypertension requiring follow-up with an obstetrician, and 6% of women required emergent evaluation and treatment. The MMC, deployed during the COVID-19 pandemic to address COVID-19 safety concerns, could be one of many dyadic outreach interventions to help to improve patient- and family-centered care and reduce disparities in access to postpartum and neonatal care for underserved populations.
From both qualitative and quantitative responses, we found high levels of satisfaction related to patient- and family-centeredness. Patient-centered care is defined by the Institute of Medicine as, “providing care that is respectful and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions” (Institute of Medicine (US) Committee on Quality of Health Care in America, 2001). Patient- and family-centered care emphasizes “collaborating with people of all ages, at all levels of care, and in all health care settings” according to the Institute for Patient- and Family-Centered Care (Institute for Patient & Family Centered Care, 2021).
Elements of the six domains of patient- and family-centeredness, described in a 2019 Academy Health report (Sinaiko et al., 2019) and modified in Fig. 2, were addressed through the MMC. The domains include (1) addressing caregiver and provider goals, (2) adjusting to life circumstances, including COVID-19 modifications, (3) respecting values and culture, (4) allowing options for provider care preference, (5) addressing health status and symptoms, and (6) promoting equitable access. All six of these domains were reflected in the qualitative responses, especially as patients shared their experiences with the MMC related to convenience, communication, and privacy. This respectful and responsive care was appreciated by families and, for some, contrasted with the patient experience in usual clinic-based care. Focusing on patient values through patient- and family-centered care must guide initiatives aimed at improving equitable access to health care and decreasing the significant inequities in US maternal and infant health outcomes (CDC Infant Mortality, 2020; CDC Pregnancy Mortality Surveillance System, 2020; Howell & Zeitlin, 2017).

Achieving domains of patient- and family-centeredness on the mobile medical clinic
Beyond offering patient- and family-centered care, the MMC provided hypertension screening for postpartum women. The MMC’s linkage to primary provider and/or specialist referrals resulted in follow-up for many, and in emergent treatment for 6% of women in our study. The US has the highest rate of maternal mortality among high-income countries, with Non-Latino Black women at disproportionately high risk of dying from a pregnancy-related complications (World Health Organization, 2019). Cardiovascular disease and hypertensive disorders of pregnancy are leading causes of maternal mortality (Petersen et al., 2019). One of the greatest shortcomings in the current health system, especially in light of the fractured care and missed visits that have occurred during the pandemic, is a safe transfer of care between the obstetrician and primary care provider for women with known risk (Hendrix et al., 2021; Parikh et al., 2021). The MMC is one possible model to provide frequent and individualized postpartum care that can help identify women with high-risk conditions and facilitate potentially life- and cost-saving follow up during the twelve week postpartum period (“the fourth trimester”) and beyond (World Health Organization, 2019).
Approximately half of the respondents reported HRSNs of food insecurity, diaper insecurity, and/or use of the Supplemental Nutrition Assistance Program. Consistent with prior research, caregivers also expressed substantial anxiety and stress related to the COVID-19 pandemic (Basu et al., 2021; Boekhorst et al., 2021; Chmielewska et al., 2021; Hessami et al., 2020; Liu et al., 2021; Mariño-Narvaez et al., 2021; Mayopoulos et al., 2021; Silverman et al., 2020). Worldwide, the pandemic has been associated with worsened maternal and infant outcomes, including significant increases in stillbirth, maternal death, and postnatal depression (Chmielewska et al., 2021). This pandemic has also worsened many material hardships, with rates of food insecurity doubling nationwide and tripling in families with children (Keith-Jennings et al., 2021). Multiple studies have found maternal stress, anxiety, and loneliness have worsened since the onset of the pandemic, although studies have found varying changes in depression scores (Basu et al., 2021; Boekhorst et al., 2021; Chmielewska et al., 2021; Hessami et al., 2020; Liu et al., 2021; Mariño-Narvaez et al., 2021; Mayopoulos et al., 2021; Silverman et al., 2020). Allaying material hardships such as diaper insecurity is one way to reduce caregiver stress (Smith et al., 2013), and many caregivers we surveyed expressed appreciation for the material items—including diapers and creams—that were provided as part of the MMC outreach efforts. Thus, direct material support through provision of items including diapers and food may continue to be key interventions for health providers’ community outreach efforts, not only to alleviate these direct material hardships but also to mitigate caregiver anxiety and stress.
A key element of this MMC iteration was the provision of dyadic mother-infant care provided by a Family Nurse Practitioner. As highlighted in a framework for maternal-infant dyad care model developed and described by Glazer, et al., applying a dyadic approach is a crucial paradigm shift which can break down silos to address the multifactorial maternal-infant health disparities and accompanying lifelong health outcomes (Glazer et al., 2021). As was noted by the multiple instances of maternal hypertension that were detected and treated through the MMC, even when caregivers were focused on their children, dyadic care offers opportunities for maternal evaluations during the “fourth trimester.” These evaluations, which may have otherwise been missed, may help to meet the mutual goals of both AAP and ACOG postpartum care schedules and reduce morbidity and mortality (“ACOG Committee Opinion No. 736,” 2018; McInerny et al., 2016).
Limitations included a small clinical sample further reduced by time and budgetary restraints which restricted the ability to contact all participating families. Social desirability bias and recall bias may have affected responses, as some respondents were surveyed months after their MMC visit. We tried to minimize social desirability bias by using an independent interviewer and to minimize recall bias by asking questions in a variety of ways to approach the constructs of interest. Furthermore, we conducted this study in English and Spanish, but respondents who spoke other languages were excluded, which constrained the evaluation of language barriers.
Conclusions for Practice
Many caregivers who accessed care on a mobile medical clinic during the COVID-19 pandemic reported a high level of satisfaction, especially related to patient- and family-centered care, and, importantly, the mobile medical clinic clinicians detected multiple instances of maternal hypertension requiring emergent treatment and care. Caregivers identified health-related social needs including food insecurity, diaper insecurity, and use of SNAP and significant anxiety related to COVID-19 transmission. These findings support the need for innovative models for postpartum mother-infant care during and beyond the pandemic to provide dyadic care and material support. Ongoing studies of community outreach efforts like the MMC, which focus on dyadic care, can evaluate comparative effectiveness of maternal and infant outcomes. Sustainability of such programs will require support from hospitals and community-based pediatric practices to support increased patient- and family-centered care initiatives for maternal-infant dyads.
Data Availability
Available at: https://dataverse.harvard.edu/dataverse/MMC
Code Availability
N/A.
References
ACOG Committee Opinion No. (2018). 736: Optimizing postpartum care. Obstetrics and Gynecology, 131(5), e140–e150. https://doi.org/10.1097/AOG.0000000000002633
Barbosa-Leiker, C., Smith, C. L., Crespi, E. J., Brooks, O., Burduli, E., Ranjo, S., Carty, C. L., Hebert, L. E., Waters, S. F., & Gartstein, M. A. (2021). Stressors, coping, and resources needed during the COVID-19 pandemic in a sample of perinatal women. BMC Pregnancy and Childbirth, 21(1), 171. https://doi.org/10.1186/s12884-021-03665-0
Basu, A., Kim, H. H., Basaldua, R., Choi, K. W., Charron, L., Kelsall, N., Hernandez-Diaz, S., Wyszynski, D. F., & Koenen, K. C. (2021). A cross-national study of factors associated with women’s perinatal mental health and wellbeing during the COVID-19 pandemic. PLoS ONE, 16(4), e0249780. https://doi.org/10.1371/journal.pone.0249780
Bennett, W. L., Chang, H.-Y., Levine, D. M., Wang, L., Neale, D., Werner, E. F., & Clark, J. M. (2014). Utilization of primary and obstetric care after medically complicated pregnancies: An analysis of medical claims data. Journal of General Internal Medicine, 29(4), 636–645. https://doi.org/10.1007/s11606-013-2744-2
Boekhorst, M. G. B. M., Muskens, L., Hulsbosch, L. P., Van Deun, K., Bergink, V., Pop, V. J. M., & van den Heuvel, M. I. (2021). The COVID-19 outbreak increases maternal stress during pregnancy, but not the risk for postpartum depression. Archives of Women’s Mental Health. https://doi.org/10.1007/s00737-021-01104-9
Bryant, A. S., Haas, J. S., McElrath, T. F., & McCormick, M. C. (2006). Predictors of compliance with the postpartum visit among women living in healthy start project areas. Maternal and Child Health Journal, 10(6), 511–516. https://doi.org/10.1007/s10995-006-0128-5
Canoy, D., Cairns, B. J., Balkwill, A., Wright, F. L., Khalil, A., Beral, V., Green, J., & Reeves, G. (2016). Hypertension in pregnancy and risk of coronary heart disease and stroke: A prospective study in a large UK cohort. International Journal of Cardiology, 222, 1012–1018. https://doi.org/10.1016/j.ijcard.2016.07.170
CDC Infant Mortality. (2020, September 10). Infant Mortality | Maternal and Infant Health | Reproductive Health | CDC. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/infantmortality.htm
CDC Pregnancy Mortality Surveillance System. (2020, November 25). Pregnancy Mortality Surveillance System | Maternal and Infant Health | CDC. https://www.cdc.gov/reproductivehealth/maternal-mortality/pregnancy-mortality-surveillance-system.htm
Chmielewska, B., Barratt, I., Townsend, R., Kalafat, E., van der Meulen, J., Gurol-Urganci, I., O’Brien, P., Morris, E., Draycott, T., Thangaratinam, S., Le Doare, K., Ladhani, S., von Dadelszen, P., Magee, L., & Khalil, A. (2021). Effects of the COVID-19 pandemic on maternal and perinatal outcomes: A systematic review and meta-analysis. The Lancet Global Health. https://doi.org/10.1016/S2214-109X(21)00079-6
Corbin, J., & Strauss, A. (2008). Basics of qualitative research: Techniques and procedures for developing grounded theory (p. 379). Sage Publications Inc.
Curry, L., & Nunez-Smith, M. (2015). Mixed methods in health sciences research: A practical primer (Vol. 1). Sage publications.
Danilack, V. A., Brousseau, E. C., Paulo, B. A., Matteson, K. A., & Clark, M. A. (2019). Characteristics of women without a postpartum checkup among PRAMS participants, 2009–2011. Maternal and Child Health Journal, 23(7), 903–909. https://doi.org/10.1007/s10995-018-02716-x
Data Haven. (2016). Greater New Haven Community Index 2016. https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwih0o7lgcXxAhVNbs0KHWQWBnkQFjAAegQIBBAD&url=https%3A%2F%2Fwww.ctdatahaven.org%2Fsites%2Fctdatahaven%2Ffiles%2FDataHaven_GNH_Community_Index.pdf&usg=AOvVaw1V5CPRJshN6F6P_ZIapNiO
Daw, J. R., Kolenic, G. E., Dalton, V. K., Zivin, K., Winkelman, T., Kozhimannil, K. B., & Admon, L. K. (2020). Racial and Ethnic Disparities in Perinatal Insurance Coverage. Obstetrics & Gynecology, 135(4), 917–924. https://doi.org/10.1097/AOG.0000000000003728
DeYoung, S. E., & Mangum, M. (2021). Pregnancy, birthing, and postpartum experiences during COVID-19 in the United States. Frontiers in Sociology, 6, 611212. https://doi.org/10.3389/fsoc.2021.611212
Edgerley, L. P., El-Sayed, Y. Y., Druzin, M. L., Kiernan, M., & Daniels, K. I. (2007). Use of a community mobile health van to increase early access to prenatal care. Maternal and Child Health Journal, 11(3), 235–239. https://doi.org/10.1007/s10995-006-0174-z
Fetters, M. D., Curry, L. A., & Creswell, J. W. (2013). Achieving integration in mixed methods designs principles and practices. Health Services Research, 48(6pt2), 2134–2156. https://doi.org/10.1111/1475-6773.12117
Gibson, B. A., Ghosh, D., Morano, J. P., & Altice, F. L. (2014). Accessibility and utilization patterns of a mobile medical clinic among vulnerable populations. Health & Place, 28, 153–166. https://doi.org/10.1016/j.healthplace.2014.04.008
GlazerZeitlin, K. B. J., & Howell, E. A. (2021). Intertwined disparities: Applying the maternal-infant dyad lens to advance perinatal health equity. Seminars in Perinatology. https://doi.org/10.1016/j.semperi.2021.151410
Grandi, S. M., Filion, K. B., Yoon, S., Ayele, H. T., Doyle, C. M., Hutcheon, J. A., Smith, G. N., Gore, G. C., Ray, J. G., Nerenberg, K., & Platt, R. W. (2019). Cardiovascular disease-related morbidity and mortality in women with a history of pregnancy complications. Circulation, 139(8), 1069–1079. https://doi.org/10.1161/CIRCULATIONAHA.118.036748
Hagan, J. F., Shaw, J. S., & Duncan, P. M. (2017). Bright futures: Guidelines for health supervision of infants, children, and adolescents, Pocket guide. American Academy of Pediatrics.
Hager, E. R., Quigg, A. M., Black, M. M., Coleman, S. M., Heeren, T., Rose-Jacobs, R., Cook, J. T., Ettinger de Cuba, S. A., Casey, P. H., Chilton, M., Cutts, D. B., Meyers, A. F., & Frank, D. A. (2010). Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics, 126(1), e26-32. https://doi.org/10.1542/peds.2009-3146
Hendel, K. (2022). The Case For Investment In Mobile Health Care Solutions To Reduce Health Inequities. Health Affairs Forefront. https://doi.org/10.1377/forefront.20220411.842564
Hendrix, C. L., Werchan, D., Lenniger, C., Ablow, J. C., Amstadter, A. B., Austin, A., Babineau, V., Bogat, G. A., Cioffredi, L.-A., Conradt, E., Crowell, S. E., Dumitriu, D., Elliott, A. J., Fifer, W., Firestein, M., Gao, W., Gotlib, I., Graham, A., Gregory, K. D., … Thomason, M. E. (2021). COVID-19 Impacts on perinatal care and maternal mental health: A geotemporal analysis of healthcare disruptions and emotional well-being across the United States (SSRN Scholarly Paper ID 3857679). Social Science Research Network. https://doi.org/10.2139/ssrn.3857679
Hessami, K., Romanelli, C., Chiurazzi, M., & Cozzolino, M. (2020). COVID-19 pandemic and maternal mental health: A systematic review and meta-analysis. The Journal of Maternal-Fetal & Neonatal Medicine: The Official Journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians. https://doi.org/10.1080/14767058.2020.1843155
Howell, E. A., & Zeitlin, J. (2017). Quality of care and disparities in obstetrics. Obstetrics and Gynecology Clinics of North America, 44(1), 13–25. https://doi.org/10.1016/j.ogc.2016.10.002
Institute for Patient and Family Centered Care. (2021). Patient- and Family-Centered Care. https://www.ipfcc.org/about/pfcc.html
Institute of Medicine (US) Committee on Quality of Health Care in America. (2001). Crossing the Quality Chasm: A New Health System for the 21st Century. National Academies Press (US). http://www.ncbi.nlm.nih.gov/books/NBK222274/
Kassebaum, N. J., Bertozzi-Villa, A., Coggeshall, M. S., Shackelford, K. A., Steiner, C., Heuton, K. R., Gonzalez-Medina, D., Barber, R., Huynh, C., Dicker, D., Templin, T., Wolock, T. M., Ozgoren, A. A., Abd-Allah, F., Abera, S. F., Abubakar, I., Achoki, T., Adelekan, A., Ademi, Z., & Lozano, R. (2014). Global, regional, and national levels and causes of maternal mortality during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. The Lancet, 384(9947), 980–1004. https://doi.org/10.1016/S0140-6736(14)60696-6
Keith-Jennings, B., Nchako, C., & Llobrera, J. (2021). Number of Families Struggling to Afford Food Rose Steeply in Pandemic and Remains High, Especially Among Children and Households of Color. Center on Budget and Policy Priorities. https://www.cbpp.org/research/food-assistance/number-of-families-struggling-to-afford-food-rose-steeply-in-pandemic-and
Kinser, P. A., Jallo, N., Amstadter, A. B., Thacker, L. R., Jones, E., Moyer, S., Rider, A., Karjane, N., & Salisbury, A. L. (2021). Depression, Anxiety, Resilience, and Coping: The Experience of Pregnant and New Mothers During the First Few Months of the COVID-19 Pandemic. Journal of Women’s Health. https://doi.org/10.1089/jwh.2020.8866
Lancaster, G. A., & Thabane, L. (2019). Guidelines for reporting non-randomised pilot and feasibility studies. Pilot and Feasibility Studies, 5(1), 114. https://doi.org/10.1186/s40814-019-0499-1
Liu, C. H., Erdei, C., & Mittal, L. (2021). Risk factors for depression, anxiety, and PTSD symptoms in perinatal women during the COVID-19 Pandemic. Psychiatry Research, 295, 113552. https://doi.org/10.1016/j.psychres.2020.113552
Mariño-Narvaez, C., Puertas-Gonzalez, J. A., Romero-Gonzalez, B., & Peralta-Ramirez, M. I. (2021). Giving birth during the COVID-19 pandemic: The impact on birth satisfaction and postpartum depression. International Journal of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics, 153(1), 83–88. https://doi.org/10.1002/ijgo.13565
Martin, J. A., Hamilton, B. E., Osterman, M. J. K., & Driscoll, A. K. (2019). Births: Final data for 2018. National Vital Statistics Reports: From the Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System, 68(13), 1–47.
Mayopoulos, G. A., Ein-Dor, T., Dishy, G. A., Nandru, R., Chan, S. J., Hanley, L. E., Kaimal, A. J., & Dekel, S. (2021). COVID-19 is associated with traumatic childbirth and subsequent mother-infant bonding problems. Journal of Affective Disorders, 282, 122–125. https://doi.org/10.1016/j.jad.2020.12.101
McInerny, T. K., Adam, H. M., Campbell, D. E., DeWitt, T. G., Foy, J. M., & Kamat, D. M. (2016). American Academy of Pediatrics Textbook of Pediatric Care. American Academy of Pediatrics. http://ebookcentral.proquest.com/lib/yale-ebooks/detail.action?docID=4612328
Morano, J. P., Gibson, B. A., & Altice, F. L. (2013a). The burgeoning HIV/HCV syndemic in the urban Northeast: HCV, HIV, and HIV/HCV coinfection in an urban setting. PLoS ONE, 8(5), e64321. https://doi.org/10.1371/journal.pone.0064321
Morano, J. P., Walton, M. R., Zelenev, A., Bruce, R. D., & Altice, F. L. (2013b). Latent tuberculosis infection: Screening and treatment in an urban setting. Journal of Community Health, 38(5), 941–950. https://doi.org/10.1007/s10900-013-9704-y
Morano, J. P., Zelenev, A., Lombard, A., Marcus, R., Gibson, B. A., & Altice, F. L. (2014a). Strategies for hepatitis C testing and linkage to care for vulnerable populations: Point-of-care and standard HCV testing in a mobile medical clinic. Journal of Community Health, 39(5), 922–934. https://doi.org/10.1007/s10900-014-9932-9
Morano, J. P., Zelenev, A., Walton, M. R., Bruce, R. D., & Altice, F. L. (2014b). Latent tuberculosis infection screening in foreign-born populations: A successful mobile clinic outreach model. American Journal of Public Health, 104(8), 1508–1515. https://doi.org/10.2105/AJPH.2014.301897
National Immunization Surveys | CDC. (2021, April 22). https://www.cdc.gov/vaccines/imz-managers/nis/index.html
Nelson, L. M., Simard, J. F., Oluyomi, A., Nava, V., Rosas, L. G., Bondy, M., & Linos, E. (2020). US public concerns about the COVID-19 pandemic from results of a survey given via social media. JAMA Internal Medicine, 180(7), 1020–1022. https://doi.org/10.1001/jamainternmed.2020.1369
NHANES - National Health and Nutrition Examination Survey Homepage. (2021, June 24). https://www.cdc.gov/nchs/nhanes/index.htm
O’Connell, E., Zhang, G., Leguen, F., & Prince, J. (2010). Impact of a mobile van on prenatal care utilization and birth outcomes in Miami-Dade County. Maternal and Child Health Journal, 14(4), 528–534. https://doi.org/10.1007/s10995-009-0496-8
Parikh, N. I., Gonzalez, J. M., Anderson, C. A. M., Judd, S. E., Rexrode, K. M., Hlatky, M. A., Gunderson, E. P., Stuart, J. J., Vaidya, D., Heart, American, American Heart Association Council on Epidemiology and Prevention; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular and Stroke Nursing; and the Stroke Council. (2021). Adverse pregnancy outcomes and cardiovascular disease risk: unique opportunities for cardiovascular disease prevention in women: A scientific statement from the American Heart Association. Circulation, 143(18), e902–e916. https://doi.org/10.1161/CIR.0000000000000961
Petersen, E. E., Davis, N. L., Goodman, D., Cox, S., Syverson, C., Seed, K., Shapiro-Mendoza, C., Callaghan, W. M., & Barfield, W. (2019). Racial/ethnic disparities in pregnancy-related deaths—United States, 2007–2016. Morbidity and Mortality Weekly Report, 68(35), 762–765. https://doi.org/10.15585/mmwr.mm6835a3
Riise, H. K. R., Sulo, G., Tell, G. S., Igland, J., Egeland, G., Nygard, O., Selmer, R., Iversen, A.-C., & Daltveit, A. K. (2019). Hypertensive pregnancy disorders increase the risk of maternal cardiovascular disease after adjustment for cardiovascular risk factors. International Journal of Cardiology, 282, 81–87. https://doi.org/10.1016/j.ijcard.2019.01.097
Silver, D., Blustein, J., & Weitzman, B. C. (2012). Transportation to clinic: Findings from a pilot clinic-based survey of low-income suburbanites. Journal of Immigrant and Minority Health, 14(2), 350–355. https://doi.org/10.1007/s10903-010-9410-0
Silverman, M. E., Burgos, L., Rodriguez, Z. I., Afzal, O., Kalishman, A., Callipari, F., Pena, Y., Gabay, R., & Loudon, H. (2020). Postpartum mood among universally screened high and low socioeconomic status patients during COVID-19 social restrictions in New York City. Scientific Reports, 10(1), 22380. https://doi.org/10.1038/s41598-020-79564-9
Sinaiko, A. D., Szumigalski, K., Eastman, D., & Chien, A. T. (2019). Delivery of patient centered care in the US Health Care System: What is standing in its way. Academy Health. Retrieved October, 30, 2019
Smith, M. V., Kruse, A., Weir, A., & Goldblum, J. (2013). Diaper need and its impact on child health. Pediatrics, 132(2), 253–259. https://doi.org/10.1542/peds.2013-0597
Song, Z., Hill, C., Bennet, J., Vavasis, A., & Oriol, N. E. (2013). Mobile clinic in Massachusetts associated with cost savings from lowering blood pressure and emergency department use. Health Affairs (Project Hope), 32(1), 36–44. https://doi.org/10.1377/hlthaff.2011.1392
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092. https://doi.org/10.1001/archinte.166.10.1092
StataCorp. (2017). Stata Statistical Software: Release 15. StataCorp LLC
Theilen, L. H., Meeks, H., Fraser, A., Esplin, M. S., Smith, K. R., & Varner, M. W. (2018). Long-term mortality risk and life expectancy following recurrent hypertensive disease of pregnancy. American Journal of Obstetrics and Gynecology, 219(1), 107.e1-107.e6. https://doi.org/10.1016/j.ajog.2018.04.002
Tong, A., Sainsbury, P., & Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care, 19(6), 349–357. https://doi.org/10.1093/intqhc/mzm042
US Census Bureau. (2021). American Community Survey (ACS). The United States Census Bureau. https://www.census.gov/programs-surveys/acs
World Health Organization. (2019). Trends in maternal mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. World Health Organization. https://apps.who.int/iris/handle/10665/327595
Yu, S. W. Y., Hill, C., Ricks, M. L., Bennet, J., & Oriol, N. E. (2017). The scope and impact of mobile health clinics in the United States: A literature review. International Journal for Equity in Health. https://doi.org/10.1186/s12939-017-0671-2
Acknowledgements
The authors extend appreciation to the caregivers for their time answering survey and interview questions. They would like to express sincere gratitude to Clifford Bogue MD, the Chair of the Yale Department of Pediatrics, who facilitated the rapid development of the MMC. They are also thankful to the MMC providers and team who provided not only invaluable clinical care and also insights as the analysis process was designed: Sharon Joslin APRN FNP, Angel Ojeda, Migdalia Williams, Taylor Litz MPH, Anna Schairer, Natalie Kil MPH, Michael Turcio, and Rolito Lopez Jr. They also are thankful to the contributions of March of Dimes and American Medical Response for their financial and logistical support. The authors would like to thank the community partnership with support from New Haven Healthy Start, including from Natasha Ray MS. They also would like to express gratitude to Katherine Kohari MD for her support and for support of mothers on the MMC. Finally, the authors would like to thank and honor the memory of Marjorie Rosenthal MD MPH, who helped to conceptualize this project.
Funding
This research was supported by the Yale Pediatric Scholar Program in the Department of Pediatrics at Yale University. The Mobile Medical Clinic was supported by funding from New Haven Healthy Start, March of Dimes, The Community Foundation for Greater New Haven, Yale University Office of New Haven Affairs, the Gilead Foundation, and the Yale New Haven Hospital Medical Staff Fund.
Author information
Authors and Affiliations
Contributions
JR: Conceptualization, Methodology, Validation, Formal Analysis, Investigation, Resources, Data Curation, Writing—Original Draft, Writing—Reviewing and Editing, Visualization. LS: Conceptualization, Methodology, Formal Analysis, Resources, Data Curation, Writing—Reviewing and Editing, Supervision, Funding Acquisition. MB: Methodology, Validation, Formal Analysis, Investigation, Writing—Reviewing and Editing, DLM: Writing—Reviewing and Editing AF: Conceptualization, Methodology, Writing—Reviewing and Editing FLA: Conceptualization, Methodology, Validation, Resources, Writing—Reviewing and Editing, Supervision, Project Administration, Funding Acquisition. MS:Conceptualization, Methodology, Writing—Reviewing and Editing, Supervision.
Corresponding author
Ethics declarations
Conflict of interest
This research was supported by the Yale Pediatric Scholar Program in the Department of Pediatrics at Yale University. The Mobile Medical Clinic was supported by funding from New Haven Healthy Start, March of Dimes, The Community Foundation for Greater New Haven, Yale University Office of New Haven Affairs, the Gilead Foundation, and the Yale New Haven Hospital Medical Staff Fund. Mobile Medical Clinic funders had no role in the study design, collection, analysis, interpretation of data, writing of the report, or decision to submit the report. All authors have declared that they have no conflicts of interest.
Ethical Approval
The study was exempt by the Yale IRB (Study #2000028292, Modification #00035287).
Consent to Participate
All persons gave their verbal informed consent prior to their inclusion in the study.
Consent for Publication
N/A
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Rosenberg, J., Sude, L., Budge, M. et al. Rapid Deployment of a Mobile Medical Clinic During the COVID-19 Pandemic: Assessment of Dyadic Maternal-Child Care. Matern Child Health J 26, 1762–1778 (2022). https://doi.org/10.1007/s10995-022-03483-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10995-022-03483-6