
Abstract
Purpose
Enhancing workplace communication and support processes to enable individuals living with disabilities to sustain employment and return to work is a priority for workers, employers, and community stakeholders. The objective of this study was to evaluate a new resource that addresses support challenges, the Job Demands and Accommodation Planning Tool (JDAPT), and assess its use, relevance, and outcomes over a nine-month follow-up period.
Methods
Workers with physical and mental health/cognitive conditions causing limitations at work were recruited using purposive sampling. Online surveys were administered at baseline (prior to using the JDAPT), and at three and nine months post-baseline. Information was collected on demographics (e.g., age, gender) and work characteristics (e.g., job sector, organization size). Outcomes included assessing JDAPT use and relevance, and changes in self-efficacy, work productivity difficulties, employment concerns, difficulties with job demands, and absenteeism.
Results
Baseline participants were 269 workers (66% women; mean age 41 years) of whom 188 (69.9%) completed all three waves of data collection. Many workers reported using JDAPT strategies at and outside of work, and held positive perceptions of the tool’s usability, relevance, and helpfulness. There were significant improvements (Time 1–2; Time 1–3) in self-efficacy, perceived work productivity, and absenteeism with moderate to large effect sizes in self-efficacy and productivity (0.46 to 0.78). Findings were consistent across gender, age, health condition, and work context variables.
Conclusions
The JDAPT can enhance support provision and provide greater transparency and consistency to workplace disability practices, which is critical to creating more inclusive and accessible employment opportunities.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Research highlights the importance and the challenges associated with providing workplace supports to individuals living with chronic physical and mental health conditions. Challenges include meeting support needs across diverse health conditions and job demands that may cause ongoing or episodic difficulties (i.e., disability) with work. Support needs can vary and be unpredictable, with others often being unaware of a worker’s health condition, changes in their job difficulties or their need for support [1,2,3,4,5,6,7,8,9]. Challenges also include the preference of many workers to maintain privacy and not share personal health information despite needing support to sustain employment. Not wanting to disclose health information is common among workers living with mental health conditions, although workers with physical conditions also report concerns about stigma, gossip, reputational damage, and misuse of health information [3, 10,11,12,13,14,15,16,17,18].
Workers living with chronic and episodic disabling conditions are also more likely to be employed in precarious and lower quality jobs with less access to workplace supports, benefits, or formal accommodations than workers with no chronic health conditions [19,20,21,22]. Even when supports are available, workers with health conditions can report unmet needs or an unwillingness to access supports, particularly formal accommodations [6, 14, 16]. Unmet accommodation needs have been associated with negative workplace outcomes like job disruptions (e.g., missed meetings, arriving late, leaving work early, career interruptions) and productivity losses.
Various measures exist to assess the extent of limitations at work, work ability, health status, and the potential need for resources and supports [23,24,25,26,27]. Tools like the Job Content Questionnaire (JCQ) and Copenhagen Psychosocial Questionnaire (COPSOQ) have been used extensively to assess worker perceptions of the work environment [28, 29]. However, they typically are designed to describe working conditions, and are not aimed at workers or the employment site to help assess individual worker needs or to provide support ideas and solutions relevant to job demands and difficulties. A scan of publicly available self-help resources and supports found that, although some resources existed to help meet needs across a range of conditions (e.g., Job Accommodation Network (JAN)), many were condition or disease-specific and focused largely on managing symptoms [30, 31]. They also tended to provide static (not interactive) information and included limited examples of job demands and informal and formal supports. There are an increasing number of interventions that aim to teach disability self-management principles in the workplace with some providing coaching, education, and skills development to workers and others like supervisors and human resources personnel [8, 32, 33]. However, such interventions are not yet widely available.
The Job Demands and Accommodation Planning Tool (JDAPT)
To address support gaps, we created the Job Demands and Accommodation Planning Tool (JDAPT). Development of the JDAPT drew on existing research, an environmental scan that assessed currently available English-language resources [31], consultations with individuals living with a disability, and community partners. The tool aims to help a worker and/or an organizational representative (e.g., supervisor, human resource professional, disability case manager, occupational health professional, union representative) identify which job demands may be challenging for a worker living with a chronic or episodic health condition (i.e., their functional limitations), and to provide informal and formal self-management and organizational support ideas that are tailored to those areas where difficulties are reported. The JDAPT was developed to be applicable to diverse job types and sectors. By focusing on job demands, the tool was intended to be relevant to a wide range of physical and mental health/cognitive conditions and to enable workplace discussions to be focused on job needs rather than revealing health diagnoses. Suggestions for supports provided within the tool take an integrated health and well-being approach [34] with a range of strategies provided that can be implemented on one’s own or with input from others, and that consider ways to prevent harm, promote individual capacity, and manage personal, social, and environmental challenges.
The JDAPT is designed to be broader than functional workplace assessments that tend to limit their focus to physical (e.g., repetition, load, time spent on tasks) and/or cognitive demands (e.g., memory, problem solving, executive functioning). The tool includes interpersonal work demands and working conditions and provides concrete examples of support strategies tailored to difficulties with specific job demands. Three versions of the tool were created to support a worker’s self-management strategies while also leveraging employer support and accommodation efforts. A worker version allows an individual living with a physical or mental health/cognitive condition experiencing challenges to self-assess their job demands and limitations. A second version can be completed by an organizational representative (e.g., supervisor, disability support caseworker) who is familiar with a worker’s job and their difficulties with specific work demands. It is similar to the JDAPT worker version. The third version does not have a specific worker situation in mind but asks an organization to identify work demands for a job role and links the job demands of that role to different strategies and work support ideas that might make the job more inclusive and accessible to people living with disabilities. All three versions are freely available at https://aced.iwh.on.ca/jdapt.
Evaluation Strategy
Previously, we undertook a formative evaluation with workers and workplace representatives to examine the need for the JDAPT and its perceived utility [35]. Findings showed that comprehensiveness, understandability, relevance, and feasibility exceeded expected thresholds and supported the utility of the tool [35]. The objective of the current study was to examine the worker version of the JDAPT and assess its use and perceived usability, relevance, and outcomes over a nine-month follow-up period (baseline, 3-months post-baseline, 9-months post-baseline) in a sample of workers living with diverse physical and mental health/cognitive conditions and employed in a wide range of jobs.
There is no “gold standard” set of practices or procedures that can be used by workplace organizations to provide support to workers with chronic or episodic health conditions who experience work challenges. Support is often provided both informally by supervisors or colleagues, as well as through a wide range of policies and practices that can involve human resources, disability case managers, union representatives, occupational health professionals, and others. Practices often vary depending on the work challenges experienced by a worker and their condition. The absence of an existing workplace support gold standard and feasibility considerations precluded the use of a randomized control trial design with a standard control group, condition blinding, randomized assignment, and control of health and job factors. For this research, we used an integrated evaluation perspective where we collected detailed information about work context, personal factors, and worker perspectives and used a pre-, post-, follow-up design [36,37,38].
Primary outcomes anticipated from the evaluation included the use of different types of strategies. We hypothesized that the JDAPT would be especially useful to help respondents consider and adopt strategies they could implement on their own in comparison with those that would require explicit permission. We hypothesized significant positive changes in confidence managing work and health needs (i.e., self-efficacy) with greater perceived self-efficacy in problem solving, meeting job demands, and meeting emotional needs post JDAPT use. We also hypothesized significant reductions in presenteeism with fewer perceived work productivity difficulties, as well as less perceived difficulty getting as much work done as others expect, and fewer worries about being unemployed. We expected moderate effect sizes for these changes (e.g., ~ 0.4 to 0.6) and positive comments from participants appraising the tool.
The JDAPT is intended to be part of an existing support process in a workplace. It does not provide treatment recommendations, and the recommended strategies were designed to not substantially alter essential aspects of a worker’s job, create undue hardship, or pose unreasonable difficulties for the employer. Because time taken by workers for health care services would remain important and because essential job tasks remain, we examined changes in absenteeism and perceptions of job demand difficulties as exploratory secondary outcomes. We also examined whether outcomes were similar by gender, age, type of condition, permanent versus contract work, different sized organizations, and union membership. We hypothesized no differences in usage and outcomes related to these latter variables.
Methods
Study Design, Participants, and Procedure
We used an integrated evaluation perspective where we collected detailed information about work context, personal factors, and worker perspectives to understand the use and perceptions of the JDAPT over time [36,37,38]. The study method and measures were registered with Open Science Framework [39] prior to analyses of the longitudinal data.
Study participants were workers who lived with self-reported chronic or episodic physical and/or mental health/cognitive conditions. Eligibility criteria were workers living with a chronic or episodic physical or mental health condition that caused limitations/difficulties at work at least some of the time; paid employment of ≥ 20 h per week; being interested in potentially using or learning about work supports or accommodations to manage health and job needs; being ≥ 18 years of age; and being able to complete an English-language questionnaire. Individuals were excluded if they did not live in Canada; were self-employed; or planned to retire or take an extended leave of absence from work (e.g., parental leave) in the upcoming year. To be able to assess moderate changes over time, power calculations recommended a final sample of 135 participants. We estimated attrition rates of 20% at each wave of data collection and aimed for a baseline sample of 195 participants. Baseline recruitment ran from February to July 2022, at which time we had exceeded our recruitment target.
Eligible participants initially completed an online questionnaire that asked for information about their current job, their health, and perceptions of their ability to manage the impacts of their condition on their work (Time 1 baseline). Within five business days of completing the baseline questionnaire, they were emailed a link to the Job Demands and Accommodation Planning Tool (Time 1 JDAPT). They were asked to complete the JDAPT and answer questions about their initial perceptions of its understandability, relevance, and helpfulness. Three months after completing the JDAPT, participants were sent a follow-up questionnaire that asked about use of any of the JDAPT strategies and perceptions of the JDAPT. The questionnaire also re-asked information about work and health status, and perceptions about the ability to manage one’s condition at work (Time 2, 3-month follow-up). Six months after Time 2, participants were sent a similar questionnaire to the Time 2 questionnaire that again asked about JDAPT use and perceptions, as well as for work and health information, and perceptions of managing one’s health condition at work (Time 3, 9-month follow-up post-baseline). At Times 2 and 3, participants were provided with a link to the JDAPT in case they were interested in completing it again. However, they were not required to do so.
Recruitment
Participants were recruited using a mixture of convenience and purposive sampling to assemble a diverse group of participants. A variety of sources were used to recruit, including websites, workplace contacts established at the Institute for Work & Health, diverse Canadian health charities serving individuals with chronic or episodic conditions, and an existing national panel of Canadians maintained by a survey research firm. Recruitment material informed potential participants that we were interested in learning more about the work experiences of people living with chronic and episodic health conditions and getting their perspectives on an online tool that provided users with support and accommodation ideas. Interested individuals were directed to the baseline questionnaire which began with the screening questions. Interested and eligible participants received an honorarium of CAD$100.00 in three installments after each wave of data collection. Informed consent was obtained from all participants. Ethics approval was received from the University of Toronto Research Ethics Board (#41940).
Job Demands and Accommodation Planning Tool (JDAPT)
The JDAPT asks about 24 job demands in four domains: five physical demands of work (e.g., moving around or working in awkward positions, doing activities that required physical endurance or stamina), six cognitive or “thinking” demands (e.g., paying attention to detail or remembering information, managing time pressures, concentrating for long periods), five demands related to working with others (e.g., supervising others, dealing with the emotions of others), and eight working conditions (e.g., working in extremes of temperature, weather, or other conditions, working in isolated conditions, working in situations where errors could have critical consequences). Users are first asked whether a particular job demand is an important part of their job (Yes/No). If a job demand is relevant to their work, they are asked to rate their ability to perform the job demand (no difficulty, some difficulty, a lot of difficulty), and whether their ability to perform the job demand changes over time because of their health (no, sometimes, often).
After completing the JDAPT questions, the online tool provides users with a summary of their responses to the different job demands questions. For every job demand where they indicate at least some difficulty or some change over time, the tool provides a list of possible support strategies specific to that job demand. Strategies include ways that a job demand might be managed on one’s own without sharing any information at work, techniques or supports that may or may not need permission from others in the workplace, and more formal support and accommodation strategies. Users can save a PDF document of their summary report and all the strategies provided. They also can create a personalized list of supports by selecting the strategies most relevant to them.
The JDAPT does not ask the user for any personal, identifying information. The worker version of the JDAPT can be found at https://aced.iwh.on.ca/jdapt. The tool is freely available in English and French. Users can save a draft of their answers and return to complete the tool on the same device at another more convenient time. However, once a user has submitted their responses and leaves the site, their answers are not saved by the website and are deleted. Users can consult the PDF they saved for their responses or re-complete the JDAPT at any time. The JDAPT became available to the public on March 31, 2023. As of April 30, 2024, more than 10,500 users had accessed the tool from Canada and internationally.
Measures
Primary Outcomes
At Time 1, after completing the JDAPT, we asked participants whether the JDAPT was easy to understand, easy to complete, relevant to their job demands, and whether the examples were helpful. Responses were on a three-point scale where 1 = not at all; 2 = somewhat; 3 = extremely. Participants were also asked whether the JDAPT took too long to complete (No/Yes) and whether they were able to complete the tool on their own without help from others (No/Yes). Based on our previous research, we hoped that at least 70% of participants would report that the JDAPT was somewhat or extremely easy to understand, complete, and relevant to their job and that fewer than 10% would report the tool was too long or that they needed help completing it [35].
JDAPT Use
At Time 2 (3-months post-baseline) and Time 3 (9-months post-baseline), we asked participants whether they used the JDAPT either in the past 3 months (Time 2) or in the past 6 months (Time 3), “Have you made any changes to the way you do your job tasks or relied on any supports or accommodations at work to help you manage your health needs and remain productive at your job” on a 5-point scale (1 = not at all; 5 = to a very large extent). Respondents who answered that they had not made any changes were asked to provide reason(s) from a list where they could check as many that applied. Six reasons were given plus an “Other” category where a respondent could provide their own reason. Example reasons included health not impacting one’s job, already having ways to manage health and job demands and not needing anything new, being concerned about negative work repercussions, and not finding any JDAPT suggestions that fit with one’s job. Participants were also asked whether they had used the JDAPT strategies to make changes outside of work (No/Yes), make changes at their job (No/Yes), and whether they had shared JDAPT tool information with others (No/Yes). Because the nature of episodic health conditions means that individuals may not always need to use supports, we expected that about two thirds of respondents would report using the JDAPT with most changes being outside of work.
Self-efficacy
At baseline (prior to viewing the JDAPT) and at Times 2 and 3, participants were asked 21 questions about their perceived confidence (i.e., self-efficacy) in managing the impact of their health on their job. Self-efficacy is a key concept in intervention and behavior change theory. Research finds that it is a precursor to sustained behavior change [40, 41]. Items were adapted from return-to-work self-efficacy measures aimed at physical or psychological injuries [42,43,44,45]. The items underwent exploratory factor analysis (see Analyses section). Items had the stem, “Thinking about my current work and health needs, I am confident that I can…”. Three underlying dimensions were identified with factor analyses that included 20 of the 21 items. Internal consistency of the three factors as measured with Cronbach’s alphas was excellent. Nine items measured self-efficacy in problem solving (e.g., “Explain to others the parts of my job that are most challenging for me due to my health condition,” “Suggest to my supervisor ways to change my work to help manage my health condition”; Cronbach’s alpha = 0.88). Six items measured self-efficacy in meeting job demands (e.g., “Meet my job demands,” “Keep up with the pace of work”; Cronbach’s alpha = 0.88). Five items assessed self-efficacy in addressing emotional demands (e.g., “Cope with work pressures,” “Deal with emotionally demanding situations”; Cronbach’s alpha = 0.81). Responses were on a 5-point scale from 1 = strongly disagree to 5 = strongly agree.
Work Productivity and Concerns About Employment
A single item from the work productivity and activity impairment instrument (WPAI) asked about the impact of respondent’s health and disability on their work productivity [46]. The WPAI has been used extensively in health studies examining the impact of disability on employment. The baseline and Time 3 questionnaires asked about productivity in the previous six months, and the Time 2 follow-up asked about productivity in the previous three months. Responses were on a scale from 0 to 10 with higher scores indicating greater productivity problems and limitations. Participants were also asked about difficulty getting as much work completed as others expect (i.e., “Because of your health, are you having difficulty getting as much work done as others expect of you?”) with responses on a scale from 1 = not at all to 5 = to a very large extent. Concerns about employment were assessed with the item, “Are you worried about becoming unemployed?” with responses on a scale from 1 = not at all to 5 = to a very large extent.
Secondary Outcomes
Respondents were asked four questions about whether, in the past three (Time 2) or six months (Time 3), they had difficulties with the physical demands of their job, cognitive or “thinking” demands of their job, working with others, and working conditions. Responses were on a three-point scale with 1 = no difficulty; 2 = some difficulty; 3 = a lot of difficulty. Participants were asked in the past 6 months, how many days in total they were absent from work related to their health or a disability, including time off because of appointments. The question was asked at Time 1 (baseline) and Time 3.
Demographic and Work Context Information
Participants were asked, “How do you self-identify in terms of gender?” (Man, Woman, I do not identify within the gender binary, I identify as [open text]). They were also asked for their age in years, highest level of education received (categories collapsed into high school or less; apprenticeship/college/university certificate or diploma; university degree; post graduate degree), and for their marital status (categories collapsed into married/living as married; divorced, separated, widowed; never married/single).
Type of health condition was assessed with three questions, “Do you have an ongoing [physical health condition; mental health or cognitive condition; any other on-going health problem or long-term condition] that has made working difficult at least some of the time during the past 3 months? (No/Yes). Examples of different types of conditions were provided in the questions. Answers were coded into three groups: physical, mental/cognitive, or both physical and mental/cognitive disability. If a condition was present, respondents were asked, “how often has your [physical, mental/cognitive, other] health condition made working difficult in the past three months (1 = sometimes; 2 = often; 3 = always). Questions were adapted from the short disability screening questionnaire (DSQ) used by Statistics Canada [47]. Respondents were also asked, “Do you ever have periods of one month or more when you do not feel limited in your job activities due to your health condition?” (No/Yes) and “Is your ability to do your daily activities [getting better, getting worse, staying about the same, you are able to do more activities during some periods but fewer activities during other periods].” These two questions were used to create four types of dynamic disability as outlined by Statistics Canada [48]. They were individuals reporting a constant level of disability, recurrent disability, progressive disability, and fluctuating level of disability. A single item asked respondents, “Compared to other people your age, how would you rate your health” (1 = poor, 2 = fair, 3 = good, 4 = very good, 5 = excellent).
Participants were asked if they were working full- or part-time, whether they had a permanent or time-limited contract position, and the sector in which they worked from a list of 20 options with an additional write-in category (“other”). They were also asked whether they belonged to a union or a professional/managerial society at their place of employment that acted as a bargaining unit (No/Yes), the size of their organization (collapsed into less than 100 employees, 100–500 employees, more than 500 employees), and their work location (mostly or entirely from home, combined home and workplace, mostly or entirely at their workplace). A single item asked, “in general, how much overall control do you have over your work activities and work-related matters” (1 = not at all; 5 = a great deal).
Analyses
The distributions of all variables were examined for normality. Correlations among variables were examined for multicollinearity. Variable frequencies, means, and standard deviations (SDs) described the sample and JDAPT item responses. Exploratory factor analyses were conducted using the 21 self-efficacy items and orthogonal and oblique rotations to examine whether patterns of relationships existed and whether items could be reduced into a smaller set of dimensions. A factor loading of ≥ 0.4 was used as an acceptable loading for an item on a factor. A three-factor solution was selected based on factor loadings and eigenvalues. One item did not load on any factor and was omitted from analyses.
Using data from the 269 participants at Time 1, logistic regression examined the likelihood of dropping out of the study and compared the sample characteristics of the 188 respondents who remained in the study with the 81 participants who dropped out at either Time 2 or Time 3. General linear regression models examined primary and secondary outcome changes at the three waves of data collection. Contrasts examined Time 1 with Time 2, Time 1 with Time 3, and Time 2 with Time 3. We expected significant changes (i.e., improvements) from Time 1 to Time 2 and from Time 1 to Time 3. We did not expect significant changes (i.e., improvements or decreases) from Time 2 to Time 3 but anticipated that Time 2 changes would be maintained over time. For contrasts that were significant, we calculated effect sizes between Time 1 and Time 2 to assess the meaningfulness of the change in the outcome in addition to its statistical significance [49]. In general, effect sizes of 0.2 are considered small, 0.5 is considered moderate, and 0.8 or above is considered large. We also conducted exploratory analyses to assess whether there were differences in the use of the JDAPT strategies, as well as in our primary and secondary outcomes. T-tests examined differences in gender, permanent versus contract work and union membership and ANOVA’s examined differences in age categories, type of health condition, and organizational size. Given the large number of tests for these analyses (36 tests for our primary outcomes and 24 tests for our secondary outcomes), we would expect three to four tests to be significant by chance. We treated these analyses as exploratory and adopted a conservative significance level of p < 0.01.
Results
Recruitment yielded 444 individuals interested in the research (see Fig. 1). Of them, 175 (39.4%) did not meet eligibility criteria. Those excluded mostly lived outside of Canada, were not employed, were self-employed, or worked fewer than 20 h per week. The remaining 269 individuals met study eligibility and completed the Time 1 baseline questionnaire, the JDAPT, and the JDAPT assessment questions. At Time 2, 210 of the Time 1 baseline participants completed the 3-month follow-up questionnaire (78.0%). At Time 3, 188 respondents completed the 9-month follow-up questionnaire (89.5% of Time 2 respondents; 69.9% of Time 1 baseline respondents).

Recruitment flow chart of participants at each wave of data collection
Table 1 presents sample characteristics. At baseline, two thirds of participants were women (66.2%). Participants ranged in age from 19 to 70 years with a median age of 41 years. Most participants had a university degree. Over half the sample lived with both a physical and mental health condition (55.8%), and most participants reported a recurrent disability (45.3%) with periods of a month or more with few if any limitations. Another 16% of respondents reported a progressive condition, 18.6% said their condition fluctuated, and 20.1% reported a constant disability. Example conditions reported by participants included depression, anxiety, multiple sclerosis, inflammatory bowel disease, arthritis, and other musculoskeletal conditions, chronic pain, migraines, ADHD, respiratory disorders, and neurodiversity. Most participants worked full-time (90.7%) with 16.4% reporting contract work. Participants worked in a range of sectors with 23.8% working in sales, services, retail and hospitality or construction, utilities, agriculture, or manufacturing. The remainder of respondents were in education, health, sciences arts and professions (42.4%) or financial, insurance, business, technology or government (33.8%). Nearly a third of participants belonged to a union, 37.2% worked in an organization of fewer than 100 employees with 44.6% working in organizations of over 500 workers. About 43% of workers reported working mostly or entirely at their workplace with 40.1% reporting working mostly from home. Participants mostly reported moderate job control. On average, participants reported being absent 6.6 days in the previous 6 months.
We examined differences between those who remained in the study at all three waves (n = 188) compared to those who dropped out at either Time 2 or Time 3 (n = 81). There were few differences. However, those who dropped out were more likely to report living with both a physical and mental health/cognitive condition, have a progressive disability, or be working in a contract job.
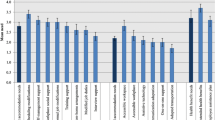
Table 2 presents frequencies for the different job demands in the JDAPT. Job demands that were endorsed most frequently by participants (i.e., ≥ 80%) were cognitive demands of working (all percentages greater than 85%), working with one’s hands (84.4%) and communicating, negotiating, or motivating others (85.1%). Job demands endorsed as an important part of work by the fewest respondents were working in locations with no easy access to facilities to meet one’s needs (17.2%), working in extremes of temperature or weather (16.0%), and working with hazardous equipment or situations (15.0%).
Although working in locations with no easy access to facilities to meet one’s needs was not a common job demand among participants, it was considered among the most difficult activities (some/a lot) for those whose jobs include it (93.5%). Also difficult were activities that required physical endurance or stamina (85.1%) and concentrating for long periods of time (80.7%) (see Table 2). Activities where most respondents reported their difficulties as changing because of their health (sometimes/often) were job demands that required physical endurance or stamina (88.1%), concentrating for long periods of time (85.8%), moving around or working in awkward positions or postures (83.9%), taking part in social activities or social expectations (83.3%) and paying attention to detail or remembering information (82.9%).
As expected, most participants reported that the JDAPT was extremely easy to understand (83.6%), extremely easy to complete (83.6%), and was a tool they were able to complete on their own (99.6%). Only 2.6% of respondents reported that it took too long to complete. Most participants reported that the examples were extremely relevant to their job (not at all relevant = 1.1%; somewhat relevant = 41.3%; extremely relevant = 67.6%) and were extremely helpful (not at all helpful = 1.1%; somewhat helpful = 29.7%; extremely helpful = 69.1%). At Times 2 and 3, participants were asked if they used the JDAPT strategies and support ideas to make changes to managing their health and job outside of work, at work, and whether they shared the JDAPT tool with others. As expected, more participants reported using the JDAPT strategies to make changes outside of work (Time 2: 72.9%; Time 3: 70.4%), although many respondents also used the JDAPT at work (Time 2: 59.0%; Time 3: 42.8%). Among participants who reported not making any changes or relying on any supports or accommodations (Time 2 = 17.4%; Time 3 = 12.6%), most reported that their health did not currently impact their job (Time 2 = 40%, Time 3 = 45.5%), that they were already using different strategies and they did not need anything new (Time 2 = 48.6%; Time 3 = 45.5%), or that they were concerned about negative repercussions at work if they requested changes (Time 2 = 25.7%; Time 3 = 18.2%). Participants also were asked whether they had shared tool information with others at their workplace. At Time 2, 21.4% of participants had shared information from the JDAPT and at Time 3, 23.6% of participants had shared information. We examined potential differences in reported use of the JDAPT by gender, age, type of health condition, having a permanent versus contract position, union membership or organization size at the end of the study (Time 3). Because of the large number of comparisons, a p value of 0.01 was used. No significant differences were found in use of the JDAPT strategies outside of work, at work, or in sharing JDAPT information with others.
Participants provided a range of comments about the JDAPT (see Table 3). Most comments were positive with negative perceptions being largely about barriers in the workplace and not the JDAPT itself. For example, two participants commented
“I used the list of strategies and accommodations, plus the language of the job demands summary, to help me request a workplace accommodations plan. These tools were critical in helping me explain how my disability impacts my work and allowed me to think about possible solutions or accommodations to implement…. Without the JDAPT, I wouldn't have had the confidence to go through this (intimidating) process and advocate for myself in such an effective way!”
(communications manager with anxiety and depression)
“I learned that all my difficulties depended on my state of health, with me not needing much, if any, accommodation when [I am] well, and progressively more if [I am] in a flare of illness. In the strategies, I found the range of accommodations listing things we can do on our own to requesting a formal accommodation, to be helpful. It was empowering to see how much one can do on one's own, especially when I'm hesitant about being supported by HR.”
(social worker with fibromyalgia and mental health needs)
Comments indicated that participants used the tool in various ways, including to isolate the components of a job that were difficult, identify and use strategies on one’s own, be more proactive in self-managing difficulties, share information and plan with others, and to monitor changes over time.
Table 4 presents the findings from the generalized linear models testing differences in the primary and secondary outcomes between Time 1 and Time 2, Time 1 and Time 3, and Time 2 and Time 3. As hypothesized, significant improvements were found between Time 1 and Time 2, and between Time 1 and Time 3 for all primary outcomes and several secondary outcomes (most p’s < 0.001). No significant differences were found between Time 2 and Time 3 contrasts except for a decrease in self-efficacy scores in meeting emotional needs (p < 0.02), suggesting that participants largely maintained the improvements they reported at Time 2 over the six months to Time 3. Specifically, respondents reported significant increases in self-efficacy for problem solving, meeting job demands, and meeting their emotional needs at Times 2 and 3 compared to Time 1 (baseline). They also reported significantly fewer difficulties getting as much work done as others expected, fewer work productivity difficulties, and were significantly less worried about being unemployed.
Difficulties with job demands also showed changes over time (see Table 4). There were significant decreases in reports of difficulties with physical demands from Time 1 to Time 3 and decreases in reports of difficulties with cognitive work demands and working with others from Time 1 to Time 2 and Time 1 to Time 3. There were no changes in reports of difficulties with working conditions. We also found a reduction in days absent reported over the previous six months from Time 1 to Time 3, p < 0.007.
We calculated effect sizes between Time 1 and Time 2 to examine the meaningfulness of changes in the primary and secondary outcomes [49] (see Table 4). Effect sizes for changes in self-efficacy, difficulty getting as much work done as others expect, and work productivity difficulties were moderate to large (range 0.46–0.78), suggesting that, in addition to being statistically significant, the changes were meaningful at a practical level. Effect sizes for changes in worries about becoming unemployed (0.30), and secondary outcomes of absenteeism (0.27) and difficulty with work activities (0.32–0.37) were smaller, suggesting that, although statistically significant, these changes may have had less practical impact.
Finally, we examined whether, at the completion of the study (Time 3), there were differences in the primary and secondary outcomes by gender, age, type of health condition, having a permanent versus contract position, union membership, or organization size. With one exception, no differences were found in the primary outcomes suggesting that the JDAPT changes were similar across different groups and variables. Being a member of a union was associated with poorer self-efficacy for problem solving (p < 0.01) and meeting emotional needs (p < 0.006) at Time 3 compared to not being a member of a union. In addition, few differences were found in secondary outcomes using p < 0.01 to explore findings. Participants with both a physical and mental health condition reported greater work productivity difficulties at Time 3 than either those with a physical disability alone or a mental health/cognitive disability alone (p < 0.002). Those with a mental health/cognitive disability alone or in combination with a physical disability also reported greater difficulties with the cognitive demands of work at Time 3 compared to those with physical difficulties alone (p < 0.001). Finally, participants working in moderate-sized organizations (100 to 500 individuals) reported more difficulty with the physical demands of work at Time 3 than those in smaller organizations (< 100 workers) or larger organizations (> 500 workers) (p < 0.007).
Discussion
Enhancing workplace communication and support processes to better enable individuals living with disabilities to sustain employment and return to work is a priority for workers, employers, and community partners. We examined the use and perceptions of an online, interactive resource, the Job Demands and Accommodation Planning Tool (JDAPT). We examined changes in workers perceived self-efficacy, presenteeism, job difficulties, and absenteeism at 3- and 9-months post introduction to the JDAPT. Overall, findings were positive with many workers reporting that they used JDAPT strategies at work and outside of work, especially strategies that could be implemented without formal workplace intervention. Participants also reported positive perceptions of the tool’s ease of use, relevance and helpfulness, and significant improvements in confidence managing health and work needs, perceived work productivity, and absenteeism. The findings were largely similar for women and men, different age groups, individuals living with physical and/or mental health/cognitive conditions, as well as across a range of job characteristics. These results are promising not only for workers, but also for organizational representatives and health professionals who manage provision of support. They suggest that the JDAPT may have wide applicability across a range of health conditions and job types, that it can help identify components of a job which are difficult, and that it can enhance existing workplace support strategies. This is useful to proactively address areas of workplace need, and to monitor changes in health at work for potential intervention over time.
Results from the JDAPT identified diverse job demands that were rated as difficult by participants. Among the consistently most difficult job demands were those where there was no easy access to facilities to meet personal needs, concentrating for long periods of time at work, and where physical endurance or stamina was important. Concentration difficulties can result from a wide range of physical and mental health conditions, especially where there are symptoms like fatigue, anxiety, or pain. Difficulties with physical endurance or stamina are commonly reported with physical conditions, but also can be present with mental health conditions. Less attention has been given to job difficulties arising from a lack of easy access to facilities to meet personal needs. Difficulties can include not having a place to store medication (e.g., no refrigeration), no private space to remove oneself from others, and no easy access to a toilet. Outdoor jobs, jobs where a worker moves around to different locations, and working in a kiosk in a public place (e.g., shopping center) are examples of types of work where access to facilities to meet personal needs are limited. Moving forward, additional research needs to be undertaken that focuses on identifying work that can be more difficult to accommodate with a goal of finding additional ways to meet support needs, as well as research on experiences with hybrid work.
The JDAPT results also showed that many respondents reported their difficulties at work varied over time and were not constant. This was especially true of cognitive job demands. This variability may relate to changing symptoms like fatigue and pain, but also may relate to factors like workload and changing job expectations. Despite internationally accepted definitions of disability that emphasize social and environmental components contributing to disability in addition to health, there remains a tendency to characterize disability as a permanent attribute of a person, focusing less on the contribution of context like workplace factors or episodic limitations [50]. The JDAPT’s ability to capture not only job demands but also changes in limitations may help workplaces to better appreciate the diverse contributors to disability, monitor workplace limitations over time and focus more on workplace supports to minimize work problems. At the same time, greater recognition is needed in research and practice to recognize the episodic and changing nature of disability.
The findings also point to the need for additional research to examine the timing of support, which may be more effective if undertaken proactively (e.g., regular breaks, regularly alternating tasks) and not in response to an unfolding crisis where support strategies may be less beneficial. This is challenging because research indicates that workers often delay sharing information so as not to draw attention to their difficulties and to avoid potential gossip or stigma [10,11,12,13,14,15, 17, 18]. Potential negative consequences of delays to sharing information have not been well studied. However, some research finds that not sharing information can be associated with disability being mislabeled as a performance problem, poor motivation, or poor interpersonal skills [3, 16].
Most participants reported that the JDAPT was easy to complete, relevant to their job, and extremely helpful. Many participants preferred to draw on strategies outside of their job or that they could use on their own without permission, rather than share their needs or the JDAPT with others in the workplace. This is in keeping with previous research on disclosure [3, 10,11,12,13,14,15,16,17,18]. Although much of this research uses qualitative methods, surveys find that anywhere from about a quarter to half of individuals living with a chronic health condition have not disclosed any health information to a supervisor and can be concerned about reputational damage, stigma, and job loss [10, 15, 16]. Our finding that nearly one quarter of participants had shared the JDAPT itself with their employer suggests that, for some participants, the tool may be a way to help focus a conversation about support needs and enhance disclosure. Open-ended comments were also largely positive and suggested that participants varied considerably in how they applied the tool, including using it on their own, as a proactive resource to avoid problems, and to consider ways to address current or potential future challenges. Problems implementing the tool pointed less to the JDAPT and more to barriers within a workplace, especially at the supervisor and manager level. Additional research on implementation facilitators and barriers is needed to better understand how resources like the JDAPT may be adopted by organizations.
Improvements included positive changes to self-efficacy and presenteeism, as well as decreased reports of absenteeism and less difficulty with job demands. Across primary outcomes, improvements were significant at three months and were sustained at nine months without a significant decline. Effect sizes were moderate to large, suggesting potentially meaningful differences. Self-efficacy changes are important as they have been identified as a significant predictor of behavior change [40]. Although additional research is needed, it is unlikely that improvements in self-efficacy are due to natural increases in confidence in managing a condition when a worker returns to work from an absence, as all participants remained working throughout the study, and most were employed at the same job in the year prior to the research. Although the JDAPT does not change the essential components of a worker’s job or provide health treatment advice, there were reports of significantly fewer difficulties with physical job demands at three months and cognitive job demands and working with others at three and nine months. However, as expected, effect sizes were smaller than for primary outcomes. There were no differences in difficulty reported with working conditions (e.g., working in extremes of temperature weather, being at work at specific times) which may indicate that many of these were considered essential components of a worker’s job that are less amenable to change. Also noteworthy was that changes in primary and secondary outcomes were largely similar across gender, age, type of health condition, permanent versus contract work, union membership, and organization size, suggesting the tool was helpful for a range of groups. Although self-management strategies can be found for many health conditions, currently there is a dearth of tools addressing workplace support needs that are linked to diverse job demands. The findings from this study are encouraging. It is possible that some changes were related to episodic variations in health symptoms. However, comments from participants suggested that this did not explain the significant changes over time with numerous participants noting the benefits of the tool in giving them new strategies and greater control or confidence in managing their condition at work. At the same time, the findings need to be replicated in additional samples with longer periods of follow-up and comparing those who have and have not used the JDAPT.
There are several limitations to this research that need to be acknowledged. Like other intervention studies, individuals who are more interested or motivated to change may be more willing to participate, which could result in some bias in the sample. Although we tested the JDAPT in a sample of respondents with diverse characteristics and maintained about 70% of participants in the study across nine months, individuals living with both a physical and mental health condition, whose disability was progressive, and who worked contract jobs were more likely to drop out of the study. We also had fewer respondents working part-time, in contract jobs, in occupational sectors like sales and service, construction, or other primary industries. Additional testing with the JDAPT is needed to examine its efficacy with different health conditions and occupational types and sectors. Participants in the study also had disproportionately higher levels of education compared with the Canadian population. Some evidence suggests that young adults with disabilities seek higher levels of education to attempt to improve their employment prospects and their ability to sustain work [51]. However, additional research with the JDAPT among individuals with less education and poorer literacy skills is needed. We also need research into diverse outcomes, with longer follow-up times to examine how participants use the JDAPT over time and whether some types of strategies are considered more helpful than others, and implementation research that tests the organizational versions of the tool.
Conclusions
This study found promising outcomes for the JDAPT—a new tool aimed at helping individuals with chronic and episodic physical and mental health conditions identify areas of job difficulty and potential strategies to help sustain or return to work. Increasing numbers of people are working with diverse health conditions and personal needs that can cause periods of disability. Workers and organizational representatives can find it challenging to identify and discuss workplace support and accommodations. The JDAPT has the potential to enhance support provision and provide greater transparency and consistency to workplace disability practices. Improving the support provided to people living with chronic and episodic physical and mental health conditions is critical to create more inclusive and accessible employment opportunities and to sustain long-term employment goals.
Data Availability
Access to data may be requested from the corresponding author and is held at the Institute for Work & Health, Toronto, Canada.
References
Bastien M-F, Corbière M. Return-to-work following depression: what work accommodations do employers and human resources directors put in place? J Occup Rehabil. 2019;29:423–432.
Cheng L, Jetha A, Cordeaux E, Lee K, Gignac MAM. Workplace challenges, supports, and accommodations for people with inflammatory bowel disease: a scoping review. Disabil Rehabil. 2022;44(24):7587–7599.
Gignac MAM, Bowring J, Jetha A, Beaton DE, Breslin FC, Franche R-L, et al. Disclosure, privacy and workplace accommodation of episodic disabilities: organizational perspectives on disability communication-support processes to sustain employment. J Occup Rehabil. 2021;31(1):153–165.
Gignac MAM, Kristman V, Smith PM, Beaton DE, Badley EM, Ibrahim S, et al. Are there differences in workplace accommodation needs, use and unmet needs among older workers with arthritis, diabetes and no chronic conditions? Examining the role of health and work context. Work Aging Retire. 2018;4(4):381–398.
Gignac MAM, Cao X, McAlpine J. Availability, need for, and use of work accommodations and benefits: are they related to employment outcomes in people with arthritis? Arthritis Care Res (Hoboken). 2015;67(6):855–864.
Jessiman-Perreault G, Gignac MA, Thompson A, Smith PM. Understanding the unmet accommodation needs of people working with mental or cognitive conditions: the importance of gender, gendered work, and employment factors. J Occup Rehabil. 2024;34:251–264.
Padkapayeva K, Posen A, Yazdani A, Buettgen A, Mahood Q, Tompa E. Workplace accommodations for persons with physical disabilities: evidence synthesis of the peer-reviewed literature. Disabil Rehabil. 2017;39(21):2134–2147.
Shaw WS, McLellan RK, Besen E, Namazi S, Nicholas MK, Dugan AG, et al. A worksite self-management program for workers with chronic health conditions improves worker engagement and retention, but not workplace function. J Occup Rehabil. 2022;32(1):77–86.
Wynne-Jones G, Buck R, Porteous C, Cooper L, Button LA, Main CJ, et al. What happens to work if you’re unwell? Beliefs and attitudes of managers and employees with musculoskeletal pain in a public sector setting. J Occup Rehabil. 2011;21(1):31–42.
Bogaers R, Geuze E, van Weeghel J, Leijten F, van de Mheen D, Greenberg N, et al. Mental health issues and illness and substance use disorder (non-) disclosure to a supervisor: a cross-sectional study on beliefs, attitudes and needs of military personnel. BMJ Open. 2023;13(4): e063125.
Brohan E, Henderson C, Wheat K, Malcolm E, Clement S, Barley EA, et al. Systematic review of beliefs, behaviours and influencing factors associated with disclosure of a mental health problem in the workplace. BMC Psychiatry. 2012;12(11):1–14.
Brouwers EP. Social stigma is an underestimated contributing factor to unemployment in people with mental illness or mental health issues: position paper and future directions. BMC Psychol. 2020;8:36.
Brouwers EPM, Joosen MCW, van Zelst C, Van Weeghel J. To disclose or not to disclose: a multi-stakeholder focus group study on mental health issues in the work environment. J Occup Rehabil. 2020;30(1):84–92.
Gignac MA, Bowring J, Shahidi FV, Kristman V, Cameron JI, Jetha A. Workplace disclosure decisions of older workers wanting to remain employed: a qualitative study of factors considered when contemplating revealing or concealing support needs. Work Aging Retire. 2024;10(2):174–187.
Gignac MA, Cao X. “Should I tell my employer and coworkers I have arthritis?” A longitudinal examination of self-disclosure in the work place. Arthritis Care Res (Hoboken). 2009;61(12):1753–1761.
Gignac MAM, Jetha A, Martin Ginis KA, Ibrahim S. Does it matter what your reasons are when deciding to disclose (or not disclose) a disability at work? The association of workers’ approach and avoidance goals with perceived positive and negative workplace outcomes. J Occup Rehabil. 2021;31(3):638–651.
Jones KP, King EB. Managing concealable stigmas at work: a review and multilevel model. J Manag. 2014;40(5):1466–1494.
Toth KE, Yvon F, Villotti P, Lecomte T, Lachance J-P, Kirsh B, et al. Disclosure dilemmas: how people with a mental health condition perceive and manage disclosure at work. Disabil Rehabil. 2022;44(25):7791–801.
Heyman M, Stokes JE, Siperstein GN. Not all jobs are the same: predictors of job quality for adults with intellectual disabilities. J Vocat Rehabil. 2016;44(3):299–306.
LaMontagne AD, Krnjacki L, Milner A, Butterworth P, Kavanagh A. Psychosocial job quality in a national sample of working Australians: a comparison of persons working with versus without disability. SSM Popul Health. 2016;2:175–181.
Shahidi FV, Jetha A, Kristman V, Smith PM, Gignac MA. The employment quality of persons with disabilities: findings from a national survey. J Occup Rehabil. 2023;33(4):785–795.
Tompa E, Scott HM, Trevithick S, Bhattacharyya S. Precarious employment and people with disabilities. In: Vosko LF, editor. Precarious employment: understanding labour market insecurity in Canada. Montreal: McGill-Queen’s University Press; 2006. p. 90–114.
Ilmarinen J. The Work Ability Index (WAI). Occup Med. 2007;57(2):160.
Karasek R, Theorell T. Healthy work: stress, productivity, and reconstruction of working life. New York: Basic Books; 1990.
Lerner D, Amick BC III, Rogers WH, Malspeis S, Bungay K, Cynn D. The work limitations questionnaire. Med Care. 2001;39(1):72–85.
Tang K, Beaton DE, Boonen A, Gignac MAM, Bombardier C. Measures of work disability and productivity: Rheumatoid Arthritis Specific Work Productivity Survey (WPS-RA), Workplace Activity Limitations Scale (WALS), Work Instability Scale for Rheumatoid Arthritis (RA-WIS), Work Limitations Questionnaire (WLQ), and Work Productivity and Activity Impairment Questionnaire (WPAI). Arthritis Care Res (Hoboken). 2011;63(S11):S337–S49.
van den Berg TI, Elders LA, de Zwart BC, Burdorf A. The effects of work-related and individual factors on the Work Ability Index: a systematic review. Occup Environ Med. 2009;66(4):211–220.
Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B. The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol. 1998;3(4):322–355.
Kristensen TS, Hannerz H, Høgh A, Borg V. The Copenhagen Psychosocial Questionnaire-a tool for the assessment and improvement of the psychosocial work environment. Scand J Work Environ Health. 2005;31(6):438–449.
The Job Accommodation Network (JAN). A to Z of disabilities and accommodations. 2021. https://askjan.org/a-to-z.cfm. Accessed 20 Mar 2024
Van Eerd D, Bowring J, Jetha A, Breslin C, Gignac MAM. Online resources supporting workers with chronic episodic disabilities: an environmental scan. Int J Workplace Health Manag. 2021;14(2):129–148.
Carruthers EC, Rogers P, Backman CL, Goldsmith CH, Gignac MA, Marra C, et al. “Employment and arthritis: making it work”. A randomized controlled trial evaluating an online program to help people with inflammatory arthritis maintain employment (study protocol). BMC Med Inform Decis Mak. 2014;14:59.
Janssens K, Joosen M, Henderson C, Bakker M, den Hollander W, van Weeghel J, et al. Effectiveness of a stigma awareness intervention on reemployment of people with mental health issues/mental illness: a cluster randomised controlled trial. J Occup Rehabil. 2024;34(1):87–99.
LaMontagne AD, Shann C, Martin A. Developing an integrated approach to workplace mental health: a hypothetical conversation with a small business owner. Ann Work Expo Health. 2018;62(S1):S93–S100.
Gignac MA, Bowring J, Tonima S, Franche R-L, Thompson A, Jetha A, et al. A sensibility assessment of the Job Demands and Accommodation Planning Tool (JDAPT): a tool to help workers with an episodic disability plan workplace support. J Occup Rehabil. 2023;33(1):145–159.
Chen HT. Practical program evaluation. Thousand Oaks: Sage Publications Inc; 2015.
Chen HT, Rossi PH. The multi-goal, theory-driven approach to evaluation: a model linking basic and applied social science. Soc Forces. 1980;59(1):106–122.
Rossi PH, Lipsey MW, Freeman HE. Evaluation: a systematic approach. 7th ed. Thousand Oaks: Sage Publications; 2004. p. 2004.
Gignac MAM. Job demands and accommodation planning tool: pilot evaluation study. OSF Registries: Center for Open Science; 2023
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215.
Maddux JE. Self-efficacy, adaptation, and adjustment: theory, research, and application. Berlin: Springer; 1995.
Black O, Sim MR, Collie A, Smith P. A return-to-work self-efficacy scale for workers with psychological or musculoskeletal work-related injuries. Qual Quant. 2017;51(1):413–424.
Brouwer S, Franche R-L, Hogg-Johnson S, Lee H, Krause N, Shaw WS. Return-to-work self-efficacy: development and validation of a scale in claimants with musculoskeletal disorders. J Occup Rehabil. 2011;21(2):244–258.
Lagerveld SE, Blonk RW, Brenninkmeijer V, Schaufeli WB. Return to work among employees with mental health problems: development and validation of a self-efficacy questionnaire. Work Stress. 2010;24(4):359–375.
Shaw WS, Reme SE, Linton SJ, Huang Y-H, Pransky G. Development of the return-to-work self-efficacy (RTWSE-19) questionnaire-psychometric properties and predictive validity. Scand J Work Environ Health. 2011;37(2):109–119.
Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365.
Grondin C. A new survey measure of disability: the Disability Screening Questions (DSQ). Canada: Statistics Canada/Statistique Canada; 2016 2016/02/29. Report No.: 0660031558.
Morris S, Fawcett G, Timoney LR, Hughes J. The dynamics of disability: progressive, recurrent or fluctuating limitations. Ottawa: Statistics Canada; 2019.
Kazis LE, Anderson JJ, Meenan RF. Effect sizes for interpreting changes in health status. Med Care. 1989;27(3 Suppl):S178–S189.
World Health Organization. International Classification of Functioning, Disability and Health (ICF). Geneva: World Health Organization; 2001.
Jetha A, Gignac MAM. Changing experiences, needs, and supports across the life course for workers living with disabilities. In: Wahrendorf M, Chandola T, Descatha A, editors. Handbook of life course occupational health. Cham: Springer; 2023. p. 1–22.
Acknowledgements
The authors would like to thank the many partner organizations involved in this research. They are the Institute for Work & Health, Arthritis Society Canada, MS Canada, Canadian Mental Health Association, Crohn’s and Colitis Canada, Realize Canada, Mindful Employer Canada, and Workplace Strategies for Mental Health. The Institute for Work & Health operates with the support of the Province of Ontario. The views expressed herein are those of the authors and do not necessarily reflect those of the Province of Ontario. Study registered with Open Science Framework (OSF Registries) prior to longitudinal data analysis. https://doi.org/https://doi.org/10.17605/OSF.IO/GXEQY
Funding
This research was funded by a Healthy and Productive Work (HPW) partnership grant from the Social Sciences and Humanities Research Council of Canada (SSHRC) and the Canadian Institutes of Health Research (CIHR) #890-2016-3002 to the Accommodating and Communicating about Episodic Disabilities (ACED) partnership team. An unrestricted grant also was received from Canada Life. The Institute for Work & Health operates with the support of the Province of Ontario. The views expressed herein are those of the authors and do not necessarily reflect those of the province of Ontario.
Author information
Authors and Affiliations
Contributions
Contributed to development of the tool: All authors; Contributed to study design: All authors; Helped with data collection: MAMG, JB, LN; Contributed to analyses: MAMG, JB, LN, RS, PS; Wrote the main manuscript text: MAMG; Edited and reviewed manuscript: All authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethical Approval
Ethics approval was received from the University of Toronto Research Ethics Board (#41940).
Consent to Participate
Informed consent was obtained from all participants.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gignac, M.A.M., Bowring, J., Navaratnerajah, L. et al. The Job Demands and Accommodation Planning Tool (JDAPT): A Nine-Month Evaluation of Use, Changes in Self-efficacy, Presenteeism, and Absenteeism in Workers with Chronic and Episodic Disabilities. J Occup Rehabil (2024). https://doi.org/10.1007/s10926-024-10231-w
Accepted:
Published:
DOI: https://doi.org/10.1007/s10926-024-10231-w