
Abstract
Purpose
Evaluate benefits and harms of needling therapies (NT) for chronic primary low back pain (CPLBP) in adults to inform a World Health Organization (WHO) standard clinical guideline.
Methods
Electronic databases were searched for randomized controlled trials (RCTs) assessing NT compared with placebo/sham, usual care, or no intervention (comparing interventions where the attributable effect could be isolated). We conducted meta-analyses where indicated and graded the certainty of evidence.
Results
We screened 1831 citations and 109 full text RCTs, yeilding 37 RCTs. The certainty of evidence was low or very low across all included outcomes. There was little or no difference between NT and comparisons across most outcomes; there may be some benefits for certain outcomes. Compared with sham, NT improved health-related quality of life (HRQoL) (physical) (2 RCTs; SMD = 0.20, 95%CI 0.07; 0.32) at 6 months. Compared with no intervention, NT reduced pain at 2 weeks (21 RCTs; MD = − 1.21, 95%CI − 1.50; − 0.92) and 3 months (9 RCTs; MD = − 1.56, 95%CI − 2.80; − 0.95); and reduced functional limitations at 2 weeks (19 RCTs; SMD = − 1.39, 95%CI − 2.00; − 0.77) and 3 months (8 RCTs; SMD = − 0.57, 95%CI − 0.92; − 0.22). In older adults, NT reduced functional limitations at 2 weeks (SMD = − 1.10, 95%CI − 1.71; − 0.48) and 3 months (SMD = − 1.04, 95%CI − 1.66; − 0.43). Compared with usual care, NT reduced pain (MD = − 1.35, 95%CI − 1.86; − 0.84) and functional limitations (MD = − 2.55, 95%CI − 3.70; − 1.40) at 3 months.
Conclusion
Based on low to very low certainty evidence, adults with CPLBP experienced some benefits in pain, functioning, or HRQoL with NT; however, evidence showed little to no differences for other outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Needling therapies are commonly used for the management of pain, including chronic primary low back pain (CPLBP) [1]. These interventions involve inserting fine, solid metallic needles through the skin at specific sites. One type of needling therapy is Traditional Chinese Medicine (TCM) acupuncture, whereby the clinician aims to alter the body’s vital energy qi flows along 12 primary and eight secondary meridians in the body [2]. According to TCM, pain occurs when qi is blocked; however, the proper flow of qi can be restored with the insertion of acupuncture needles at specific points along the meridians [2, 3]. A second type of needling therapy is myofascial acupuncture, or dry needling [4]. It is used to treat myofascial pain by inserting needles (acupuncture needle or other hypodermic needle) into myofascial trigger points and/or tender points. The needles used with both traditional and myofascial acupuncture can be further stimulated manually, with small electrical currents (electroacupuncture), moxibustion (burning the moxa herb at the needle handle), or heat lamps [5]. Various mechanisms have been proposed regarding how needling therapies may help relieve pain. Needle insertion may inhibit the perception of pain via the gate control theory of pain [6]; the release of endogenous opioids [7]; or local physiological and blood flow changes [8, 9].
Mu and colleagues published a Cochrane systematic review (2020) to assess the effects of needling therapies compared to sham intervention, no treatment, or usual care for chronic non-specific LBP (33 randomized controlled trials (RCTs); 8270 participants; search end date of August 2019) [10]. They found that compared with sham, needling therapies may not be more effective in reducing pain or improving back-specific functioning immediately after treatment, or quality of life in the short term. Compared with no treatment, needling therapies were not beneficial for pain relief and functional improvement immediately after treatment. Compared with usual care, needling therapies may improve function, but not pain, immediately after treatment; and did not improve quality of life in the short term. Adverse events related to needling therapies were minor or moderate, and the incidence was similar with sham and usual care. To develop clinical practice recommendations for the management of CPLBP in adults, the World Health Organization (WHO) commissioned the current systematic review to update the evidence and expand the aims of the Cochrane review [10]. The current review aimed to assess additional important outcomes, and subgroups.
The objectives of this systematic review of RCTs were to determine: (1) the benefits and harms (as reported in RCTs) of needling therapies compared with placebo/sham, usual care, or no intervention for the management of CPLBP in adults, including older adults (aged ≥ 60 years); and (2) whether the benefits and harms of needling therapies vary by age, gender/sex, presence of leg pain, race/ethnicity, or national economic development of the countries where the RCTs were conducted.
Methods
This systematic review was conducted as part of a series of reviews to inform the WHO guideline on the management of CPLBP in adults. CPLBP is defined as pain of more than three months duration between the lower costal margin and the gluteal fold with no specific underlying cause. Guideline development was ongoing at the time of submission of this manuscript. The methods are detailed in the methodology article of this series [11].
Briefly, we updated and expanded the scope of the previously published high-quality Cochrane systematic review by Mu et al. [10]. We registered our review protocol with Prospero (CRD42022314824) on 7 March 2022. We searched the Cochrane Central Register of Controlled Trials (Wiley), MEDLINE (Ovid), Embase (Ovid), Cumulative Index to Nursing and Allied Health Literature (CINAHL) (EBSCO), China National Knowledge Infrastructure database (CNKI), WangFang database, and the World Health Organization International Clinical Trials Registry Platform (ICTRP) from the period of 1 August 2019 (end date of previous Cochrane review) to 9 March 2022 (see Online Resource 1). We also searched the reference lists of systematic reviews and included RCTs.
We included RCTs that compared needling therapies to placebo/sham (e.g., sham needling without skin penetration or at non-acupuncture points), usual care, no intervention (including comparison interventions where the attributable effect of needling therapies could be isolated e.g., needling therapy + medication vs. same medication alone) in adults (aged ≥ 20 years) with CPLBP. Eligible needling therapies included those conducted according to TCM theory or myofascial acupuncture methods (i.e., dry needling including neuroreflexotherapy, western medical acupuncture). Specifically, we included interventions where needles were inserted into classical meridian points, tender points, or trigger points through the skin. Manual stimulation, heating by moxa, heat lamps, cupping or electrical current stimulation could be further administered to maximize the treatment effect [10]. We excluded trials that did not use hypodermic needles (e.g., acupressure, laser acupuncture). Further details on the eligibility criteria can be found in the methodology article in this series [11]. In addition to the main critical outcomes requested by the WHO Guideline Development Group (GDG) and assessed for all reviews in this series (pain, function, health-related quality of life (HRQoL), harms/adverse events, psychological functioning, and social participation including work), we also assessed additional critical outcomes requested by the WHO GDG for this review—the change in use of medications and falls in older adults aged ≥ 60 years. These additional outcomes were deemed important for people and their caregivers and had the potential to inform future research. We reported outcomes based on post-intervention follow-up intervals including: (1) immediate term (closest to 2 weeks after the intervention period); (2) short term (closest to 3 months after the intervention period); (3) intermediate term (closest to 6 months after the intervention period); (4) long term (closest to 12 months after the intervention period); and (5) extra-long term (more than 12 months after the intervention period).
We assessed between-group differences to determine the magnitude of the effect of an intervention and to assess its effectiveness [12, 13] (details in the methodology article in this series) [11]. Briefly, we considered a mean difference (MD) of ≥ 10% of the scale range or ≥ 10% difference in risk for dichotomous outcomes to be a minimally important difference (MID) [14, 15]. If the standardized mean difference (SMD) was calculated, SMD ≥ 0.2 was considered a MID [16].
Pairs of reviewers independently screened studies for eligibility, and critically appraised risk of bias (ROB) using the Cochrane ROB 1 tool [17], modified from the Cochrane Back and Neck Methods Guidelines [18]. One reviewer extracted data for all included RCTs, which was then verified by a second reviewer. Any disagreements were resolved by consensus between paired reviewers or with a third reviewer when necessary. Forms and guidance for screening, ROB assessment, and data extraction were adapted from those used by Hayden et al. in the conduct of the ‘exercise for chronic low back pain’ collaborative review, in which members of our team participated [19]. The forms were modified and completed using a web-based electronic systematic review software DistillerSR Inc. [20].
In addition to the main sub-group analyses conducted for all reviews in this series (age, gender/sex, presence of leg pain, race/ethnicity, national economic development of country where RCT was conducted), we conducted the following pre-specified sub-group analyses: needling therapy type (i.e., TCM or myofascial acupuncture), and stimulation used with needling therapies (e.g., electrical, manual, moxibustion). We conducted sensitivity analyses by excluding RCTs judged to have high risk of bias.
We performed random-effects meta-analyses and narrative synthesis where meta-analysis was not appropriate [21], and graded the certainty of evidence using Grading of Recommendations Assessment, Development and Evaluation (GRADE) [22]. Comparisons to no intervention and sets of interventions where the specific attributable effect of needling therapies could be isolated (e.g., needling therapy + treatment B versus treatment B alone) were combined in meta-analyses. Meta-analyses were conducted using R [23, 24]. GRADE Evidence Profiles and GRADE Summary of Findings tables were developed using GRADEpro software [25].
Results
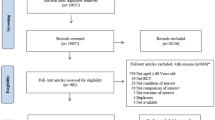
We screened 1831 records and 109 full-text reports (Fig. 1). We identified 16 unpublished RCTs in the WHO ICTRP, of which we contacted the authors who had contact information listed (2 of 16). Both authors responded to inform us that the RCTs were ongoing. Thus, none of the 16 unpublished RCTs identified in the WHO ICTRP were included. We included 37 published RCTs [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] with a total of 7573 adults ranging from 32 to 3093 adults per RCT (see Online Resources 2, 3).

Flow diagram of literature search
The RCTs were conducted in high-income economies [63]: Germany (5 RCTs) [26, 32, 41, 52, 53], Ireland (1 RCT) [34], Korea (2 RCTs) [28, 47], Spain (1 RCT) [39], and the United States (6 RCTs) [27, 36, 40, 55, 62, 64]; upper-middle income economies: Brazil (4 RCTs) [29,30,31, 49] and China (15 RCTs) [33, 37, 38, 37,43,44,45,38, 37,43,44,45,50,38, 54, 37,43,44,45,50,56,38, 37,43,44,45,50,56,59,60,38]; and lower-middle income economies: Iran (3 RCTs) [42, 48, 58]. The mean age ranged from 30 to 72 years; one RCT assessed older adults (n = 55) [40]. The percentage of females within the trials ranged from 0 to 85%. Thirteen of 37 RCTs (35%) were published in a Chinese language.
In 7 RCTs, adults had CPLBP with radicular leg pain [33, 43, 50, 51, 56, 50,59,51]; in 15 RCTs, adults had CPLBP without leg pain [26, 31, 35,36,37,38, 35,36,37,40,38, 47, 49, 53, 35,36,37,40,57,38, 35,36,37,40,57,61,38]; in 3 RCTs, adults had CPLBP either with or without leg pain (radicular or non-radicular) [27, 48, 54]; and presence of leg pain was not reported in 12 RCTs [28,29,30, 32, 34, 39, 42, 28,29,44,45,30, 52, 55]. Where reported by authors, CPLBP duration ranged from 4 months to 15 years.
Most RCTs assessed needling therapies based on TCM (31/37, 84%); while 6 of 37 RCTs (16%) assessed mysofascial acupuncture [26, 36, 39, 42, 48, 62]. Different stimulation types were used. Seven RCTs included electrical stimulation [31, 36, 40, 42, 54, 56, 58], 16 RCTs manual stimulation [26, 28, 34, 35, 38, 41, 34,43,44,45,35, 50, 55, 57, 34,43,44,45,59,35, 62], 2 RCTs moxibustion [44, 61], 1 RCT heated needles [51], and 1 RCT electromagnetic wave therapy device (1 RCT) [60]. The number of sessions delivered ranged from 1 to 40, with the duration of each session ranging from 10 to 45 min. Needling therapies were compared to sham (sham acupuncture or sham electrotherapy [no needles penetrating skin and no electronic stimulation]) (15 RCTs) [26,27,28, 30, 26,27,32,33,34,35,28, 39, 41, 49, 55, 57, 62]; usual care (1 RCT) [27]; no intervention (6 RCTs) [26, 30, 48, 53, 57, 58]; or comparison interventions where the attributable effect of needling therapies could be isolated (20 RCTs) [31, 37, 38, 37,40,41,42,43,38, 37,40,41,42,43,46,38, 37,40,41,42,43,46,50,51,38, 54, 56, 37,40,41,42,43,46,50,51,58,59,60,38, 65].
The outcomes were assessed in the immediate term (31 RCTs) [29, 31,32,33,34, 31,32,33,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,34, 31,32,33,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,54,55,56,57,58,59,60,61,34], short term (19 RCTs) [26,27,28,29,30,31,32,33, 26,27,28,29,30,31,32,35,33, 26,27,28,29,30,31,32,35,39,40,33, 50, 26,27,28,29,30,31,32,35,39,40,52,53,33, 26,27,28,29,30,31,32,35,39,40,52,53,57,33], intermediate term (5 RCTs) [26,27,28, 26,27,32,28], and long term (2 RCTs) [26, 27]. The majority of RCTs assessed pain and function in the immediate and short terms (Table 1). Most of the RCTs (30, 81%) were rated as high overall ROB, five (13.5%) were rated as unclear overall ROB, and two (5.5%) were rated as low overall ROB (see Online Resource 4). The agreement on overall ROB ratings was high (weighted overall kappa score 0.94).
Certainty of Evidence
The certainty of the evidence for all outcomes was low or very low, downgraded due to risk of bias, inconsistency, indirectness, and imprecision of the effect estimates (see Online Resources 5, 6 and 7).
Needling Therapies Versus Sham
All Adults
With low certainty evidence, needling therapies may reduce pain (scale 0 to 10, 0 = no pain) in the immediate term (7 RCTs; MD = − 0.41, 95% CI − 0.72 to − 0.10) (effect estimate did not reach the threshold for a minimally important between-group difference, MD = − 1) (see Online Resource 7, plot 1.1.1) [32, 34, 39, 41, 57, 62, 66]. Needling therapies may make little or no difference to pain in the intermediate (4 RCTs; MD − 0.21, 95% CI − 0.58 to 0.16) (plot 1.1.3) [26,27,28, 32], or long term (2 RCTs; MD = − 0.02, 95% CI − 0.51 to 0.47) (plot 1.1.4) [26, 27]. Due to very low certainty evidence, it is uncertain whether needling therapies make little or no difference to pain in the short term (9 RCTs; MD = − 0.42, 95% CI − 0.88 to 0.05) (plot 1.1.2) [26,27,28, 30, 32, 35, 39, 41, 57].
Due to very low certainty evidence, it is uncertain whether needling therapies make little or no difference to functional limitations (benefit indicated by lower values) in the immediate (4 RCTs; SMD = − 0.22, 95% CI − 0.54 to 0.11) (plot 1.2.1) [32, 39, 57, 62], or intermediate term (4 RCTs; SMD = − 0.10, 95% CI − 0.22 to 0.02) (plot 1.2.3) [26,27,28, 32]. Due to low certainty evidence, needling therapies may make little or no difference to function in the short term (7 RCTs; SMD = − 0.03, 95% CI − 0.17 to 0.11) (plot 1.2.2) [26,27,28, 30, 32, 39, 57].
Due to very low certainty evidence, it is uncertain whether needling therapies make little or no difference to HRQoL (scale 0 to 100, 0 = poor HRQoL, benefit indicated by higher values; PCS: physical component summary, MCS: mental compenent summary) in the immediate term (1 RCT; MD = 6.40, 95% CI − 6.42 to 19.22) (plot 1.3.1) [34]. In the short term, it is uncertain whether needling therapies improve HRQoL (1 RCT; MD = 7.78, 95% CI 1.41 to 14.15) (plot 1.3.2) (effect estimate did not reach the threshold for a minimally important between-group difference, MD = 10) [34], or make little or no difference to HRQoL (PCS) (2 RCTs; SMD = 0.25, 95% CI − 0.07 to 0.56) (plot 1.3.2.1) [26, 32]. In the intermediate term, it is uncertain whether needling therapies make little or no difference to HRQoL (1 RCT; MD = 3.39, 95% CI − 2.98 to 9.76) (plot 1.3.3) [28], or to HRQoL (MCS) (2 RCTs; SMD = 0.10, 95% CI − 0.18 to 0.39) (plot 1.3.3.2) [26, 32]. Due to low certainty evidence, needling therapies may make little or no difference to HRQoL (MCS) in the short term (2 RCTs; SMD = 0.01, 95% CI − 0.12 to 0.14) (plot 1.3.2.2) [26, 32]; and may improve HRQoL (PCS) in the intermediate term (2 RCTs; SMD = 0.20, 95% CI 0.07 to 0.32) (plot 1.3.3.1) [26, 32].
Due to very low certainty evidence, it is uncertain whether needling therapies make little or no difference to depression (scale 0 to 60, benefit indicated by lower values) in the immediate (1 RCT; MD = − 2.50, 95% CI − 5.23 to 0.23) ( plot 1.4.1) [26], short (2 RCTs; SMD = − 0.17, 95% CI − 0.44 to 0.10) (plot 1.4.2) [26, 28], or intermediate term (2 RCTs; SMD = − 0.10, 95% CI − 0.33 to 0.12) (plot 1.4.3) [26, 28].
Due to very low certainty evidence, it is uncertain whether needling therapies make little or no difference to adverse events/harms (6 RCTs; odds ratio (OR) = 1.62, 95% CI 0.67 to 3.90) (plot 1.5) [26, 27, 33, 36, 57, 62].
Older Adults (Aged ≥ 60 years)
Based on one RCT [33] and reported as a narrative synthesis of the authors’ findings (no corresponding plots), there is very low certainty evidence for all outcomes.
It is uncertain whether needling therapy makes little or no difference to: pain (scale 0 to 100, 0 = no pain) in the immediate (MD = − 6.85, 95% CI − 16.82 to 3.11), short (MD = − 6.06, 95% CI − 18.50 to 6.38), or intermediate term (MD = − 7.01, 95% CI − 17.50 to 3.48); function (scale 0 to 100, 0 = no disability) in the immediate (MD = − 4.52, 95% CI − 13.05 to 4.01), short (MD = − 3.04, 95% CI − 12.34 to 6.25), or intermediate term (MD = 0.09, 95% CI − 10.80 to 10.98); or HRQoL in the immediate term (effect estimates not provided). Authors reported no serious harms/adverse events occurred during the 4-week RCT; 2 of 46 participants total (4.3%) had subcutaneous hematoma after needling (both from the needling therapy group) [33].
Needling Therapies Versus no Intervention or Comparison Interventions Where the Attributable Effect of Needling Therapies Could be Isolated
All Adults
Due to low certainty evidence, needling therapies may reduce pain (scale 0 to 10, 0 = no pain) in the immediate (21 RCTs; MD = − 1.21, 95% CI − 1.50 to − 0.92) (Fig. 2, Online Resource 7, plot 2.1.1) [31, 37, 38, 37,40,41,42,43,44,45,46,47,38, 37,40,41,42,43,44,45,46,47,50,38, 54, 37,40,41,42,43,44,45,46,47,50,56,57,58,59,60,38], and short term (9 RCTs; MD = − 1.56, 95% CI − 2.80 to − 0.95) (Fig. 3, plot 2.1.2) [26, 30, 31, 30,40,31, 50, 54, 57].

Needling therapies versus no intervention, and needling therapies versus additional comparison interventions where the attributable effect of could be isolated for pain in the immediate term (closest to 2 weeks); scale range is 0 to 10

Needling therapies versus no intervention, and needling therapies versus additional comparison interventions where the attributable effect could be isolated for pain in the short term (closest to 3 months); scale range is 0 to 10
Due to low certainty evidence, needling therapies may reduce functional limitations (scale 0 to 100, 0 = no functional limitations; benefit indicated by lower values) in the immediate (19 RCTs; SMD = − 1.39, 95% CI − 2.00 to − 0.77) (Fig. 4, Online Resource 7, plot 2.2.1) [31, 37, 38, 40, 37,42,43,44,45,46,47,38, 37,42,43,44,45,46,47,50,38, 54, 57, 37,42,43,44,45,46,47,50,59,60,38], and short term (8 RCTs; SMD = − 0.57, 95% CI − 0.92 to − 0.22) (plot 2.2.2) [26, 30, 31, 40, 50, 54, 30,57,31]. Due to very low certainty evidence, it is uncertain whether needling therapy reduces functional limitations in the intermediate term (1 RCT; MD = − 8.30, 95% CI − 13.93 to − 2.67) (effect estimate did not reach the thresholds for a minimally important between-group difference, MD = − 10) (plot 2.2.3) [26].

Needling therapies versus no intervention, and needling therapies versus additional comparison interventions where the attributable effect could be isolated for function in the immediate term (closest to 2 weeks)
Due to very low certainty evidence, it is uncertain whether needling therapy makes little or no difference to HRQoL (scale 0 to 1, 0 = poor HRQoL) in the immediate term (1 RCT; MD = 0.02, 95% CI − 0.09 to 0.14) (plot 2.3.1) [47]. In the short term, it is uncertain whether needling therapy improves HRQoL (scale 0 to 100, 0 = poor quality of life; PCS: physical component summary, MCS: mental component summary) with respect to the PCS (1 RCT; MD = 6.60, 95% CI 3.90 to 9.30) (effect estimate did not reach the threshold for a minimally important between-group difference, MD = 10) (plot 2.3.2.1) [26]. It is uncertain whether needling therapy makes little or no difference to HRQoL (MCS) (1 RCT; MD = 1.20; 95% CI − 1.86 to 4.26) (plot 2.3.2.2) [26].
Due to very low certainty evidence, it is uncertain whether needling therapy makes little or no difference to depression (scale 0 to 60, 0 = no depression) in the short term (1 RCT; MD = − 0.80, 95% CI − 3.60 to 2.00) (plot 2.4.1) [26].
Due to very low certainty evidence, it is uncertain whether needling therapies make little or no difference to adverse events/harms (3 RCTs; OR = 3.12, 95% CI 0.42 to 23.44) (plot 2.5) [34, 49, 57].
Older Adults (Aged ≥ 60 Years)
One RCT assessed older adults [40]. Due to very low certainty evidence, it is uncertain if needling therapy reduces: pain (scale 0 to 10, 0 = no pain) in the immediate (MD = − 0.90, 95% CI − 1.53 to − 0.27) (effect estimate did not reach the threshold for a minimally important between-group difference, MD = − 1) (plot.2.6.1.1), or short term (MD = − 1.10, 95% CI − 1.62 to − 0.58) (plot2.6.2.1); or functional limitations (benefit indicated by lower values) in the immediate (SMD = − 1.10, 95% CI − 1.71 to − 0.48) (plot 2.7.1.1), or short term (SMD = − 1.04, 95% CI − 1.66 to − 0.43) (plot 2.7.2.1). No RCTs assessed harms/adverse events.
Needling Therapies Versus Usual Care
All Adults
One trial assessed benefits [27]. Due to very low certainty evidence, it is uncertain whether needling therapy reduces pain (scale 0 to 10, 0 = no pain) in the short (MD = − 1.35, 95% CI − 1.86 to − 0.84) (plot 3.1.1), or intermediate term (MD = − 0.65, 95% CI − 1.17 to − 0.13) (effect estimate did not reach the threshold for a minimally important between-group difference, MD = − 1) (plot 3.2.1); or whether needling therapy makes little or no difference to pain in the long term (MD = − 0.50, 95% CI − 1.02 to 0.02) (plot 3.1.3). It is uncertain whether needling therapy reduces functional limitations (scale 0 to 24, 0 = no functional limitations) in the short (MD = − 2.55, 95% CI − 3.70 to − 1.40) (plot 3.2.1), intermediate (MD = − 1.65, 95% CI − 2.83 to − 0.47) (plot 3.2.2), or long term (MD = − 1.90, 95% CI − 3.15 to − 0.65) (effect estimate did not reach the threshold for a minimally important between-group difference for the latter 2 timepoints, MD = − 2.4) (plot 3.2.3). No RCTs assessed harms/adverse events.
Results of Subgroup and Sensitivity Analyses
The subgroups were small (consisting of 1 to 3 RCTs per group), yielding small, imprecise pooled effects (see Online Resource 7). In addition, there was inadequate reporting of some factors, such as gender/sex or presence of leg pain in participants, which further limited the usefulness of the pooled results. Despite limitations, subgroup effects were overall in line with those of the main analysis.
We examined publication bias using funnel plots when the number of RCTs per comparison was 10 or more. Two funnel plots (needling therapy versus no treatment for pain and function in the immediate term) showed no substantial publication bias (plots 4.1.1, 4.2.1).
Discussion
Recent evidence regarding the benefits and harms of needling therapies for CPLBP in adults is based on 37 RCTs (n = 7573 total adults, n = 55 older adults). Most of the RCTs (30, 81%) were rated as having a high overall ROB and the certainty of the evidence for all outcomes ranged from low to very low. For most outcomes, there was little or no difference between needling therapies and comparison interventions. Evidence suggested the following clinically important benefits for certain outcomes (with low to very low certainty): (1) compared to sham, evidence suggested a small improvement in HRQoL (physical) in the intermediate term; (2) compared to no intervention (including comparison interventions where the attributable effect of needling therapies could be isolated), evidence suggested small reductions in pain in the immediate and short terms, and large and moderate reductions in functional limitations in the immediate and short term, respectively. In older adults, evidence suggested a larger reduction in functional limitations in the immediate and short terms; (3) compared to usual care, evidence suggested a small reduction in pain and functional limitations in the short term. Of nine RCTs reporting on harms/adverse events, 4.3% (2/46) older adults reported mild subcutaneous hematoma after needling compared with sham needling (1 RCT).
Our findings align with those by Mu et al. [10], as discussed at the onset. They also align with Asano et al. [67], who stated that acupuncture as an adjunct to usual care may provide some benefits in reducing immediate and short-term pain and disability among adults with CPLBP (|no other outcomes were assessed).
Our systematic review has several strengths. First, we had an expert review team that included international clinical and methodological experts in the fields of LBP, systematic reviews and evidence syntheses, and answering important policy questions from the WHO. Second, our review employed comprehensive and peer-reviewed literature search strategies that did not have any language restrictions. Third, we ensured that at least half of the screening and ROB pairs were formed by a member of the core team, who was the most trained and reliable in screening and ROB judgements. Fourth, unlike other systematic reviews that relied on the number of items at risk of bias or summary scores for ROB assessments, we developed and used adjunct guidance forms based on the ROB1 criteria, which allowed reviewers to consider important critical flaws [11]. Consequently, there was high agreement for overall ROB ratings. Finally, we maintained transparency in all review steps by providing detailed ROB assessments and footnotes for grading the certainty of the evidence (see Online Resources 4, 5). This approach allowed readers to understand how we came to our judgements, enabling them to make their own judgements and conclusions.
There are potential limitations to our systematic review. First, despite our rigorous literature search strategies, we may have missed some potentially relevant RCTs, especially as we were unable to retrieve and assess the eligibility of 54 full-text RCTs identified from our database search (mainly due to restricted international access). This may have increased or decreased our effect estimates. Second, our pre-specified eligibility criteria was restricted to published trials and did not search the grey literature. However, we do not have strong evidence to suggest our review was impacted by publication bias, based on our publication bias assessment. We searched for unpublished RCTs in the WHO ICTRP registry and contacted authors of unpublished RCTs. However, only two authors responded, and the reason given for non-publication was ongoing RCTs. While we are uncertain how publication bias may have impacted our findings, unpublished studies have been shown to represent a small proportion of studies and rarely impact the results and conclusions [68, 69]. Finally, the decision to combine different sets of comparison interventions in meta-analysis (i.e., no intervention and sets of interventions where the attributable effect of needling therapies could be isolated) may have contributed to inconsistent pooled effects.
We identified evidence gaps across all comparisons. First, there were some outcomes for which there were no RCTs, mainly psychological outcomes (including fear avoidance, catastrophizing, anxiety, and self-efficacy), social participation including work; or change in medication use or falls in older adults. Further research is needed to explore these outcomes comprehensively.
For the comparison of needling therapies to sham, we found no RCTs to inform the long-term benefits on function, or depression. For the comparison of needling therapies to no intervention or interventions where the attributable effect of needling therapies could be isolated, we found no RCTs to inform the intermediate- to long-term benefits on pain, HRQoL and depression and no RCTs to inform the long-term benefits on function. Finally, we identified a scarcity of pragmatic RCTs comparing needling therapies with usual care, which may limit our understanding of their comparative effectiveness in real-world settings.
In terms of assessing benefits and harms, subgroup analyses posed challenges, particularly when considering mode of delivery and spine-related leg pain. This limitation may prevent guideline developers from providing specific case mix recommendations for clinical practice. Moreover, the reporting of harms/adverse events across studies was inadequate and inconsistent. This is particularly concerning for older adults and individuals taking anti-coagulants, as it hampers our ability to assess potential risks accurately.
Conclusion
Based on low or very low certainty evidence, adults with CPLBP experienced small improvements with respect to pain and HRQoL (physical), and both adults and older adults experienced larger reductions in functional limitations. Needling therapy was associated with a small increased risk of subcutaneous hematoma in older adults, compared to sham needling. The remaining evidence showed little to no difference in benefits between needling therapies and comparisons for other outcomes, such as depression. Patient care plans should be developed through a collaborative decision-making process, that carefully considers scientific evidence, cost-effectiveness, and relevant contextual factors, such as values and preferences of users of needling therapies. Adverse events should be investigated systematically.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Lu L, Zhang Y, Tang X, Ge S, Wen H, Zeng J, et al. Evidence on acupuncture therapies is underused in clinical practice and health policy. BMJ. 2022;376:e067475.
Berman BM, Langevin HM, Witt CM, Dubner R. Acupuncture for chronic low back pain. N Engl J Med. 2010;363(5):454–461.
Cabyoglu MT, Ergene N, Tan U. The mechanism of acupuncture and clinical applications. Int J Neurosci. 2006;116(2):115–125.
Dommerholt J. Dry needling in orthpedic physical therapy practice. Orthop Phy Ther Pract. 2004;16(3):15–20.
Lao L. Acupuncture techniques and devices. J Altern Complement Med. 1996;2(1):23–25.
Melzack R. Myofascial trigger points: relation to acupuncture and mechanisms of pain. Arch Phys Med Rehabil. 1981;62(3):114–117.
Han JS. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci. 2003;26(1):17–22.
Goldman N, Chen M, Fujita T, Xu Q, Peng W, Liu W, et al. Adenosine A1 receptors mediate local anti-nociceptive effects of acupuncture. Nat Neurosci. 2010;13(7):883–888.
Kim SY, Min S, Lee H, Cheon S, Zhang X, Park JY, et al. Changes of local blood flow in response to acupuncture stimulation: a systematic review. Evid Based Complement Alternat Med. 2016;2016:9874207.
Mu J, Furlan AD, Lam WY, Hsu MY, Ning Z, Lao L. Acupuncture for chronic nonspecific low back pain. Cochrane Database Syst Rev. 1996;2020(12):CD013814.
Cancelliere C, Verville L, Southerst D, Yu H, Hayden JA, Ogilvie R, Bussières A, Gross DP, Pereira P, Mior S, Tricco AC, Cedraschi C, Brunton G, Nordin M, Wong JJ, Shearer HM, Connell G, Hincapié CA. Systematic review procedures for the World Health Organization (WHO) evidence syntheses on benefits and harms of structured and standardized education/advice, structured exercise programs, transcutaneous electrical nerve stimulation (TENS), and needling therapies for the management of chronic low back pain in adults. J Occup Rehabil. 2023. https://doi.org/10.1007/s10926-023-10156-w.
Herbert RD. How to estimate treatment effects from reports of clinical trials. I: continuous outcomes. Aust J Physiother. 2000;46(3):229–235.
Herbert RD. How to estimate treatment effects from reports of clinical trials. II: dichotomous outcomes. Aust J Physiother. 2000;46(4):309–313.
Rubinstein SM, Terwee CB, Assendelft WJ, de Boer MR, van Tulder MW. Spinal manipulative therapy for acute low-back pain. Cochrane Database Syst Rev. 2012;2012(9):CD008880.
Dworkin RH, Turk DC, Wyrwich KW, Beaton D, Cleeland CS, Farrar JT, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain. 2008;9(2):105–121.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New Jersey: Lawrence Erlbaum Associates; 1988.
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Furlan AD, Malmivaara A, Chou R, Maher CG, Deyo RA, Schoene M, et al. 2015 Updated method guideline for systematic reviews in the Cochrane Back and Neck Group. Spine. 2015;40(21):1660–1673.
Hayden JA, Group BEC-CRW. Commentary: collaborative systematic review may produce and share high-quality, comparative evidence more efficiently. J Clin Epidemiol. 2022;152:288–294.
DistillerSR. Version 2023.2.1. 2023.2.1 ed. Ottawa, Canada: DistillerSR; 2023.
Campbell M, McKenzie JE, Sowden A, Katikireddi SV, Brennan SE, Ellis S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ. 2020;368:l6890.
Schünemann HJ, Higgins JPT, Vist GE, Glasziou P, Akl EA, Skoetz N, et al. Chapter 14: Completing ‘Summary of findings’ tables and grading the certainty of the evidence. 2022 [cited January 5, 2022]. In: Cochrane Handbook for Systematic Reviews of Interventions version 63 (updated February 2022). Cochrane. www.training.cochrane.org/handbook. Accessed 5 Jan 2022
R Core Team. A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2022.
Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1–48.
GRADEpro. GDT: GRADEpro Guideline Development Tool (Software]. McMaster University and Evidence Prime; 2021.
Brinkhaus B, Witt CM, Jena S, Linde K, Streng A, Wagenpfeil S, et al. Acupuncture in patients with chronic low back pain: a randomized controlled trial. Arch Intern Med. 2006;166(4):450–457.
Cherkin DC, Sherman KJ, Avins AL, Erro JH, Ichikawa L, Barlow WE, et al. A randomized trial comparing acupuncture, simulated acupuncture, and usual care for chronic low back pain. Arch Intern Med. 2009;169(9):858–866.
Cho YJ, Song YK, Cha YY, Shin BC, Shin IH, Park HJ, et al. Acupuncture for chronic low back pain: a multicenter, randomized, patient-assessor blind, sham-controlled clinical trial. Spine. 2013;38(7):549–557.
de Castro MC, Chaves ECL, Chianca TCM, Ruginsk SG, Nogueira DA, Souza VHS, et al. Contribution of Chinese and French ear acupuncture for the management of chronic back pain: a randomised controlled trial. J Clin Nurs. 2019;28(21–22):3796–3806.
de Castro Moura C, de Cássia Lopes Chaves E, Couto Machado Chianca T, Ruginsk SG, Alves Nogueira D, Iunes DH. Effects of auricular acupuncture on chronic pain in people with back musculoskeletal disorders: a randomized clinical trial. Revista da escola de enfermagem da USP. 2019;53:1–9.
Depaoli Lemos VJ, Selau RC, Blos C, Baptista Dohnert M, Boff Daitx R, de Almeida Brito V. Electroacupuncture and transcutaneous electrical nerve stimulation in chronic nonspecific low back pain: a blind randomized clinical trial. Muscles Ligaments Tendons J. 2021;11(4):719–727.
Haake M, Muller HH, Schade-Brittinger C, Basler HD, Schafer H, Maier C, et al. German Acupuncture Trials (GERAC) for chronic low back pain: randomized, multicenter, blinded, parallel-group trial with 3 groups. Arch Intern Med. 2007;167(17):1892–1898.
Huang Z, Liu S, Zhou J, Yao Q, Liu Z. Efficacy and safety of acupuncture for chronic discogenic sciatica, a randomized controlled sham acupuncture trial. Pain Med. 2019;20(11):2303–2310.
Kerr DP, Walsh DM, Baxter D. Acupuncture in the management of chronic low back pain: a blinded randomized controlled trial. Clin J Pain. 2003;19(6):364–370.
Kim H, Mawla I, Lee J, Gerber J, Walker K, Kim J, et al. Reduced tactile acuity in chronic low back pain is linked with structural neuroplasticity in primary somatosensory cortex and is modulated by acupuncture therapy. Neuroimage. 2020;217:116899.
Kong JT, Puetz C, Tian L, Haynes I, Lee E, Stafford RS, et al. Effect of electroacupuncture vs sham treatment on change in pain severity among adults with chronic low back pain: a randomized clinical trial. JAMA Netw Open. 2020;3(10):e2022787.
Li SK, Zhao J, Cao XW, Zhu S, Liu ZQ, Fan YX. Core stability training combined with acupuncture in treatment of chronic nonspecific low back pain: a prospective randomized controlled trial. Zhen Ci Yan Jiu. 2022;47(2):160–164.
Li YJ, Zhuang WS, Cai XG, Yang Y, Han MM, Zhang DW. Effect of acupuncture at “ three points of ilioumbar” on lumbar function and pain in patients with iliopsoas muscle strain. Zhongguo Zhen Jiu. 2019;39(12):1279–1282.
Martín-Corrales C, Bautista IV, Méndez-Mera JE, Fernández-Matías R, Achalandabaso-Ochoa A, Gallego-Izquierdo T, et al. Benefits of adding gluteal dry needling to a four-week physical exercise program in a chronic low back pain population. A randomized clinical trial. Pain Med. 2020;21(11):2948–2957.
Meng CF, Wang D, Ngeow J, Lao L, Peterson M, Paget S. Acupuncture for chronic low back pain in older patients: a randomized, controlled trial. Rheumatology. 2003;42(12):1508–1517.
Molsberger AF, Mau J, Pawelec DB, Winkler J. Does acupuncture improve the orthopedic management of chronic low back pain—a randomized, blinded, controlled trial with 3 months follow up. Pain. 2002;99(3):579–587.
Moslemi F, Farokhi ZS. Effects of electroacupuncture on pain, functional disability and ultrasonographic changes of gluteus maximus muscle in non-specific chronic low back pain patients with gluteus maximus muscle trigger points. Koomesh. 2020;22(4):604–610.
Pan J, Yang L, Qiu Y, Lyu X, Ye J, Dong Y, et al. Clinical study on effect of acupuncture combined with sling exercise training on lumbar disc herniation (article in Chinese). J New Chin Med. 2019;51(11):237–239.
Ran P. Effect of acupuncture on pain and lumbar function in patients with discogenic low back pain (article in Chinese). Clin J Tradit Chin Med. 2021;33(5):968–971.
Ren B, Feng X, Zhang C. Clinical study on the analgesic effect of acupuncture based on meridian-tendon dialectical theory in chronic low back pain. Chin J Rehabil Med. 2021;36(6):676–680.
Shi F, Dong B, Lin X, Fu Y. Clinical observation on treatment of non-specific low back pain based on meridian theory and acupuncture. J Pract Tradit Chin Int Med. 2021;35(2):93–96.
Sung WS, Hong Y, Jeon SR, Yoon J, Chung EK, Jo HG, et al. Efficacy and safety of thread embedding acupuncture combined with acupuncture for chronic low back pain: a randomized, controlled, assessor-blinded, multicenter clinical trial. Medicine. 2020;99(49):e22526.
Tabatabaiee A, Takamjani IE, Sarrafzadeh J, Salehi R, Ahmadi M. Ultrasound-guided dry needling decreases pain in patients with piriformis syndrome. Muscle Nerve. 2019;60(5):558–565.
Ushinohama A, Cunha BP, Costa LO, Barela AM, Freitas PB. Effect of a single session of ear acupuncture on pain intensity and postural control in individuals with chronic low back pain: a randomized controlled trial. Braz J Phys Ther. 2016;20(4):328–335.
Wang L, Wang Z, Wang Y, Guo Y. Observations on the efficacy of acupuncture for lumbar intervertebral disc herniation. Shanghai J Acu-mox. 2020;39(12):1605–1608.
Wang X, Yu X, Huang F, Luo X, Gong Y. Effect of acupuncture combined with fire acupuncture on pain and serum inflammatory factor in patients with lumbar disc herniation (article in Chinese). Prog Modern Biomed. 2020;20(17):3309–3312.
Weiß J, Quante S, Xue F, Muche R, Reuss-Borst M. Effectiveness and acceptance of acupuncture in patients with chronic low back pain: results of a prospective, randomized, controlled trial. J Altern Complement Med. 2013;19(12):935–941.
Witt CM, Jena S, Selim D, Brinkhaus B, Reinhold T, Wruck K, et al. Pragmatic randomized trial evaluating the clinical and economic effectiveness of acupuncture for chronic low back pain. Am J Epidemiol. 2006;164(5):487–496.
Yeung CK, Leung MC, Chow DH. The use of electro-acupuncture in conjunction with exercise for the treatment of chronic low-back pain. J Altern Complement Med. 2003;9(4):479–490.
Yu S, Ortiz A, Gollub RL, Wilson G, Gerber J, Park J, et al. Acupuncture treatment modulates the connectivity of key regions of the descending pain modulation and reward systems in patients with chronic low back pain. J Clin Med. 2020;9(6):1–16.
Yu XJ, Zhang L, Lu WY, Gao Q, Liu L, Wang Y. Effect of electroacupuncture combined with caudal epidural injection on functional rehabilitation of patients with lumbar hernia. Zhen CI yan jiu = acupuncture research. 2021;46(7):605–609.
Yuan Q, Liu L, Ma J, Wu W, Ye M, Zhang Y. A clinical study of acupuncture therapy for treatment of chronic nonspecific low back pain (article in Chinese). J Tradit Chin Orthop Trauma. 2016;28(6):12–17.
Zaringhalam J, Manaheji H, Rastqar A, Zaringhalam M. Reduction of chronic non-specific low back pain: a randomised controlled clinical trial on acupuncture and baclofen. Chin Med. 2010;5:1–7.
Zhai B, Wang C. Therapeutic effect of drug cupping combined with deep puncture on Jiaji point on lumbar disc herniation and its effect on M-JOA score, ODI index and quality of life. Modern J Integr Tradit Chin West Med. 2019;28(7):692–700.
Zhu X, Shen X, Kang L, et al. Clinical study on acupuncture combined with bone setting manipulation in the treatment of lumbar disc herniation. Hebei J Tradit Chin Med. 2020;42(6):927–931.
Zhu Z. Clinical study on warming-needle moxibustion combined with joint loosening for chronic low back pain. J New Chin Med. 2021;53(1):117–120.
Koppenhaver SL, Weaver AM, Randall TL, Hollins RJ, Young BA, Hebert JJ, et al. Effect of dry needling on lumbar muscle stiffness in patients with low back pain: a double blind, randomized controlled trial using shear wave elastography. J Man Manip Ther. 2022;30(3):154–164.
World Bank Country and Lending Groups. https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups. Accessed 1 May 2022
Kim J, Mawla I, Lee J, Gerber J, Chan ST, Kim H, et al. Resting state functional brain connectivity predicts clinical improvements in chronic low back pain following acupuncture. Integr Med Res. 2020;9:100503.
Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021): Cochrane; 2021. www.training.cochrane.org/handbook.
Endres HG, Zenz M, Schaub C, Molsberger A, Haake M, Streitberger K, et al. German Acupuncture Trials (gerac) address problems of methodology associated with acupuncture studies. Schmerz. 2005;19(3):201.
Asano H, Plonka D, Weeger J. Effectiveness of acupuncture for nonspecific chronic low back pain: a systematic review and meta-analysis. Med Acupunct. 2022;34(2):96–106.
Hopewell S, McDonald S, Clark MJ, Egger M. Grey literature in meta-analyses of randomized trials of health care interventions. Cochrane Database Syst Rev. 2007;2007(2):MR000010.
Hartling L, Featherstone R, Nuspl M, Shave K, Dryden DM, Vandermeer B. Grey literature in systematic reviews: a cross-sectional study of the contribution of non-English reports, unpublished studies and dissertations to the results of meta-analyses in child-relevant reviews. BMC Med Res Methodol. 2017;17(1):64.
Funding
Open access funding provided by University of Zurich. This work was supported by the World Health Organization (Switzerland/Ageing and Health Unit).
Author information
Authors and Affiliations
Contributions
CC, LV, CAH, DS, HY, AB, DPG, PP, SM, ACT, CC, GB, MN, GC, HMS, JJW, and KM contributed to the study conception and design. Material preparation, data collection and analysis were performed by all authors. The first draft of the manuscript was written by HY and CC (Carol Cancelliere) and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
All team members provided DOI forms to WHO for evaluation at inception. CC (Carol Cancelliere), LV, DS, HY, GC, JJW, HMS report funding from the Canadian Chiropractic Guideline Initiative. ACT is funded by a Tier 2 Canada Research Chair in Knowledge Synthesis. JJW is funded by a Banting Postdoctoral Fellowship from the Canadian Institutes of Health Research (CIHR). CAH reports grants to the University of Zurich from the Foundation for the Education of Chiropractors in Switzerland, the Swiss National Science Foundation (SNSF), and the European Centre for Chiropractic Research Excellence (ECCRE) outside the submitted work. SM reports grants from the Canadian Chiropractic Association, Canadian Chiropractic Research Foundation, and CIHR outside of submitted work. JJW reports grants from the CIHR and Canadian Chiropractic Research Foundation (paid to university), and travel reimbursement for research meetings from the Chiropractic Academy of Research Leadership outside the submitted work. JML reports a grant from the European Cooperation in Science and Technology (COST) outside the submitted work. AB reports grants from the Canadian Chiropractic Association, Canadian Chiropractic Research Foundation, and Health Canada outside the submitted work. JJY is funded by an Arthritis Society Canada Postdoctoral Training Fellowship, CIHR Fellowship, and grant from the Danish Foundation for Chiropractic Research and Post-graduate Education, all outside the submitted work.
Ethical Approval
Ethical approval was not required for this systematic review of previously published studies.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yu, H., Wang, D., Verville, L. et al. Systematic Review to Inform a World Health Organization (WHO) Clinical Practice Guideline: Benefits and Harms of Needling Therapies for Chronic Primary Low Back Pain in Adults. J Occup Rehabil 33, 661–672 (2023). https://doi.org/10.1007/s10926-023-10125-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10926-023-10125-3