
Abstract
Gambling Disorder (GD) is a prominent psychiatric disorder affecting individuals worldwide. Research suggests that key risk factors for GD include stressful life events (SLEs) and specific psychological factors, such as gambling-related cognitive distortions. The present study investigated the potential mediating role of specific psychological factors (i.e., gambling-related cognitive distortions, difficulty in emotion regulation, and self-control) in the relationship between SLEs and GD. A cross-sectional study using an online survey was developed to investigate the relationship between SLEs and GD in a mediation model. A total of 516 participants were initially recruited online to the present study, and data from 290 participants were fully included in the statistical analyses conducted. Sociodemographic and gambling-related data were collected in addition to data related to participants’ SLEs, GD, gambling-related cognitive distortions, difficulty in emotion regulation, and self-control. The results of the parallel multiple mediation analysis conducted found that gambling-related cognitive distortions and difficulty in emotion regulation mediated the relationship between SLEs events and GD. However, self-control was not found to mediate this relationship. The findings suggest that individuals who experience SLEs may be more vulnerable to the development of GD through their belief in gambling-related cognitive distortions and experience of difficulty regulating their emotions. Implications regarding potential preventive efforts for GD are discussed.
Similar content being viewed by others


Introduction
According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association [APA], 2013), ‘Gambling Disorder’ (GD) is a psychiatric condition characterised by persistent and recurrent maladaptive patterns of gambling behaviour leading to clinically significant distress or impairment. Globally, prevalence rates for GD have been reported to range from 0.7 to 6.5% (Calado & Griffiths, 2016). GD is a significant global health issue, and in Australia, it has been estimated that approximately 1.5% of men and 0.8% of women are disordered gamblers (Wilkins, 2017).
Previous research has suggested that GD is highly co-morbid with other psychiatric conditions, such as mood, anxiety, and alcohol-use disorders (Potenza et al., 2019). Furthermore, longitudinal studies have found GD to be associated with the subsequent development of additional psychiatric conditions (Parhami et al., 2014). Studies have also shown GD to be a significant source of psychosocial harm, with GD being associated with poorer quality of life and increased suicide attempts (Ledgerwood & Petry, 2004) as well as decreased job productivity, unpaid debts, and engagement in crime to fund the activity (Walker & Sobel, 2016).
Given the numerous adverse effects associated with GD and its negative impact on individuals and those around them, it is important that individuals are prevented from becoming disordered gamblers. To achieve this goal, knowledge of the key risk factors that render individuals more vulnerable to the development of GD is paramount. Empirical evidence has demonstrated that key risk factors for GD (among others) include stressful life events (SLEs) (Poole et al., 2017; Tang & Oei, 2011).
Stressful Life Events and Gambling Disorder
SLEs have been shown to predict the onset of GD as the more SLEs an individual experiences, the more likely that person is to develop GD (Wang et al., 2020). Indeed, disordered gamblers have been found to experience more SLEs than both social and non-gamblers (Bergevin et al., 2006). A number of models have long theorised that gambling, like other maladaptive behaviours, may represent a strategy to help individuals cope with SLEs and related negative emotions (Blaszczynski & Nower, 2002; Jacobs, 1986).
Jacob’s (1986) General Theory of Addiction postulates that SLEs may predispose individuals to maladaptive behaviours, such as gambling, which are engaged in as a way of relieving and/or escaping from the negative emotions associated with stressful events. Furthermore, according to Blaszczynski and Nower’s (2002) pathways model of gambling, there are three subgroups of disordered gamblers, including the emotionally vulnerable disordered gambler. Emotionally vulnerable individuals, by their very nature, struggle to adaptively cope with stress, leading emotionally vulnerable disordered gamblers to gamble as a way of coping with SLEs and associated negative emotions (Blaszczynski & Nower, 2002). Qualitative studies support these theoretical models, with participants stating gambling helped them to escape from SLEs as well as improve their associated negative mood (Hagen et al., 2013; Wood & Griffiths, 2007). Since addictive disorders are thought to constitute a maladaptive form of coping (Tobin et al., 2014), it is possible GD will follow a similar pattern in relation to SLEs.
Although longitudinal studies have shown SLEs to predict GD (e.g., Luce et al., 2016), alternative evidence exists suggesting SLEs may be unrelated to gambling and the subsequent development of GD. For example, Lightsey and Hulsey (2002) found among females, SLEs were not a direct predictor of GD, while among males, SLEs only indirectly predicted GD through lower levels of impulsiveness. Similarly, Storr et al. (2012) reported no association between adverse life events and GD in their study.
Blaszczynski and Nower’s (2002) pathways model of gambling also serves to support the idea that SLEs may be unrelated to GD. That is, in addition to the emotionally vulnerable disordered gambler who gambles as a way of coping with SLEs, Blaszczynski and Nower (2002) also identified the behaviourally conditioned disordered gambler and the antisocial impulsivist disordered gambler. Behaviourally conditioned disordered gamblers are theorised to become disordered gamblers through behavioural reinforcements, such as classical and operant conditioning (e.g., learning to associate gambling with positive emotions; Blaszczynski & Nower, 2002). However, antisocial impulsivist disordered gamblers are said to become disordered gamblers due to the impulsive traits they possess (Blaszczynski & Nower, 2002).
Jacob’s (1986) general theory of addiction also reinforces the idea that SLEs and GD may be unrelated. Along with individuals gambling to relieve or escape from negative emotions associated with SLEs, this theory posits that another predisposing condition for maladaptive behaviours, such as disordered gambling, is abnormally high or low physiological arousal states (Jacobs, 1986). More specifically, it is theorised that individuals with chronically high or low arousal levels will likely only respond to a narrow window of stress-reducing substances or experiences, which may potentially be addictive (e.g., gambling). For example, an individual with chronic low levels of arousal may gamble and subsequently develop GD because gambling is a stimulating activity which enhances their physiological arousal state (Jacobs, 1986).
Given the existing conflicting evidence, Tang and Oei (2011) suggested that not all gamblers who experience SLEs subsequently develop GD, indicating that the relationship between these two phenomena may not be straightforward. Consequently, it is important to further investigate the relationship between SLEs and GD to delineate the underlying factors that may mediate this relationship.
Gambling-Related Cognitive Distortions
Gambling-related cognitive distortions are erroneous beliefs gamblers may hold regarding their ability to influence, control, or predict the outcome of a chance-based event (Griffiths, 1994; Jacobsen et al., 2007). Such cognitive distortions also encompass the belief gambling will result in various positive outcomes and money lost to gambling will be recovered by gambling further (Griffiths, 1994; Jacobsen et al., 2007). A robust relationship has been shown between gambling-related cognitive distortions and GD, with disordered gamblers consistently being found to hold more cognitive distortions about gambling than non-disordered gamblers (Griffiths, 1994; Leonard & Williams, 2016).
The cognitive model of gambling posits that gambling-related cognitive distortions play a significant role in the development of GD (Leonard & Williams, 2016). More specifically, gamblers who hold such erroneous beliefs may come to gamble at disordered levels as they mistakenly believe they are more likely to win, due to their perceived control over gambling outcomes and misunderstanding as to the nature of probability in chance-based events (Griffiths, 1994; MacKay & Hodgins, 2012). Although the relationship between gambling-related cognitive distortions and GD is supported by several studies, including robust longitudinal research (e.g., Leonard & Williams, 2016), it remains unclear whether such cognitive distortions predispose disordered gambling or whether these erroneous beliefs stem from disordered levels of gambling (Brooks et al., 2020). Consequently, causal inferences between these variables cannot currently be established.
According to Tang and Oei (2011), SLEs can trigger cognitive distortions, including gambling-related cognitive distortions, which in turn, may increase an individual’s vulnerability to GD. For example, Friedland et al. (1992) found participants experiencing high levels of stress were more likely to hold distorted beliefs about gambling in comparison to participants experiencing low levels of stress. Previous research has demonstrated that SLEs can compromise skills associated with executive functioning, including the ability to successfully appraise situations (Pechtel & Pizzagalli, 2011). Due to this deficit in cognitive appraisal ability, individuals who experience SLEs may be more susceptible to cognitive distortions, such as gambling-related cognitive distortions (Tang & Oei, 2011). This is because individuals with an impaired cognitive appraisal ability struggle to adequately evaluate situations, resulting in a potentially distorted view of those situations (Tang & Oei, 2011).
Psychological interventions targeting gambling-related cognitive distortions have been shown to be moderately effective in the treatment of GD (Ladouceur et al., 2001). However, upon review of these studies, high rates of treatment non-response and relapse were found to be present (Daughters et al., 2003), suggesting that additional psychological factors (e.g., difficulty in emotion regulation and lack of self-control) may underlie the relationship between SLEs and GD.
Difficulty in Emotion Regulation
The term ‘emotion regulation’ refers to the cognitive process whereby individuals exert control over which emotions they experience, and when and how they experience them (Poole et al., 2017). Difficulty in emotion regulation, therefore, refers to deficits in this complex process. Difficulty in emotion regulation is a key risk factor for the development of GD (Poole et al., 2017), with the DSM-5 diagnostic criteria for GD (APA, 2013) accounting for this and including “gambling when feeling distressed” within the core diagnostic criteria for GD. This indicates that disordered gamblers may have difficulty regulating their negative emotions, potentially leading them to gamble more to cope with these emotions (Navas et al., 2017). Several studies have found difficulty in emotion regulation to be positively associated with GD, with disordered gamblers consistently exhibiting greater difficulty regulating their emotions when compared to non-disordered gamblers (Navas et al., 2017; Poole et al., 2017).
An individual’s emotion regulation skills are thought to influence their mood (Marchica et al., 2020). More specifically, individuals with poor emotion regulation skills are likely to experience negative emotions more fully owing to the fact that they struggle to control their emotions, particularly negative emotions (Marchica et al., 2020). Consequently, individuals who experience difficulty regulating their emotions may be more likely to engage in maladaptive behaviours, such as gambling, in order to relieve their negative mood, potentially rendering them more vulnerable to the development of GD as a maladaptive coping mechanism (Marchica et al., 2020).
Wang et al. (2020) have suggested that SLEs can facilitate emotion regulation difficulties, in turn, increasing susceptibility to GD. Burns et al. (2010) found females who had experienced SLEs (e.g., physical, emotional, or sexual abuse) had greater difficulty regulating their emotions compared to females who had not experienced such adversities. Building on this, Poole et al. (2017) found that difficulty in emotion regulation mediated the relationship between adverse childhood experiences (i.e., a specific type of stressful life event occurring during childhood) and GD.
According to Burns et al. (2010), SLEs trigger intense negative emotions which overwhelm and consequently impair an individual’s capacity to effectively regulate their emotions. This difficulty in emotion regulation among individuals who experience SLEs results in them being less able to control their negative emotions (Burns et al., 2010). Consequently, such individuals may be more likely to engage in potentially problematic behaviours (e.g., problematic gambling) to down-regulate their adverse emotions, possibly rendering them more susceptible to the development of GD as a maladaptive coping strategy (Burns et al., 2010). While there is evidence suggesting that SLEs can elicit emotional vulnerabilities, such as deficits in emotional regulation, it is important to note that such emotional vulnerabilities may also render individuals more sensitive to stress (Tang & Oei, 2011).
Self-Control
Self-control refers to an individual’s capacity to modify or override their impulses, urges, desires, and habitual responses (Hagger et al., 2010). Therefore, in the context of disordered gambling, self-control may refer to an individual’s ability to modify or override their urge to gamble. According to Baumeister et al. (2007), individuals who lack self-control are more likely to experience maladaptive behavioural and social outcomes, such as GD. Indeed, self-control failures are central to the development of GD (Bergen et al., 2012), with repeated unsuccessful attempts to resist the urge to gamble being one of the key DSM-5 diagnostic criteria for GD (APA, 2013). Previous research has demonstrated a negative relationship between self-control and GD, wherein disordered gamblers report lower levels of self-control and exhibit less controlled behaviours compared to non-disordered gamblers (e.g., Bergen et al., 2012; McQuade & Gill, 2012).
Arguably, the dominant theoretical model with regards to self-control is the strength model (Baumeister et al., 2007). This model proposes that self-control is a finite resource whereby acts of self-control temporarily deplete an individual’s self-control store, thus impairing successive acts of self-control in the short-term. Consistent with this model, those who have a weakened self-control store may be more vulnerable to the development of GD because such individuals may be less able to control their gambling urges (McQuade & Gill, 2012). While most studies investigating the strength model of self-control have provided supporting evidence (see Hagger et al., 2010), a few studies have found conflicting evidence. Specifically, that participants’ self-control stores were not significantly weaker after engaging in activities requiring self-control (e.g., Stillman et al., 2009).
SLEs are thought to deplete an individual’s self-control store, consequently increasing vulnerability to GD (Friedland et al., 1992). Evidence for this notion comes from a qualitative study conducted by Ricketts and Macaskill (2003), which found participants with GD did not believe they would be able to modify or override their urge to gamble in the face of a negative emotional trigger, such as SLEs. According to Hamilton (1982), when confronted with SLEs, individuals automatically represent that stress and the effort needed to cope with it in their conscious minds. However, this conscious representation requires finite resources, such as self-control, leading this automatic event to unintentionally weaken an individual’s self-control store (Hamilton, 1982). Furthermore, SLEs trigger intense negative emotions (Burns et al., 2010), and attempting to control or suppress emotions has been found to weaken an individual’s self-control store (Muraven et al., 1998). Namely, the act of controlling or suppressing emotions involves individuals overriding the habitual response of experiencing emotions as they are, which requires self-control (Hagger et al., 2010).
Study Aim and Hypothesis
Based on the aforementioned rationale, the aim of the present study was to establish the potential mediating role of specific psychological factors (i.e., gambling-related cognitive distortions, difficulty in emotion regulation, and self-control) in the relationship between SLEs and GD. Consistent with previously discussed theory and research findings, it was hypothesised that gambling-related cognitive distortions, difficulty in emotion regulation, and self-control would mediate (through significant indirect effects) the relationship between SLEs and GD.
Methods
Design and Sample Size Considerations
This study adopted a cross-sectional design utilising an online survey to investigate the aforementioned hypothesis. Accordingly, a mediation model comprising one main predictor variable (i.e., SLEs), three mediating variables (i.e., gambling-related cognitive distortions, difficulty in emotion regulation, and self-control), and one outcome variable (i.e., GD) was computed. Prior to data collection, an a priori power analysis was conducted using G*Power 3.1.9.7 to determine the minimum sample size the present study required. Based on a pre-set power (1 − β = 0.95), medium effect size (f2=0.15), and alpha of 0.05 with six predictor variables, it was estimated a minimum of 146 participants would need to be recruited to achieve sufficient statistical power.
Participants and Procedure
Initially, 516 participants were recruited to the study using an online survey created on SurveyMonkey. In order to be eligible to participate, all participants had to fulfil the following inclusion criteria: (i) being Australian citizens or permanent residents, (ii) being at least 18 years old, (iii) having proficiency in English, and (iv) having gambled within the past 12 months. The present study was granted ethics approval by the Tasmania Social Sciences Human Research Ethics Committee (Project ID: 20,602).
Participants recruited were either undergraduate psychology students from the University of Tasmania (n = 42) or members of the broader Australian population either recruited through Prolific (n = 365) or social media platforms (e.g., Facebook) (n = 109). Participants recruited from the University of Tasmania were compensated with course credit (i.e., 0.25 credits per 15 min), while those recruited through Prolific received monetary compensation (i.e., £7.80 per hour). Participants recruited through social media did not receive any form of compensation.
Prior to commencing the survey, participants were required to read a participant information and informed consent sheet, which informed them about their right to remain anonymous as well as that full participation would take approximately 15 min. All participants provided informed consent before beginning the survey. In order to determine participant eligibility, those who responded ‘no’ to the question, ‘Have you engaged in any gambling activity in the past 12 months’ (n = 212), were screened-out. Similarly, participants who failed an attention check question included in the survey (i.e., ‘Please select strongly disagree’, n = 14) were also excluded to increase the quality of the data collected. Consequently, the final sample size used in the analyses included a total of 290 participants.
Measures
Socio-demographics and gambling-related behaviours. Demographic data were collected on participants’ gender, age, relationship status, and gambling expenditure (see Supplementary Table 1 for full descriptive statistics). The question ‘Have you been negatively impacted by the COVID-19 pandemic?’ was also included to estimate potential effects related to the global pandemic. Data pertaining to participants’ gambling behaviours were assessed in the context of a typical month in the past year, and collected by asking for frequency of engagement in land-based and online gambling (1 = ‘Not at all’ to 5 = ‘Daily’), average AUD amount spent on gambling, and frequency of spending on a variety of gambling activities as outlined in Boldero and Bell (2012) (1 = ‘Not at all’ to 5 = ‘Daily’).
DSM-5 Diagnostic Criteria for GD (APA, 2013). Disordered gambling was assessed using the nine DSM-5 diagnostic criteria for GD. All nine criteria were responded to on a binary scale (0 = ‘No’ or 1 = ‘Yes’), with participants indicating whether they had endorsed each criterion in the past 12 months. A total score for the nine criteria was calculated, with respondents who scored four or above being classed as potentially disordered gamblers (APA, 2013). In the present study, the DSM-5 diagnostic criteria for GD exhibited good internal consistency (α = 0.81).
Stressful Life Events Scale (Santini et al., 2015). The Stressful Life Events Scale assesses an individual’s experience of 12 SLEs using a binary scale (0 = ‘I have never experienced this event’ or 1 = ‘I have experienced this event’). In response to the COVID-19 pandemic, three new items were added to this self-report scale to estimate stressful events related to the global pandemic (i.e., ‘Death of a significant other due to illness’, ‘Professional or financial difficulties’, and ‘Significant unplanned change to your lifestyle’). A total score for this 15-item scale was calculated, with higher scores indicating a greater number of SLEs experienced. The Stressful Life Events Scale had acceptable internal consistency in the present study (α = 0.79).
Gamblers’ Beliefs Questionnaire (GBQ; Steenberg et al., 2002). The GBQ is a 21-item self-report scale assessing the extent to which gamblers hold distorted beliefs about gambling. Participants were asked to specify their belief in each gambling-related cognitive distortion using a seven-point Likert scale (1 = ‘Strongly disagree’ to 7 = ‘Strongly agree’). A total score was computed for the GBQ, with higher scores representing a greater belief in gambling-related cognitive distortions. In the present study, the GBQ exhibited excellent internal consistency (α = 0.94).
Difficulties in Emotion Regulation Scale Short Form (DERS-SF; Kaufman et al., 2016). The DERS-SF assesses self-perceived emotion regulation difficulties. The 18 items were rated on a five-point Likert scale (1 = ‘Almost never’ to 5 = ‘Almost always’), with participants indicating how often a variety of statements apply to them. A total score for the DERS-SF was calculated, with higher scores indicating greater deficits in emotion regulation. The DERS-SF demonstrated excellent internal consistency in the present study (α = 0.91).
Amsterdam Executive Function Inventory (AEFI; Van der Elst et al., 2012). The AEFI is a 13-item self-report scale assessing important components of executive functioning across three subscales. To achieve the aims of the present study only the ‘self-control’ subscale (five items) was included. Respondents rate the extent to which they agree with each statement using a five-point Likert scale (1 = ‘Strongly disagree’ to 5 = ‘Strongly agree’). A total score for this subscale was computed, with higher scores indicating greater impairments in self-control. In the present study, the self-control subscale of the AEFI exhibited acceptable internal consistency (α = 0.67).
Statistical Analyses
All data analyses were conducted utilising the statistical package, R (version 1.3.1056; R Core Team, 2020). Statistical analyses included (i) descriptive analysis of the sample’s sociodemographic features and gambling-related behaviours, as well as of all the measures used in the present study, (ii) correlational analysis of the study’s main variables using Holm adjustment to mitigate potential Type 1 error, and (iii) a parallel multiple mediation analysis to examine whether gambling-related cognitive distortions, difficulty in emotion regulation, and self-control would mediate the relationship between SLEs and GD. In order to perform the correlational and mediation analyses in R, the corr.test() and mediate() functions within the ‘psych’ package (Revelle, 2020) were utilised.
Assumptions of the parallel multiple mediation were checked to ascertain the suitability of the data for this analysis. In parallel multiple mediation models, mediators are thought to not causally influence one another (Hayes, 2013). This is in opposition to serial multiple mediation models wherein mediators do causally influence each other (Hayes, 2013). However, mediators in parallel multiple mediation models are assumed to be correlated to some extent since they share a common theme, specifically they are all theorised to play a role in the relationship between the same two variables (Hayes, 2013). Preliminary correlational analysis between the three mediators used in the mediation model demonstrated that these variables were related, but not multicollinear. According to Berry and Feldman (1985), multicollinearity between variables may be evidenced at r ≥ 0.80. The correlation coefficients for the mediators in the present study were all between r = 0.22 and 0.51 (see Table 1), supporting the absence of multicollinearity among the mediators.
Results
Socio-Demographics and Gambling-Related Behaviours
The average age of participants was 33.63 years (SD = 11.87 years), with 167 being male (57.59%), 121 being female (41.72%), and two identifying as ‘other’ (0.69%). With regards to gambling expenditure among participants, the average amount spent on gambling activities in a typical month in the past year was $170.50 AUD (SD = $365.14 AUD). In relation to GD, 36 participants (12.41%) met at least four of the diagnostic criteria for GD as outlined in the DSM-5 (APA, 2013), and were classed as potentially disordered gamblers (see Supplementary Table 1).
Gambling Disorder Correlates
Correlational analysis indicated that GD was positively associated with gambling-related cognitive distortions (r = 0.53, p < 0.001), difficulty in emotion regulation (r = 0.38, p < 0.001), and SLEs (r = 0.22, p < 0.001), and negatively associated with self-control (r = − 0.23, p < 0.001) (see Table 1).
Stressful Life Events and Gambling Disorder Mediators
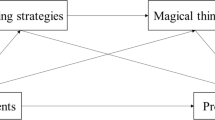
A parallel multiple mediation analysis was conducted to assess whether gambling-related cognitive distortions, difficulty in emotion regulation, and self-control mediated the relationship between SLEs and GD. Overall, the results of this analysis found this mediation model to be statistically significant (F[4, 285] = 43.21, p < 0.001), accounting for approximately 38% of the total variance in GD (R2 = 0.38).
As evidenced in Fig. 1, SLEs produced statistically significant effects on two of the three mediator variables, difficulty in emotion regulation (a2 = 0.18, SE = 0.06, p = 0.002) and self-control (a3 = -0.21, SE = 0.06, p < 0.001), as well as a statistically significant direct effect on the outcome variable, GD (c’ = 0.18, SE = 0.05, p < 0.001). However, SLEs did not have a significant effect on gambling-related cognitive distortions (a1 = 0.02, SE = 0.06, p = 0.779). Furthermore, gambling-related cognitive distortions (b1 = 0.48, SE = 0.05, p < 0.001) and difficulty in emotion regulation (b2 = 0.27, SE = 0.05, p < 0.001) both produced statistically significant effects on GD, while the path from self-control to GD was non-significant (b3 = 0.05, SE = 0.06, p = 0.340).

Indirect effect of gambling-related cognitive distortions, difficulty in emotion regulation, and self-control on the relationship between stressful life events and GD. p-value = *** < .001, ** < .01, * < .05. GD = Gambling Disorder
SLEs had significant indirect effects on GD as mediated through gambling-related cognitive distortions (ab1 = 0.09, 95%CI [0.02, 0.15]) and difficulty in emotion regulation (ab2 = − 0.06, 95%CI [ − 0.11, − 0.02]), but not through self-control (ab3 = 0.01, 95%CI [ − 0.01, 0.03]). The total indirect effect of SLEs on GD through all three mediator variables was non-significant (βa×b = 0.04, 95%CI [ − 0.03, 0.12]). Finally, after taking into account all three mediator variables, the total effect of SLEs on GD was statistically significant (c = 0.22, SE = 0.06, p < 0.001).
In order to determine the statistical significance of indirect effects in multiple mediation analyses, 95% confidence intervals need to be interpreted (Shrout & Bolger, 2002). If zero is encompassed within the 95% confidence range, then the mediation effect is non-significant. Consistent with this approach, support was found for two of the three indirect effects in the present study, SLEs and GD as mediated by gambling-related cognitive distortions (95%CI [0.02, 0.15]) and SLEs and GD as mediated by difficulty in emotion regulation (95%CI [ − 0.11, − 0.02]). However, support was not provided for the relationship between SLEs and GD as mediated by self-control (95%CI [ − 0.01, 0.03]). Accounting for the significant direct effect of SLEs on GD (i.e., c’), these findings indicate that partial mediation effects were present for two of the three mediator variables (i.e., gambling-related cognitive distortions and difficulty in emotion regulation) in the relationship between SLEs and GD.
Discussion
In the absence of a robust body of research seeking to establish factors which may underlie the relationship between SLEs and GD, the present study is the first to determine the potential mediating role of specific psychological factors in the relationship between SLEs and GD. These psychological factors included gambling-related cognitive distortions, difficulty in emotion regulation, and self-control.
The hypothesis that gambling-related cognitive distortions, difficulty in emotion regulation, and self-control would mediate (through significant indirect effects) the relationship between SLEs and GD, was partially supported in the present study. More specifically, gambling-related cognitive distortions and difficulty in emotion regulation were both found to mediate the relationship between SLEs and GD. However, in contrast to that hypothesised, self-control was not found to mediate this relationship. Based on these findings, individuals who experience SLEs may be more susceptible to the development of GD through their belief in gambling-related cognitive distortions and experience of difficulty regulating their emotions.
The finding that gambling-related cognitive distortions mediated the relationship between SLEs and GD is consistent with prior research. Specifically, individuals experiencing high levels of stress have been shown to hold more distorted beliefs about gambling than those experiencing low levels of stress (Friedland et al., 1992). In turn, it has been consistently demonstrated that disordered gamblers hold more gambling-related cognitive distortions compared with non-disordered gamblers (Griffiths, 1994), with disordered gamblers also being found to experience more SLEs than both non-disordered gamblers and non-gamblers (Bergevin et al., 2006).
Stress has been shown to impair an individual’s executive functioning skills, including the ability to successfully appraise situations (Pechtel & Pizzagalli, 2011). Due to this deficit in cognitive appraisal ability, individuals who experience SLEs may be more vulnerable to cognitive distortions, including those which are gambling-related (Tang & Oei, 2011). Gambling-related cognitive distortions are erroneous beliefs regarding the ability to influence or predict the outcome of a chance-based event (Griffiths, 1994; Jacobsen et al., 2007). Consequently, individuals who hold such erroneous beliefs may engage in disordered gambling because they mistakenly believe they are more likely to win, due to their perceived control over gambling outcomes and misunderstanding as to the nature of probability (Griffiths, 1994; MacKay & Hodgins, 2012).
Additionally, the finding that difficulty in emotion regulation mediated the relationship between SLEs and GD is also in line with past research, as difficulty in emotion regulation was found by Poole et al. (2017) to mediate the relationship between stressful childhood experiences and GD. SLEs can trigger intense negative emotions which are thought to overwhelm and consequently compromise an individual’s capacity to successfully regulate their emotions (Burns et al., 2010). This emotion regulation impairment may lead individuals experiencing SLEs to be less able to control their negative emotions, therefore experiencing these adverse emotions more fully (Burns et al., 2010). Consequently, those who experience SLEs and subsequent difficulties in emotion regulation may be more likely to engage in maladaptive behaviours (e.g., gambling) to modify or escape from their negative emotions, potentially rendering such individuals more vulnerable to the development of GD as a maladaptive coping mechanism (Marchica et al., 2020).
The finding that self-control did not mediate the relationship between SLEs and GD is inconsistent with previous research. For example, previous qualitative research reported that participants with GD did not believe they would have the self-control required to modify or override their urge to gamble when experiencing SLEs (Ricketts & Macaskill, 2003), suggesting self-control would mediate the relationship between SLEs and GD.
The strength model of self-control is a state-based theory which conceptualises self-control as a finite resource whereby acts of self-control temporarily deplete an individual’s self-control store, consequently impairing successive acts of self-control in the short-term (Baumeister et al., 2007). Therefore, acts of self-control stemming from the experience of SLEs (e.g., trying to control or suppress the intense negative emotions such events trigger) are expected to only briefly weaken an individual’s self-control store. However, the self-control measure utilised in the present study (Van der Elst et al., 2012) may be assessing more stable trait-based levels of self-control (i.e., ‘I often forget what I have done yesterday’ and ‘I often lose things’). Consequently, this instrument may not have been sensitive enough to the state-based changes in self-control, potentially confounding the present findings in relation to self-control.
Implications
In relation to GD prevention, previous research has suggested that preventive efforts targeting at-risk gambling behaviours alone may be ineffective at reducing the incidence of GD in the community (Felsher et al., 2010), with a more effective approach being to develop prevention strategies which address identified risk factors for GD (Hagen et al., 2013). The results reported in the present study suggest that individuals who experience SLEs may be more susceptible to the development of GD through their belief in gambling-related cognitive distortions and experience of difficulty regulating their emotions. Therefore, in order to prevent the development of GD, those who experience SLEs may benefit from in-depth emotion regulation skills training (Lakey et al., 2007) as well as cognitive behavioural therapy (CBT) skills training focusing on cognitive restructuring techniques for fallacious gambling beliefs (Yakovenko et al., 2016).
Limitations
There are several potential limitations in the present study that should be noted. Firstly, the present study utilised a cross-sectional design which does not allow for the experimental manipulation of variables. Therefore, causal inferences based on the results reported cannot be established. Secondly, the present study utilised self-report measures to collect data, therefore observed results may have been subjected to specific biases, such as social desirability bias. Finally, because the present study’s findings are based on a convenience sample of individuals who had gambled within the past 12 months, observed results may not necessarily generalise to a clinical sample of disordered gamblers. Future studies may benefit from rectifying these limitations, as well as investigating the COVID-related items added to the Stressful Life Events Scale (Santini et al., 2015).
Conclusion
The present study found gambling-related cognitive distortions and difficulty in emotion regulation to mediate the relationship between SLEs and GD. Despite its potential limitations, the present study’s findings help refine current understandings of the possible risk factors for GD, potentially enabling more specific and targeted prevention efforts for GD. However, future research utilising a robust longitudinal design and clinical sample of disordered gamblers is needed to supplement the knowledge on risk factors for GD.
References
American Psychiatric Association. (2013). Substance-related and addictive disorders. In Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596.dsm16
Baumeister, R. F., Vohs, K. D., & Tice, D. M. (2007). The strength model of self-control. Current Directions in Psychological Science, 16(6), 351–355. https://doi.org/10.1111/j.1467-8721.2007.00534.x
Bergen, A. E., Newby-Clark, I. R., & Brown, A. (2012). Low trait self-control in problem gamblers: Evidence from self-report and behavioral measures. Journal of Gambling Studies, 28(4), 637–648. https://doi.org/10.1007/s10899-011-9274-9
Bergevin, T., Gupta, R., Derevensky, J., & Kaufman, F. (2006). Adolescent gambling: Understanding the role of stress and coping. Journal of Gambling Studies, 22(2), 195–208. https://doi.org/10.1007/s10899-006-9010-z
Berry, W. D., & Feldman, S. (1985). Multiple regression in practice: Qualitative applications in the social sciences. SAGE Publications. https://doi.org/10.4135/9781412985208
Blaszczynski, A., & Nower, L. (2002). A pathways model of problem and pathological gambling. Addiction, 97(5), 487–499. https://doi.org/10.1046/j.1360-0443.2002.00015.x
Boldero, J. M., & Bell, R. C. (2012). Chance-and skill-based dimensions underlying young Australians’ gambling activities and their relationships with gambling problems and other factors. International Gambling Studies, 12(2), 145–162. https://doi.org/10.1080/14459795.2011.643907
Brooks, G., Ferrari, M., & Clark, L. (2020). Cognitive factors in gambling disorder, a behavioral addiction. In: Verdejo-Garcia, A. (Ed.), Cognition and addiction (pp. 209–219). Elsevier.
Burns, E. E., Jackson, J. L., & Harding, H. G. (2010). Child maltreatment, emotion regulation, and posttraumatic stress: The impact of emotional abuse. Journal of Aggression, Maltreatment & Trauma, 19(8), 801–819. https://doi.org/10.1080/10926771.2010.522947
Calado, F., & Griffiths, M. D. (2016). Problem gambling worldwide: An update and systematic review of empirical research (2000–2015). Journal of Behavioral Addictions, 5(4), 592–613. https://doi.org/10.1556/2006.5.2016.073
Daughters, S. B., Lejuez, C., Lesieur, H. R., Strong, D. R., & Zvolensky, M. J. (2003). Towards a better understanding of gambling treatment failure: Implications of translational research. Clinical Psychology Review, 23(4), 573–586. https://doi.org/10.1016/S0272-7358(03)00037-0
Felsher, J. R., Derevensky, J. L., & Gupta, R. (2010). Young adults with gambling problems: The impact of childhood maltreatment. International Journal of Mental Health and Addiction, 8(4), 545–556. https://doi.org/10.1007/s11469-009-9230-4
Friedland, N., Keinan, G., & Regev, Y. (1992). Controlling the uncontrollable: Effects of stress on illusory perceptions of controllability. Journal of Personality and Social Psychology, 63(6), 923–931. https://doi.org/10.1037/0022-3514.63.6.923
Griffiths, M. D. (1994). The role of cognitive bias and skill in fruit machine gambling. British Journal of Psychology, 85(3), 351–369. https://doi.org/10.1111/j.2044-8295.1994.tb02529.x
Hagen, B., Kalishuk, R. G., Currie, C., Solowoniuk, J., & Nixon, G. (2013). A big hole with the wind blowing through it: Aboriginal women’s experiences of trauma and problem gambling. International Gambling Studies, 13(3), 356–370. https://doi.org/10.1080/14459795.2013.819934
Hagger, M. S., Wood, C., Stiff, C., & Chatzisarantis, N. L. (2010). Ego depletion and the strength model of self-control: A meta-analysis. Psychological Bulletin, 136(4), 495–525. https://doi.org/10.1037/a0019486
Hamilton, V. (1982). Cognition and stress: An information processing model. In L. Goldberger & S. Breznitz (Eds.), Handbook of stress (pp. 105–120). Free Press.
Hayes, A. F. (2013). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. The Guilford Press.
Jacobs, D. F. (1986). A general theory of addictions: A new theoretical model. Journal of Gambling Behavior, 2(1), 15–31. https://doi.org/10.1007/BF01019931
Jacobsen, L. H., Knudsen, A. K., Krogh, E., Pallesen, S., & Molde, H. (2007). An overview of cognitive mechanisms in pathological gambling. Nordic Psychology, 59(4), 347–361. https://doi.org/10.1027/1901-2276.59.4.347
Kaufman, E. A., Xia, M., Fosco, G., Yaptangco, M., Skidmore, C. R., & Crowell, S. E. (2016). The Difficulties in emotion regulation scale short form (DERS-SF): Validation and replication in adolescent and adult samples. Journal of Psychopathology and Behavioral Assessment, 38(3), 443–455. https://doi.org/10.1007/s10862-015-9529-3
Ladouceur, R., Sylvain, C., Boutin, C., Lachance, S., Doucet, C., Leblond, J., & Jacques, C. (2001). Cognitive treatment of pathological gambling. The Journal of Nervous and Mental Disease, 189(11), 774–780.
Lakey, C. E., Campbell, W. K., Brown, K. W., & Goodie, A. S. (2007). Dispositional mindfulness as a predictor of the severity of gambling outcomes. Personality and Individual Differences, 43(7), 1698–1710. https://doi.org/10.1016/j.paid.2007.05.007
Ledgerwood, D. M., & Petry, N. M. (2004). Gambling and suicidality in treatment-seeking pathological gamblers. The Journal of Nervous and Mental Disease, 192(10), 711–714. https://doi.org/10.1097/01.nmd.0000142021.71880.ce
Leonard, C. A., & Williams, R. J. (2016). The relationship between gambling fallacies and problem gambling. Psychology of Addictive Behaviors, 30(6), 694–704. https://doi.org/10.1037/adb0000189
Lightsey, O. R., Jr., & Hulsey, C. D. (2002). Impulsivity, coping, stress, and problem gambling among university students. Journal of Counseling Psychology, 49(2), 202–211. https://doi.org/10.1037/0022-0167.49.2.202
Luce, C., Kairouz, S., Nadeau, L., & Monson, E. (2016). Life events and problem gambling severity: A prospective study of adult gamblers. Psychology of Addictive Behaviors, 30(8), 922–930. https://doi.org/10.1037/adb0000227
MacKay, T.-L., & Hodgins, D. C. (2012). Cognitive distortions as a problem gambling risk factor in internet gambling. International Gambling Studies, 12(2), 163–175. https://doi.org/10.1080/14459795.2011.648652
Marchica, L. A., Keough, M. T., Montreuil, T. C., & Derevensky, J. L. (2020). Emotion regulation interacts with gambling motives to predict problem gambling among emerging adults. Addictive Behaviors, 106, 106378. https://doi.org/10.1016/j.addbeh.2020.106378
McQuade, A., & Gill, P. (2012). The role of loneliness and self-control in predicting problem gambling behaviour. Gambling Research, 24(1), 18–30.
Muraven, M., Tice, D. M., & Baumeister, R. F. (1998). Self-control as a limited resource: Regulatory depletion patterns. Journal of Personality and Social Psychology, 74(3), 774–789. https://doi.org/10.1037/0022-3514.74.3.774
Navas, J. F., Contreras-Rodríguez, O., Verdejo-Román, J., Perandrés-Gómez, A., Albein-Urios, N., Verdejo-García, A., & Perales, J. C. (2017). Trait and neurobiological underpinnings of negative emotion regulation in gambling disorder. Addiction, 112(6), 1086–1094. https://doi.org/10.1111/add.13751
Parhami, I., Mojtabai, R., Rosenthal, R. J., Afifi, T. O., & Fong, T. W. (2014). Gambling and the onset of comorbid mental disorders: A longitudinal study evaluating severity and specific symptoms. Journal of Psychiatric Practice, 20(3), 207–219. https://doi.org/10.1097/01.pra.0000450320.98988.7c
Pechtel, P., & Pizzagalli, D. A. (2011). Effects of early life stress on cognitive and affective function: An integrated review of human literature. Psychopharmacology, 214(1), 55–70. https://doi.org/10.1007/s00213-010-2009-2
Poole, J. C., Kim, H. S., Dobson, K. S., & Hodgins, D. C. (2017). Adverse childhood experiences and disordered gambling: Assessing the mediating role of emotion dysregulation. Journal of Gambling Studies, 33(4), 1187–1200. https://doi.org/10.1007/s10899-017-9680-8
Potenza, M. N., Balodis, I. M., Derevensky, J., Grant, J. E., Petry, N. M., Verdejo-Garcia, A., & Yip, S. W. (2019). Gambling disorder. Nature Reviews Disease Primers, 5(1), 1–21. https://doi.org/10.1038/s41572-019-0099-7
R Core Team. (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing.
Revelle, W. (2020). psych: Procedures for psychological, psychometric, and personality research. R package version 2.0.9. Northwestern University. https://CRAN.R-project.org/package=psych
Ricketts, T., & Macaskill, A. (2003). Gambling as emotion management: Developing a grounded theory of problem gambling. Addiction Research & Theory, 11(6), 383–400. https://doi.org/10.1080/1606635031000062074
Santini, Z. I., Koyanagi, A., Tyrovolas, S., & Haro, J. M. (2015). The association of relationship quality and social networks with depression, anxiety, and suicidal ideation among older married adults: Findings from a cross-sectional analysis of the Irish Longitudinal Study on Ageing (TILDA). Journal of Affective Disorders, 179, 134–141. https://doi.org/10.1016/j.jad.2015.03.015
Shrout, P. E., & Bolger, N. (2002). Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychological Methods, 7(4), 422–445. https://doi.org/10.1037/1082-989X.7.4.422
Steenbergh, T. A., Meyers, A. W., May, R. K., & Whelan, J. P. (2002). Development and validation of the Gamblers’ Beliefs Questionnaire. Psychology of Addictive Behaviors, 16(2), 143–149. https://doi.org/10.1037/0893-164X.16.2.143
Stillman, T. F., Tice, D. M., Fincham, F. D., & Lambert, N. M. (2009). The psychological presence of family improves self-control. Journal of Social and Clinical Psychology, 28(4), 498–529. https://doi.org/10.1521/jscp.2009.28.4.498
Storr, C. L., Lee, G. P., Derevensky, J. L., Ialongo, N. S., & Martins, S. S. (2012). Gambling and adverse life events among urban adolescents. Journal of Gambling Studies, 28(2), 325–336. https://doi.org/10.1007/s10899-011-9254-0
Tang, C.S.-K., & Oei, T. P. (2011). Gambling cognition and subjective well-being as mediators between perceived stress and problem gambling: A cross-cultural study on White and Chinese problem gamblers. Psychology of Addictive Behaviors, 25(3), 511–520. https://doi.org/10.1037/a0024013
Tobin, S. J., Loxton, N. J., & Neighbors, C. (2014). Coping with causal uncertainty through alcohol use. Addictive Behaviors, 39(3), 580–585. https://doi.org/10.1016/j.addbeh.2013.11.009
Van der Elst, W., Ouwehand, C., van der Werf, G., Kuyper, H., Lee, N., & Jolles, J. (2012). The Amsterdam Executive Function Inventory (AEFI): Psychometric properties and demographically corrected normative data for adolescents aged between 15 and 18 years. Journal of Clinical and Experimental Neuropsychology, 34(2), 160–171. https://doi.org/10.1080/13803395.2011.625353
Walker, D. M., & Sobel, R. S. (2016). Social and economic impacts of gambling. Current Addiction Reports, 3(3), 293–298. https://doi.org/10.1007/s40429-016-0109-8
Wang, C., Neighbors, C., Cunningham-Erdogdu, P., Steers, M.-L.N., & Weinstein, A. P. (2020). Stressful life events and gambling: The roles of coping and impulsivity among college students. Addictive Behaviors, 107, 106386. https://doi.org/10.1016/j.addbeh.2020.106386
Wilkins, R. (2017). The household, income and labour dynamics in Australia survey: Selected findings from waves 1 to 15 (Statistical Report No. 12). Retrieved from Melbourne Institute, University of Melbourne website: https://melbourneinstitute.unimelb.edu.au/__data/assets/pdf_file/0010/2437426/HILDA-SR-med-res.pdf
Wood, R. T. A., & Griffiths, M. D. (2007). A qualitative investigation of problem gambling as an escape-based coping strategy. Psychology and Psychotherapy: Theory, Research and Practice, 80(1), 107–125. https://doi.org/10.1348/147608306X107881
Yakovenko, I., Hodgins, D. C., el-Guebaly, N., Casey, D. M., Currie, S. R., Smith, G. J., Williams, R. J., & Schopflocher, D. P. (2016). Cognitive distortions predict future gambling involvement. International Gambling Studies, 16(2), 175–192. https://doi.org/10.1080/14459795.2016.1147592
Funding
MDG's university has received funding from Norsk Tipping (the gambling operator owned by the Norwegian Government). MDG has received funding for a number of research projects in the area of gambling education for young people, social responsibility in gambling and gambling treatment from Gamble Aware (formerly the Responsibility in Gambling Trust), a charitable body which funds its research program based on donations from the gambling industry. MDG undertakes consultancy for various gaming companies in the area of social responsibility in gambling.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no conflicts of interest except MDG.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Thurm, A., Satel, J., Montag, C. et al. The Relationship Between Gambling Disorder, Stressful Life Events, Gambling-Related Cognitive Distortions, Difficulty in Emotion Regulation, and Self-Control. J Gambl Stud 39, 87–101 (2023). https://doi.org/10.1007/s10899-022-10151-5
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10899-022-10151-5