
Abstract
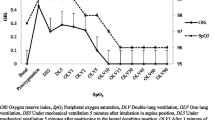
Oxygenation impairment can be assessed non-invasively by determining the degree of right-to-left shunt and ventilation/perfusion (VA/Q) inequality. These indices have been used in sick newborn infants, but normative values have not been reported which are essential to determine the magnitude of the abnormality. We, therefore, aimed to measure the shunt and VA/Q in infants with no history of respiratory conditions and determine if there was any effect of supine or prone position and the reproducibility of the data. Data were analysed from infants who had undergone a hypoxic challenge and in a subset who had been assessed in the supine or prone position. Transcutaneous oxygen saturations (SpO2) were recorded at fractions of inspired oxygen (FIO2) of 0.21 and 0.15. Two independent raters used a computer software algorithm which analysed and fitted paired data for FIO2 and SpO2 and derived a curve which represented the best fit for each infant’s data and calculated the shunt and VA/Q. The raters ability to interpret the SpO2 value which corresponded to a given FIO2 was compared. The downwards displacement of the FIO2 versus SpO2 curve was used to estimate the degree of right-to-left shunt and the rightwards shift of the curve was used to calculate the VA/Q ratio. The mean (SD) gestational age of the 145 infants was 39 (1.6) weeks, their birth weight was 2990 (578) gms and median (range) postnatal age at measurement 3 (1–8) days. The mean (SD) VA/Q ratio was 0.95 (0.21). None of the infants had a right-to-left shunt. No significant differences were found in VA/Q in the supine compared to the prone position. The intraclass correlation coefficient of VA/Q between two independent raters was 0.968 (95% CI 0.947–0.980), p < 0.001. Right-to-left shunt and VA/Q ratio in healthy newborn infants were similar in the prone compared to the supine position.




Similar content being viewed by others

References
Kinsella JP, Greenough A, Abman SH. Bronchopulmonary dysplasia. Lancet. 2006;367(9520):1421–31.
Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001;163(7):1723–9.
Smith HL, Jones JG. Non-invasive assessment of shunt and ventilation/perfusion ratio in neonates with pulmonary failure. Arch Dis Child Fetal Neonatal Ed. 2001;85(2):F127–32.
Bamat N, Ghavam S, Liu Y, DeMauro SB, Jensen EA, Roberts R, et al. Reliability of a Noninvasive Measure of V./Q. Mismatch for Bronchopulmonary Dysplasia. Ann Am Thorac Soc. 2015;12(5):727–33.
Dassios T, Curley A, Morley C, Ross-Russell R. Using Measurements of Shunt and Ventilation-to-Perfusion Ratio to Quantify the Severity of Bronchopulmonary Dysplasia. Neonatology. 2015;107(4):283–8.
Quine D, Wong CM, Boyle EM, Jones JG, Stenson BJ. Non-invasive measurement of reduced ventilation:perfusion ratio and shunt in infants with bronchopulmonary dysplasia: a physiological definition of the disease. Arch Dis Child Fetal Neonatal Ed. 2006;91(6):F409–14.
Roe PG, Jones JG. Analysis of factors which affect the relationship between inspired oxygen partial pressure and arterial oxygen saturation. Br J Anaesth. 1993;71(4):488–94.
Sapsford DJ, Jones JG. The PIO2 vs. SpO2 diagram: a non-invasive measure of pulmonary oxygen exchange. Eur J Anaesthesiol. 1995;12(4):375–86.
Itti E, Nguyen S, Robin F, Desarnaud S, Rosso J, Harf A, et al. Distribution of ventilation/perfusion ratios in pulmonary embolism: an adjunct to the interpretation of ventilation/perfusion lung scans. J Nucl Med. 2002;43(12):1596–602.
Rhodes CG, Valind SO, Brudin LH, Wollmer PE, Jones T, Buckingham PD, et al. Quantification of regional V/Q ratios in humans by use of PET. II. Procedure and normal values. J Appl Physiol. 1989;66(4):1905–13.
Poets CF, Samuels MP, Southall DP. Potential role of intrapulmonary shunting in the genesis of hypoxemic episodes in infants and young children. Pediatrics. 1992;90(3):385–91.
Bhutani VK, Rubenstein SD, Shaffer TH. Pressure–volume relationships of tracheae in fetal newborn and adult rabbits. Respir Physiol. 1981;43(3):221–31.
Hoffman J, Heymann M. Normal Pulmonary circulation In: Scarpelli E, editor. Pulmonary Physiology: Fetus, Newborn, Child and Adolescent. 2nd ed. Philadelphia: Lea & Febiger; 1989. pp. 233–56.
Ali K, Rossor T, Bhat R, Wolff K, Hannam S, Rafferty GF, et al. Antenatal substance misuse and smoking and newborn hypoxic challenge response. Arch Dis Child Fetal Neonatal Ed. 2016;101(2):F143–8.
Prechtl HF, Fargel JW, Weinmann HM, Bakker HH. Postures, motility and respiration of low-risk pre-term infants. Dev Med Child Neurol. 1979;21(1):581–90.
Lockwood GG, Fung NL, Jones JG. Evaluation of a computer program for non-invasive determination of pulmonary shunt and ventilation-perfusion mismatch. J Clin Monit Comput. 2014;28(6):581–90.
Jones JG, Lockwood GG, Fung N, Lasenby J, Ross-Russell RI, Quine D, et al. Influence of pulmonary factors on pulse oximeter saturation in preterm infants. Arch Dis Child Fetal Neonatal Ed. 2016;101(4):F319–22.
Andropoulos D. Monitoring and Vascular Access. In: Gregory G, Andropoulos D, editors. Gregory’s Pediatric Anesthesia. 5th ed. Oxford: Wiley-Blackwell; 2012. pp. 381–418.
Jopling J, Henry E, Wiedmeier SE, Christensen RD. Reference ranges for hematocrit and blood hemoglobin concentration during the neonatal period: data from a multihospital health care system. Pediatrics. 2009;123(2):e333–7.
West J. Pulmonary gas exchange. In: West J, editor. Best and Taylor’s physiological basis of medical practice. Baltimore: Williams & Wilkins; 1991. pp. 546–59.
Sinclair-Smith CC, Emery JL, Gadsdon D, Dinsdale F, Baddeley J. Cartilage in children’s lungs: a quantitative assessment using the right middle lobe. Thorax. 1976;31(1):40–3.
Hislop A, Reid L. Fetal and childhood development of the intrapulmonary veins in man–branching pattern and structure. Thorax. 1973;28(3):313–9.
Gutierrez JA, Duke T, Henning R, South M. Respiratory failure and acute respiratory distress syndrome. In: Taussig LM, Landau LI, editors. Pediatric Respiratory Medicine. 2nd ed. Philadelphia: Mosby Elsevier; 2008. pp. 253–74.
Dassios T, Curley A, Krokidis M, Morley C, Ross-Russell R. Correlation of radiographic thoracic area and oxygenation impairment in bronchopulmonary dysplasia. Respir Physiol Neurobiol. 2016;220:40–5.
Wagner P. Ventilation-Perfusion Relationships. In: Hamid Q, Shannon J, Martin J, editors. Physiologic Basis of Respiratory Disease. Hamilton: BC Decker Inc; 2005. pp. 165–84.
Poets CF, Stebbens VA, Lang JA, O’Brien LM, Boon AW, Southall DP. Arterial oxygen saturation in healthy term neonates. Eur J Pediatr. 1996;155(3):219–23.
Bard H. The postnatal decline of hemoglobin F synthesis in normal full-term infants. J Clin Invest. 1975;55(2):395–8.
Bhat RY, Hannam S, Pressler R, Rafferty GF, Peacock JL, Greenough A. Effect of prone and supine position on sleep, apneas, and arousal in preterm infants. Pediatrics. 2006;118(1):101–7.
Funding
The research was supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. Dr Ali was supported by the King’s College Hospital Research Initiative Grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Dassios, T., Ali, K., Rossor, T. et al. Ventilation/perfusion ratio and right to left shunt in healthy newborn infants. J Clin Monit Comput 31, 1229–1234 (2017). https://doi.org/10.1007/s10877-016-9969-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-016-9969-7