
Abstract
Objective
To test whether an Internet-delivered cognitive behavioral therapy for insomnia (CBT-I) program for older adults attenuates symptoms of depression and anxiety.
Methods
Adults aged ≥ 55 with insomnia were randomized to SHUTi-OASIS (Sleep Healthy Using the Internet for Older Adult Sufferers of Insomnia and Sleeplessness; N = 207) or Patient Education (PE; N = 104). Depression and anxiety were assessed (HADS-D and HADS-A, respectively) at baseline, post-assessment, and 6- and 12-month follow-ups.
Results
Multilevel modeling of HADS-D showed a condition by time interaction (F[3,779] = 3.23, p = .02): SHUTi-OASIS participants reported lower symptoms than PE at post-assessment. There was no such interaction effect for HADS-A (F[3,779] = 2.12, p = .10). Generalized linear modeling showed no moderation of effects by baseline symptom severity.
Conclusions
Participants randomized to Internet-delivered CBT-I showed stable depression and anxiety across time, while control participants’ depressive symptoms briefly increased. CBT-I may help prevent development or worsening of psychological distress among older adults with insomnia.
TRIAL REGISTRATION
[Registered at ClinicalTrials.gov; identifier removed for anonymity]
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Between 20 and 30% of adults aged 55 and older experience insomnia, a rate higher than any other age group (Ancoli-Israel, 2000; Foley et al., 1995, 2004; Maggi et al., 1998; Petit et al., 2003). Older adults with insomnia are also more likely to experience co-occurring psychiatric symptoms, with insomnia conferring greater risk for depression (Nowell & Buysse, 2001; Perlis et al., 2006; Roberts et al., 2000) and anxiety (Brenes et al., 2009). Cognitive behavioral therapy for insomnia (CBT-I) is the recommended treatment for insomnia (Schutte-Rodin et al., 2008) and has also demonstrated treatment benefits on reduced symptoms of depression (Christensen et al., 2016; Suh, 2015; Thorndike et al., 2013) and anxiety (Jansson-Fröjmark & Norell-Clarke, 2016; Thorndike et al., 2013). Moreover, while there is some mixed evidence on this point (Mirchandaney et al., 2022), the benefits of CBT-I on the symptoms of depression and anxiety appear greatest among those entering treatment with higher initial symptomatology (Blake et al., 2018; Lancee et al., 2013; Sandlund & Norell-Clarke, 2020). Addressing insomnia with CBT-I among older adults may therefore help address comorbid symptoms of depression and anxiety.
Historically, sleep difficulties in adults 55 and older were considered the result of normal aging biological processes, and thus inevitable; however, the field now clearly recognizes that insomnia is not a normal part of aging and is a treatable problem for the older adult (Brewster et al., 2018; Fichten et al., 2000). CBT-I effectively treats insomnia among older adults (Irwin et al., 2006; Rybarczyk et al., 2013) by targeting maladaptive cognitions and behaviors that perpetuate insomnia (Chow et al., 2018). Secondary benefits of CBT-I to comorbid symptoms of depression and anxiety may be in part due to addressing shared maladaptive patterns, like catastrophic thinking and irregular sleep scheduling. Like insomnia, psychiatric symptoms of depression and anxiety are also often inappropriately normalized as part of aging, but addressing symptoms remains important to older adults given these symptoms are associated with increased morbidity and mortality (Forlani et al., 2014; Mykletun et al., 2009; Pratt et al., 2016). As stigma against mental illness remains a significant barrier to older adults seeking mental health services (Conner et al., 2010; Stark et al., 2018), CBT-I may represent a more acceptable and appealing option for addressing comorbid psychiatric symptoms among older adults with insomnia by focusing on sleep rather than mood and anxiety directly.
CBT-I has also been effectively delivered by the Internet (Zachariae et al., 2016). Sleep Healthy Using the Internet (SHUTi) is one such fully-automated CBT-I program, which has been demonstrated effective in treating insomnia and addressing comorbid symptoms across various populations both with and without medical and psychiatric comorbidities (Christensen et al., 2016; Luyster et al., 2018; Moloney et al., 2020; Ritterband et al., 2017; Zachariae et al., 2018). Delivering CBT-I by the Internet has several benefits, including: reducing geographical inequities in access to this care, addressing the significant gap in demand to available clinicians, and being more cost-effective than delivering care by a clinician (Chow et al., 2019; De Bruin et al., 2016; Thomas et al., 2016). These benefits are of particular importance for older adults, given that older adults comprise a larger share of the population in rural areas relative to suburban or urban areas (Pew Research Center, 2018), and behavioral sleep medicine providers are less available in rural areas (Chow et al., 2019; Thomas et al., 2016). Also, fully-automated Internet interventions are private, which helps reduce the barrier of stigma to accessing care.
Despite common assumptions to the contrary, most older adults are Internet users: 75% of Americans aged 65 and older, and 96% of Americans aged 50 to 64, say they use the Internet as of 2021 (Pew Research Center, 2021). As such, our team tailored the SHUTi intervention to better address the insomnia treatment needs of older adults, creating SHUTi for Older Adult Sufferers of Insomnia and Sleeplessness (SHUTi OASIS). The objective of this analysis was to determine the extent to which SHUTi OASIS addressed comorbid symptoms of depression and anxiety among older adults with insomnia. We hypothesized that those randomized to receive SHUTi OASIS would report decreased symptoms relative to those receiving an active sleep educational control condition, and that the effect would be most pronounced among those with higher symptoms (relative to less severe symptoms) at baseline.
Materials and methods
Participants and Procedure
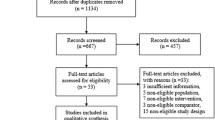
This is a secondary analysis of a national (U.S.) randomized clinical trial (ClinicalTrials.gov registration NCT03213132, approved by the University of Virginia Institutional Review Board). The primary purpose of the trial was to evaluate the efficacy of SHUTi OASIS compared to Internet-delivered patient education (PE) on sleep outcomes among older adults with chronic insomnia. Methodological details for the trial (including full CONSORT diagram) are reported as part of the primary outcomes paper (in preparation); key aspects are reviewed here.
Participants were recruited from across the U.S. via a study website from May 2018 through April 2019. Adults aged 55 and older with regular Internet access were eligible to participate if they met DSM-TR-IV criteria for sleep onset and/or maintenance insomnia for at least the past 6 months, with total sleep time per night averaging 6.5 h or less. While the definition of ‘older adult’ has differed across the insomnia literature, the cutoff for this trial was set at age 55. This decision was made to help address the significant knowledge gap on those aged 55 to 64 who have typically been excluded from most prior studies of ‘older adult’ insomnia (Fichten et al., 2000).
Exclusion criteria included: (1) another untreated sleep disorder; (2) presence of certain (uncontrolled) medical conditions interfering with study procedures (e.g., report Alzheimer’s disease diagnosis, unrecovered from a traumatic brain injury); (3) current or past behavioral insomnia treatment; (4) shift work schedule; and (5) mental health condition deemed to put participant at risk for exacerbation of psychiatric symptoms from participating in treatment and/or to require a higher level of care (i.e., current severe major depressive episode [by clinical interview and Quick Inventory of Depressive Symptomatology score of severe or very severe symptoms (Rush et al., 2003)], current moderate or severe suicidal ideation, substance use disorder [alcohol, drug] within past year, or history of psychotic or bipolar disorder). There were no eligibility criteria related to anxiety symptoms.
Informed consentwas obtained from all participants prior to data collection. Participants completed online assessments at baseline (pre-assessment). A block randomization scheme (n = 3 per block) stratified by age group (55 to 69; 70 and older) was used to assign participants 1:1:1 between three conditions for a nine-week intervention period: SHUTi OASIS, SHUTi OASIS with stepped care to support treatment engagement, or PE. The two SHUTi OASIS conditions have been collapsed for all analyses, as few participants required stepped care and outcomes did not differ between these conditions ([removed for anonymity]).
Following the intervention period, follow-up assessment data were collected at post-assessment (10 weeks after baseline), 6-month follow-up, and 12-month follow-up. Participants received online gift cards as compensation for completing the post-assessment and 6-month follow-up ($50 each) and the 1-year follow-up ($100).
Intervention
SHUTi – Sleep Healthy Using the Internet – is a fully-automated and interactive Internet-delivered insomnia intervention that is tailored based on user-inputted data (Ritterband et al., 2017; Thorndike et al., 2008). The intervention is based on CBT-I, covering the primary tenets of sleep restriction, stimulus control, cognitive restructuring, sleep hygiene, and relapse prevention (Morin, 1993; Thorndike et al., 2008). The intervention is delivered in six “Cores,” or lessons, which each take about 45 min to one hour to complete. Cores are metered out to users on a time- and activity-based schedule. Specifically, the next Core is made available to the user one week following their completion of the prior Core, which allows participants to practice skills between Cores. Users track their sleep using daily online Sleep Diaries, which take about 3 min or less to complete. The intervention provides tailored content to users based on these sleep diaries (e.g., tailored ‘sleep prescriptions’ as part of the sleep restriction technique) and other user-entered data. Automated emails are incorporated into the program to encourage engagement. See Ritterband et al. 2018 and Thorndike et al., 2008 for further description of the SHUTi program.
The SHUTi OASIS program – SHUTi for Older Adult Sufferers of Insomnia and Sleeplessness – modified the original SHUTi program that was designed for the general population to better address the unique needs of older adults with insomnia. Modifications included: Modifying information to better meet the unique needs of the older adult population (e.g., allowing brief naps, norms for older adult sleep, strategies to safely practice stimulus control if mobility limited at night); adding strategies to address factors more common among older adults that precipitate and perpetuate insomnia (e.g., nocturia); modifying intervention vignettes of example users to be more pertinent to older adults (e.g., using pictures and stories of older adults); and user interface changes to improve readability and simplify navigation.
Participants randomized to the Patient Education (PE) condition receive a website of widely available educational material about insomnia. There is overlapping content between SHUTi OASIS and PE conditions, namely, basic educational content about CBT-I principles. In contrast with SHUTi OASIS, however, PE content is not tailored to the user and is not interactive, meaning the content is static and text-based. PE content is also not metered out over time like SHUTi OASIS, meaning PE content is delivered altogether at once. See Ritterband et al. 2018 for further description of the PE program. For both PE and SHUTi OASIS conditions, technical support was available, but no clinical direction was provided. Neither condition provided any direct information or interventions targeting symptoms of depression or anxiety.
Outcome Measure
The Hospital Anxiety and Depression Scale (HADS) was used to measure both symptoms of depression (HADS-D) and anxiety (HADS-A(Zigmond & Snaith, 1983). The HADS is a validated self-report questionnaire with 7 questions addressing depression symptoms and 7 questions addressing anxiety symptoms, answered on a Likert scale (0 “none at all” to 3 “severe”). The subscales demonstrated satisfactory internal reliability at each time point (Cronbach’s alphas = 0.81–0.84 for HADS-D, 0.80–0.82 for HADS-A).
Statistical Analysis
All analyses were conducted using SAS v9.4 (SAS Institute, 2016). Demographic and baseline characteristics of the sample were summarized with measures of central tendency. There was a significant difference between conditions at baseline on reported depression symptoms: prior to randomization, participants who were assigned to SHUTi OASIS (N = 207) reported less severe depression symptoms than those assigned to PE (N = 104; HADS-D independent samples t[309] = 2.86, p = .01). Therefore, a conservative analytic approach of mixed-effects linear modeling (MLM) was used to allow baseline differences between groups, instead of competing and more powerful approaches that assume no baseline differences (e.g., constrained longitudinal data analysis [cLDA]; Coffman et al., 2016). Although there was no such baseline difference between conditions for anxiety symptoms (HADS-A independent samples t[309] = 0.89, p = .37), MLM was also used for the anxiety symptom analyses for consistency. Separate 2 (condition) by 4 (time) MLMs represent time point as a categorical variable; therefore, findings are interpreted as the difference between baseline HADS score and each of the three follow-up time points. The interaction effects of condition by time point evaluated whether change in HADS score differed as a function of randomized assignment to PE or SHUTi OASIS.
Moderation hypotheses, namely, that older adults reporting more severe baseline symptoms would show greater improvement from SHUTi OASIS, were tested using generalized linear regression models using an identity link function. HADS subscale change scores from baseline to follow-up time point were regressed on condition, baseline HADS score, and the interaction between condition and baseline score. In order to control overall type I error in moderation analyses, Holm-Bonferroni adjusted p-values were interpreted.
Results
Demographic characteristics of the overall study sample and by condition are presented in Table 1. Most study participants were female, white, and not Hispanic/Latino/a. The average age of study participants at enrollment was 66 years old, with 30.5% of the sample (95 of 311) aged 70 or older. The study sample was relatively well-educated, affluent, and comfortable using the Internet. Participants’ average reported symptom scores on the HADS-D and HADS-A are listed in Table 2.
Depression symptoms
Depression symptom (HADS-D) MLM model results are shown in Table 1; Fig. 1. There was an interaction between condition and time. Post-hoc contrasts showed that SHUTi participants did not report a change in depression symptoms from baseline to any follow-up time point; however, PE participants reported increased depression symptoms from baseline to post-assessment but no differences between baseline and 6-month or 12-month follow-up assessments. These change trajectories from baseline to post-assessment for SHUTi (i.e., no change) and PE (i.e., increased symptoms) differed; there was no difference between the baseline to 6-month or 12-month follow-up assessment change trajectories between conditions.

Depressive symptom (HADS-D) means and 95% confidence intervals across study time points by group
Note: PE = Patient education (control); SHUTi = Sleep Healthy Using the Internet for Older Adult Sufferers of Insomnia and Sleeplessness (treatment).
Generalized linear regression model results for moderation by baseline depressive symptoms (HADS-D) on change in symptoms of depression demonstrated no significant moderation effects of baseline depressive symptoms on change in depressive symptoms from baseline to post-assessment (χ2[1] = 1.12, Holm-Bonferroni adjusted p = .58), 6-month follow-up (χ2[1] = 0.54, adjusted p = .58), or 12-month follow-up (χ2[1] = 3.54, adjusted p = .18).
Anxiety Symptoms
Anxiety symptom (HADS-A) MLM model results are shown in Table 4; Fig. 2. There was no interaction effect between condition and time. Generalized linear regression model results for moderation by baseline anxiety symptoms (HADS-A) on change in symptoms of anxiety demonstrated no significant moderation effects of baseline anxiety symptoms on change in anxiety symptoms from baseline to post-assessment (χ2[1] = 0.16, adjusted p = 1), 6-month follow-up (χ2[1] = 0.10, adjusted p = 1), or 12-month follow-up (χ2[1] = 0.02, adjusted p = 1).

Anxiety symptom (HADS-A) means and 95% confidence intervals across study time points by group
Note: PE = Patient education (control); SHUTi = Sleep Healthy Using the Internet for Older Adult Sufferers of Insomnia and Sleeplessness (treatment)
Discussion
In this secondary analysis of a trial of an Internet-delivered CBT-I program for older adults, participants randomized to CBT-I tended to show stable symptoms of depression and anxiety up to a year following baseline, while control participants showed a brief increase in depressive symptoms during the intervention period. Average depressive and anxiety symptom scores were modest across assessment time points, but comparable to other samples of community-dwelling older adults on the same measure (Brett et al., 2012). Findings provided partial support for our first hypothesis, namely, that participants randomized to CBT-I showed lower symptoms of depression following the intervention period relative to control participants. There were no differences in anxiety symptoms between groups over the course of the one-year study. Findings did not support that the effect of treatment on comorbid symptoms of depression and anxiety was moderated by baseline symptom severity. It is important to note that SHUTi OASIS participants reported statistically and clinically significant improvements on their subjective and objective insomnia symptoms, and these improvements were greater than those reported by PE participants (primary outcomes manuscript in preparation). This indicates that the intervention was effective for treating insomnia among older adults, while findings from this secondary analysis indicate that the intervention did not impact secondary symptoms of depression or anxiety as hypothesized.
Findings from the present study deviate from some prior research, which has demonstrated positive effects of CBT-I on reducing comorbid psychiatric symptoms in addition to insomnia symptoms. One trial of SHUTi among adults of all ages with insomnia and a history of major depressive disorder demonstrated substantial reductions in symptoms of depression and anxiety relative to control participants across a 6-month follow-up period (Christensen et al., 2016). Similarly, a large-scale trial of another Internet-delivered CBT-I program (Sleepio) among adults of all ages showed small-to-moderate, significant differences in favor of Sleepio relative to a health educational control condition for both symptoms of depression and anxiety (Espie et al., 2019). In a real-world clinical service evaluation, clients from a community-based psychological services provider receiving Sleepio plus support calls reported large reductions in their symptoms of depression and anxiety from pre- to post-treatment (Luik et al., 2017). An important difference between the present study with these three trials is sample age, with the mean ages of the above-mentioned trials being 43, 48, and 44 years, respectively.
In terms of studies of CBT-I among older adults, there are two smaller-scale studies that report effects of face-to-face CBT-I on mood outcomes. These also demonstrated significant reductions in depressive symptoms among older participants receiving CBT-I (Sadler et al., 2018; Tanaka et al., 2019); however, there was a marked difference in effect sizes between trials. In the first trial, Sadler and colleagues (2018) included older adults with comorbid insomnia and major depression and demonstrated a large effect of CBT-I on depressive symptoms relative to a patient education control group (Sadler et al., 2018), and also found significant reductions in anxiety among those receiving CBT-I but not patient education. In the second trial, Tanaka and colleagues (2019) enrolled older adults with insomnia without requiring significant depressive symptoms and demonstrated a small effect of CBT-I relative to wait-list control on depressive symptoms; they did not report findings related to anxiety (Tanaka et al., 2019). Differences between our study and these two trials of face-to-face CBT-I may be due in part to the nature of fully-automating delivery of CBT-I without clinical contact. Even when following a treatment protocol, study therapists may teach cognitive coping skills with more tailored examples pertinent to a participant’s maladaptive thoughts driving not only insomnia but also other psychiatric symptoms. A third recent and larger-scale trial of face-to-face CBT-I versus sleep education among older adults documented lower rates of incident and recurrent depression among older adults receiving CBT-I, with differences most pronounced from 18-month through 36-month follow-ups (Irwin et al., 2022). While our trial followed participants to one year following baseline, a longer follow-up period may have been needed to detect effects on the secondary outcomes of depression and anxiety.
Not all studies have demonstrated CBT-I superior to control on reducing depressive symptoms, however (e.g., Carney et al., 2017; Manber et al., 2016). A review of key moderators of the impact of CBT-I on depression and anxiety highlights two additional possible explanations for our null findings (Mirchandaney et al., 2022). First, individuals with evening circadian preferences appear to benefit most from CBT-I on comorbid psychological symptoms like depression. As sleep timing shifts earlier with aging (Duffy et al., 2015), it is possible that the chronotype of older adults plays a role in their likelihood of receiving secondary benefits of CBT-I to depressive or anxiety symptoms. Secondly, while also not universally demonstrated across past studies, individuals with higher initial depressive and anxiety symptoms have tended to show larger improvements in these symptoms in past CBT-I trials. Participants in our trial were not required to report elevated symptoms of depression or anxiety to qualify for enrollment. The overall modest symptoms reported by our sample may have restricted our ability to detect a decrease in symptoms due to a floor effect, although moderation analyses did not suggest a more powerful effect of treatment among those with elevated symptoms.
While findings did not suggest that CBT-I reduced comorbid symptoms of depression or anxiety, there was a limited protective effect against increased depression symptoms seen among control participants. This potential protective effect is supported by the prior SHUTi trial among adults with a history of major depressive disorder, which showed that those randomized to SHUTi were less likely to endorse moderate or severe depressive symptoms over time relative to control participants (Christensen et al., 2016). This effect for depressive symptoms was, however, small (i.e., one point difference between group averages) and temporary. A prior study suggests the minimally clinically important difference in HADS subscale scores is 1.7, although the estimate ranged from 0.5 to 5.6 points (Lemay et al., 2019); however, the impact of this effect is scaled across the significant reach of fully-automated, Internet-delivered interventions. Moreover, given the comorbidity of insomnia, depression, and anxiety (Jansson-Fröjmark & Lindblom, 2008; Taylor et al., 2005), further study is warranted to better understand why the trajectories of these three sets of symptoms differed over the course of our year-long trial.
The restricted range of reported symptoms of depression and anxiety in the study sample is a limitation of this study. That the sample reported modest overall symptoms may be a function of the use of self-reported symptom severity, as older adults may underreport their mood and anxiety symptoms due to stigma (Fiske et al., 2009; Rosenman et al., 2011). Self-report measures exist that have been developed to specifically assess symptoms of depression and anxiety among older adults with less bias, such as the Geriatric Depression Scale (Yesavage et al., 1982) and the Geriatric Anxiety Scale (Byrne & Pachana, 2011), which were used by Sadler et al. and Tanaka et al. These scales were validated for use among populations aged 65 and older, while the present study recruited individuals aged 55 and older. As such, the HADS was selected for the present trial as it has been validated among adults of all ages and limits bias from comorbid physical health impairments common to aging. In addition to the measurement limitations, the recruited study sample was primarily highly-educated, of high socioeconomic status, and non-Hispanic white, limiting generalizability. A strength of our study includes the use of online recruitment methods (Glazer et al., 2021) to identify a sample generalizable to older individuals who are likely to be interested in using an Internet intervention – and our accrual of 311 participants within 1 year suggests that there is considerable interest.
This secondary analysis of a large-scale RCT comparing SHUTi OASIS to a patient education control group suggests that Internet-delivered CBT-I may help prevent development or worsening of psychological distress commonly comorbid with insomnia among older adults. Participants randomized to Internet-delivered CBT-I tended to show stable symptoms of depression across time, while control participants’ depressive symptoms briefly increased – although there were no differences between groups in change in anxiety across time. Elevated symptoms of depression are associated with increased morbidity and mortality from comorbid physical health conditions (Blay et al., 2007; Pratt et al., 2016), so attenuating the progression of these symptoms among older adults is critical to supporting their long-term well-being. Access to mental health care, and particularly CBT-I, is extremely limited with demand outstripping supply of providers (Thomas et al., 2016). Older adults are more likely to be living in rural areas (Smith & Trevelyan, 2018) and living in poverty (O’Brien et al., 2010), factors that further limit accessibility of evidence-based psychological therapies. Delivering CBT-I by the Internet may increase access to this intervention that may help prevent development or worsening of psychological distress commonly comorbid with insomnia among older adults.
Data Availability
Data available upon reasonable request from the authors.
References
Ancoli-Israel, S. (2000). Insomnia in the elderly: A review for the primary care practitioner. Sleep, 23, S23–30
Blake, M. J., Blake, L. M., Schwartz, O., Raniti, M., Waloszek, J. M., Murray, G., Simmons, J. G., Landau, E., Dahl, R. E., & McMakin, D. L. (2018). Who benefits from adolescent sleep interventions? Moderators of treatment efficacy in a randomized controlled trial of a cognitive-behavioral and mindfulness-based group sleep intervention for at-risk adolescents. Journal of Child Psychology and Psychiatry, 59(6), 637–649
Blay, S. L., Andreoli, S. B., Fillenbaum, G. G., & Gastal, F. L. (2007). Depression morbidity in later life: Prevalence and correlates in a developing country. The American Journal of Geriatric Psychiatry, 15(9), 790–799
Brenes, G., Miller, M., Stanley, M., Williamson, J., Knudson, M., & McCall, W. (2009). Insomnia in older adults with generalized anxiety disorder. The American Journal of Geriatric Psychiatry: Official Journal of the American Association for Geriatric Psychiatry, 17(6), 465–472
Brett, C. E., Gow, A. J., Corley, J., Pattie, A., Starr, J. M., & Deary, I. J. (2012). Psychosocial factors and health as determinants of quality of life in community-dwelling older adults. Quality of Life Research, 21(3), 505–516
Brewster, G., Riegel, B., & Gehrman, P. R. (2018). Insomnia in the Older Adult. Sleep Medicine Clinics, 13(1), 13–19
Byrne, G. J., & Pachana, N. A. (2011). Development and validation of a short form of the Geriatric Anxiety Inventory–the GAI-SF. International Psychogeriatrics, 23(1), 125–131
Carney, C. E., Edinger, J. D., Kuchibhatla, M., Lachowski, A. M., Bogouslavsky, O., Krystal, A. D., & Shapiro, C. M. (2017). Cognitive behavioral insomnia therapy for those with insomnia and depression: A randomized controlled clinical trial. Sleep, 40(4), zsx019
Chow, P. I., Gonzalez, B. D., Ingersoll, K. S., Thorndike, F. P., Shaffer, K. M., Camacho, F., Perlis, M. L., & Ritterband, L. M. (2019). A secondary analysis of the role of geography in engagement and outcomes in a clinical trial of an efficacious Internet intervention for insomnia. Internet Interventions, 18, 100294
Chow, P. I., Ingersoll, K. S., Thorndike, F. P., Lord, H. R., Gonder-Frederick, L., Morin, C. M., & Ritterband, L. M. (2018). Cognitive mechanisms of sleep outcomes in a randomized clinical trial of internet-based cognitive behavioral therapy for insomnia. Sleep Medicine, 47, 77–85
Christensen, H., Batterham, P. J., Gosling, J. A., Ritterband, L. M., Griffiths, K. M., Thorndike, F. P., Glozier, N., O’Dea, B., Hickie, I. B., & Mackinnon, A. J. (2016). Effectiveness of an online insomnia program (SHUTi) for prevention of depressive episodes (the GoodNight Study): A randomised controlled trial. The Lancet Psychiatry, 3(4), 333–341
Coffman, C. J., Edelman, D., & Woolson, R. F. (2016). To condition or not condition? Analysing ‘change’in longitudinal randomised controlled trials.BMJ Open, 6(12), e013096
Conner, K. O., Copeland, V. C., Grote, N. K., Koeske, G., Rosen, D., Reynolds, C. F., & Brown, C. (2010). Mental Health Treatment Seeking Among Older Adults with Depression: The Impact of Stigma and Race. The American Journal of Geriatric Psychiatry: Official Journal of the American Association for Geriatric Psychiatry, 18(6), 531–543
De Bruin, E. J., van Steensel, F. J. A., & Meijer, A. M. (2016). Cost-Effectiveness of Group and Internet Cognitive Behavioral Therapy for Insomnia in Adolescents: Results from a Randomized Controlled Trial. Sleep, 39(8), 1571–1581. https://doi.org/10.5665/sleep.6024
Duffy, J. F., Zitting, K. M., & Chinoy, E. D. (2015). Aging and circadian rhythms. Sleep Medicine Clinics, 10(4), 423–434
Espie, C. A., Emsley, R., & Kyle, S. D. (2019). Effect of Digital Cognitive Behavioral Therapy for Insomnia on Health, Psychological Well-being, and Sleep-Related Quality of Life: A Randomized Clinical Trial. JAMA Psychiatry, 76(1), 21–30
Fichten, C., Libman, E., Bailes, S., & Alapin, L. (2000). Treatment of late-life insomnia. In K. Lichstein, & C. Morin (Eds.), Characteristics of older adults with insomnia (pp. 37–80). Sage Publications
Fiske, A., Wetherell, J., & Gatz, M. (2009). Depression in older adults. Annu Rev Clin Psychol, 5, 363–389
Foley, D., Ancoli-Israel, S., Britz, P., & Walsh, J. (2004). Sleep disturbances and chronic disease in older adults: Results of the 2003 National Sleep Foundation Sleep in America Survey. Journal of Psychosomatic Research, 56(5), 497–502
Foley, D. J., Monjan, A. A., Brown, S. L., Simonsick, E. M., Wallace, R. B., & Blazer, D. G. (1995). Sleep complaints among elderly persons: An epidemiologic study of three communities. Sleep, 18(6), 425–432
Forlani, M., Morri, M., Murri, M. B., Bernabei, V., Moretti, F., Attili, T., Biondini, A., Ronchi, D. D., & Atti, A. R. (2014). Anxiety Symptoms in 74 + Community-Dwelling Elderly: Associations with Physical Morbidity, Depression and Alcohol Consumption. PLOS ONE, 9(2), e89859
Glazer, J. V., MacDonnell, K., Frederick, C., Ingersoll, K., & Ritterband, L. M. (2021). Liar! Liar! Identifying eligibility fraud by applicants in digital health research. Internet Interventions, 25, 100401
Irwin, M. R., Carrillo, C., Sadeghi, N., Bjurstrom, M. F., Breen, E. C., & Olmstead, R. (2022). Prevention of incident and recurrent major depression in older adults with insomnia: A randomized clinical trial. JAMA Psychiatry, 79(1), 33–41
Irwin, M. R., Cole, J. C., & Nicassio, P. M. (2006). Comparative meta-analysis of behavioral interventions for insomnia and their efficacy in middle-aged adults and in older adults 55 + years of age. Health Psychology, 25(1), 3–14
Jansson-Fröjmark, M., & Lindblom, K. (2008). A bidirectional relationship between anxiety and depression, and insomnia? A prospective study in the general population. Journal of Psychosomatic Research, 64(4), 443–449
Jansson-Fröjmark, M., & Norell-Clarke, A. (2016). Cognitive Behavioural Therapy for Insomnia in Psychiatric Disorders. Current Sleep Medicine Reports, 2(4), 233–240
Lancee, J., van den Straten, J., A., & Spoormaker, V. (2013). Baseline depression levels do not affect efficacy of cognitive-behavioral self-help treatment for insomnia. Depression and Anxiety, 30(2), 149–156
Lemay, K. R., Tulloch, H. E., Pipe, A. L., & Reed, J. L. (2019). Establishing the Minimal Clinically Important Difference for the Hospital Anxiety and Depression Scale in Patients With Cardiovascular Disease. Journal of Cardiopulmonary Rehabilitation and Prevention, 39(6), E6
Luik, A. I., Bostock, S., Chisnall, L., Kyle, S. D., Lidbetter, N., Baldwin, N., & Espie, C. A. (2017). Treating depression and anxiety with digital cognitive behavioural therapy for insomnia: A real world NHS evaluation using standardized outcome measures. Behavioural and Cognitive Psychotherapy, 45(1), 91–96
Luyster, F. S., Ritterband, L. M., Sereika, S. M., Buysse, D. J., Wenzel, S. E., & Strollo, P. J. (2018). Internet-based cognitive-behavioral therapy for insomnia in adults with asthma: A pilot study. Behavioral Sleep Medicine, 0(0), 1–13
Maggi, S., Langlois, J. A., Minicuci, N., Grigoletto, F., Pavan, M., Foley, D. J., & Enzi, G. (1998). Sleep complaints in community-dwelling older persons: Prevalence, associated factors, and reported causes. 46, 161–168
Manber, R., Buysse, D. J., Edinger, J., Krystal, A., Luther, J. F., Wisniewski, S. R., Trockel, M., Kraemer, H. C., & Thase, M. E. (2016). Efficacy of cognitive-behavioral therapy for insomnia combined with antidepressant pharmacotherapy in patients with comorbid depression and insomnia: A randomized controlled trial. The Journal of Clinical Psychiatry, 77(10), 2446
Mirchandaney, R., Barete, R., & Asarnow, L. D. (2022). Moderators of Cognitive Behavioral Treatment for Insomnia on Depression and Anxiety Outcomes. Current Psychiatry Reports, 24(2), 121–128
Moloney, M. E., Dunfee, M., Rutledge, M., & Schoenberg, N. (2020). Evaluating the Feasibility and Acceptability of Internet-Based Cognitive Behavioral Therapy for Insomnia in Rural Women. Women’s Health Reports (New Rochelle N y), 1(1), 114–122
Morin, C. M. (1993). Insomnia: Psychological assessment and management. The Guilford Press
Mykletun, A., Bjerkeset, O., Øverland, S., Prince, M., Dewey, M., & Stewart, R. (2009). Levels of anxiety and depression as predictors of mortality: The HUNT study. The British Journal of Psychiatry, 195(2), 118–125
Nowell, P. D., & Buysse, D. J. (2001). Treatment of insomnia in patients with mood disorders. 14, 7–18
O’Brien, E., Wu, K. B., & Baer, D. (2010). Older Americans in Poverty: A Snapshot. AARP Public Policy Institute
Perlis, M. L., Smith, L. J., Lyness, J. M., Matteson, S. R., Pigeon, W. R., Jungquist, C. R., & Tu, X. (2006). Insomnia as a risk factor for onset of depression in the elderly. Behavioral Sleep Medicine, 4, 104–113
Petit, L., Azad, N., Byszewski, A., Sarazan, F., & Power, B. (2003). Non-pharmacological management of primary and secondary insomnia among older people: Review of assessment tools and treatments. Age and Ageing, 32(1), 19–25
Pew Research Center (2018). Demographic and economic trends in urban, suburban and rural communities. https://www.pewresearch.org/social-trends/2018/05/22/demographic-and-economic-trends-in-urban-suburban-and-rural-communities/
Pew Research Center (2021). Demographics of Internet and Home Broadband Usage in the United States. Pew Research Center: Internet, Science & Tech. https://www.pewresearch.org/internet/fact-sheet/internet-broadband/
Pratt, L. A., Druss, B. G., Manderscheid, R. W., & Walker, E. R. (2016). Excess mortality due to Depression and Anxiety in the United States: Results from a Nationally Representative Survey. General Hospital Psychiatry, 39, 39–45
Ritterband, L. M., Thorndike, F. P., Ingersoll, K. S., Lord, H. R., Gonder-Frederick, L., Frederick, C., Quigg, M. S., Cohn, W. F., & Morin, C. M. (2017). Effect of a web-based cognitive behavior therapy for insomnia intervention with 1-year follow-up: A randomized clinical trial. JAMA Psychiatry, 74(1), 68–75
Roberts, R. E., Shema, S. J., Kaplan, G. A., & Strawbridge, W. J. (2000). Sleep complaints and depression in an aging cohort: A prospective perspective. 157, 81–88
Rosenman, R., Tennekoon, V., & Hill, L. G. (2011). Measuring bias in self-reported data. International Journal of Behavioural & Healthcare Research, 2(4), 320–332
Rush, A. J., Trivedi, M. H., Ibrahim, H. M., Carmody, T. J., Arnow, B., Klein, D. N., Markowitz, J. C., Ninan, P. T., Kornstein, S., Manber, R., Thase, M. E., Kocsis, J. H., & Keller, M. B. (2003). The 16-item Quick Inventory of Depressive Symptomatology (QIDS), Clinician Rating (QIDS-C), and Self-Report (QIDS-SR): A psychometric evaluation in patients with chronic major depression. 54,573–583
Rybarczyk, B., Lund, H. G., Garroway, A. M., & Mack, L. (2013). Cognitive behavioral therapy for insomnia in older adults: Background, evidence, and overview of treatment protocol. 36,70–93
Sadler, P., McLaren, S., Klein, B., Harvey, J., & Jenkins, M. (2018). Cognitive behavior therapy for older adults with insomnia and depression: A randomized controlled trial in community mental health services. Sleep, 41, zsy104
Sandlund, C., & Norell-Clarke, A. (2020). Is it more about mood than about sleep?: An investigation into depression as amoderator and mediator of remission after CBT-I. Sömn Och Hälsa, 3, 33–35
Schutte-Rodin, S., Broch, L., Buysse, D., Dorsey, C., & Sateia, M. (2008). Clinical guideline for the evaluation and management of chronic insomnia in adults. Journal of Clinical Sleep Medicine, 4, 487–504
Smith, A., & Trevelyan, E. (2018). The Older Population in Rural America: 2012–2016. U.S. Census Bureau. (American Community Survey Reports)
Stark, A., Kaduszkiewicz, H., Stein, J., Maier, W., Heser, K., Weyerer, S., Werle, J., Wiese, B., Mamone, S., König, H. H., Bock, J. O., Riedel-Heller, S. G., & Scherer, M. (2018). A qualitative study on older primary care patients’ perspectives on depression and its treatments—Potential barriers to and opportunities for managing depression. BMC Family Practice, 19(1), 2
Suh, S. (2015). Cognitive Behavioral Therapy for Insomnia: Is it Effective in Treating Symptoms of Comorbid Psychiatric and Medical Disorders? Sleep Medicine Research, 6(1), 10–15
Tanaka, M., Kusaga, M., Nyamathi, A. M., & Tanaka, K. (2019). Effects of Brief Cognitive Behavioral Therapy for Insomnia on Improving Depression Among Community-Dwelling Older Adults: A Randomized Controlled Comparative Study. Worldviews on Evidence-Based Nursing, 16(1), 78–86
Taylor, D. J., Lichstein, K. L., Durrence, H. H., Reidel, B. W., & Bush, A. J. (2005). Epidemiology of insomnia, depression, and anxiety. 28, 1457–1464
Thomas, A., Grandner, M., Nowakowski, S., Nesom, G., Corbitt, C., & Perlis, M. L. (2016). Where are the behavioral sleep medicine providers and where are they needed? A geographic assessment. Behavioral Sleep Medicine, 14(6), 687–698
Thorndike, F. P., Ritterband, L. M., Gonder-Frederick, L. A., Lord, H. R., Ingersoll, K. S., & Morin, C. M. (2013). A randomized controlled trial of an internet intervention for adults with insomnia: Effects on comorbid psychological and fatigue symptoms. Journal of Clinical Psychology, 69(10), 1078–1093
Thorndike, F. P., Saylor, D. K., Bailey, E. T., Gonder-Frederick, L., Morin, C. M., & Ritterband, L. M. (2008). Development and perceived utility and impact of an Internet intervention for insomnia. E-Journal of Applied Psychology: Clinical and Social Issues, 4(2), 32–42
Yesavage, J. A., Brink, T. L., Rose, T. L., Lum, O., Huang, V., Adey, M., & Leirer, V. O. (1982). Development and validation of a geriatric depression screening scale: A preliminary report. Journal of Psychiatric Research, 17(1), 37–49
Zachariae, R., Amidi, A., Damholdt, M. F., Clausen, C. D. R., Dahlgaard, J., Lord, H., Thorndike, F. P., & Ritterband, L. M. (2018). Internet-delivered Cognitive-Behavioral Therapy for insomnia in breast cancer survivors: A randomized controlled trial. Journal of the National Cancer Institute, 110(8), 880–887
Zachariae, R., Lyby, M. S., Ritterband, L. M., & O’Toole, M. S. (2016). Efficacy of internet-delivered cognitive-behavioral therapy for insomnia: A systematic review and meta-analysis of randomized controlled trials. Sleep Medicine Reviews, 30(1), 1–10
Zigmond, A. S., & Snaith, R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67(6), 361–370
Funding
This research was supported by the National Institute of Aging (R01AG047885; PI: Ritterband). Writing of this manuscript was supported in part by the National Center For Advancing Translational Sciences (UL1TR003015, KL2TR003016; Shaffer). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author information
Authors and Affiliations
Contributions
Shaffer, Smith, and Ritterband were responsible for the conception and design of the work; Glazer, Ingersoll, and Ritterband were responsible for the acquisition of data; Shaffer, Smith, Camacho, Ingersoll, and Ritterband were responsible for the analysis and interpretation of data; Shaffer, Smith, and Ritterband were responsible for drafting the work; and all authors were responsible for revising the work critically for important intellectual content, provided final approval of the submitted manuscript, and are accountable for all aspects of the work.
Corresponding author
Ethics declarations
Disclosure statement
Shaffer, Smith, Glazer, Camacho, Chow, Mattos and Ingersoll report no conflicts of interest. Ritterband reports having a financial and/or business interest in BeHealth Solutions and Pear Therapeutics, two companies that develop and disseminate digital therapeutics, including by licensing the therapeutic developed, based in part, on early versions of the software utilized in research reported in the enclosed paper. These companies had no role in preparing this manuscript. Ritterband is also a consultant to Mahana Therapeutics, a separate digital therapeutic company not affiliated with this research. The terms of these arrangements have been reviewed and approved by the University of Virginia in accordance with its policies.
Previous presentation
This work was previously presented as a poster presentation at the annual meeting and scientific session of the Society of Behavioral Medicine: Smith, J. G., Glazer, J. V., Camacho, F., Ingersoll, K., Ritterband, L. M., & Shaffer, K. M. (2021, April 12–16). Effects of an Internet-delivered insomnia intervention for older adults on depression and anxiety: A secondary analysis. Poster presentation at the 42nd Annual Meeting & Scientific Sessions of the Society of Behavioral Medicine, virtual conference (due to COVID-19).
Ethics approval
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the University of Virginia Institutional Review Board.
Consent to participate
All participants provided informed consent to participate prior to data collection.
Clinical Trial Registration
ClinicalTrials.gov NCT03213132.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Shaffer, K.M., Smith, J.G., Glazer, J.V. et al. Effects of an internet-delivered insomnia intervention for older adults: A secondary analysis on symptoms of depression and anxiety. J Behav Med 45, 728–738 (2022). https://doi.org/10.1007/s10865-022-00353-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10865-022-00353-y