
Abstract
DSM-5 added a categorically defined specifier (‘with Limited Prosocial Emotions’; LPE) for the diagnosis of conduct disorder (CD). This paper systematically reviews the evidence base for this specifier in children and adolescents who are diagnosed with CD. Computer-assisted searches were executed and identified 181 potentially relevant papers. Eventually, nine papers were included in this review, referring to eight unique samples. All studies constructed an LPE measure by pulling the same items from the same rating scales that were used in the development of the DSM-5 LPE specifier. The prevalence of youth with CD who met criteria for this novel LPE specifier (CD + LPE) ranged from 6.1% to 83.7%. The studies greatly varied in the features used to test the viability of the DSM-5 LPE specifier. The most commonly used features relate to severity of antisocial behavior, low neuroticism (or lack of anxiety and depression), and treatment responsiveness. Available work altogether showed that CD + LPE youth displayed higher levels of past antisocial behaviour than CD Only youth, but failed to reveal other group differences that corroborate with expectations. Effect sizes typically were in the small to moderate range, suggesting that the practical usefulness of the group differences is limited. Empirical work shows that this specifier should not be used for clinical decision-making when relying on items from measures that have been used in the development of the LPE specifier. Crucially, limitations that hallmark the few studies on the topic hamper any firm conclusion about the usefulness of the specifier.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Callous-unemotional (CU) traits are commonly characterized by deficient empathy and guilt, insensitivity to others’ feelings, shallow emotions (Andershed et al. 2002; Colins et al. 2014), and sometimes also by being unconcerned about poor performance (APA 2013; Frick 2003). CU traits are increasingly used as a subtyping scheme to understand heterogeneity among children with conduct problems (CP), and to delineate a small but important subgroup of youth with severe CP (Dadds et al. 2014; Frick 2009). Specifically, it is estimated that 20–50% of children with CP exhibit high levels of CU traits and there is evidence to suggest that these children differ from children with CP and low levels of CU traits in various theoretically and clinically relevant features (Frick et al. 2014). Some studies, for example, showed that children with CP and CU display higher levels of severe and stable antisocial behavior (e.g., criminality, aggression, and substance use problems), to exhibit a fearless temperament, to be impaired in their responsiveness to and recognition of cues to fear and sadness in others, and to display higher levels of interpersonal (e.g., grandiosity) and behavioral/lifestyle (e.g., thrill-seeking) psychopathic personality traits (Christian et al. 1997; Frick et al. 2014; Dadds et al. 2003; Frick 2009).
In response to this research, DSM-5 added a CU-based specifier for the diagnosis of conduct disorder (CD), which refers to a repetitive and persistent pattern of behaviour where the basic rights of others, and age appropriate rules and norms are violated (APA 2013). This specifier is labelled ‘with Limited Prosocial Emotions’ (LPE) and is used when an individual meeting diagnostic criteria for CD exhibits 2 or more of the following symptoms over at least 12 months and in multiple relationships and settings: (a) lack of remorse or guilt; (b) callous–lack of empathy; (c) unconcerned about performance; and (d) shallow or deficient affect (APA 2013). Regardless of the potential usefulness of this novel subtyping scheme, researchers and clinicians only recently have an opportunity to use a novel clinical assessment system that was specifically designed to assess the LPE specifier as being described in DSM-5. Echoing DSM-5, this novel system – the Clinical Assessment of Prosocial Emotions (CAPE; Frick 2013) – focuses on the presence (2 ≤), duration (12 months ≤), and pervasiveness (multiple settings and relationships) of the four symptoms. Prior work on the DSM-5 LPE specifier only focused on the presence (2 ≤) of the DSM-5 LPE symptoms by pulling items from commonly used CU rating scales, such as the Antisocial Process Screening Device (Frick and Hare 2001) and the Inventory of Callous-Unemotional Traits (Frick 2003). Consequently, it stands to reason to argue that no study to date tested the DSM-5 LPE specifier as being defined in DSM-5, that is whilst also taking duration and pervasiveness of the symptoms into account.
The first CAPE or other interview-based study that measures the DSM-5 LPE specifier among children and adolescents with CD needed to be published when this review study was performed (see also Discussion). Nevertheless, it is important to systematically review research that construct proxy measures of this specifier by pulling items from rating scales. This research applied the same approach that has been used to develop the DSM-5 LPE specifier symptoms, that is by pulling four and nine items from the APSD and ICU, respectively (Frick and Moffitt 2010). In addition, proponents of the DSM-5 LPE specifier considered studies that used a few APSD and ICU items to construct an DSM-5 LPE measure of extreme relevance to this new specifier (Frick et al. 2014). Therefore, research on the DSM-5 LPE specifier that relied on rating scales such as the APSD or ICU should not be disregarded as uninformative. Also, research that triggered the incorporation of the categorical LPE specifier in DSM-5 relied on dimensional CU scores (Frick and White 2008), or alternative categorical approaches (e.g. median split), to identify children and adolescents with elevated and low levels of CU traits (Schwenck et al. 2012). Hence, it is relevant to scrutinize to what extent findings from studies that explored the potential usefulness of the categorically defined DSM-5 LPE specifier converge with findings from the bulk of prior CU research that fostered the incorporation of the LPE specifier in DSM-5.
The present article aims to review studies that tested the DSM-5 LPE specifier in children and adolescents with CD. Studies included in this review will first be used to illuminate how many children and adolescents with CD meet criteria for the DSM-5 specifier. In line with prior estimates (Frick et al. 2014), a prevalence of 20–50% was expected, although it should be noted that estimates close to 50% are high prevalence rates (see Discussion). Studies reviewed here will also be used to elucidate if children and adolescents with CD who are diagnosed with the DSM-5 LPE specifier (CD + LPE) differ from their CD counterparts who do not meet criteria for the DSM-5 LPE specifier (CD Only) in various clinically and theoretically relevant features. Specific hypotheses will be provided after we have described the features that were used in group comparisons (see Result section).
Method
Data Sources and Search Strategies
Computer-assisted searches were executed using two different search engines (Web of Science and PubMed) looking for English-language, peer-reviewed studies published between 2010 (the year the LPE specifier was first proposed; Frick and Moffitt 2010) and January 31, 2019. Combinations of search terms (Web of Science: Topic; PubMed: Title/abstract) were used relating to both the LPE specifier (i.e. CU specifier; DSM-5 specifier; LPE specifier; limited prosocial emotions; callous-unemotional specifier) and indices of CD (i.e. conduct disorder; conduct problems; antisocial; criminality; aggression; delinquency; criminal justice; behavior problems). The exact search strategy can be retrieved from Appendix 1, available online.
Inclusion Criteria
Studies were included if they met the following three inclusion criteria. First, the application of the DSM-5 LPE specifier requires that the person meets full criteria for CD. Therefore, we only included studies that used a (semi-) structured diagnostic interview or a well-described clinical assessment protocol to determine if a youth met criteria for DSM-IV or DSM-5 defined CD.Footnote 1 This criterion, for example, implies that studies that used rating scales of CD symptoms to confirm the presence of CD were not included (e.g., Fanti et al. 2016; Pardini et al. 2012). Second, we included studies that tested the categorically defined DSM-5 LPE specifier criteria via measures that allow assessing the four DSM-LPE symptoms. Thus, studies that could not assess all symptoms (e.g., Colins 2016; Jambroes et al. 2016) or used CU measures that cannot straightforwardly be linked to the four LPE symptoms, for example, because CU measures also tapped interpersonal traits (Rowe et al. 2010), were not included for review purposes. The first and second inclusion criteria were used to be stringent about assessment procedures. Third, studies were only considered relevant if they reported results from analyses (e.g. group comparisons or CD x LPE interaction effects) that aimed to test if the two groups of interest differ in theoretically and clinically relevant features. Thus, studies that did not formally compare both groups were not included (e.g., McMahon et al. 2010).
Selection
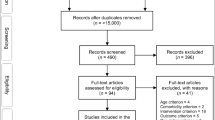
Articles that based upon the abstracts proved not to be relevant were removed. If the suitability of an article, based on abstract and title, was unclear, the full text was examined. Articles remaining after this procedure were all studied in full text and a selection of eligible studies was made. Next, reference lists of the selected articles were carefully checked. Our search strategy results are shown in Fig. 1. The search identified a total of 181 publications whose titles and abstracts were all individually checked, resulting in a second selection of 89 papers. Full texts of the 89 potentially eligible articles were critically appraised; 82 papers deemed not eligible for inclusion. After checking the references lists of the seven selected papers and after an update of advanced online publications (January 2019), five additional potentially relevant papers were identified, though merely two of these latter five studies were included in the review. In total, nine papers were eligible, referring to eight unique samples (see Fig. 1).

PRISMA Flow Diagram * Papers were predominantly excluded for review purposes because CU measures were not used to assess the DSM-5 specifier symptoms. Other reasons were, for example, the use of CU measures that only enable to assess three of the four LPE specifier criteria (Colins 2016; Colins and Vermeiren 2013; Jambroes et al. 2016), the lack of formal comparison of CD + LPE with CD Only youth (McMahon et al. 2010), or lack of information about the assessment procedure followed to determine a CD diagnosis (Pechorro et al. 2015); ** Two papers were identified after checking the references (Kolko and Pardini 2010; Sakai et al. 2017), whilst three papers were identified by advance online publication explorations (Byrd et al. 2018; Sethi et al. 2018; Oldenhof et al. 2018); *** Three of the five aforementioned potentially relevant papers were not included for review purposes because no measures of CD were used (Byrd et al. 2018), and because youth who did not met criteria for CD also enrolled in the study whilst analyses were not run separately for youth with a CD diagnosis (Oldenhof et al. 2018; Sakai et al. 2017); **** Two papers used largely overlapping samples (Colins et al. 2017; Van Damme et al. 2016), but focused on a different research question, and therefore added significant incremental information to the review. Consequently, both papers were included for review purposes but will be treated as one and the same study
Data-Extraction and Data-Analysis
From the included articles, information was extracted about sample and study characteristics; assessment, informant, and coding characteristics; the prevalence of youth with CD who were diagnosed with the LPE specifier; and the external correlates (“features”) used for group comparison purposes. If the original studies did not report effect sizes, Cohen’s d’s were calculated where possible to get an impression of the magnitude of the significant group differences. The methodological heterogeneity (e.g. the number and kind of co-variates included in the analyses) between studies, unfortunately, hampered a formal meta-analysis.
Results
Sample and Study Characteristics
Table 1 shows that eight studies sampled participants from three different countries (United States: n = 5, Belgium: n = 2, England: n = 1), three different settings (clinical: n = 4; detention/incarceration: n = 2; community: n = 1; mixed: n = 1), and three different age groups (ages 12–18: n = 6; ages 6–11: n = 1; ages 5–18: n = 1). Samples sizes ranged from 43 to 566. Boys or girls were recruited in three and two studies, respectively whereas three studies used mixed-gender samples (boys: 37%–81%). Percentages of ethnic majority youth ranged from 6% to 77%.
Assessment, Informant and Coding Characteristics
Table S1, available online, shows that the Schedule for Affective Disorders and Schizophrenia for School-age children (n = 4) was the most commonly used diagnostic interview to assess CD criteria, followed by the Diagnostic Interview Schedule for Children-IV (DISC-IV: n = 3), and the computerized version of the DISC-IV (n = 1). These interviews were completed by the child in three studies and by both parents and children in five studies. Table 1 (and Table S1, available online) also shows that six studies used only one measure to assess the LPE specifier (APSD: n = 5; ICU: n = 1)], whereas two studies used two measures (APSD and ICU). APSD-based studies used four items to assess the four DSM-5 LPE specifier symptoms (one item for one symptom), whereas the number of ICU items used to construct the LPE measure ranged from four to nine. In four studies these LPE measures were completed by a single informant (child: n = 3; teacher: n = 1), and in four studies by both the parent and the child. Some studies reported results (prevalence and group differences) for various tools, item sets (e.g. four or nine ICU items), and/or informants. All studies took the most extreme responses on the Likert scale to approximate symptom presence (i.e. extreme coding method; e.g. APSD score of 2), though two studies also considered less extreme responses (i.e., less extreme coding method). Because the extreme coding method is used in most studies reviewed here and incorporated in the aforementioned novel clinical assessment system (see introduction), the findings described next focus on analyses that used the extreme coding method, unless otherwise noticed.
Prevalence
In line with expectations, less than 50% (6.1–40%) of the youth with CD met criteria for the DSM-5 LPE specifier when using child self-reports only (Table 2). Two studies also showed that when relying on parent-ratings only or when combining parent- and child self-reports, less than 50% (22.1–49.2%) of CD youth were diagnosed with the DSM-5 LPE specifier (Kahn et al. 2012; Vanwoerden et al. 2016). Yet, there is also evidence that when using teacher- ratings only (Kolko and Pardini 2010) and parent-ratings only (Van Damme et al. 2016), or when combining parent- and child self-report ratings (Sethi et al. 2018; Van Damme et al. 2016), the prevalence was higher than expected (i.e., 50%≤) and ranged from 50.0% to 76.7%. Table 2 demonstrates that studies that relied on child self-ratings and applied the less extreme coding method reported high prevalence rates (50.5–83.7%) (Sakai et al. 2016; Vanwoerden et al. 2016).
Group Differences
Antisocial Behavior
As shown in Table 1, most studies used indices of antisocial behavior (AB) that can be used to test the hypotheses that CD + LPE youth display more severe AB, have an earlier onset, and exhibit a more stable pattern of their AB than CD Only youth (Frick et al. 2014).
Severity of AB: Six studies included measures of severe AB (Colins and Andershed 2015; Hyde et al. 2015; Kahn et al. 2012; Sakai et al. 2016; Vanwoerden et al. 2016; Van Damme et al. 2016). Specifically, the most common index of severe AB in these studies was aggression (n = 5 studies), followed by ODD symptoms or diagnosis (n = 4) SUD diagnoses (n = 3), number of CD symptoms, rule-breaking behavior, violent and non-violent delinquency, and externalizing problems (n = 2), and cruelty and arrest records (n = 1). CD + LPE youth had higher levels of aggression in three studies (Colins and Andershed 2015; Kahn et al. 2012; Van Damme et al. 2016), and a higher level of non-violent delinquency (Colins and Andershed 2015), CD symptoms (Sakai et al. 2016), and cruelty (Kahn et al. 2012) in one study. No other significant group differences were revealed. Two studies also showed that findings might depend on the LPE measure and the informant(s). For example, CD + LPE youth were higher in levels of self-reported aggression when the DSM-5 LPE specifier was assessed by means of the ICU instead of the APSD (Colins and Andershed 2015) or when LPE assessments were based on self-reports only instead of parent-reports only (Colins and Andershed 2015; Kahn et al. 2012).
Onset of AB: One study tested if and showed that CD + LPE youth more often had a childhood-onset CD diagnosis than CD Only youth (Colins and Andershed 2015).
Stability of AB: One study reported that CD + LPE youth exhibited lower levels of future delinquency and had fewer arrest records in adulthood (Hyde et al. 2015). Findings also showed that both groups did not differ in future antisocial personality disorder symptoms and diagnosis, and SUD diagnoses (Hyde et al. 2015).
Personality Features
CD + LPE youth are hypothesized to display lower levels of neuroticism, and, therefore, to display lower levels of anxiety and depression (Frick 2009; Frick et al. 2014).Footnote 2 Altogether, Table 1 shows that four studies that included measures of anxiety and/or depressionFootnote 3 and tested this hypothesis, failed to reveal group differences (Colins and Andershed 2015; Sakai et al. 2016; Van Damme et al. 2016; Vanwoerden et al. 2016). CD + LPE youth are also expected to exhibit higher levels of interpersonal and behavioral/lifestyle psychopathic personality traits (Christian et al. 1997; Frick 2009; Frick et al. 2014). One study tested this expectation and revealed that CD + LPE youth exhibited higher levels behavioral/lifestyle traits, but did not differ from CD Only youth in level of interpersonal traits (Colins and Andershed 2015).
Biological Features
One study included a biological correlate (Table 1). Echoing research on adult psychopathy and consistent with the idea that psychopathy is a neurodevelopmental disorder that originates early in life, this study explored if, but failed to confirm that, CD + LPE youth show microstructural abnormalities in the dorsal ‘default-mode’ network compared to CD Only youth (Sethi et al. 2018).
Treatment Responsiveness
The DSM-5 LPE specifier is hypothesized to designate a group of children and adolescents with CD who are less likely to engage and benefit from treatment (Frick et al. 2014). One study could not reveal group differences in level of treatment engagement (Colins et al. 2017). Another study tested if CD + LPE youth are more likely to exhibit continued problems across multiple domains of functioning following treatment (Kolko and Pardini 2010). Both groups did not differ in any of the 17 post treatment outcomes (e.g., social problems and impairment), with one exception, being that CD + LPE youth were less likely to have a post treatment ADHD diagnosis (Kolko and Pardini 2010). A third study explored change after treatment in a variety of outcomes (Table 1), but could not confirm that CD + LPE youth showed less change than their CD Only counterparts, at least not when using the extreme coding method (Vanwoerden et al. 2016).
Discussion
The aim of this review was to estimate the evidence-base for the DSM-5 LPE specifier whilst relying on studies that assessed this specifier in youth with a CD. Results are discussed first in regard to prevalence followed by a reflection upon group differences (or lack thereof), recommendations for future research, and clinical implications.
Prevalence
The expectation that the DSM-5 LPE specifier delineates a small subgroup of youth with CD was most robustly confirmed when solely relying on child self-ratings of the LPE criteria, with prevalence rates in the 6.1–40% range. When relying on other informants, findings were quite mixed, though. Specifically, with two exceptions (Kahn et al. 2012; Vanwoerden et al. 2016) 50% or more of the youth with CD met criteria for the DSM-5 LPE specifier according to studies that relied on teacher- or parent-ratings only (59.5–76.7%)(Kolko and Pardini 2010; Van Damme et al. 2016), or that combined parent- and child self-reports (49.2–63.5%) (Kahn et al. 2012; Sethi et al. 2018; Van Damme et al. 2016). Admittedly, it can be argued that prevalence rates close to 50%, for examples as those reported in Kahn (49.2%) and Sethi (51.9%) are still in concordance with estimates that up to 50% of children with serious conduct problems exhibit non-normative levels of CU traits. However, these rates should be critically interpreted for at least three reasons. First, findings that approximately 50% of CD youth meet criteria for the DSM-5 specifier are difficult to converge with the idea that this subtyping scheme delineates a small subgroup of youth with CD. Second, there is evidence that CD + LPE youth may be perceived more negatively than CD Only youth (Edens et al. 2017). Therefore, the concern that too many youth with CD are diagnosed with the DSM-5 LPE specifier is particularly salient, though it must be noted that this stigmatizing effect has not yet been replicated (Prasad and Kimonis 2018). Third, CD + LPE youth are often considered to display personality traits and deficits that hallmark adults with psychopathy (Frick 2009; Sethi et al. 2018). Since adult psychopathy has been shown to occur in a minority (e.g. 8–16%) of adults with antisocial personality disorder (Hildebrand and de Ruiter 2004; Pham and Saloppé 2010), DSM-5 LPE prevalence rates do not align with adult prevalence rates of psychopathy, and generally seem high, and, therefore, must be critically and carefully interpreted. Clearly, much work is to be done to illuminate how prevalent the LPE diagnosis truly is among youth with CD.
Group Differences
The studies reviewed here greatly varied in the features used to test the viability of the DSM-5 LPE specifier. The most common features used relate to severity of antisocial behavior, low neuroticism (or lack of anxiety and depression), and treatment responsiveness. Available evidence to some extent supported the idea that CD + LPE youth display more severe antisocial behaviour, though one study actually revealed higher delinquency scores in CD Only youth.Footnote 4 Prior work failed to support the hypotheses that CD + LPE youth are less anxious or depressed (Blair 2013), and responsive to treatment (Frick et al. 2014). Other features of interest were merely considered in one study, making it impossible to draw any conclusion. Consequently, positive findings (e.g., a higher prevalence of childhood-onset CD in CD + LPE youth; Colins and Andershed 2015) and negative findings (e.g., CD + LPE youth were at a lower risk to be arrested in adulthood; Hyde et al. 2015) are in need of replication. Considering the magnitude of the expected significant group differences, all but two of the effect sizes were in the small to moderate range (d < 80). As such, it can be wondered if the significant group differences bear practical usefulness. For now, empirical support for the novel DSM-5 LPE specifier is poor, thereby contrasting the bulk of prior CU research that triggered the incorporation of CU traits into DSM-5 CD.
There are various plausible explanations why studies failed to provide convincing support for the viability of the DSM-5 LPE specifier. A first explanation relates to inaccurate assessments of the DSM-5 LPE specifier that hallmarked all prior work. DSM-5 explicitly states that criteria must be persistently displayed in multiple relationships and settings. Yet, none of the instruments used in the studies that were reviewed, refer to any time frame, relationship, and setting in particular. Thus, available research may have failed to find strong support for the LPE specifier simply and most likely because these studies did not entirely test the LPE specifier as defined in DSM-5. However, this is how evidence was gathered to propose the LPE specifier in the first place. Thus, it stands to reason to argue that it should work in independent investigations as well. Nevertheless, prior attempts in the literature to take a few items from existing measures of CU traits and construct an LPE measure do not seem very successful. Therefore, future research on the DSM-5 LPE specifier should consider alternative, better, and more comprehensive ways to test this specifier. From this perspective, interview-based assessment tools, such as the CAPE, are very much welcomed, but still awaiting in-depth scrutiny. Interestingly, the first available study that explored this CAPE’s psychometric properties revealed some promising findings in a small sample of youth from families with a low socioeconomic status (Centifanti et al. 2019). Nevertheless, it is relevant to note that this study did not consider CD diagnosis and reported findings that contrast common expectations surrounding the DSM-5 LPE specifier.Footnote 5 A second study that explored the psychometric properties of the CAPE, reported group comparisons between children and adolescents with ODD or CD who met DSM-5 criteria for the DSM-5 specifier (ODD/CD + LPE; n = 20) and who did not (n = 34) (Hawes et al. 2019).Footnote 6 Both groups did not significantly differ in antisocial behavior and proactive aggression, though the ODD/CD + LPE group displayed significantly lower levels of affective empathy (d = .70). Consequently, interview-based studies among CD youths are urgently warranted to see if better assessment will increase support for this novel CD subtyping scheme. Alternatively, clinicians might already use the DSM-5 LPE specifier for applied purposes since the publication of DSM-5 in 2013, and rely on unstandardized assessments of the LPE specifier. Therefore, future studies might use file information to test if CD + LPE and CD Only groups differ from each other when LPE diagnoses were provided by clinicians in applied settings.
A second explanation relates to the features that have been considered in available DSM-5 LPE specifier studies. Research on CU traits have considered genetic, cognitive, emotional, biological, environmental, and personality features, along with antisocial behavior and treatment responsiveness (Frick et al. 2014). Yet, as shown in Table 1, prior work on the DSM-5 LPE specifier merely focused on a restricted number of features, while some features were merely considered in one study, such as the onset and stability of antisocial behavior, psychopathic personality traits, or brain activation. Unfortunately, no study to date considered features that quite consistently have been associated with CU traits, such as responsiveness to and recognition of cues to fear and sadness in others (i.e. emotional features), abnormalities in the processing of punishment cues (i.e. cognitive features), harsh and warm parenting (i.e. environmental features), and amygdala deficits (i.e. biological features) (Frick et al. 2014). Speculative, it is possible that support for the LPE specifier is currently limited because various important features have not yet been considered.
Third, diagnostic assessment of children emphasizes information from multiple informants (Handwerk et al. 1999), and, therefore, clinicians typically also resort to descriptions of children and adolescent by others. In regard of the LPE specifier, DSM-5 explicitly states that self-report of LPE must be complemented with information from others, who have known the individual for extended periods of time, such as parents, teachers, co-workers, and peers (APA 2013). What is clear from the present review is that most studies on the DSM-5 LPE specifier reviewed here relied on child reports, which might have diminished support for the LPE specifier. Though not impossible, it is important to keep in mind that three of the four studies that were used in the development of the LPE specifier solely relied on child reports (Frick and Moffitt 2010) and that proponents of the LPE specifier considered child report as an important source of information to put the LPE specifier to the test (Kimonis et al. 2015). That is, these were standards used to design, propose, and include the LPE specifier, so self-report only studies should be sufficiently robust to test the LPE specifier. Put differently, the overreliance on child self-reports can and should not be used to discard prior work on the DSM-5 LPE specifier, especially not since there is evidence to suggest that extending child with parent-reports does not necessarily increase support for the LPE specifier (Vanwoerden et al. 2016; Van Damme et al. 2016; Kahn et al. 2012) and might result in very high prevalence rates of children and adolescents who met criteria for the DSM-5 LPE specifier (supra).
Recommendations for Future Research
Assessment of the DSM-5 LPE specifier should remain a major focus in future work. The current review clearly shows that attempts in the past decade to take a few items from existing measures of CU traits and construct a LPE measure have not been successful. Future studies that systematically use interview-based tools to test the viability of the LPE specifier among children and adolescents with CD may greatly enhance research on the DSM-5 LPE specifier. Using such interviews will be time consuming, costly, and much more complex as compared to using a restricted number of items from excising CU measures. Hence, it will be relevant to test if these interviews provides important information above and beyond prior attempts in the literature to construct an LPE measure (Centifanti et al. 2019).
Future studies that gather information from different informants are needed to assess the LPE specifier as recommended by DSM-5. Yet, including multiple informants inevitably confronts clinicians and researchers with the question how to deal with these multiple sources. Studies that relied on multiple informant-reports greatly differed in the way these reports were combined, not only to measure CD (Table S1, available online) but also to measure the DSM-5 LPE specifier (Table 1), and often yielded prevalence rates of LPE among children and adolescents with CD that seem too high. Therefore, systematic research on this particular topic is needed and may result in recommendations on how information from multiple sources should be combined. Such endeavors may eventually show that certain informants in certain settings are less accurate reporters of LPE specifier criteria (e.g., parents from detained youth). This would imply that information from different reporters should be weighted differently, and, consequently, that using the commonly applied highest score prevails method or OR-rule might not (always) be the best way to combine information from different reporters. However, nothing is known about how to weight the different sources, even though it is likely that different sources deserve different weights.
The LPE specifier may work less well in a context in which the assessment of the LPE specifier may bring actual consequences to the reporter (Kimonis et al. 2014). All studies reviewed here were performed in a research context, and thus guaranteed anonymity and confidentiality to its participants. Therefore, it is particularly worrisome that evidence in support of the LPE specifier stemming, overall, is poor, even though the assessment methods were less than optimal. Clearly, studies are needed to illuminate how well the LPE specifier works in clinical practice, for example, by means of comprehensive standardized measurement tools, such as interviews.
Clinical Implications
For now, available work strongly suggests that clinicians should not yet use the DSM-5 LPE specifier for diagnostic purposes and treatment planning, at least not when relying on items from CU measures that have been used in the development of the four LPE specifier criteria. Clinicians are also recommended not to use the LPE specifier for prognostic purposes, especially since the few prospective studies demonstrated that children with CD who were diagnosed with the LPE specifier were not at an increased risk for future criminality and poor treatment outcomes.
Notes
Because the main diagnostic criteria of CD remained unchanged in the DSM–5, studies that assessed DSM-IV CD are equally valid to assess DSM–5 CD.
For example, because youth with conduct problems who do not exhibit CU traits have vulnerabilities involving problems regulating emotions, leading to higher levels of depression, anger, and anxiety (Frick 2009).
One other study also measured internalizing problems, but focused on another research question (i.e. post treatment outcomes) and did not compare both groups in baseline levels of internalizing problems (Kolko & Pardini, 2010).
While the current paper was under review, one additional study would have been included if our search strategy was performed in January 2020, instead of January 2019 (see Method, Selection). This study recruited 264 children (Mage = 8.5; 40.5% girls) who received school-based psychosocial problems for conduct problems (Dery et al. 2019). Of the 103 children with a CD diagnosis as measured by the DISC (parents or teacher), 48 (46.6%) met criteria for the DSM-5 LPE specifier as measured by the APSD (extreme coding, teacher or parent). Group comparisons revealed only one significant difference in the presence of 15 specific CD symptoms (i.e. used weapon to cause harm; CD + LPE > CD Only; d = 0.48), whilst CD + LPE children also displayed higher levels of ADHD symptoms. No significant differences were reported in levels of ODD symptoms, total number of aggressive CD symptoms, total number of CD symptoms, and stability of conduct problems over time.
For example, children who met and did not meet criteria for the DSM-5 LPE specifier did not significantly differ in externalizing and internalizing problems and risk for violence.
This study, as well as the aforementioned Centifanti study (2019), became available after January 2019 (see Method, Selection). Yet, both studies would not have been included because of our inclusion criteria. The Centifanti et al. (2019) study did not consider a CD diagnosis, whilst the Hawes et al. (2019) study did not differentiate between an ODD and CD diagnosis when testing the LPE specifier.
References
Andershed, H., Kerr, M., Stattin, H., & Levander, S. (2002). Psychopathic traits in non-referred youths: Initial test of a new assessment tool. In E. Blaauw & L. Sheridan (Eds.), Psychopaths: Current international perspectives (pp. 131–158). The Hague: Elsevier.
APA (2013). Diagnostic and Statistical Manual of Mental Disorders (4ed.). Washington DC: American Psychiatric Publishing.
Blair, R. J. (2013). The neurobiology of psychopathic traits in youths. Nature Reviews Neuroscience, 14(11), 786–799.
Byrd, A. L., Hawes, S. W., Burke, J. D., Loeber, R., & Pardini, D. A. (2018). Boys with conduct problems and callous-unemotional traits: Neural response to reward and punishment and associations with treatment response. Developmental Cognitive Neuroscience, 30, 51–59.
Centifanti, L. C., Shaw, H., Atherton, K. J., Thomson, N. D., MacLellan, S., & Frick, P. J. (2019). CAPE for measuring callous-unemotional traits in disadvantaged families: A cross-sectional validation study. F1000Research; 8(1027).
Chinn, S. (2000). A simple method for converting an odds ratio to effect size for use in meta-analysis. Statistics in Medicine, 19(22), 3127–3131.
Christian, R. E., Frick, P. J., Hill, N. L., Tyler, L., & Frazer, D. R. (1997). Psychopathy and conduct problems in children: II. Implications for subtyping children with conduct problems. Journal of the American Academy of Child & Adolescent Psychiatrty, 36(2), 233–241.
Colins, O. F. (2016). The clinical usefulness of the DSM-5 specifier for conduct disorder outside of a research context. Law and Human Behavior, 40(3), 310–318.
Colins, O. F., & Andershed, H. (2015). The DSM-5 with limited Prosocial emotions Specifier for conduct disorder among detained girls. Law and Human Behavior, 39(2), 198–207.
Colins, O. F., & Vermeiren, R. R. J. (2013). The usefulness of DSM-IV and DSM-5 conduct disorder subtyping in detained adolescents. Journal of Nervous and Mental Disease, 201(9), 736–743.
Colins, O. F., Andershed, H., Frogner, L., Lopez-Romero, L., Veen, V., & Andershed, A.-K. (2014). A new measure to assess psychopathic personality in children: The child problematic traits inventory. Journal of Psychopathology and Behavioral Assessment, 36, 4–21.
Colins, O. F., Van Damme, L., Fanti, K. A., & Andershed, H. (2017). The prospective usefulness of callous-unemotional traits and conduct disorder in predicting treatment engagement among detained girls. European Child & Adolescent Psychiatry, 26(1), 75–85.
Dadds, M. R., Salmon, K. J. C. C., & review, f. p. (2003). Punishment insensitivity and parenting: Temperament and learning as interacting risks for antisocial behavior. Clinical Child & Family Psychology Review, 6(2), 69–86.
Dadds, M. R., Allen, J. L., McGregor, K., Woolgar, M., Viding, E., Scott, S., et al. (2014). Callous-unemotional traits in children and mechanisms of impaired eye contact during expressions of love: A treatment target? Journal of Child Psychology & Psychiatry, 55(7), 771–780.
Déry, M., Bégin, V., Toupin, J., & Temcheff, C. (2019). Clinical utility of the limited Prosocial emotions Specifier in the childhood-onset subtype of conduct disorder. The Canadian Journal of Psychiatry, 64(12), 838–845.
Edens, J. F., Mowle, E. N., Clark, J. W., & Magyar, M. S. (2017). “A psychopath by any other name?”: Juror perceptions of the DSM-5 “limited Prosocial emotions” Specifier. Journal of Personality Disorders, 31(1), 90–109.
Fanti, K. A., Panayiotou, G., Lazarou, C., Michael, R., & Georgiou, G. (2016). The better of two evils? Evidence that children exhibiting continuous conduct problems high or low on callous-unemotional traits score on opposite directions on physiological and behavioral measures of fear. Development and Psychopathology, 28(1), 185–198.
Frick, P. J. (2003). The inventory of callous-unemotional traits. Unpublished rating scale. University of New Orleans.
Frick, P. J. (2009). Extending the construct of psychopathy to youth: Implications for understanding, diagnosing, and treating antisocial children and adolescents. The Canadian Journal of Psychiatry, 54(12), 803–812.
Frick, P. J. (2013). Clinical assessment of prosocial emotions: Version 1.1 (CAPE 1.1). University of New Orleans.
Frick, P. J., & Hare, R. D. (2001). Antisocial process screening device: APSD: Multi-health systems Toronto.
Frick, P. J., & Moffitt, T. E. (2010). A proposal to the DSM-V childhood disorders and the ADHD and disruptive behavior disorders work groups to include a Specifier to the diagnosis of conduct disorder based on the presence of callous-unemotional traits.
Frick, P. J., & White, S. F. (2008). Research review: The importance of callous-unemotional traits for developmental models of aggressive and antisocial behavior. Journal of Child Psychology & Psychiatry, 49(4), 359–375.
Frick, P. J., Ray, J. V., Thornton, L. C., & Kahn, R. E. (2014). Can callous-unemotional traits enhance the understanding, diagnosis, and treatment of serious conduct problems in children and adolescents? A comprehensive review. Psychologicl Bulletin, 140(1), 1–57.
Handwerk, M. L., Larzelere, R. E., Soper, S. H., & Friman, P. C. (1999). Parent and child discrepancies in reporting severity of problem behaviors in three out-of-home settings. Psychological Assessment, 11(1), 14–23.
Hawes, D. J., Kimonis, E. R., Mendoza Diaz, A., Frick, P. J., & Dadds, M. R. (2019) (advanced online, 2019, December 12). The clinical assessment of Prosocial emotions (CAPE 1.1): A multi-informant validation study. Psychological Assessment.
Hildebrand, M., & de Ruiter, C. J. (2004). PCL-R psychopathy and its relation to DSM-IV Axis I and II disorders in a sample of male forensic psychiatric patients in the Netherlands. International Journal of Law & Psychiatry, 27(3), 233–248.
Hyde, L. W., Burt, S. A., Shaw, D. S., Donnellan, M. B., & Forbes, E. E. (2015). Early starting, aggressive, and/or callous-unemotional? Examining the overlap and predictive utility of antisocial behavior subtypes. Journal of Abnormal Psychololgy, 124(2), 329–342.
Jambroes, T., Jansen, L. M., Vermeiren, R. R., Doreleijers, T. A., Colins, O. F., & Popma, A. (2016). The clinical usefulness of the new LPE specifier for subtyping adolescents with conduct disorder in the DSM 5. European Child & Adolescent Psychiatry, 25(8), 891–902.
Kahn, R. E., Frick, P. J., Youngstrom, E., Findling, R. L., & Youngstrom, J. K. (2012). The effects of including a callous-unemotional specifier for the diagnosis of conduct disorder. Journal of Child Psychology & Psychiatry, 53(3), 271–282.
Kimonis, E. R., Fanti, K. A., Goldweber, A., Marsee, M. A., Frick, P. J., & Cauffman, E. (2014). Callous-unemotional traits in incarcerated adolescents. Psychological Assessment, 26(1), 227–237.
Kimonis, E. R., Fanti, K. A., Frick, P. J., Moffitt, T. E., Essau, C., Bijttebier, P., & Marsee, M. A. (2015). Using self-reported callous-unemotional traits to cross-nationally assess the DSM-5 'With limited Prosocial Emotions' specifier. Journal of Child Psychology & Psychiatry, 56(11), 1249–1261.
Kolko, D. J., & Pardini, D. (2010). ODD dimensions, ADHD, and callous–unemotional traits as predictors of treatment response in children with disruptive behavior disorders. Journal of Abnormal Psychology, 119(4), 713–725.
McMahon, R. J., Witkiewitz, K., & Kotler, J. S. (2010). Predictive validity of callous-unemotional traits measured in early adolescence with respect to multiple antisocial outcomes. Journal of Abnormal Psychology, 119(4), 752–763.
Oldenhof, H., Prätzlich, M., Ackermann, K., Baker, R., Batchelor, M., Baumann, S., et al. (2018). Baseline autonomic nervous system activity in female children and adolescents with conduct disorder: Psychophysiological findings from the FemNAT-CD study. Journal of Criminal Justice.
Pardini, D., Stepp, S., Hipwell, A., Stouthamer-Loeber, M., & Loeber, R. (2012). The clinical utility of the proposed DSM-5 callous-unemotional subtype of conduct disorder in young girls. Journal of the Americal Academy for Child & Adolescent Psychiatry, 51(1), 62–73.
Pechorro, P., Jimenez, L., Hidalgo, V., & Nunes, C. (2015). The DSM-5 limited Prosocial emotions subtype of conduct disorder in incarcerated male and female juvenile delinquents. International Journal of Law & Psychiatry, 39, 77–82.
Pham, T. H., & Saloppé, X. J. (2010). PCL-R psychopathy and its relation to DSM Axis I and II disoders in a sample of male forensic patients in a Belgian security hospital. International Journal of Law & Psychiatry, 9(3), 205–214.
Prasad, A. H., & Kimonis, E. R. (2018). Effects of the “limited Prosocial emotions” Specifier for conduct disorder on juror perceptions of juvenile offenders. Criminal Justice and Behavior.
Rowe, R., Maughan, B., Moran, P., Ford, T., Briskman, J., & Goodman, R. (2010). The role of callous and unemotional traits in the diagnosis of conduct disorder. Journal of Child Psychology & Psychiatry, 51(6), 688–695.
Sakai, J. T., Mikulich-Gilbertson, S. K., Young, S. E., Rhee, S. H., McWilliams, S. K., Dunn, R., et al. (2016). Adolescent male conduct-disordered patients in substance use disorder treatment: Examining the "limited Prosocial emotions" Specifier. Journal of Child & Adolescent Substance Abuse, 25(6), 613–625.
Sakai, J. T., Dalwani, M. S., Mikulich-Gilbertson, S. K., Raymond, K., McWilliams, S., Tanabe, J., et al. (2017). Imaging decision about whether to benefit self by harming others: Adolescents with conduct and substance problems, with or without callous-unemotionality, or developing typically. Psychiatry Research, 263, 103–112.
Sarkar, S., Craig, M., Catani, M., Dell'Acqua, F., Fahy, T., Deeley, Q., et al. (2013). Frontotemporal white-matter microstructural abnormalities in adolescents with conduct disorder: A diffusion tensor imaging study. Psychological Medicine, 43(2), 401–411.
Schwenck, C., Mergenthaler, J., Keller, K., Zech, J., Salehi, S., Taurines, R., Romanos, M., Schecklmann, M., Schneider, W., Warnke, A., & Freitag, C. M. (2012). Empathy in children with autism and conduct disorder: Group-specific profiles and developmental aspects. Journal of Child Psychology & Psychiatry, 53(6), 651–659.
Sethi, A., Sarkar, S., Dell’Acqua, F., Viding, E., Catani, M., Murphy, D. G., et al. (2018). Anatomy of the dorsal default-mode network in conduct disorder: Association with callous-unemotional traits. Developmental Cognitive Neuroscience, 30, 87–92.
Van Damme, L., Colins, O. F., & Vanderplasschen, W. (2016). The limited Prosocial emotions Specifier for conduct disorder among detained girls: A multi-informant approach. Criminal Justice and Behavior, 43(6), 778–792.
Vanwoerden, S., Reuter, T., & Sharp, C. (2016). Exploring the clinical utility of the DSM-5 conduct disorder specifier of 'with limited prosocial emotions' in an adolescent inpatient sample. Comprehensive Psychiatry, 69, 116–131.
Funding
Open access funding provided by Örebro University. This work was partially supported by an FWO Odysseus Grant (FWO.ODY.2019.0001.01) awarded to the first author.
Author information
Authors and Affiliations
Contributions
O.F.C. had the idea for and drafted the review paper, O.F.C. and L.V.D. performed the literature search and data analysis, and all authors critically revised the work.
Corresponding author
Ethics declarations
This article does not contain any studies with human participants performed by any of the authors.
Conflict of Interest
Olivier F. Colins declares that he has no conflict of interest. Lore Van Damme declares that she has no conflict of interest. Anne Hendriks declares that she has no conflict of interest. Giorgos Georgiou declarers that he has no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Colins, O.F., Van Damme, L., Hendriks, A.M. et al. The DSM-5 with Limited Prosocial Emotions Specifier for Conduct Disorder: a Systematic Literature Review. J Psychopathol Behav Assess 42, 248–258 (2020). https://doi.org/10.1007/s10862-020-09799-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10862-020-09799-3