
Abstract
Background
Radiofrequency (RF) catheter ablation for persistent atrial fibrillation (peAF) is associated with less favorable outcomes than for paroxysmal AF (PAF). Recent studies have shown improved clinical outcomes with use of ablation index (AI) targets for pulmonary vein isolation (PVI) in PAF. AI is a novel ablation quality marker that incorporates contact force (CF), time, and power in a weighted formula. This is a single-arm registry to investigate the 1-year efficacy of AF ablation guided by the AI in patients with peAF, and further to evaluate pulmonary vein reconduction at repeat electrophysiology study in case of recurrent AF.
Methods
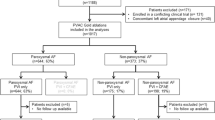
In total, 55 consecutive patients (69 ± 10 years, 55% male, median time since first AF diagnosis: 31 months (Q1–Q3: 10–70)) with peAF underwent AIguided PVI using a CF surround-flow catheter. AI targets were 600 for anterior and 450 for roof/posterior/inferior antral segments. Patients were monitored for atrial tachyarrhythmia recurrence using 5-day Holter-ECG recordings at 3, 6, and 12 months.
Results
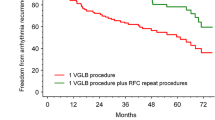
The median procedure time was 173 min (Q1–Q3: 152–204). The median fluoroscopy time was 4 min (Q1–Q3: 3–6) and the median fluoroscopy dose was 2.64 Gy/cm2 (Q1–Q3: 1.04–3.99). The median ablation time was 57 min (Q1–Q3: 47–63). At 12 months, 42% of the patients were in sinus rhythm. AF recurrence was seen in 58% of patients. No major complications occurred.
Conclusions
RF ablation using AI in peAF is a feasible and safe technique. At 1 year, AI-guided ablation was associated with AF recurrence in 58% of the patients.



Similar content being viewed by others
References
Kirchhof P, Breithardt G, Bax J, Benninger G, Blomstrom-Lundqvist C, Boriani G, et al. A roadmap to improve the quality of atrial fibrillation management: proceedings from the fifth Atrial Fibrillation Network/European Heart Rhythm Association consensus conference. Europace. 2016;18:37–50.
Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace. 2016;18:1609–78.
Arbelo E, Brugada J, Blomström-Lundqvist C, Laroche C, Kautzner J, Pokushalov E, et al. on TBOTESC-EHRAAFAL-tRI. Contemporary management of patients undergoing atrial fibrillation ablation: in-hospital and 1-year follow-up findings from the ESC-EHRA atrial fibrillation ablation long-term registry. Eur Heart J. 2017;38:1303–16.
Providência R, Lambiase PD, Srinivasan N, Ganesh Babu G, Bronis K, Ahsan S, et al. Is there still a role for complex fractionated atrial electrogram ablation in addition to pulmonary vein isolation in patients with paroxysmal and persistent atrial fibrillation? Meta-Analysis of 1415 Patients. Circ Arrhythm Electrophysiol. 2015;8:1017–29.
Scott PA, Silberbauer J, Murgatroyd FD. The impact of adjunctive complex fractionated atrial electrogram ablation and linear lesions on outcomes in persistent atrial fibrillation: a meta-analysis. Europace. 2016;18:359–67.
Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372:1812–22.
Kautzner J, Neuzil P, Lambert H, Peichl P, Petru J, Cihak R, et al. EFFICAS II: optimization of catheter contact force improves outcome of pulmonary vein isolation for paroxysmal atrial fibrillation. Europace. 2015;17:1229–35.
Neuzil P, Reddy VY, Kautzner J, Petru J, Wichterle D, Shah D, et al. Electrical reconnection after pulmonary vein isolation is contingent on contact force during initial treatment: results from the EFFICAS I study. Circ Arrhythm Electrophysiol. 2013;6:327–33.
Conti S, Weerasooriya R, Novak P, Champagne J, Lim HE, Macle L, et al. Contact force sensing for ablation of persistent atrial fibrillation: a randomized, multicenter trial. Heart Rhythm. 2018;15:201–8.
Coeman M, Haddad ME, Wol M, Choudhury R, Vandekerckhove Y, Choudhury R, et al. ‘CLOSE’-guided pulmonary vein isolation and changes in local bipolar and unipolar atrial electrograms: observations from the EP lab. J Atr Fibrillation. 2018;10:1794.
Taghji P, El Haddad M, Phlips T, Wolf M, Knecht S, Vandekerckhove Y, et al. Evaluation of a strategy aiming to enclose the pulmonary veins with contiguous and optimized radiofrequency lesions in paroxysmal atrial fibrillation: a pilot study. JACC Clin Electrophysiol. 2018;4:99–108.
El Haddad M, Taghji P, Phlips T, Wolf M, Demolder A, Choudhury R, et al. Determinants of acute and late pulmonary vein reconnection in contact force-guided pulmonary vein isolation: identifying the weakest link in the ablation chain. Circ Arrhythm Electrophysiol. 2017;10.
Phlips T, Taghji P, El Haddad M, Wolf M, Knecht S, Vandekerckhove Y, et al. Improving procedural and one-year outcome after contact force-guided pulmonary vein isolation: the role of interlesion distance, ablation index, and contact force variability in the ‘CLOSE’-protocol. Europace. 2018;20:f419–27.
Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, et al. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace. 2012;14:528–606.
Stabile G, Di Donna P, Schillaci V, Di Monaco A, Iuliano A, Caponi D, et al. Safety and efficacy of pulmonary vein isolation using a surround flow catheter with contact force measurement capabilities: a multicenter registry. J Cardiovasc Electrophysiol. 2017;28:762–7.
Solimene F, Schillaci V, Shopova G, Urraro F, Arestia A, Iuliano A, et al. Safety and efficacy of atrial fibrillation ablation guided by Ablation Index module. J Interv Card Electrophysiol. 2018.
Das M, Loveday JJ, Wynn GJ, Gomes S, Saeed Y, Bonnett LJ, et al. Ablation index, a novel marker of ablation lesion quality: prediction of pulmonary vein reconnection at repeat electrophysiology study and regional differences in target values. Europace. 2017;19:775–83.
Hussein A, Das M, Riva S, Morgan M, Ronayne C, Sahni A, et al. Use of ablation index-guided ablation results in high rates of durable pulmonary vein isolation and freedom from arrhythmia in persistent atrial fibrillation patients. Circ Arrhythm Electrophysiol. 2018;11:e006576.
Willems S, Khairy P, Andrade JG, Hoffmann BA, Levesque S, Verma A, et al. Redefining the blanking period after catheter ablation for paroxysmal atrial fibrillation: insights from the ADVICE (adenosine following pulmonary vein isolation to target dormant conduction elimination) trial. Circ Arrhythm Electrophysiol. 2016;9.
De Pooter JST, El Haddad M, Wolf M, Phlips T, Vandekerckhove Y, Tavernier R, et al. Pulmonary vein reconnection no longer occurs in the majority of patients after a single pulmonary vein isolation procedure. J Am Coll Cardiol EP. 2019.
Fink T, Schlüter M, Heeger CH, Lemes C, Maurer T, Reissmann B, Riedl J, Rottner L, Santoro F, Schmidt B, Wohlmuth P, Mathew S, Sohns C, Ouyang F, Metzner A, Kuck KH. Stand-alone pulmonary vein isolation versus pulmonary vein isolation with additional substrate modification as index ablation procedures in patients with persistent and long-standing persistent atrial fibrillation: the randomized Alster-Lost-AF trial (ablation at St. Georg Hospital for long-standing persistent atrial fibrillation). Circ Arrhythm Electrophysiol. 2017;10
Ho SY, Cabrera JA, Sanchez-Quintana D. Left atrial anatomy revisited. Circ Arrhythm Electrophysiol. 2012;5:220–8.
Iso K, Okumura Y, Watanabe I, Nagashima K, Sonoda K, Kogawa R, et al. Wall thickness of the pulmonary vein-left atrial junction rather than electrical information as the major determinant of dormant conduction after contact force-guided pulmonary vein isolation. J Interv Card Electrophysiol. 2016;46:325–33.
Cabrera JA, Ho SY, Climent V, Fuertes B, Murillo M, Sánchez-Quintana D. Morphological evidence of muscular connections between contiguous pulmonary venous orifices: relevance of the interpulmonary isthmus for catheter ablation in atrial fibrillation. Heart Rhythm. 2009;6:1192–8.
Yoshida K, Baba M, Shinoda Y, Harunari T, Tsumagari Y, Koda N, et al. Epicardial connection between the right-sided pulmonary venous carina and the right atrium in patients with atrial fibrillation: a possible mechanism for preclusion of pulmonary vein isolation without carina ablation. Heart Rhythm. 2019;16:671–8.
Reddy VY, Sediva L, Petru J, Skoda J, Chovanec M, Chitovova Z, et al. Durability of pulmonary vein isolation with cryoballoon ablation: results from the Sustained PV Isolation with Arctic Front Advance (SUPIR) study. J Cardiovasc Electrophysiol. 2015;26:493–500.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Each patient provided written informed consent. The principle outlined in the latest update of the Declaration of Helsinki was followed. The local ethical committee of the University Witten/Herdecke approved this study (133/2020).
Conflict of interest
Ute Ruprecht is a consultant for Biosense Webster. Kars Neven reported having received speaker fees from Biosense Webster, Inc. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Reinsch, N., Füting, A., Buchholz, J. et al. One-year outcome and durability of pulmonary vein isolation after prospective use of ablation index for catheter ablation in patients with persistent atrial fibrillation. J Interv Card Electrophysiol 62, 143–151 (2021). https://doi.org/10.1007/s10840-020-00880-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00880-1