
Abstract
Purpose
Pulmonary vein isolation (PVI) by catheter ablation has reduced efficacy for the treatment of persistent atrial fibrillation (persAF), as compared to paroxysmal atrial fibrillation (paroxAF). We investigated whether the selection of persAF patients for PVI who “step back” to the paroxysmal stage on amiodarone offers a success rate comparable to that of patients with paroxAF.
Methods
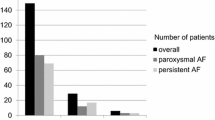
Sixty-two consecutive persAF patients and 62 matched control patients with paroxAF were included. Persistent patients were started on amiodarone and cardioverted to sinus rhythm (SR). PVI was performed after 3 months in those who “stepped back” and had sustained SR and in all paroxAF patients.
Results
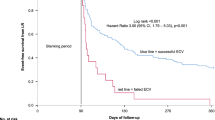
Five of the 62 (8%) study patients returned to persAF after cardioversion; despite amiodarone, they did not undergo PVI. The rest received PVI and was followed for a mean of 31 ± 14 months. Redo procedures were performed in 44% and 29% in the persAF and paroxAF group (p = 0.093), respectively. The recurrence rate after multiple procedures without antiarrhythmic drugs was similar among the persAF and paroxAF patients (11% and 7%) at 6 months (p = 0.510), but increased in the persAF group at 1 year (21% and 9%, p = 0.065) and exceeded that of the paroxAF group at the end of the follow-up (26% and 12%, p = 0.046). Kaplan-Meier survival analysis showed shorter time to recurrence in the persAF group (p = 0.045).
Conclusion
PersAF patients who “step back” to the paroxysmal stage on amiodarone can expect long-term success of a PVI-only strategy in more than 70% of the time. However, late recurrences are more common compared to paroxAF.


Similar content being viewed by others

References
Parkash R, Tang AS, Sapp JL, Wells G. Approach to the catheter ablation technique of paroxysmal and persistent atrial fibrillation: a meta-analysis of the randomized controlled trials. J Cardiovasc Electrophysiol. 2011;22(7):729–38.
Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10):659–66.
Nattel S, Burstein B, Dobrev D. Atrial remodeling and atrial fibrillation: mechanisms and implications. Circ Arrhythm Electrophysiol. 2008;1(1):62–73.
Padfield GJ, Steinberg C, Swampillai J, Qian H, Connolly SJ, Dorian P, et al. Progression of paroxysmal to persistent atrial fibrillation: 10-year follow-up in the Canadian Registry of Atrial Fibrillation. Heart Rhythm. 2017 Jun;14(6):801–7.
Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372(19):1812–22.
Miyazaki S, Kuwahara T, Kobori A, Takahashi Y, Takei A, Sato A, et al. Pharmacological cardioversion preceding left atrial ablation: bepridil predicts the clinical outcome following ablation in patients with persistent atrial fibrillation. Europace. 2009;11:1620–3.
Igarashi M, Tada H, Sekiguchi Y, Yamasaki H, Arimoto T, Kuroki K, et al. Effect of restoration of sinus rhythm by extensive antiarrhythmic drugs in predicting results of catheter ablation of persistent atrial fibrillation. Am J Cardiol. 2010;106(1):62–8.
Shinagawa K, Shiroshita-Takeshita A, Schram G, Nattel S. Effects of antiarrhythmic drugs on fibrillation in the remodeled atrium: insights into the mechanism of the superior efficacy of amiodarone. Circulation. 2003;107(10):1440–6.
Ashikaga K, Kobayashi T, Kimura M, Owada S, Sasaki S, Iwasa A, et al. Effects of amiodarone on electrical and structural remodeling induced in a canine rapid pacing-induced persistent atrial fibrillation model. Eur J Pharmacol. 2006;536(1–2):148–53.
Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893–962.
Slotwiner D, Steinberg J. Limited ablation for persistent atrial fibrillation using preprocedure reverse remodelling. Arrhythm Electrophysiol Rev. 2014;3(2):101–6
Khan A, Mittal S, Kamath GS, Garikipati NV, Marrero D, Steinberg JS. Pulmonary vein isolation alone in patients with persistent atrial fibrillation: an ablation strategy facilitated by antiarrhythmic drug induced reverse remodeling. J Cardiovasc Electrophysiol. 2011;22(2):142–8.
Gökoğlan Y, Mohanty S, Güneş MF, Trivedi C, Santangeli P, Gianni C, et al. Pulmonary vein antrum isolation in patients with paroxysmal atrial fibrillation: more than a decade of follow-up. Circ Arrhythm Electrophysiol. 2016;9(5):e003660.
Andrade JG, Monir G, Pollak SJ, Khairy P, Dubuc M, Roy D, et al. Pulmonary vein isolation using contact force ablation: the effect on dormant conduction and long-term freedom from recurrent atrial fibrillation—a prospective study. Heart Rhythm. 2014;11:1919–24.
Marijon E, Fazaa S, Narayanan K, et al. Real-time contact force sensing for pulmonary vein isolation in the setting of paroxysmal atrial fibrillation: procedural and 1-year results. J Cardiovasc Electrophysiol. 2014;25:130–7.
Zhang Z, Letsas KP, Zhang N, Efremidis M, Xu G, Li G, et al. Linear ablation following pulmonary vein isolation in patients with atrial fibrillation: a meta-analysis. Pacing Clin Electrophysiol. 2016;39(6):623–30.
Scott PA, Silberbauer J, Murgatroyd FD. The impact of adjunctive complex fractionated atrial electrogram ablation and linear lesions on outcomes in persistent atrial fibrillation: a meta-analysis. Europace. 2016;18(3):359–67.
Fink T, Schlüter M, Heeger CH, Lemes C, Maurer T, Reissmann B, Riedl J, Rottner L, Santoro F, Schmidt B, Wohlmuth P, Mathew S, Sohns C, Ouyang F, Metzner A, Kuck KH. Stand-alone pulmonary vein isolation versus pulmonary vein isolation with additional substrate modification as index ablation procedures in patients with persistent and long-standing persistent atrial fibrillation: the randomized Alster-lost-AF trial (ablation at St. Georg Hospital for Long-Standing Persistent Atrial Fibrillation). Circ Arrhythm Electrophysiol 2017;10(7). https://doi.org/10.1161/CIRCEP.117.005114.
Dixit S, Marchlinski FE, Lin D, Callans DJ, Bala R, Riley MP, et al. Randomized ablation strategies for the treatment of persistent atrial fibrillation: RASTA study. Circ Arrhythm Electrophysiol. 2012;5(2):287–94.
Vogler J, Willems S, Sultan A, Schreiber D, Lüker J, Servatius H, et al. J Am Coll Cardiol. 2015;66(24):2743–52.
Bassiouny M, Saliba W, Hussein A, Rickard J, Diab M, Aman W, et al. Randomized study of persistent atrial fibrillation ablation: ablate in sinus rhythm versus ablate complex-fractionated atrial electrograms in atrial fibrillation. Circ Arrhythm Electrophysiol. 2016;9(2):e003596.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was provided according to institutional protocols.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Benák, A., Kohári, M., Herczeg, A. et al. Selecting persistent atrial fibrillation patients for pulmonary vein isolation based on the response to amiodarone: efficacy of the “one step back” strategy. J Interv Card Electrophysiol 56, 291–297 (2019). https://doi.org/10.1007/s10840-019-00524-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-019-00524-z