
Abstract
Adverse childhood experiences (ACEs) are prevalent across the globe. They have been associated with a range of demographic characteristics and poor outcomes throughout the life course, however, little is known of the Australian context. We aimed to estimate the prevalence of ACEs in an Australian sample and identify demographic characteristics of children who experience adversity. We used data from the National Health Survey Australia 2014–15 to explore adversities experienced by children (aged 0–17) living with the 4161 adult respondents. Three types of adversity were examined: living with only one parent, parental mental health condition, and parental substance use problem. Bivariate associations and hierarchical multiple regression analyses were used to investigate the relationships between the number of adversities reported and demographic characteristics. At least one-third of children had experienced one or more adversities, and almost 8% had experienced multiple adversities. Adversity was reported by respondents across all categories of demographic variables. The experience of adversity was significantly related to demographic characteristics measured at the level of geographic area, household, and individual. Adversity may be affecting at least one-third of Australian children, across a broad range of contexts. Implications for policy, practice and research are discussed.
Highlights
-
At least one-third of children had experienced one or more adversities, and almost 8% had experienced multiple adversities.
-
Adversity was reported by respondents across all categories of demographic variables.
-
Experiencing adversity was related to demographic characteristics at the level of geographic area, household, and individual.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Adverse Childhood Experiences (ACEs) do not discriminate: they can be experienced by any child, in any household, in any area of the world (Australian Institute of Family Studies, 2017; Bellis et al., 2014b; Stoltenborgh et al., 2015). The ACEs, as defined by Felitti and colleagues (1998), are common adversities that have been widely found to have negative, cumulative effects across the lifespan, in the two decades since they were first studied (Anda et al., 2006; Chartier et al., 2010; Kalmakis & Chandler, 2015). The ten adversities captured in the ACEs are: physical, emotional, and sexual abuse; physical and emotional neglect; parental separation/divorce; witnessing inter-partner violence; and living with someone who has a mental health condition or substance use problem, or becomes incarcerated (Anda et al., 2006). The first five ACEs may be thought of as maltreatment-type adversities, and the last five as dysfunction-type adversities (Negriff, 2020). These ten ACEs may occur any time between birth and age 18, and often co-occur with one another (Felitti et al., 1998). Their cumulative impact may be seen across health, wellbeing and socioeconomic domains, whereby experiencing a higher number of different types of ACEs is linked to increased risk for poor outcomes such as poor self-rated health, increased health risk behaviours, cancer, heart disease, respiratory disease, mental ill health, problematic use of alcohol and drugs, interpersonal and self-directed violence (Hughes et al., 2017), homelessness (Kalmakis & Chandler, 2015), low educational attainment, and unemployment (Hardcastle et al., 2018). Although the characteristics and impact of each of the ten ACEs differ from one another, their combined impact across the lifespan may be persistent and pervasive (Bellis et al., 2019), and extend intergenerationally (Chung et al., 2010; Fonseka et al., 2015; Hammett et al., 2020; Hughes et al., 2017; Reavis et al., 2013). ACEs are positioned within a wider context that includes other adversities (e.g., neighbourhood violence, peer victimisation; Finkelhor et al., 2015; Kalmakis & Chandler, 2014), and other factors that may be important to consider alongside ACEs (e.g., socioeconomic position, positive life experiences; Bethell et al., 2019; Taylor-Robinson et al., 2018). By focusing on a standard set of ten types of maltreatment and dysfunction, the ACEs framework provides a unifying theoretical basis for a broad evidence base focused on understanding and mitigating the impact of these adversities across the life span, across generations, and across the globe.
The Prevalence of Adversity
A large body of international literature has therefore taken shape over the past few decades, unfortunately indicating that a high proportion of children across the world experience adversity. Meta-analyses estimate that globally, between 46% and 64% of children experience at least one ACE (Kalmakis & Chandler, 2015), 19% to 35% of children experience two or more ACEs (Bellis et al., 2019), and between 7% and 20% of children experience at least four ACEs (Bellis, et al., 2014b; Felitti et al., 1998; Logan-Greene et al., 2014). The prevalence and impact of ACEs may differ from place to place, however (Bellis et al., 2019), and it is therefore important to understand and address local contexts of adversity. While most of the ACEs literature has thus far focused on the U.S. context, and a body of research is growing in Europe and Canada, little has been done in other regions including in Australia (Karatekin et al., 2022). Towards this aim, a recent Australian study of four ACEs (family violence, household mental illness, household substance abuse, parental separation/divorce) by O’Connor and colleagues (2020), alongside five other adversities (legal problems, harsh parenting, unsafe neighbourhood, family member death), found that 53% of Australian children experience two or more of these nine types of adversity by age 10–11 years. The international and emerging Australian literature therefore indicate that adversity is prevalent in Australia, and future exploration is warranted to better prevent ACEs and mitigate their potentially far-reaching impacts.
The Social and Economic Context of Adversity
Across the world, adversity is present in all geographic areas, regardless of socioeconomic status, and in all families regardless of income, parental employment, educational attainment, or ethnicity (Bellis et al., 2014b; Shaefer et al., 2018; Soares et al., 2016). Consistent with this international literature, emerging Australian evidence indicates that adversity may be present in Australian families regardless of the remoteness or socioeconomic status (SES) of the area in which they live, or their ethnicity (Australian Institute of Health and Welfare, 2018; O’Connor et al., 2020).
While adversity may be found in all sectors of society, some demographic characteristics have been associated with a greater risk. Learning from international evidence, we may hypothesise that children may have a higher risk for experiencing multiple types of adversity if they live in a low income household (Dhondt et al., 2019; Shaefer et al., 2018; Soares et al., 2016), or if they have parents with low levels of education (Dhondt et al., 2019; Soares et al., 2016) or employment (Maitoza, 2019). Children may additionally have increased risk for adversity if they have an ethnic minority background, however this association may differ depending on the type/s of adversity and the measures of ethnicity used, which may include self-ascribed ethnicity (Bellis, et al., 2014b), skin colour (Soares et al., 2016), country of birth, and the language spoken in the family home (O’Connor et al., 2020). In Australia, such evidence is scarce, however the O’Connor et al. (2020) study of 5107 children from the Longitudinal Study of Australian Children found that children tended to have higher levels of adversity if they had parents who were born in countries that were assumed to be non-white and/or where they did not speak English at home. This study also found that Indigenous children are at increased risk for adversity, as are children who live in families with low socioeconomic status (i.e., where parents have low levels of education and income, and have occupations that are low in skill and prestige; O’Connor et al., 2020). These findings are supported by administrative data from Australian Child Protection agencies, which indicate that child maltreatment is more prevalent among Indigenous children, and children living in lower SES areas, as well as remote or very remote areas (Australian Institute of Health and Welfare, 2017a).
While evidence on the mechanisms for the link between demographic characteristics and cumulative adversity is lacking, there has been some exploration of the mechanisms for individual adversities. Theories of social selection and social stress in mental health may therefore be helpful in understanding the links between demographic characteristics and adversity (Walsh et al., 2013). The social selection model suggests that adversity may contribute to parents having lower capacity for education and employment, which subsequently leads to a lower household income and living in a lower SES area (which may be cheaper to live in and have other people with similar levels of education, employment, and income). The social stress model indicates that the stresses of living in a low SES area (e.g., discrimination, poor quality housing, high crime rates), having poor access to support services (e.g., due to low education, low income, and low proximity), and having limited personal resources (i.e., low income, reduced opportunity, housing instability), may precipitate, exacerbate, or perpetuate adversities such as problems with relationships, mental health, and substance use. Social selection and social stress may form a feedback loop (wherein selection increases stress and vice versa) that worsens over time and persists over generations, leading to entrenched disadvantage and intergenerational adversity (Schoon & Melis, 2019).
The extant evidence and theory therefore indicate that family-level and area-level demographic characteristics may be linked to increased risk for adversity in complex ways. There are, however, key limitations to the available evidence. Unfortunately, the Australian child protection data do not distinguish between different kinds of maltreatment, or indicate what demographic factors may be related to risk for cumulative adversity (Australian Institute of Health and Welfare, 2017a). While the O’Connor et al. (2020) paper provides useful insights to what these demographic factors might be, its results pertain to ACEs and other types of adversity captured to age 10/11 only, and a composite measure of socioeconomic status that does not allow for the individual effects of education, employment and income to be ascertained. It is therefore important that further study be conducted into the relationships between demographic characteristics and ACEs within the Australian context, as it should not be assumed that international evidence is directly translatable to the unique Australian demographic landscape. Such research would benefit from exploring the effects of adversity occurring in adolescence as well as childhood, to account for potential differences in ACEs’ prevalence between these life stages (Wolitzky-Taylor et al., 2017), and to better align with widely-used definition of ACEs as occurring in the first 18 years of life (Felitti et al., 1998; Kalmakis & Chandler, 2015).
Although Australia is the sixth largest country in the world (Geoscience Australia, 2014) and has the third lowest population density globally (The World Bank, 2020), 85% of its 25 million residents live within 50 kilometres of the coastline, and only one quarter of the population reside outside of the seven major cities (Australian Bureau of Statistics, 2020). The Australian population rank sixth and eighth for tertiary education and employment rates among OECD countries, respectively (OECD, 2022a, 2022b). It is a culturally diverse country, with almost half of all Australians (49%) either born overseas or having parent/s born overseas (Australian Bureau of Statistics, 2017a), ranking it third among OECD countries for overseas-born population (OECD, 2018). In addition, approximately 4% of the population are Aboriginal or Torres Strait Islander; Indigenous peoples unique to this country (Australian Bureau of Statistics, 2022). Income inequality in Australia is higher than in most developed economies (OECD, 2021), and entrenched disadvantage (including multi-generational welfare dependence, low employment, low educational attainment) is experienced by families and communities across Australia, with at-risk groups including culturally and linguistically diverse populations, Aboriginal and Torres Strait Islander peoples, and Australians living in regional and remote areas (House of Representatives Select Committee on Intergenerational Welfare Dependence, 2019). Many of the demographic characteristics previously found to be associated with risk for adversity (e.g., low education, low income, ethnic minority status) may therefore have prevalence rates and inter-relationships in the Australian context that differ from those found in other countries. This unique demographic context means that it is critical that Australian-specific research be conducted to identify how demographic characteristics may contribute to risk that adversity will affect Australian families.
While the available evidence provides an indication of the prevalence of adversity and the demographic characteristics that may be associated with adversity in Australia, evidence is however lacking regarding the associations between demographic factors and multiple (i.e., cumulative) adversities in the Australian context among nationally representative samples of children across the full 0- to 18-years age range. Research is required to determine whether Australian children are likely to experience more adversity if they have the demographic characteristics previously identified as being associated with increased risk for adversity across the extant international and/or Australian literature (i.e., low area SES, living in a remote area, low income, ethnic minority status, Indigenous status, low parental employment and education). A more cohesive and comprehensive evidence base may inform research, policy, and practice, to provide crucial supports for Australian families and children at risk for adversity and its related outcomes.
The Current Paper
This paper aimed to extend our understanding of adverse childhood experiences in the Australian context. The ACEs framework is utilised to enable comparison with the broader ACEs literature in Australia and internationally. It uses the National Health Survey 2014–15 (NHS) to demonstrate what an official, nationally representative dataset can tell us about adversity among Australian families of children aged 0 to 18. The NHS captures three ACEs: Parental separation and divorce, household mental health condition, and household substance use problem. These three ACEs are therefore the focus of this study.
The study aims to investigate: 1) the prevalence of adversity in Australian families; and 2) whether there are demographic characteristics associated with increased risk for adversity. As the first aim was exploratory, no hypotheses were created to address this aim. Aim 2 was motivated by the following proposition (hypothesis 1): The following demographic characteristics will be associated with a higher level of adversity: living in an area that is remote or has low socioeconomic status (Australian Institute of Health and Welfare, 2017b), living in a lower income household (Soares et al., 2016), being an ethnic minority (Soares et al., 2016), parents having lower educational attainment (Bellis et al., 2014a), and parents having lower employment levels (Bellis et al., 2014b).
Method
A review of surveys administered by the Australian Bureau of Statistics (ABS) was undertaken to determine the most appropriate dataset for investigating the prevalence of adversities experienced by Australian children. Table 1 lists the publicly available surveys that collect relevant information on the range of adversities experienced by children, and their demographic characteristics. Of the six surveys listed, the NHS was chosen for this study because it captured the highest number of ACEs across the available ABS surveys (i.e., three of the ten ACEs; Felitti et al., 1998), and comprised a sample designed to be representative of the Australian population at the time of data collection (Australian Bureau of Statistics, 2017b).
Sample
The National Health Survey 2014–15 (NHS) was a cross-sectional survey of Australian residents aged 18 years and older, collected by the ABS (Australian Bureau of Statistics, 2017b). The overall NHS sample was designed to be representative of the Australian population in regards to state/territory of residence, area remoteness, and area socioeconomic status (Australian Bureau of Statistics, 2017b). The sampling frame included all dwellings located in urban and rural areas of Australia, in which approximately 97% of Australian residents live. Prospective participants across 20,892 dwellings were approached via post and asked to register for participation online. Part of the interview was conducted over the phone, and part was conducted via Computer Assisted Personal Interview in the respondent’s home. With an overall response rate of 82.0%, the final total sample included 14,723 households.
This paper utilised an analytic sample extracted from the complete dataset (N = 4161) comprising all respondents aged 18 years and older who resided with at least one child under the age of 18 years, in a household classified as either a one- or two-parent family with children. For the purposes of this paper, the adults in these households are referred to as “parents”. The respondents were aged between 18 and 82 years (M = 38.81, SD = 9.05), with 99% of the sample aged 18–59 years. Comparisons with the 2016 Census of Population and Housing indicate this sample was generally representative of the Australian general population of 18- to 59-year-olds. Differences between the sample and the population were observed to be small (less than 10%) when comparing the proportions represented within the categories of gender, educational attainment, employment, remoteness, and area socioeconomic status. There were more English-speaking adults, and families with one child in this sample than in the general population, with differences in these categories of 17.5% and 14.6% respectively. The spread of respondents was more consistent across the states and territories than is seen in the general population. Demographic characteristics of the sample are presented in Table 2.
Measures
The measures used in this paper were developed by the Australian Bureau of Statistics (ABS) for the National Health Survey conducted in the years 2014 and 2015 (NHS 14-15; Australian Bureau of Statistics, 2016b). The unit-level data were released publicly (upon approval from Australian Bureau of Statistics) in Detailed Microdata format. A description of each measure as it is used in the current study is included below. For details of the measures as they appeared in the original NHS 14-15 questionnaire, see the National Health Survey Users’ Guide 2014-15 (Australian Bureau of Statistics, 2017b).
Adversity
The primary measure of interest was the number of adversities experienced by children (aged 0 to 18) living with the respondents. Three household dysfunction ACEs are captured in the NHS 14-15: having a single parent, living with someone with a mental health condition, and living with someone with a substance use problem. It was calculated as a count of how many of the three ACEs were reported (ranging from 0 to 3).
Single parenthood was measured using respondents’ reported relationships between household members, as collated by the ABS into a measure of household type. Respondents residing in a couple family with children were classified as ‘not a single parent’, and respondents in a one parent family with children were classified as ‘a single parent’. Both household types could also include one other relative. As it was not possible to determine whether the respondents in one-parent households had ever been partnered (and thus had ever been separated or divorced), for the purposes of this paper the measure was referred to as ‘single parenthood’ rather than the more common ACE definition of ‘parental separation/divorce’.
Mental health condition was measured using respondents’ reports of “any conditions you are currently managing with treatment or medication”. Respondents were prompted with cards listing a range of mental health problems including diagnosed conditions and self-assessed states, such as depression, anxiety and panic disorder as well as ‘feeling depressed’, ‘feeling anxious, nervous or tense’, ‘panic attacks’, and ‘any other mental or behavioural condition’ (Australian Bureau of Statistics, 2015). Respondents who reported having one or more condition were classified as ‘having a mental health condition’. All other respondents were classified as ‘not having a mental health condition’.
Substance use problem was measured using the same question and prompt cards as the above mental health condition item, which also included managing a substance use problem with treatment or medication, such as harmful use or dependence on alcohol, drugs or medicinal/prescription drugs. Respondents who reported one or more substance use problems were categorised as ‘having a substance use problem’. All other respondents were classified as ‘not having a substance use problem’.
Demographic Characteristics
State or territory of residence corresponded to the state or territory of Australia in which the respondent resided.
Remoteness of respondents’ area of residence corresponded to the Australian Statistical Geography Standard 2011 Remoteness Area (Australian Bureau of Statistics, 2013). For this study, seven categories were aggregated to three categories: Major City, Inner Regional, and Outer Regional or Remote. Major City was used as the reference category in analyses.
Socioeconomic status of the area of residence (Area SES) was measured using the ABS Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-economic Disadvantage 2011 (IRSD) (REF). The IRSD is an aggregate measure derived from a range of socioeconomic indicators such as income, educational attainment, unemployment, and the number of dwellings without motor vehicles (Australian Bureau of Statistics, 2017b). It ranks geographic areas (equivalent to suburbs) according to their level of disadvantage (Australian Bureau of Statistics, 2017b). Ranks were ordered into deciles, providing a score from 1 (most disadvantaged) to 10 (least disadvantaged), where a higher score indicated that respondents resided in a less disadvantaged area.
Number of children in household corresponds to the number of children aged 0–17 years residing in the respondent’s household. This data was provided in categories of 0, 1, 2, 3, and 4 or more children. NHS data tables indicate that less than 1% of responding single- and double-parent households reported five or more children (Australian Bureau of Statistics, 2016c). For the purposes of the current paper, respondents in the category of “4 or more children” were represented by the category value 4.
Household income was measured using the respondent’s reported gross household income, adjusted for the number of adults and children resident in the home. The adjustment was conducted by the ABS, to provide a standardised measure of Household Gross Weekly Equivalised Income. This income estimate accounts for the number of potential income earners in the home and was thus not conflated with the focal variable of single parenthood. Higher scores on the household income variable indicate a higher per-resident income for the respondent’s household.
Age of respondent was self-reported and measured using age in years from 0 to 84 years, with persons aged 85 years and older classified as “85+”.
Sex of respondent was self-reported and measured as a dichotomous variable with categories Male and Female.
Educational attainment was measured using respondent’s self-reported highest completed qualification. There were five categories: Below Year 12, Year 12, Certificate or diploma, Bachelor or graduate qualification, and Postgraduate qualification. Year 12 was used as the reference category in analyses.
Employment status was measured using respondents’ self-reported employment status, with three categories: Employed, Unemployed, and Not in the labour force (NITLF). Employed respondents had worked in a paid job, business or farm, or had a job but were absent during the previous week; excluding those who usually worked less than one hour, or were away from work due to workers compensation and were not, or did not know if, they were returning to work for their employer. Unemployed respondents were those not ‘Employed’, who had actively looked for work during the previous four weeks, and were available to start, or waiting to start within the following four weeks. Respondents were considered NITLF if they were not ‘Employed’ or ‘Unemployed’. The reference category for analyses was Employed.
Language was included as a proxy measure for ethnic minority status, and was measured using respondents’ self-report of which language they mainly spoke at home, as classified by the Australian Standard Classification of Languages (ASCL; Australian Bureau of Statistics, 2011a). Responses were collapsed into two categories: English, and Language other than English. English was the reference category in analyses.
Analysis
Analyses of the unit record data for individuals was conducted using Stata Version 10.0, hosted on the Australian Bureau of Statistics Remote Access Data Laboratory (RADL; Australian Bureau of Statistics, 2011b). Technical restrictions of the now-decommissioned RADL precluded estimation or imputation of missing data. Analyses were not weighted, as most of the variables used to calibrate the weights (i.e., geographic area of residence, age, sex) were included as focal predictors in the main analyses. To address the first aim of the paper, the prevalence of adversity was investigated for respondents and the children with whom they lived. Estimates of the number and types of adversities reported by respondents were calculated to provide prevalence rates and sample proportions. In addition, the number of children in the respondents’ households were cross tabulated with the prevalence rates. These cross-tabulations were used to calculate estimates of the number and proportion of children affected by each type of adversity, and how many adversities the children were affected by. The prevalence of adversity was explored across the categories of the demographic variables, with sample prevalence estimates calculated using the counts of the number of respondents reporting one or more adversities across the demographic variables’ categories. To address hypothesis one, relationships between participants’ number of ACEs and demographic characteristics were assessed with bivariate and multivariate analyses. Bivariate analyses used Chi-square statistics and Pearson’s R statistics to ascertain the relationship between ACEs and demographics, not accounting for any other factors. Multivariate analysis comprised of a hierarchical multiple regression conducted to examine the unique relationships between each demographic factor and the number of ACEs, once the variance shared by the demographic variables was portioned out. The dependent variable was the number of adversities reported, ranging from 0 to 3. Predictor variables were: Remoteness, Area SES, Household income, Employment, Education, and Language. State/Territory, Age and Sex were included as control variables. Categorical predictors with more than two categories were entered as dummy variables.
Results
The Prevalence of Adversity
Over one-third (35%) of respondents reported at least one of the three measured adversities (i.e., single parenthood, mental health condition, problematic substance use). An estimated 27% reported one type of adversity, 8% reported two types, and 0.4% reported all three adversities. Mental health conditions were the most common, reported by approximately one-quarter (23%) of the total sample. Single parenthood was reported by one-fifth (20%) of the sample, while substance use problems were reported by 1% of respondents. The proportions of children affected by each of these adversities were approximately equal to those reported for respondents. That is, the prevalence rates among respondents and children were almost identical. See Fig. 1 for a summary of the number and type of adversities reported by the respondents.

Proportion of respondents reporting each type of adversity, by the number of adversities reported
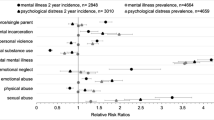
Singular and multiple experiences of adversity were reported by respondents across all demographic groups. Results indicate that the prevalence of adversity varied considerably according to demographic characteristics. For example, approximately half (48%) of respondents with less than 12 years of schooling reported at least one type of adversity, which was almost 2.5 times the rate for respondents with postgraduate degrees (21%). The proportion of respondents who reported adversity was roughly equal across the categories of remoteness, state/territory, and number of children. Adversity was reported by a larger proportion of respondents in lower SES areas, and those who had lower levels of educational attainment or employment, spoke English at home, and/or were female. For multi-categorical demographic variables, differences were not prominent when comparing adjacent categories, and were more pronounced when comparing distal categories. For example, rates of adversity were similar among respondents living in the areas with the highest (24%) and second highest (28%) socioeconomic status, but were much lower than for respondents in the areas with the lowest socioeconomic status (57%). See Fig. 2 for a summary of the proportion of respondents who reported adversity across each of the demographic variables’ categories.

Proportion of respondents within categories of demographic variables who reported any adversity, by the number of adversities reported. Note. Error bars refer to the 95% confidence interval for sample estimates of the number of respondents reporting one or more adversities
Are Any Demographic Characteristics Associated with Increased Risk for Adversity?
Bivariate relationships between adversity and demographic characteristics
Hypothesis one was partially supported by the results of the bivariate analyses (Table 3). Most bivariate relationships between adversity and demographic characteristics were significantly associated in the expected direction; however, some unexpected results were obtained. Chi-square statistics (for categorical variables) and Pearson’s R statistics (for continuous variables) showed that adversity was significantly associated with Remoteness (Χ2(6) = 33.40), Area SES (R = −0.19), Income (R = −0.23), Language (Χ2(3) = 39.76), Education (Χ2(12) = 126.92), and Employment (Χ2(6) = 179.36), and p-values associated with all statistics listed were <0.001. All associations were in the expected direction, except for the association between the number of ACEs and Language. Although it was hypothesised that respondents who spoke a Language other than English would report more adversity, results indicated that these respondents reported significantly fewer adversities than those who spoke English. This association was investigated further in the multivariate analysis reported below. With the exception of the association between Remoteness and Employment, all relationships between demographic characteristics were significant, with p-values <0.01. Overall, the bivariate results confirmed that there were significant relationships between adversity and demographic characteristics. Multivariate analysis was warranted to further explore these relationships.
Multivariate relationships between adversity and demographic characteristics
Hypothesis one was further supported by results of a hierarchical multiple regression, which identified demographic characteristics that were significant predictors of respondents’ level of adversity. See Table 4 for results. Step one included area-level predictors, and accounted for 4.7% of the variance in adversity, F(10, 3505) = 17.41, p < 0.001. Results indicated that respondents were likely to experience more Adversity when living in a lower SES area. Step two included addition of the household-level predictor Income; and accounted for an additional 2.7% of variance in adversity, F(1, 3504) = 101.99, p < 0.001; with respondents in lower Income households likely to experience significantly more Adversity, and Area SES still a significant predictor. Step three included the addition of individual-level predictors, and accounted for an additional 8.6% of variance, producing an overall regression model accounting for 16.0% of variance in Adversity, F(9, 3495) = 39.48, p < 0.001. The final regression model revealed that when the variance in Adversity that is explained by other demographic characteristics was portioned out, there were significant associations between the following characteristics, and a higher level of Adversity (in descending order of explanatory power): lower Income household; spoke English at home; lower SES area; Unemployed rather than Employed; Major City rather than an Outer Regional or Remote area; NITLF rather than Employed; and completed Less than Year 12 or never attended school, rather than finished Year 12.
As bivariate results showed that respondents in Outer Regional or Remote areas tend to report higher levels of Adversity than respondents in Major Cities, the multivariate results indicate that the effect of Remoteness may be absorbed by the effects of other demographic characteristics which share large amounts of variance with Remoteness, for example, education level, and area SES. The partial positive effect between Adversity and living in a Major City may be a consequence of other factors that interplay in the city to foster adversity, in a way that was not observed in remote areas.
Discussion
This study used a secondary data source to provide new evidence around ACEs in Australia, and insights to the prevalence of adversity in children and associated risk and protective factors. The Australian government-administered National Health Survey 2014–15 dataset used for analysis (Australian Bureau of Statistics, 2017b) included three household dysfunction ACEs: having a single parent, living with someone with a mental health condition, and living with someone with a substance use problem. The two key aims were to: 1) investigate the prevalence of these three adversities across Australia; and 2) identify demographic characteristics associated with an increased risk for ACEs.
Although the current paper was only able to capture three of the ten ACEs described by Felitti and colleagues (1998), results indicated that over one-third of respondents reported at least one adversity, while one in twelve reported two or more adversities. These estimates were similar to international estimates of one-half to two-thirds of children experiencing at least one ACE (Kalmakis & Chandler, 2015); but are lower than international estimates of children with two or more ACEs (i.e., one-fifth to one-third of children, Bellis et al., 2019). This is likely attributable to the limited number of ACEs captured in the current study, and a lower-than-expected reporting of substance use problems. The small number of reported substance use problems may reflect a true low prevalence of this adversity in this sample, however, the narrow definition of substance use, and problems with social desirability bias, may have contributed to under-reporting. Even with this potential limitation, the overall prevalence rates were similar to those from international studies (Bellis et al., 2019; Kalmakis & Chandler, 2015), indicating that international estimates and studies may have some usefulness in understanding adversity in Australia. Overall, these results show that even when only three of the ten ACEs are measured, national data indicates that adversity is affecting many children and families across Australia. It is likely that the prevalence estimates would be much higher if more types of adversity were captured. At the time of writing, however, no large datasets from population surveys that are publicly collected and available in Australia contain data on more than three ACEs. This limited scope is problematic as it precludes research regarding people who experience four or more adversities, who may be particularly at risk for poor outcomes (Felitti et al., 1998). With each type of adversity having unique and cumulative effects across the life course (Kalmakis & Chandler, 2015), and the current results indicating that adversity affects at least one-third of Australian families, it is critical that the prevalence and correlates of all ten ACEs be explored in Australia in the future.
Recent Australian research has shown that adversity occurs across ethnic groups and area-level socioeconomic contexts (O’Connor et al., 2020), as has previously been found in England (Bellis et al., 2014b). The current paper extends these findings by including additional demographic characteristics and indicating that adversity occurs in a broad range of contexts. Across the demographic characteristics measured in this study, no category was exempt from adversity. It was found in every state and territory, from major cities to remote Australia, across the most and the least disadvantaged areas; regardless of language, employment, or education.
To better understand how such contexts might relate to children’s risk for adversity, the relationships between demographic characteristics and adversity were explored. Previous international and Australian literature has identified a range of demographic characteristics that may be associated with singular or multiple adversities. It was hypothesised that these same demographic characteristics would be associated with adversity in this Australian sample. Results partially supported this hypothesis. In both the absence and presence of other demographic characteristics, higher levels of adversity were associated with lower area SES and household incomes; having a parent who was unemployed or NITLF, or had less than 12 years of schooling; and mainly speaking English at home. The results regarding the socioeconomic demographic characteristics (i.e., area SES, household income, employment, and education) were as expected, based on international literature that has indicated that children whose parents have these characteristics may be more at risk for adversity (Soares et al., 2016); and Australian evidence for the links between adversity and the socioeconomic status of families (O’Connor et al., 2020) and the area in which they live (Australian Institute of Health and Welfare, 2017b). The current results reveal that parents were more likely to be single parents, have mental health concerns, and/or have substance use problems if they held these demographic characteristics that contribute to low socioeconomic status. The observed association may be bidirectional or cyclical, with the stresses of low socioeconomic status (e.g., low personal resources, poor access to services, dealing with crime and discrimination) impeding functioning in areas such as interpersonal relationships, mental health and substance use, therefore leading to adversity; and adversity reducing parents’ capacity for education and employment, leading to a lower household income and living in a low SES area. It is important to note, however, that as these demographic characteristics were not too highly correlated with one another, it does not appear that any one characteristic necessarily follows another (e.g., low education causing low employment) in influencing risk for adversity. Similarly, the significant multivariate results indicate that it is not a single underlying construct that is driving the relationships between these socioeconomic demographic characteristics (as the shared variance has been portioned out). The links between adversity and individual- and area-level socioeconomic demographic characteristics therefore appear to be important to consider together and independently. An additional complexity is the potential role of the inter-generational continuity of adversity, as parents who have experienced adversity are more likely to have poor socioeconomic outcomes (Hardcastle et al., 2018), and inter- and intra-personal issues that may contribute to their children experiencing adversity (Bellis et al., 2019; Schofield et al., 2018). Future research may investigate the mechanisms by which these characteristics are associated with adversity; and how the convergence of family characteristics and adversity influence outcomes. Such research may provide insights to points of vulnerability that may be targeted to prevent adversity and reduce its impact across the life course.
The finding that higher adversity was associated with lower levels of education and employment has additional implications for the interpretation of the adversity prevalence rates found in this study. As the prevalence rates were derived from a sample that is slightly more educated and employed in comparison to the Australian population (Australian Bureau of Statistics, 2016a), ACEs may be even more prevalent in the Australian population than in this sample. Further research using nationally representative samples, capturing a greater range of adversities is required to provide more accurate estimates of the prevalence of adversity in Australia.
In contrast to the results regarding the included socioeconomic factors, the findings around English-speaking households were unexpected. Although previous Australian research has indicated that adversity may be more prevalent in ethnic minority households (O’Connor et al., 2020), the current results indicated that English-speaking families may be more at risk for adversity. This discrepancy adds to the already-mixed evidence for the relationship between ethnicity and adversity. One potential reason for differences in this area relates to measurement. O’Connor and colleagues (2020) measured ethnic minority in an Australian sample using language and country of birth, and measured nine types of adversity. In contrast, the current study used only language, and measured three types of adversity. Thus factors such as country of birth may be the main driver behind the previously identified link between ethnic minority status and adversity; and/or it is possible that ethnic minority families are more at risk for adversities other than single parenthood, mental health conditions and substance use problems. This would in part be consistent with Bellis et al. (2014b), wherein in their nationally representative survey of English residents aged 18 to 69 found that white respondents reported more household mental illness than Asian or “other” ethnicity respondents, while other adversities varied across the three ethnic groups, with rates of adversity generally lower for Asian respondents. As the ethnic profile of each country is idiosyncratic, it may not be possible to extrapolate the results of international studies to Australia. Further, while other characteristics are measured as “relative” characteristics (e.g., relatively higher or lower income), ethnicity is often measured as descriptive characteristics (e.g., white or non-white); which do not consider the meaning of ethnicity. It is therefore important to interpret results regarding ethnicity within their given context. Future research is required to explore the relationship between ethnicity and adversity in the Australian context, using a sample with a more representative mix of ethnicities than is provided in the current sample.
Remoteness was another factor that had associations with adversity that were unexpected. It was hypothesised that respondents living in major cities would experience less adversity than respondents living in more remote areas. Although the hypothesis was supported by bivariate analyses, once the effects of other demographic characteristics were taken into account, the additional partial effect of living in a major city was associated with greater adversity. It may therefore not be remoteness itself, but rather the sociodemographic factors that co-occur with remoteness, that are conferring risk to rural and remote areas. These results are in partial agreement and partial contrast with international evidence. While the current results show major cities to be associated with adversity only after controlling for other factors, a recent paper from Marryat and Frank (2019) drew on a national sample of Scottish children (N = 3119) to show that living in a major city was associated with greater risk for ACEs than living rurally, both before and after controlling for factors such as income, area SES, and education. The current results also partially align with US studies using national samples, which found that rural children had an overall higher prevalence of adversity than urban children (similar to the current study), but (unlike the current study) found no differences between urban and rural prevalence rates after accounting for the effects of poverty (Crouch et al., 2020), or after controlling for sex, age, and ethnicity (Talbot et al., 2016). In addition, the results support literature that highlights the complex inter-relationships between remoteness and socioeconomic status in Australia (Inder et al., 2011). Taken together, the mixed results from the extant evidence, including this study, suggest that the relationship between geographic location and adversity is complex and potentially influenced by factors associated with the broader community context. Further research is therefore required to explore the inter-relationships between remoteness, other demographic characteristics, and adversity in both the international and Australian context.
Overall, the results indicate that adversity is experienced by children across all demographic contexts, with a range of social and economic factors associated with an increased risk for adversity. The results highlight that although specific known demographic characteristics may place children and families at greater risk for adversity, adversity may occur for people with a wide variety of demographic characteristics, not just the characteristics previously identified as related to risk. These characteristics span many domains and levels of measurement (i.e., the geographic area, the household, and the individual). It is therefore important that research on adversity explores the impact of demographic characteristics across geographic area, household, and individual levels. Services and policies that aim to support families and address adversity in the Australian context may benefit from utilising a blend of population-based and targeted approaches, known as progressive universalism (Marmot, 2013; Prinz, 2015) or targeted universalism (Powell et al., 2019). This blended approach has previously been found to be an effective strategy for addressing large-scale public health matters such as mental health (Barry, 2019) and family functioning (Frost et al., 2015); and involves providing a broad suite of supports to the whole population, with supplementary supports offered to those with additional needs (Marmot, 2013). With adversity affecting families across Australia, and some families at increased risk due to demographic characteristics, a progressive universalist approach to service delivery and policy making may be most effective at supporting these families to prevent adversity and its harms.
Strengths and Limitations
There are a few points to consider when interpreting the results of this paper’s analysis. Firstly, the number of adversities captured in the dataset is limited to three of the ten ACEs (Felitti et al., 1998). As the different types of adversity can have differing relationships with demographic characteristics (Walsh et al., 2019), it is important to interpret the results of this paper as referring to the characteristics associated with increased prevalence of single parenthood, mental health conditions, and substance use problems. Further, the data collection method and scope of the items may under-represent the prevalence of adversity. This is due to social desirability bias (respondents declining to report dysfunction), selection bias (individuals dealing with multiple challenges are not as likely to participate in research), and limited scope (data captures only three adversities pertaining to one adult in the household).
Adversities that involve persons other than the responding adult, or that occur outside of the reference period of the survey (e.g., the period of time around data collection) are also not captured in the NHS 14-15 data. This would likely result in further under-estimation of adversity in this sample. Previous ACE literature has shown that adversities experienced at any time in a child’s first 18 years of life have significant impact on their health and wellbeing (Giovanelli, 2018), as may adversities pertaining to persons other than one’s primary caregiver (Asmussen et al., 2020). As such, future research should aim to determine the lifetime prevalence of childhood adversities in Australia, including those that relate to a broader range of household members, such as other parents, caregivers, and siblings. It is important to note that the cross-sectional nature of the NHS 14-15 precludes study of directionality or time/order effects, although it can be used to provide powerful cross-sectional insights, due to its large, national sample. The restrictions of the now-decommissioned Remote Access Data Laboratory prevented the estimation or exploration of missing data, and thus only complete cases were included in the regression analyses. As the resulting exclusion of 15% of the dataset gave a final sample of over 3000 participants, there would not have been a significant loss of power to detect significant effects, however the obtained estimates may have been biased by the use of complete case analysis. In addition, as sample weights were not utilised, the analyses did not adjust for the relative importance or representativeness of cases or variables. It is however important to note that because many of the variables used to benchmark the weights were included as predictors in the main analysis, potential use of weights may have introduced redundant or collinear information without providing additional insights or improving accuracy. The general alignment of the analytic sample’s demographic characteristics with the Australian population (see Table 2), and of the obtained results with extant evidence and theory, indicate that the estimates were not likely substantially biased, however, future analyses using other methods for handling missing data and weighting may serve to further support or clarify the observed results.
Despite issues of limited scope and potential under-reporting, the current results indicate that adversity is highly prevalent in Australia. With only limited evidence available on ACEs in this country, there is a great need for further data collection and research in this area. Future work that is less restricted by limitations may reveal higher prevalence rates and different demographic correlates. This would provide a more accurate and comprehensive picture of the adversities faced by families in this country, and valuable insights to the characteristics of the families who may be affected. Such information may be valuable for targeting and developing supports for families, to prevent adversity and ameliorate its effects.
Conclusion
This study provides a valuable insight into childhood adversity in Australia, and its relationships with demographic characteristics. It provides evidence that adversity affects many children across Australia, occurs across all demographic contexts, and is associated with a range of area-, household-, and person-level characteristics. There is therefore a need to take a blended, population-based, and targeted approach when supporting the families who may be experiencing adversity. Further exploration of the relationships between adversity and demographic characteristics may help provide a clear picture of the risk and protective factors that can be targeted by services, policies and funding aimed at reducing adversity and its harms for children, families and communities in Australia. Such steps towards better supporting families may have wide reaching implications for the health and wellbeing of children, families and communities across the nation.
References
Anda, R. F., Felitti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C., Perry, B. D., Dube, S. R., & Giles, W. H. (2006). The enduring effects of abuse and related adverse experiences in childhood: a convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience, 256(3), 174–186. https://doi.org/10.1007/s00406-005-0624-4.
Asmussen, K., Fischer, F., Drayton, E., & McBride, T. (2020). Adverse childhood experiences: What we know, what we don’t know, and what should happen next. Early Intervention Foundation. https://www.eif.org.uk/report/adverse-childhood-experiences-what-we-know-what-we-dont-know-and-what-should-happen-next.
Australian Bureau of Statistics. (2011a). 1267.0 - Australian Standard Classification of Languages (ASCL), 2011 http://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/1267.0Main+Features12011?OpenDocument.
Australian Bureau of Statistics. (2011b). General information for Stata users. Retrieved 13 November, 2017 from https://www7.abs.gov.au/forums/radl.nsf/bd95505367a3a0e0ca256c3d0004f8ec/2e91b5075d39a7f2ca25728b00296f69?OpenDocument.
Australian Bureau of Statistics. (2013). 1270.0.55.005 - Australian Statistical Geography Standard (ASGS): Volume 5 - Remoteness structure. https://www.abs.gov.au/ausstats/abs@.nsf/mf/1270.0.55.005.
Australian Bureau of Statistics. (2015). 4364.0.55.001 - National Health Survey 2014-15 Prompt Cards. https://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/4364.0.55.0012014-15?OpenDocument.
Australian Bureau of Statistics. (2016a). 2016 Census - Counting persons, place of usual residence. https://auth.censusdata.abs.gov.au/.
Australian Bureau of Statistics. (2016b). 4324.0.55.001 - Microdata: National Health Survey, 2014-15. https://www.abs.gov.au/ausstats/abs@.nsf/Previousproducts/4324.0.55.001Main%20Features702014-15?opendocument&tabname=Summary&prodno=4324.0.55.001&issue=2014-15&num=&view=.
Australian Bureau of Statistics. (2016c). National Health Survey 2014-15 TableBuilder. https://tablebuilder.abs.gov.au.
Australian Bureau of Statistics. (2017a). Census of Population and Housing: Reflecting Australia – Stories from the Census, 2016. Retrieved 08 November from https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/2071.0~2016~Main%20Features~In%20this%20Issue~1.
Australian Bureau of Statistics. (2017b). National Health Survey: Users’ guide, 2014-2015. https://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/4363.0Main+Features12014-15?OpenDocument.
Australian Bureau of Statistics. (2020). Regional population. https://www.abs.gov.au/statistics/people/population/regional-population/2018-19.
Australian Bureau of Statistics. (2022). Estimates of Aboriginal and Torres Strait Islander Australians. https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/estimates-aboriginal-and-torres-strait-islander-australians/jun-2021.
Australian Institute of Family Studies. (2017). The prevalence of child abuse and neglect. https://aifs.gov.au/cfca/publications/prevalence-child-abuse-and-neglect.
Australian Institute of Health and Welfare. (2017a). Child protection Australia 2015–16 (Vol. 66). https://www.aihw.gov.au/reports/child-protection/child-protection-australia-2015-16.
Australian Institute of Health and Welfare. (2017b). National Framework for Protecting Australia’s Children. http://www.aihw.gov.au/nfpac/.
Australian Institute of Health and Welfare. (2018). Child protection Australia 2016–17 (Vol. 68). https://www.aihw.gov.au/reports/child-protection/child-protection-australia-2016-17.
Barry, M. M. (2019). Reframing the challenge of promoting population mental health. In M. M. Barry, A. M. Clarke, I. Petersen, & R. Jenkins (Eds.), Implementing mental health promotion (pp. 35–57). Springer International Publishing. https://doi.org/10.1007/978-3-030-23455-3_2.
Bellis, M. A., Hughes, K., Ford, K., Ramos Rodriguez, G., Sethi, D., & Passmore, J. (2019). Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America: A systematic review and meta-analysis. The Lancet Public Health, 4(10), E517–E528. https://doi.org/10.1016/S2468-2667(19)30145-8.
Bellis, M. A., Hughes, K., Leckenby, N., Jones, L., Baban, A., Kachaeva, M., Povilaitis, R., Pudule, I., Qirjako, G., Ulukol, B., Raleva, M., & Terzic, N. (2014). Adverse childhood experiences and associations with health-harming behaviours in young adults: Surveys in eight Eastern European countries. Bulletin of the World Health Organization, 92(9), 641–655. https://doi.org/10.2471/BLT.13.129247.
Bellis, M. A., Hughes, K., Leckenby, N., Perkins, C., & Lowey, H. (2014b). National household survey of adverse childhood experiences and their relationship with resilience to health-harming behaviors in England. BMC Medicine, 12(1), 72 https://doi.org/10.1186/1741-7015-12-72.
Bethell, C., Jones, J., Gombojav, N., Linkenbach, J., & Sege, R. (2019). Positive childhood experiences and adult mental and relational health in a statewide sample: Associations across adverse childhood experiences levels. JAMA Pediatrics, 173(11), e193007. https://doi.org/10.1001/jamapediatrics.2019.3007.
Chartier, M. J., Walker, J. R., & Naimark, B. (2010). Separate and cumulative effects of adverse childhood experiences in predicting adult health and health care utilization. Child Abuse and Neglect, 34(6), 454–464. https://doi.org/10.1016/j.chiabu.2009.09.020.
Chung, E. K., Nurmohamed, L., Mathew, L., Elo, I. T., Coyne, J. C., & Culhane, J. F. (2010). Risky health behaviors among mothers-to-be: The impact of adverse childhood experiences. Academic Pediatrics, 10(4), 245–251. https://doi.org/10.1016/j.acap.2010.04.003.
Crouch, E., Radcliff, E., Probst, J. C., Bennett, K. J., & McKinney, S. H. (2020). Rural-urban differences in adverse childhood experiences across a national sample of children. The Journal of Rural Health, 36(1), 55–64. https://doi.org/10.1111/jrh.12366.
Dhondt, N., Healy, C., Clarke, M., & Cannon, M. (2019). Childhood adversity and adolescent psychopathology: evidence for mediation in a national longitudinal cohort study. British Journal of Psychiatry, 215(3), 559–564. https://doi.org/10.1192/bjp.2019.108.
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/S0749-3797(98)00017-8.
Finkelhor, D., Shattuck, A., Turner, H., & Hamby, S. (2015). A revised inventory of Adverse Childhood Experiences. Child Abuse and Neglect, 48, 13–21. https://doi.org/10.1016/j.chiabu.2015.07.011.
Fonseka, R. W., Minnis, A. M., & Gomez, A. M. (2015). Impact of adverse childhood experiences on intimate partner violence perpetration among Sri Lankan men. PloS One, 10(8), e0136321 https://doi.org/10.1371/journal.pone.0136321.
Frost, N., Abbott, S., & Race, T. (2015). Family support: prevention, early intervention and early help. Polity Press. http://ebookcentral.proquest.com/lib/uql/detail.action?docID=4094506.
Geoscience Australia. (2014). Australia’s size compared. https://www.ga.gov.au/scientific-topics/national-location-information/dimensions/australias-size-compared.
Giovanelli, A. (2018). Adverse childhood experiences and adult well-being: impacts by type, timing, and early childhood intervention [Doctoral dissertation, University of Minnesota]. ProQuest Dissertations & Theses Global. http://hdl.handle.net/11299/201045.
Hammett, J. F., Karney, B. R., & Bradbury, T. N. (2020). Adverse childhood experiences, stress, and intimate partner violence among newlywed couples living with low incomes. Journal of Family Psychology, 34(4), 436–447. https://doi.org/10.1037/fam0000629.
Hardcastle, K., Bellis, M. A., Ford, K., Hughes, K., Garner, J., & Ramos Rodriguez, G. (2018). Measuring the relationships between adverse childhood experiences and educational and employment success in England and Wales: findings from a retrospective study. Public Health, 165, 106–116. https://doi.org/10.1016/j.puhe.2018.09.014.
House of Representatives Select Committee on Intergenerational Welfare Dependence. (2019). Living on the edge: inquiry into intergenerational welfare dependence. Commonwealth of Australia. https://parlinfo.aph.gov.au/parlInfo/download/committees/reportrep/024242/toc_pdf/LivingontheEdge.pdf;fileType=application%2Fpdf.
Hughes, K., Bellis, M. A., Hardcastle, K. A., Sethi, D., Butchart, A., Mikton, C., Jones, L., & Dunne, M. P. (2017). The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health, 2(8), e356–e366. https://doi.org/10.1016/S2468-2667(17)30118-4.
Inder, K. J., Berry, H., & Kelly, B. J. (2011). Using cohort studies to investigate rural and remote mental health. Australian Journal of Rural Health, 19(4), 171–178. https://doi.org/10.1111/j.1440-1584.2011.01208.x.
Kalmakis, K. A., & Chandler, G. E. (2014). Adverse childhood experiences: towards a clear conceptual meaning. Journal of Advanced Nursing, 70(7), 1489–1501. https://doi.org/10.1111/jan.12329.
Kalmakis, K. A., & Chandler, G. E. (2015). Health consequences of adverse childhood experiences: a systematic review. Journal of the American Association of Nurse Practitioners, 27(8), 457–465. https://doi.org/10.1002/2327-6924.12215.
Karatekin, C., Mason, S. M., Riegelman, A., Bakker, C., Hunt, S., Gresham, B., Corcoran, F., & Barnes, A. (2022). Adverse childhood experiences: a scoping review of measures and methods. Children and Youth Services Review, 136, 106425 https://doi.org/10.1016/j.childyouth.2022.106425.
Logan-Greene, P., Green, S., Nurius, P. S., & Longhi, D. (2014). Distinct contributions of adverse childhood experiences and resilience resources: a cohort analysis of adult physical and mental health. Social Work in Health Care, 53(8), 776–797. https://doi.org/10.1080/00981389.2014.944251.
Maitoza, R. (2019). Family challenges created by unemployment. Journal of Family Social Work, 22(2), 187–205. https://doi.org/10.1080/10522158.2018.1558430.
Marmot, M. (2013). Inequalities in health. Oxford University Press. https://doi.org/10.1093/acprof:oso/9780199931392.003.0019.
Marryat, L., & Frank, J. (2019). Factors associated with adverse childhood experiences in Scottish children: a prospective cohort study. BMJ Paediatrics Open, 3(1), e000340 https://doi.org/10.1136/bmjpo-2018-000340.
Negriff, S. (2020). ACEs are not equal: examining the relative impact of household dysfunction versus childhood maltreatment on mental health in adolescence. Social Science and Medicine, 245, 112696 https://doi.org/10.1016/j.socscimed.2019.112696.
O’Connor, M., Slopen, N., Becares, L., Burgner, D., Williams, D. R., & Priest, N. (2020). Inequalities in the distribution of childhood adversity from birth to 11 years. Academic Pediatrics, 20(5), 609–618. https://doi.org/10.1016/j.acap.2019.12.004.
OECD. (2018). Recruiting immigrant workers: Australia 2018. https://doi.org/10.1787/9789264288287-en.
OECD. (2021). Economic policy reforms 2021: going for growth. https://www.oecd.org/economy/growth/Australia-country-note-going-for-growth-2021.pdf.
OECD. (2022a). Australia: overview of the education system. Retrieved 08 November from http://gpseducation.oecd.org/.
OECD. (2022b). Employment rate. Retrieved 08 November from https://data.oecd.org/emp/employment-rate.
Powell, J. A., Ake, W., & Menendian, S. (2019). Targeted universalism: Policy & practice. Haas Institute for a Fair and Inclusive Society, University of California. https://belonging.berkeley.edu/targeteduniversalism.
Prinz, R. J. (2015). A population approach to parenting and family intervention. In Handbook of adolescent drug use prevention: Research, intervention strategies, and practice (pp. 237-247). American Psychological Association. https://doi.org/10.1037/14550-014.
Reavis, J. A., Looman, J., Franco, K. A., & Rojas, B. (2013). Adverse childhood experiences and adult criminality: how long must we live before we possess our own lives? The Permanente Journal, 17. https://doi.org/10.7812/tpp/12-072.
Schofield, T. J., Donnellan, M. B., Merrick, M. T., Ports, K. A., Klevens, J., & Leeb, R. (2018). Intergenerational continuity in adverse childhood experiences and rural community environments. American Journal of Public Health, 108(9), 1148–1152. https://doi.org/10.2105/AJPH.2018.304598.
Schoon, I., & Melis, G. (2019). Intergenerational transmission of family adversity: examining constellations of risk factors. PloS One, 14(4), e0214801 https://doi.org/10.1371/journal.pone.0214801.
Shaefer, H. L., Lapidos, A., Wilson, R., & Danziger, S. (2018). Association of income and adversity in childhood with adult health and well-being. Social Service Review, 92(1), 69–92. https://doi.org/10.1086/696891.
Soares, A. L. G., Howe, L. D., Matijasevich, A., Wehrmeister, F. C., Menezes, A. M. B., & Gonçalves, H. (2016). Adverse childhood experiences: prevalence and related factors in adolescents of a Brazilian birth cohort. Child Abuse and Neglect, 51, 21–30. https://doi.org/10.1016/j.chiabu.2015.11.017.
Stoltenborgh, M., Bakermans-Kranenburg, M. J., Alink, L. R. A., & van Ijzendoorn, M. H. (2015). The prevalence of child maltreatment across the globe: review of a series of meta-analyses. Child Abuse Review, 24(1), 37–50. https://doi.org/10.1002/car.2353.
Talbot, J., Szlosek, D., & Ziller, E. (2016). Adverse childhood experiences in rural and urban contexts. Maine Rural Health Research Centre. http://muskie.usm.maine.edu/Publications/rural/AdverseChildhood-Experiences-Rural.pdf.
Taylor-Robinson, D. C., Straatmann, V. S., & Whitehead, M. (2018). Adverse childhood experiences or adverse childhood socioeconomic conditions. The Lancet Public Health, 3(6), e262–e263. https://doi.org/10.1016/S2468-2667(18)30094-X.
The World Bank. (2020). Population density (people per sq. km of land area) - Australia. https://data.worldbank.org/indicator/EN.POP.DNST?locations=AU&most_recent_value_desc=false.
Walsh, D., McCartney, G., Smith, M., & Armour, G. (2019). Relationship between childhood socioeconomic position and adverse childhood experiences (ACEs): a systematic review. Journal of Epidemiology and Community Health, 73(12), 1087 https://doi.org/10.1136/jech-2019-212738.
Walsh, Z., Shea, M. T., Yen, S., Ansell, E. B., Grilo, C. M., McGlashan, T. H., Stout, R. L., Bender, D. S., Skodol, A. E., Sanislow, C. A., Morey, L. C., & Gunderson, J. G. (2013). Socioeconomic-status and mental health in a personality disorder sample: the importance of neighborhood factors. Journal of Personality disorders, 27(6), 820–831. 101521pedi201226061.
Wolitzky-Taylor, K., Sewart, A., Vrshek-Schallhorn, S., Zinbarg, R., Mineka, S., Hammen, C., Bobova, L., Adam, E. K., & Craske, M. G. (2017). The effects of childhood and adolescent adversity on substance use disorders and poor health in early adulthood. Journal of Youth and Adolescence, 46(1), 15–27. https://doi.org/10.1007/s10964-016-0566-3.
Acknowledgements
This research was supported by the Australian Research Council Centre of Excellence for Children and Families over the Life Course (CE140100027).
Author Contributions
C.C. designed, executed, and wrote the paper. K.B. and M.H. provided feedback on the design and writing of the paper.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The Parenting and Family Support Centre is partly funded by royalties stemming from published resources of the Triple P – Positive Parenting Program, which is developed and owned by The University of Queensland (UQ). Royalties are also distributed to the Faculty of Health and Behavioural Sciences at UQ and contributory authors of published Triple P resources. Triple P International (TPI) Pty Ltd is a private company licensed by UniQuest Pty Ltd on behalf of UQ, to publish and disseminate Triple P worldwide. The authors of this report have no share or ownership of TPI. At the time of publishing, Author Chainey is currently employed and Author Burke was previously employed by The University of Queensland in the Parenting and Family Support Centre.
Ethical Approval
This research study was conducted retrospectively from data obtained for the Longitudinal Study of Australian Children. We consulted extensively with the ethics committee of The University of Queensland, who granted an official waiver of ethical approval as the study uses non-identifiable secondary data and is of negligible risk (Clearance number 2017001553). All procedures performed in studies involving human participants were in accordance the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study, by the administrators of the National Health Survey 2014–15.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chainey, C., Burke, K. & Haynes, M. Relationships between Adverse Childhood Experiences and Demographic Characteristics in a National Australian Sample. J Child Fam Stud 32, 3960–3975 (2023). https://doi.org/10.1007/s10826-023-02664-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-023-02664-3