
Abstract
Early parenting programs can prevent the development of child behavioral and emotional difficulties. Despite the high prevalence of these difficulties in Greek children aged 2 to 12, no evidence-based parenting programs have been tested in randomized trials in Greece. We pilot-tested the efficacy of a brief parenting intervention for universal prevention of child behavioral and emotional difficulties. Parents from the general population (N = 124) were randomly assigned to receive the Triple P (Positive Parenting Program) Seminar Series (n = 83), or leaflet information on child health (n = 41). Most participants were highly educated mothers with boys and girls aged 2–12, from middle-income, inner-city households. Participants reported on child behavior, parenting style and parenting adjustment, before and after the intervention and six months later. At post-intervention, parent-reported behavioral problems were reduced in the intervention group, but increased in the control group (p = 0.001); these differences remained at 6-month follow-up. Of those in the clinical range (28%) at baseline, significantly more intervention children than control children moved to normal range six months later. Disrupted parenting practices were reduced more in intervention parents at post-intervention but were not maintained at follow-up. No significant differences were found in secondary child behavioral difficulties, child emotional difficulties, parenting confidence and distress over time. This Seminar Series is a brief, easily replicable and likely cost-effective early intervention leading to significant medium-sized reductions over six months in behavioral difficulties, and improvements in disrupted parenting. These findings broadly support other evidence about effective transportability of parenting interventions across countries.
Highlights
-
We examined a brief parenting program to prevent behavioral and emotional difficulties in Greek children aged 2 to 12.
-
Parents who received the Seminar Series reported significantly less child difficulties over time than control parents.
-
Parents reported significantly less disrupted parenting practices after receiving the Seminar Series but not six months later.
-
There may be clinical effects on child behavior provided that parents attended at least one seminar.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Emotional and behavioral difficulties are amongst the most common chronic problems of childhood. The prevalence of behavior problems varies globally between 2–16% (American Psychiatric Association, 2000). During toddlerhood more intense, frequent and persistent manifestations of typical emotions and behaviors may lead to the development of internalizing and externalizing difficulties in middle childhood, and generate more severe disorders later in adolescence (Gardner & Shaw, 2008). Poor academic performance, school dropout, delinquency, substance abuse, social exclusion and psychiatric disorders are some of the long-term consequences (Fergusson et al., 2005). These disorders may be disturbing to the individual and are costly to society. The average public cost of children with behavioral disorders is up to 10 times more than that of children without difficulties over their life (Scott et al., 2001).
Parenting plays a significant role in the development and maintenance of behavioral and emotional difficulties (Gardner et al., 1999). Evidence-based parent management training programs such as Triple P (Positive Parenting Program) (Sanders, 1999), The Incredible Years (Gardner et al., 2006) or Parent-Child Interaction Therapy (Eyberg et al., 1995) share similar theoretical basis and goals, promoting positive parenting and improving child behaviors. Triple P was chosen for its advantages in prevention and intervention programs, offering a unique structure, flexible delivery methods, and a population-based approach. It provides five levels of intervention, from universal prevention for the general population to targeted interventions for high-risk families. It is delivered through individual or group sessions, or self-directed resources and is tailored to the level and intensity of the family’s needs (Sanders, 1999). Lastly, it is one of the few programs that have been evaluated in real-life settings across cultures (Bodenmann et al., 2008).
Research evidence has shown increased behavioral and emotional difficulties in Southern European children compared to their counterparts in Northern and Central Europe. In an epidemiological research including 44 societies, Greece and Portugal scored above the average in behavioral and emotional difficulties and amongst the highest worldwide (Rescorla et al., 2012). This aligns with previous findings where Southern European children in Italy, Spain and Portugal shared similar levels of conduct problems (Marzocchi et al., 2004). Similarly, in a systematic review on prevalence studies we found a high prevalence of emotional and behavioral difficulties in Greek school-aged children suggesting possibilities for early prevention. These difficulties may be related to the parenting style followed by Northern and Southern European parents, as Greek and Italian parents were perceived as more authoritarian than Swedish parents (Olivari et al., 2015). Since changes in parenting practices have shown to mediate changes in child outcomes (Gardner et al., 2010), Triple P may assist parents to address the increased child difficulties in Greece. Triple P has been effectively disseminated in Northern and Central European countries like the UK, Germany, Sweden, Switzerland and the Netherlands to reduce child difficulties. Investigating the transferability of Triple P to a Southern country like Greece would be beneficial on the wider dissemination of the positive parenting program, since Greek parents rated Triple P strategies as acceptable, feasible and culturally relevant in a pilot focus group.
The dissemination of universal prevention Triple P was chosen to reach the Greek population where overall there is high prevalence of child emotional and behavioral difficulties, raise awareness about the importance of positive parenting and its impact on child development and offer psychoeducational support to all parents, including those not seeking help or at perceived risk (Sanders et al., 2008). Universal Triple P studies have examined the self-directed universal format using audio, video and written materials (O’Brien & Daley, 2011). Other universal Triple P interventions, such as universal Group Triple P, which are delivered directly to small or large parent groups to improve child and parenting behaviors, have also been extensively investigated worldwide. There is mixed evidence for the effectiveness of universal Group Triple P, and for universal parenting interventions generally, with some trials with parents of children under 8 years old showing positive child and parenting outcomes (Hahlweg et al., 2010; Prinz et al., 2009; Zubrick et al., 2005), and others showing mixed or no effects (Hiscock et al., 2008; Malti et al., 2011). Findings should be treated with caution as in some studies (Prinz et al., 2009; Zubrick et al., 2005) there may be a misuse of the word “universal”, where Triple P may have been delivered as targeted rather than universal prevention. The type of prevention used in some studies is also unclear due to poor reporting standards, including unclear recruitment process and lack of information on eligibility criteria (Hahlweg et al., 2010). High attrition rates and hence smaller sample sizes also lead to a decrease in the precision of estimates of population parameters. Lastly, all studies focused on toddlers (1–3), preschoolers (3–5) and school-aged (6–8) children, hence it is unknown whether interventions benefit teens too. Thus, definitive conclusions on the effectiveness of universal Group Triple P cannot be drawn and further investigation of universal programs is necessary to address these methodological issues and assess their effectiveness.
We could find no systematic review assessing whether universal parenting programs are effective in general, and even less is known about the effectiveness of low-cost universal preventing interventions that minimize therapist contact. The Triple P Seminar Series is a less intensive, less time-consuming and more cost-effective option, which may be more appealing to the general population. It is designed to address difficulties in children from birth to 12 years by providing strategies that can be adapted to child’s development through their delivery. Yet, its effectiveness has not been adequately investigated. Only a few studies, and none in Europe, have assessed the Seminar Series in a randomized controlled trial (RCT) and have found positive child and parenting improvements (Sanders et al., 2009; Sumargi et al., 2015), which remained at a 6-month follow-up (Sumargi et al., 2015). However, this is the first RCT on the Seminar Series that is independent of the Triple P organization, the University of Queensland that owns Triple P and affiliated researchers, and the first investigation addressing the limitations of previous studies (Sumargi et al., 2015) by employing a stringent design and a rigorous methodology. To our knowledge, no evidence-based parenting programs have been tested in RCTs in Greece.
We investigated the impact of a Triple P Seminar Series for universal prevention of behavioral and emotional difficulties in a general Greek sample of parents with children aged 2 to 12. According to the limited evidence on the effectiveness of Triple P Seminar Series and the general purposes of Triple P, it was predicted that compared to a control condition, parents randomized to the Seminar Series would report lower levels of children’s behavioral and emotional difficulties at post-intervention. It was also postulated that parents would show a decrease in disrupted parenting, greater feelings of self-efficacy as well as lower levels of distress. Lastly, any effects observed at post-intervention would remain at 6-month follow-up.
Method
The trial was registered with ClinicalTrials.gov (Registration number: NCT02030730) and is reported following the guidelines provided by the CONSORT statement on the reporting of RCTs (Schulz et al., 2010) and on other extended versions of the CONSORT statement (Boutron et al., 2008). The University of Oxford Central Research Ethics Committee approved the trial (Ref: SSD/CUREC2/12-05).
Sample
A non-governmental organization, the Network for Children’s Rights in cooperation with the Institution of Social and Preventive Medicine, organized the seminars and advertised the study to the general public through member lists, contacts with schools and health institutions, social networks, and mass media. They administered baseline assessments and the informed consent form to parents who met two eligibility criteria: having at least one child aged 2 to 12 years and living in the general area of Athens. From 167 families that applied, 124 were eligible, returned the baseline booklets and consented to participate in the RCT. Most parents were university-educated (81%), working (71%) mothers (84%) from middle-income (44%) urban households (Table 1). The mean age of the children was 5.5 years (SD = 2.19).
Measures
Parents completed an assessment booklet with questionnaires at baseline, at post-intervention and six months later. The booklet was available online or we sent it by post with a pre-paid envelope if parents had no online access. At baseline, one parent completed the booklet for all the children within the age range. The same parent completed the post- and 6-month follow-up assessments only for the child who had the highest ECBI intensity score at baseline to control for the number of children in the family as an extraneous variable. When both parents attended the seminars we asked the parent who completed the baseline assessment to fill in the other assessments.
Child Behavior
In line with previous studies, we measured behavioral problems as the primary outcome using the intensity scale of the 36-item Eyberg Child Behavior Inventory (ECBI; Eyberg & Pincus, 1999), scored on a 7-point scale. A clinical cut-off of 132 was used since it has not been standardized in Greece, may have been more precise than older, lower cut-off points (Colvin et al., 1999) and was a more conservative one. Other secondary behavioral measures included the Eyberg’s problem scale to estimate the number of behavioral difficulties seen as problematic by the parent and the 48-item Conners Parent Rating Scale (CPRS; Goyette et al., 1978) to measure conduct on a 4-point scale. The CPRS was also used to assess emotional problems using the anxiety scale.
Parent Behavior
Secondary outcomes included the 30-item Parenting Scale (PS; Arnold et al., 1993) to assess dysfunctional discipline styles on a 7-point scale, the 28-item Parenting Tasks Checklist (PTC; Sanders & Wooley, 2005) to measure parental confidence in dealing with specific child behaviors and in different settings using a 0–100 scale, and the 11-item General Health Questionnaire (GHQ; Goldberg & Williams, 1988) to assess common psychological distress on a 4-point scale.
Intervention
The Seminar Series (Level 2- Selected Triple P) includes three 90-minute seminars, covering 60 min of scripted presentation material and 30 min question time for discussion. Parents received tip sheets with the material presented at the end of each seminar. We used standardised materials to enhance the adherence of the practitioner to the protocol and principles of Triple P Organisation. Forward and back translations of all materials were strictly followed to enhance their validity. A Greek assessor of the Triple P Organisation translated the final versions of the Greek PowerPoint presentations and Tip Sheets. Triple P International published them without any charge. The researcher and accredited Triple P practitioner delivered the intervention. The free-of-charge seminars took place in a conference room of a bookshop. We provided child care services to reduce barriers to accessing the seminars. The delivery of each seminar was 2 to 4 weeks apart. We offered each seminar twice for parents who could not attend on the scheduled day.
The first seminar is entitled “The Power of Positive Parenting” and focuses on the principles of positive parenting. It presents strategies for building positive relationships between parents and their children, encouraging desirable behavior, teaching children new skills, managing misbehavior and helping parents take care of themselves. The second seminar is entitled “Raising Resilient Children” and focuses on strategies so that children learn to recognize and accept feelings, express feelings appropriately, build a positive outlook, develop coping skills and deal with negative feelings and stressful events. The last Seminar is entitled “Raising Confident, Competent Children” and focuses on strategies so that children learn to show respect to others, be considerate, have good communication and social skills, have healthy self-esteem, become a good problem solver and become independent. Although the presentations were not planned to be personalized, all examples used were adjusted to reflect the age range of children as well as the social, economic and cultural aspects of life in Greece.
In parallel, a control group received leaflet information on child health and development provided by the Greek National Health Services of the Ministry of Health. It covered topics such as vaccinations, common childhood illnesses, first aid guide on severe injuries and cuts, and nutrition. The topics did not overlap with the topics of the Seminar Series or the general purpose of the study. Control families received the seminar tip sheets after the 6-month follow-up.
Design
Randomization
We used a pragmatic randomized controlled trial design. The researcher stratified participants into permuted blocks according to three child factors (gender, age and clinical status of child behavior difficulties) to balance potential confounders across the groups. The researcher’s assistant then randomly allocated participants on a 2:1 basis, using an online computerized random integer generator. This design allows evaluation of a larger intervention sample than a 1:1 ratio with only a small loss of statistical power.
After baseline analyses, there were some administrative errors made during the stratification process. Due to an increased interest in participation, we delayed the randomization to increase the sample of the study. In addition, although we included all parents who completed child measures in the initial randomization plan, we excluded some of them later since they did not submit parenting measures. We also mistakenly stratified children according to their behavioral difficulties status (clinical, non-clinical), instead of the actual score on the intensity scale of the ECBI, which is the primary measure of the study. Thus, there were slight imbalances in child factors between the groups.
The researcher’s assistant followed the same unequal randomization process for parents who turned up uninvited to the seminars, so-called “on-the-day” or “late entries” (Clayton & Hills, 1993). Parents who were allocated to the seminar group remained in the analyses, but those allocated to the control group did not as they received the intervention, and so were not part of the trial. Figure 1 illustrates the flow of participants into and through the study.

Flow of Participants Through the Trial: Intention to Treat Analysis (ITT)
Blinding
Due to limited resources, the researcher delivered the intervention and ran the analyses. To ensure blindness the researcher’s assistant collected all data and it was shared with the researcher only after the assistant removed all participants’ identifying features. Only the assistant could identify the participants.
Data Analysis
A sample size calculator formula indicated that 130 participants would be required to achieve an effect size of 0.8 for the primary outcome at the 5% significance level with a ratio of 2:1 intervention to control. After we allowed for expected drop out of 40% based on similar studies (Sanders et al., 2009) the target population was 182 parents and the final randomized sample was 124 parents.
To check for demographic differences, we ran baseline and attrition analyses. We conducted a series of chi-squares on categorical variables, and independent sample t-tests on continuous variables to test for differences in socio-demographic variables between the allocation groups. Regarding chi-squares, we used the median of each categorical variable to convert all multinary categorical variables to binary in order to increase the power of analyses. For 2 × 2 chi-squares, we used the Pearson’s chi-square unless cells had an expected count of less than 5. In these cases, we applied the Fisher’s Exact Test.
We assessed differences between groups on all outcomes by ANCOVAs for uni-dimensional questionnaires (Conners conduct problem scale, Conners anxiety scale, four PS scales, GHQ), and MANCOVAs for multi-dimensional questionnaires (two ECBI scales, two PTC scales). To control for baseline differences in the primary outcome, results present the treatment effect as the estimated mean group difference in change scores from baseline to post-intervention controlling for baseline demographic differences in parental education and number of children in the family, at a conventional p value of 0.05, the effect sizes using Cohen’s d, and the estimated effect at 95% confidence intervals (Altman, 2005). We calculated change scores by simple subtraction, such that a positive change score represents greater improvement in the desired therapeutic direction. We reported the estimated marginal means as means scores adjusted for covariates. We further explored significant effects using pairwise comparisons to determine any significant differences between conditions. We made Bonferroni adjustments based on the number of pairwise comparisons conducted.
Intent-To-Treat and Missing Data
We included all families in an intention-to-treat (ITT) analysis irrespective of uptake of intervention using the group median score for those lost to follow-up to eliminate the effects of a severe outlier presented in the data (High, 2000). We compared these results to those who adhered strictly to the protocol in a per protocol (PP) analysis. PP analysis is restricted to the subjects who fulfilled the protocol, in terms of eligibility, interventions, and outcome assessment, so to those who adhered perfectly to the trial guidelines as specified in the protocol. PP analysis included 66 parents (40 intervention, 26 control) at post-intervention and 60 parents (35 intervention, 25 control) at 6-month follow-up.
We used the group median score at post-intervention to impute values based on existing data to eliminate the effects of a severe outlier and skewed data presented in the dataset. The mean imputation is generally “pulled” in the direction of the outliers, but the median imputation is influenced only by the most common cases, and so it is less affected by outliers or skewed data.
Results
Baseline Characteristics
At the end of a two-phase randomization, we included 124 participants in the ITT analysis, 83 from the intervention and 41 from the control group. At post-intervention 62 (75%) participants of the intervention group and 27 (66%) of the control group remained. At 6-month follow-up 52 (63%) participants of the intervention group and 27 (66%) of the control group remained.
Most participants were mothers, married, mostly university-educated, worked full-time, had average monthly family incomes and had one or two children (Table 1). There were more university-educated parents and fewer children within the families in the intervention group, compared to the control group. Regarding attrition, apart from parents’ gender, χ2 (1, N = 124) = 7.02, p = 0.008, φ = 0.24, there were more fathers who did not submit the post-assessment than expected; there were no other significant baseline differences in demographics or dependent variables. At baseline, 28% of the children were above the cut-off for conduct problems (Table 2). There was also a significant difference in the ECBI intensity scale between the intervention (M = 118.35, SD = 26.24) and control group (M = 106.53, SD = 26.29), t(122) = 2.34, p = 0.021. There were no other significant baseline differences on any variables.
Regarding the 47 participants who did not meet inclusion criteria before randomization, they seemed to match the selected sample based on these demographic characteristics. Although there were some demographic differences in terms of education, monthly income, and the age of the children, due to the small sample size, no conclusion can be drawn.
Program Attendance
Of the 83 intervention parents, 62 (75%) completed post-intervention assessments, and, of these, 42 (51%) attended all the whole Seminar Series, 20 (24%) attended two seminars, 19 (23%) attended one seminar and 2 did not attend any seminar. 21 intervention parents did not attend the entire series due to health issues, other personal arrangements or clashes with family schedules at the time of the seminars. At 6-month follow-up, 52 (63%) completed the assessments, and, of these, 36 (70%) attended all three seminars, 9 (17%) attended two seminars, and 7 (13%) attended one seminar. From the control parents, 27 (66%) completed post- and 6-month follow-up assessments, one parent dropped out and one parent moved to the intervention group. Figure 1 illustrates the exact number of seminars that participants attended.
Main Findings
Table 3 presents the main findings on child and parenting measures at post-intervention. Table 4 presents the main findings on child and parenting measures at 6-month follow-up.
Child Behavior
At post-intervention, the ITT analysis for the primary outcome, ECBI intensity scale, showed a significant reduction in behavioral problems in the intervention group, but an increase in the control group, F(1, 120) = 11.79, p = 0.001, ES = 0.74, 95% C.I. [5.70–21.23]. These effects remained at 6-month follow-up, F(1,120) = 4.87, p = 0.029, ES = 0.47, 95% C.I. [1.16 – 21.47]. In the PP analysis, no changes were found at post-intervention, F(1, 63) = 8.23, p = 0.006, ES = 0.58, 95% C.I. [5.55–31.07] and at 6-month follow-up, F(1, 57) = 7.77, p = 0.007, ES = 0.84, 95% C.I. [5.26– 32.10].
In the ITT analysis, changes on the ECBI problem scale were not significant at post-intervention, F(1, 120) = 0.07, p = 0.788 and six months later, F(1, 120) = 1.45, p = 0.230. The same outcomes were found in the PP analysis, F(1, 63) = 0.29, p = 0.594 and F(1, 57) = 3.60, p = 0.063, respectively.
For other child outcomes, in the ITT analysis, no significant changes were found on the Conners conduct problem, F(1, 120) = 2.57, p = 0.111 and anxiety scale, F(1, 120) = 1.34, p = 0.249 at post-intervention and at 6-month follow-up, F(1, 120) = 0.66, p = 0.417 and F(1, 120) = 0.98, p = 0.325, respectively. However, in the PP analysis, behavioral problems reduced significantly more in the children of adherent intervention parents on the Conners conduct problem scale, F(1, 62) = 5.36, p = 0.024, ES = 0.66, 95% C.I. [0.09–1.23]. No significant changes were found on the anxiety scale, F(1, 62) = 3.64, p = 0.061 at post-intervention. No significant changes were found on Conners conduct problem, F(1, 56) = 3.24, p = 0.077 and anxiety scale, F(1, 56) = 2.27, p = 0.137 at 6-month follow-up.
Parent Behavior
In the ITT analysis, disrupted parenting practices reduced significantly more in the intervention group, F(1, 120) = 5.51, p = 0.021, ES = 0.49, 95% C.I. [0.04–0.49] on the PS total score. The effect was not sustained at 6-month follow-up, F(1, 120) = 3.48, p = 0.065. In the PP analysis, parenting disrupted practices reduced significantly more in the adherent intervention parents at post-intervention, F(1, 62) = 6.37, p = 0.014, ES = 0.72, 95% C.I. [0.06–0.52]. Again, the effect was not sustained at 6-month follow-up, F(1, 56) = 0.81, p = 0.371.
In the ITT analysis, no significant changes were found on the PTC setting, F(1, 120) = 0.58, p = 0.450 and behavioral scales, F(1, 120) = 2.64, p = 0.107 at post-intervention and at 6-month follow-up, F(1,120) = 1.29, p = 0.258 and F(1, 120) = 1.50, p = 0.224, respectively. In the PP analysis, no significant changes were found on the PTC setting scale, F(1, 63) = 3.21, p = 0.078 at post-intervention and at 6-month follow-up, F(1,57) = 3.26, p = 0.076. However, parental confidence in dealing with specific child behaviors increased significantly more at adherent intervention parents, F(1,63) = 6.49, p = 0.013, ES = 0.73, 95% C.I. [1.54–12.76]. The effect was not sustained at 6-month follow-up, F(1,57) = 2.44, p = 0.124.
In the ITT analysis, no significant change were found on the GHQ at post-intervention, F(1,120) = 0.16, p = 0.686 and at 6-month follow-up, F(1,120) = 0.003, p = 0.959. The same outcomes were found in the PP analysis, F(1,62) = 0.04, p = 0.844 and F(1,56) = 1.30, p = 0.259, respectively.
Association between Number of Seminars and Outcomes
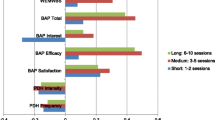
In an ITT analysis, there was a significant association for the number of seminars attended and outcomes on the ECBI intensity scale, F(3,116) = 5.21, p = 0.002, and on the Conners conduct disorder scale, F(3,116) = 3.61, p = 0.016 at post-intervention. After making Bonferroni adjustments for six different comparisons (p = 0.008), there was a significant difference only in ECBI intensity scores between those who attended all three seminars and those in the control group, p = 0.001 (Μdiff = 16.81, SE = 4.43, p = 0.001, ES = 5.60, 95% C.I. [4.92–28.71]. At 6-month follow-up, the associations remained significant; however, the adjusted mean group differences in change scores were no longer significant after Bonferroni adjustments.
Parents who attended the whole Seminar Series than control parents reported similar improvements in child behaviors for ECBI intensity scale, the mean group difference in change scores was 16.55 points, F(2, 77) = 10.48, p = 0.002, ES = 0.82, 95% C.I. [6.37–26.73] and for Conners conduct disorders scale, the mean group difference in change scores was 3.41 points, F(2, 77) = 5.41, p = 0.023, ES = 0.59, 95% C.I. [0.49–6.32]; at 6-month follow-up, the effect remained significant on the ECBI intensity scale, the mean group difference in change scores was 14.48 points, F(2, 77) = 5.66, p = 0.020, ES = 0.60, 95% C.I. [2.36–26.61]. The effect did not remain significant on the Conners conduct disorders scale, F(2, 77) = 1.06, p = 0.307. Disrupted parenting practices were also reduced more in those who attended the whole Seminar Series than in the control group at post-intervention. The mean group difference in change scores was 0.30 points on the PS total score, F(2, 77) = 7.83, p = 0.006, ES = 0.71, 95% C.I. [0.09–0.51]. The effect remained significant at 6-month follow-up, the mean group difference in change scores was 0.26, F(2, 77) = 4.05, p = 0.048, ES = 0.51, 95% C.I. [0.003–0.50]. Overall, attending all seminars resulted in more positive changes in child difficulties and disrupted parenting practices than being in the control group.
Clinical Change
At baseline, 31% (n = 26) of intervention children and 22% of control children (n = 9) were above the clinical range on ECBI intensity scale. At post-intervention, 54% (n = 14) of intervention children and 44% of control children (n = 4) moved from the clinical to non-clinical range. At 6-month follow-up, 65% (n = 17) of intervention children and 11% of control children (n = 1) moved from the clinical to non-clinical range. Using Chi-square analyses, there was no significant difference in the number of children who moved from the clinical range to the non-clinical range and those who remained at the clinical range between the groups at post-intervention (exact p = 0.711). At 6-month follow-up this difference was significant (exact p = 0.007, two-tailed, V = 0.48, 50% of the cells had an expected frequency of less than 5). More children moved from the clinical range to the non-clinical range in the Seminar group (n = 17, 65%), and more children remained at the clinical range in the control group (n = 8, 89%). The relative risk was 5.88, 95% C.I. [1.43–33.33] and the relative difference was 0.54, 95% C.I. [0.17–0.75].
Discussion
In this pilot randomized controlled trial, Triple P Seminar Series appeared to improve behavioral difficulties in pre- and school-aged Greek children. Medium effect sizes and significant differences at post-intervention indicated that this brief parenting intervention had a positive effect on child behavioral difficulties, which remained at 6-month follow-up. The Seminar Series may be also beneficial to parents who have children in the clinical range for behavioral problems.
The Seminar Series also affected parenting as disrupted parenting practices were reduced more in the intervention parents at post-intervention; however, these differences were not sustained six months later. Similar results were found in the PP analysis. These findings suggest that changes in child behavior may be mediated through improving disrupted parenting practices at least in the short term. Children whose parents attended all three seminars were more likely to display fewer behavioral difficulties, and parents were more likely to reduce disrupted parenting practices over time. These findings suggest the importance of attending the whole series for improving child and parent behavior.
To our knowledge, this is the first European study on the Seminar Series, and findings are consistent with the outcomes on other Triple P interventions in European countries such as Germany (Hahlweg et al., 2010) and Switzerland (Bodenmann et al., 2008). The results found in this study are broadly in line with the findings reported in studies on the Seminar Series conducted in Australia (Sanders et al., 2009) and results from Indonesia (Sumargi et al. 2015). In all studies, parents reported significantly fewer child behavioral difficulties after attending the Seminar Series than those in the control group. In both the Australian and our study, 50% of the children who were above the clinical range pre-intervention moved to non-clinical range post-intervention on child behavior scales provided that their parents attended at least one seminar. No significant effect was found on child emotional difficulties in all three studies.
Parents reported significant improvement in their parenting skills at post-intervention in all studies. Yet, in a pre-post study in Canada, although parents who attended the Seminar Series reduced shaking or grabbing their child, non-physical punishment and non-punitive punishment did not change over time. Specifically, parents were more likely to emphasize rules and punish their children by taking things away from them (Gonzalez et al., 2019). Parental confidence and parental adjustment were increased only in the Indonesian study. The Parenting Scale was used in all three studies to measure disrupted parenting, but different measures for parental confidence and parental adjustment were used in the Indonesian study.
Other universal brief parenting programs which have been investigated in RCTs with parents of children aged 2 to 5 and 6 to 12 demonstrated either no difference in child behavior measures (Hiscock et al., 2008) or a significant decrease in the short-term (Bradley et al., 2003), while our study was the only one to demonstrate improvement at both time points. In addition, positive effects on parenting measures were maintained over time, in contrast with our findings (Bayer et al., 2010; Bradley et al., 2003; Hiscock et al., 2008). This could be because it was the first time that positive parenting was introduced to Greek parents. Greek parents have been reported to use strict discipline practices including physical punishment, have high expectations regarding academic achievement and are overprotective of their children, showing a mix of permissive and authoritarian parenting style, and so resulting in dependent children (Tsiantis et al., 1982). Other Southern European and Latin American parents use permissive parenting too, which has been linked to increased behavioral and emotional difficulties (García & Gracia, 2014). So, Greek, and it may be that Southern European and Latin American parents need more time to change permissive and authoritarian practices and assimilate the authoritative style proposed by Triple P.
The Seminar Series produced medium effects on child and parenting measures at post-intervention despite baseline imbalances on the primary outcome, non-significant changes on some measures, and a slight decrease in power from 80 to 75% due to unequal randomization. Changes in child behavioral problems were maintained over six months. Surprisingly, changes on secondary behavioral scales were not significant. This may be because changes were not robust enough to show on all measures. The ECBI may also be more sensitive when measuring child behavior problems, while CPRS is more sensitive to treatment effects when measuring specific neurodevelopmental disorders such as ADHD. Although one seminar was based on the development of resilience in children, the Seminar Series does not appear to prevent child emotional difficulties. This may be due to the rapid changes in the development of emotions, especially in the early years as well as the inability for young children to clearly communicate about emotions. It is also hard for adults to differentiate developmentally typical emotions from more severe and prolonged anxiety that might be seen as a disorder, and recognize them as problematic (Gardner & Shaw, 2008).
Regarding parenting practices, it seemed that disrupted practices reduced significantly more in intervention parents; yet, this effect did not remain six months later. The Seminar Series promotes positive parenting practices but having no further contact with the practitioner, parents could rely on the tip sheets that they received at the end of each seminar to review the strategies. However, parents may have forgotten what they learned, may not have reviewed the material, or may start being less consistent when applying the strategies. We speculate that the Seminar Series modifies parental cognitions temporarily, but parents may revert to preconceptions in the long term or be inconsistent with their practices. For this reason, it might be useful to provide additional, brief, booster sessions at least six months after the parents have completed the Seminar Series. It may also be helpful for parents to attend all seminars so that their children and themselves benefit most from the intervention, although causal inferences cannot be drawn from our data, as parents were not randomly allocated to a specific number of seminars. Any improvement in child or parenting outcomes could be due to full attendance or higher commitment to their children, better organizational skills, better response to the intervention or other factors linked to their baseline characteristics. No changes were found in parents’ general distress after the intervention, as they might have struggled to moderate their daily life stress due to a recession in Greece (Kentikelenis et al., 2014).
To test the robustness of the results, we also carried out statistical analyses using the LOCF method. All significant results of post-intervention and 6-month follow-up analyses using the group median were also significant using the LOCF. It was also found that in contrast to the non-significant results in emotional difficulties as measured by Conners anxiety scale using the group median, intervention children now improved significantly more than control children at post-intervention and at 6-month follow-up.
This study contributes to the literature on the efficacy of Triple P Seminar Series, as we conducted a rigorous RCT to overcome previous methodological issues (Sumargi et al., 2015). Specific procedures during recruitment and before randomization were followed to reduce attrition rates. Eligibility criteria were clearly set to enhance external validity. Although the seminar provider was also the outcome assessor, blinding was followed to avoid assessment bias. The standardized and scripted materials helped to ensure high level of fidelity. Finally, this study was independent of the developer, affiliates of the organization and no Triple P staff contributed at any methodological or evaluation stage (Eisner, 2009). There was no financial or non-financial conflict of interest that may result in potential sources of bias (Montgomery & Weisman, 2021). Lastly, in parent training interventions attrition rates may be as high as 50% at follow-up (Gallagher, 2003); yet, in this study there was 28% attrition rate at post-intervention, and 36% at 6-month follow-up.
The current findings have significant importance as their reliability across cultures strengthens the idea that the Seminar Series is a brief and replicable universal prevention parenting program that provides information relevant to the needs of a greater number of parents, rather than being restricted to those with concerns or existing problems. Moreover, such intervention is less time-consuming as it requires a low time commitment from parents, and may be more cost-effective as it uses minimal therapist contact and minimal parenting resources. Thus, a whole population might greatly benefit from such a feasible, scalable and deliverable intervention. It may be a promising evidence-based prevention and intervention strategy that could potentially have an impact on population levels of behavioral and emotional problems not only in Greece and in other countries in South Europe with increased child difficulties, but also in other cultures where permissive or authoritarian parenting styles are practised. Therefore, parenting prevention programs could be considered for population-based approaches in Europe.
The study has some limitations. In psychosocial trials, blinding of the participants to allocation is hard to achieve, and so intervention parents may have responded more favorably (Macpherson, 2004). Secondly, it was important to control for substantial baseline differences in the primary outcome. To estimate the effect of the treatment on the outcome, we used change scores instead of including baseline scores as a separate covariate to avoid any addition power reduction (Austin et al., 2010). Also, as non-ITT analyses lose the balance of randomization and are based on small sample sizes, non-ITT findings should be interpreted with caution. Additionally, generalizations should be avoided due to the broad age range of children and so subgroup analyses on pre-school and school-aged children could inform us on the effects of the intervention across key developmental stages. However, didactic seminars may be hard to tailor to different ages. In contrast to seminars, group-based programs work well across a range of ages, presumably as some tailoring can be done within the longer discussions during group-based (or individual) regular programs or discussions. A systematic review and meta-analysis of parenting interventions showed that narrower age ranges, presumably with more age-tailored programs did not produce larger effects than regular parenting programs (Gardner et al., 2019). Lastly, measures were based on parental reports and were not triangulated with reports from other sources, such as teachers or independent behavioral observations. However, different child measures were used to check for possible inconsistencies in the primary outcome.
Future research may focus on the causal mechanisms between the intervention and improvements in child outcomes, and explore their direction and magnitude through moderator and mediator analyses. Based on previous studies, positive parenting and parent-child interactions (Parkes & Sweeting, 2018), or reduction in disrupted parenting (Beauchaine et al., 2005) would improve child problem behavior.
Studies should examine parenting skills using independent behavioral observations or reports from other sources to eliminate self-report biases. Since mothers were overrepresented in this sample, future studies should equally focus on fathers, their perspectives and role in other “traditional” cultures. For clinical and training purposes, it would be useful to determine the exact number of seminars necessary for child and parent improvements to reduce time and cost barriers. Also, the effects of brief, group parenting interventions on clinical samples need to be further investigated. Research exploring parental perceptions on the acceptability, feasibility and cultural relevance of the program would shed light on the mechanisms of change in parenting and child measures, and we could possibly improve different aspects of the program.
References
Altman, D. G. (2005). Confidence intervals. In: S. Straus, W. S. Richardson, R. B Haynes, P. Glasziou, & R. B. Haynes (Eds.). Evidence-based medicine. How to practice and teach EBM, (3rd ed., pp. 263–277). Churchill-Livingstone.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.).
Arnold, D. S., O’Leary, S. G., Wolff, L. S., & Acker, M. M. (1993). The Parenting Scale: A measure of dysfunctional parenting in discipline situations. Psychological Assessment, 5(2), 137–144. https://doi.org/10.1037/1040-3590.5.2.137.
Austin, P. C., Manca, A., Zwarenstein, M., Juurlink, D. N., & Stanbrook, M. B. (2010). Covariate adjustment in RCTs results in increased power to detect conditional effects compared with the power to detect unadjusted or marginal effects. Journal of Clinical Epidemiology, 63(12), 1392–1393. https://doi.org/10.1016/j.jclinepi.2010.05.004.
Beauchaine, T., Webster-Stratton, C., & Reid, M. J. (2005). Mediators, moderators, and predictors of one-year outcomes among children treated for early-onset conduct problems: A latent growth curve analysis. Journal of Consulting and Clinical Psychology, 73(3), 371–388. https://doi.org/10.1037/0022-006X.73.3.371.
Bayer, J. K., Hiscock, H., Ukoumunne, O. C., Scalzo, K., & Wake, M. (2010). 3-year-old outcomes of a brief universal parenting intervention to prevent behaviour problems: Randomised controlled trial. Archives of Disease in Childhood, 95(3), 187–192. https://doi.org/10.1136/adc.2009.168302.
Bradley, S. J., Jadaa, D. A., Brody, J., Landy, S., Tallett, S. E., Watson, W., Shea, B., & Stephens, D. (2003). Brief psychoeducational parenting program: An evaluation and 1-year follow-up. Journal of the American Academy of Child and Adolescent Psychiatry, 42(10), 1171–1178. https://doi.org/10.1097/00004583-200310000-00007.
Bodenmann, G., Cina, A., Ledermann, T., & Sanders, M. R. (2008). The efficacy of Positive Parenting Program (Triple P) in improving parenting and child behaviour: A comparison with two other treatment conditions. Behaviour Research and Therapy, 46, 411–427. https://doi.org/10.1016/j.brat.2008.01.001.
Boutron, I., Moher, D., Altman, D. G., Schulz, K. F., & Ravaud, P., CONSORT Group. (2008). Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Annals of Internal Medicine, 148(4), 295–309. https://doi.org/10.7326/0003-4819-148-4-200802190-00008.
Clayton, D., & Hills, M. (1993). Statistical Models in Epidemiology. Oxford University Press.
Colvin, A., Eyberg, S. M., & Adams, C. (1999). Restandardization of the Eyberg Child Behavior Inventory. University of Florida, Child Study Laboratory.
Eisner, M. (2009). No effects in independent prevention trials. Can we reject the cynical view? Journal of Experimental Criminology, 5(2), 163–183. https://doi.org/10.1007/s11292-009-9071-y.
Eyberg, S. M., Boggs, S. R., & Algina, J. (1995). Parent-child interaction therapy: A psychosocial model for the treatment of young children with conduct problem behaviour and their families. Psychopharmacology Bulletin, 31(1), 83–91.
Eyberg, S. M., & Pincus, D. (1999). Eyberg child behavior inventory and Sutter-Eyberg student behavior inventory-revised professional manual. Psychological Assessment Resources.
Fergusson, D. M., Horwood, J. L., & Ridder, E. M. (2005). Show me the child at seven: The consequences of conduct problems in childhood for psychosocial functioning in adulthood. Journal of Child Psychology and Psychiatry, 46(8), 837–849. https://doi.org/10.1111/j.1469-7610.2004.00387.x.
Gallagher, N. (2003). Effects of parent-child interaction therapy on young children with disruptive behavior disorders. Bridges: Practice-Based Research Syntheses, 1(4), 1–17.
García, F., & Gracia, E. (2014). The indulgent parenting style and developmental outcomes in South European and Latin American countries. In H. Selin ed, Parenting across cultures: Childrearing, motherhood and fatherhood in non-Western cultures (Vol. 7, pp. 419–433). Springer. https://doi.org/10.1007/978-94-007-7503-9_31.
Gardner, F., Sonuga-Barke, E., & Sayal, K. (1999). Parents anticipating misbehaviour. An observational study of strategies parents use to prevent conflict with behaviour problem children. Journal of Child Psychology and Psychiatry, 40, 1185–1196.
Gardner, F., Burton, J., & Klimes, I. (2006). Randomised controlled trial of a parenting intervention in the voluntary sector for reducing child conduct problems: outcomes and mechanisms of change. Journal of Child Psychology and Psychiatry, 47, 1123–1132. https://doi.org/10.1111/j.1469-7610.2006.01668.x.
Gardner, F., & Shaw, D. S. (2008). Behavioural problems of infancy and pre-school children. In M. Rutter, D. Bishop, D. Pine, S. Scott, J. Stevenson, E. Taylor, & A. Thapar (Eds.). Rutter’s child and adolescent psychiatry (5th ed., pp. 882–894). Blackwell Press.
Gardner, F., Hutchings, J., Bywater, T., & Whitaker, C. (2010). Who benefits and how does it work? Moderators and mediators of outcome in an effectiveness trial of a parenting intervention. Journal of Clinical Child and Adolescent Psychology, 39, 568–580. https://doi.org/10.1080/15374416.2010.486315.
Gardner, F., Leijten, P., Melendez-Torres, G. J., Landau, S., Harris, V., Mann, J., Beecham, J., Hutchings, J., & Scott, S. (2019). The earlier the better? Individual participant data and traditional meta‐analysis of age effects of parenting interventions. Child Development, 90(1), 7–19. https://doi.org/10.1111/cdev.13138.
Goldberg, D., & Williams, P. (1988). A users guide to the general health questionnaire. NFER-Nelson.
Gonzalez, M., Ateah, C. A., Durrant, J. E., & Feldgaier, S. (2019). The impact of the Triple P Seminar Series on Canadian parents’ use of physical punishment, non-physical punishment and non-punitive responses. Behaviour Change, 36(2), 102–120. https://doi.org/10.1017/bec.2019.7.
Goyette, C. H., Conners, C. K., & Ulrich, R. F. (1978). Normative data for revised Conners parent and teacher rating scales. Journal of Abnormal Child Psychology, 6(2), 221–236. https://doi.org/10.1007/BF00919127.
Hahlweg, K., Heinrichs, N., Kuschel, A., Bertram, H., & Naumann, S. (2010). Long-term outcome of a randomized controlled universal prevention trial through a positive parenting program: Is it worth the effort. Child and Adolescent Psychiatry and Mental Health, 4(14), 14–27. https://doi.org/10.1186/1753-2000-4-14.
High, R. (2000). Dealing with ‘outliers’: How to maintain your data’s integrity. University of Oregon. Computing News, 15(3), 14–16. http://hdl.handle.net/1794/3129.
Hiscock, H., Bayer, J. K., Price, A., Ukoumunne, O. C., Rogers, S., & Wake, M. (2008). Universal parenting programmer to prevent early childhood behavioural problems: Cluster randomised trial. British Medical Journal, 336(7639), 318–324. https://doi.org/10.1136/bmj.39451.609676.AE.
Kentikelenis, A., Karanikolos, M., Reeves, A., McKee, M., & Stuckler, D. (2014). Greece’s health crisis: from austerity to denialism. Lancet, 383(9918), 748–753. https://doi.org/10.1016/S0140-6736(13)62291-6.
Macpherson, H. (2004). Pragmatic clinical trials. Complementary Therapies in Medicine, 12(2-3), 136–140. https://doi.org/10.1016/j.ctim.2004.07.043.
Malti, T., Ribeaud, D., & Eisner, M. P. (2011). The effects of two universal preventive interventions to reduce children’s externalizing behavior: A cluster-randomized controlled trial. Journal of Clinical Child and Adolescent Psychology, 40(5), 677–692. https://doi.org/10.1080/15374416.2011.597084.
Marzocchi, G. M., Capron, C., di Pietro, M., Tauleria, E. D., Duyme, M., Frigerio, A., Gaspar, M. F., Hamilton, H., Pithon, G., Simões, A., & Thérond, C. (2004). The use of the strenghts and difficulties questionnaires (SDQ) in Southern European countries. European Child & Adolescent Psychiatry, 13(2), 40–46. https://doi.org/10.1007/s00787-004-2007-1.
Montgomery, P., & Weisman, C. B. (2021). Non-financial conflict of interest in social intervention trials and systematic reviews: An analysis of the issues with case studies and proposals for management. Children and Youth Services Review, 120, 105642. https://doi.org/10.1016/j.childyouth.2020.105642.
O’Brien, M., & Daley, D. (2011). Self-help parenting interventions for childhood behaviour disorders: A review of the evidence. Child: Care, Health and Development, 37(5), 623–637. https://doi.org/10.1111/j.1365-2214.2011.01231.x.
Olivari, M. G., Hertfelt Wahn, E., Maridaki-Kassotaki, K., Antonopoulou, K., & Confalonieri, E. (2015). Adolescent Perceptions of Parenting Styles in Sweden, Italy and Greece: An Exploratory Study. Europe’s Journal of Psychology, 11(2), 244–258. https://doi.org/10.5964/ejop.v11i2.887.
Parkes, A., & Sweeting, H. (2018). Direct, indirect, and buffering effects of support for mothers on children’s socioemotional adjustment. Journal of Family Psychology, 32(7), 894–903. https://doi.org/10.1037/fam0000438.
Prinz, R. J., Sanders, M. R., Shapiro, C., Whitaker, D., & Lutzker, J. (2009). Population-based prevention of child maltreatment: The U.S. Triple P System population trial. Prevention Science, 10(1), 1–13. https://doi.org/10.1007/s11121-009-0123-3.
Rescorla, L. A., Ivanova, M. Y., Achenbach, T. M., Begovac, I., Chahed, M., Drugli, M. B., Emerich, D. R., Fung, D. S., Haider, M., Hansson, K., Hewitt, N., Jaimes, S., Larsson, B., Maggiolini, A., Marković, J., Mitrović, D., Moreira, P., Oliveira, J. T., Olsson, M., & Zhang, E. Y. (2012). International epidemiology of child and adolescent psychopathology II: Integration and applications of dimensional findings from 44 societies. Journal of the American Academy of Child and Adolescent Psychiatry, 51(12), 1273–1283.e8. https://doi.org/10.1016/j.jaac.2012.09.012.
Sanders, M. R. (1999). The Triple P-Positive parenting program: Towards an empirically validated multilevel parenting and family support strategy for the prevention of behaviour and emotional problems in children. Clinical Child and Family Psychology Review, 2(2), 71–90. https://doi.org/10.1023/a:1021843613840.
Sanders, M. R., Prior, J., & Ralph, A. (2009). An evaluation of a brief universal seminar series on positive parenting: A feasibility study. Journal of Children’s Services, 4(1), 4–20. http://www.metapress.com/content/c576165738350w56/fulltext.pdf.
Sanders, M. R., Ralph, A., Sofronoff, K., Gardiner, P., Thompson, R., Dwyer, S., & Bidwell, K. (2008). Every family: A population approach to reducing behavioral and emotional problems in children making the transition to school. Journal of Primary Prevention, 29(3), 197–222. https://doi.org/10.1007/s10935-008-0139-7.
Sanders, M. R., & Woolley, M. L. (2005). The relationship between maternal self-efficacy and parenting practices: Implications for parent training. Child: Care, Health and Development, 31(1), 65–73. https://doi.org/10.1111/j.1365-2214.2005.00487.x.
Schulz, K. F., Altman, D. G., & Moher, D. (2010). Consort 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Medicine, 8(18). https://doi.org/10.1186/1741-7015-8-18.
Scott, S., Knapp, M., Henderson, J., & Maughan, B. (2001). Financial cost of social exclusion: follow-up study of antisocial children into adulthood. British Medical Journal, 323(7306), 1–5. https://doi.org/10.1136/bmj.323.7306.191.
Sumargi, A., Sofronoff, K., & Morawska, A. (2015). A randomized-controlled trial of the Triple P-Positive Parenting Program Seminar Series with Indonesian parents. Child Psychiatry & Human Development, 46(5), 749–761. https://doi.org/10.1007/s10578-014-0517-8.
Tsiantis, J., Mardikian-Gazerian, B., Sipitanou, A., & Tata-Stamboulopoulou, L. (1982). Child Mental Health and Psychosocial Development: National Case Study. Unpublished report to WHO.
Zubrick, S. R., Ward, K. A., Silburn, S. R., Lawrence, D., Williams, A. A., Blair, E., Robertson, D., & Sanders, M. R. (2005). Prevention of child behavior problems through universal implementation of a group behavioral family intervention. Prevention Science, 6(4), 287–304. https://doi.org/10.1007/s11121-005-0013-2.
Acknowledgements
The Triple P–Positive Parenting Program is owned by the University of Queensland. No author has any share or ownership in Triple P International Pty Ltd.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Foskolos, K., Gardner, F. & Montgomery, P. Brief Parenting Seminars for Preventing Child Behavioral and Emotional Difficulties: a Pilot Randomized Controlled Trial. J Child Fam Stud 32, 3063–3075 (2023). https://doi.org/10.1007/s10826-023-02653-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10826-023-02653-6