
Abstract
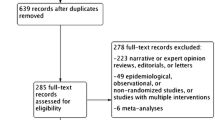
Although mineralocorticoid antagonists (MRAs) have been proposed as effective fourth-line blood pressure (BP) lowering agents in resistant hypertension, this effect in heart failure is undetermined. In this synthesis of heart failure randomized controlled trials (RCTs), we evaluated the extent of BP lowering following MRA treatment against placebo. We searched Medline and the Cochrane Collaboration Library databases from 1991 to September 2016 for RCTs, in which MRAs were compared with placebo. The quality of RCTs was assessed with Cochrane risk of bias tool. Outcomes were the extent of systolic and diastolic BP lowering. We included seven studies (13,354 patients, 65.8% males, mean age of 66.3 years, mean follow-up period of 9.4 months, mean baseline BP of 123.5/75.0 mmHg) of MRAs compared with placebo. MRAs were not significantly associated with systolic − 1.8 (95% CI: − 8.0, 4.4) mmHg or diastolic − 0.3 (95% CI: − 3.4, 2.7) mmHg, BP reduction. Although systolic BP was not lowered by spironolactone, diastolic BP was lowered by − 3.0 (95% CI: − 3.4, − 2.6) mmHg. Eplerenone treatment did not significantly lowered systolic [− 0.04 (95% CI: − 4.4, 4.3) mmHg], but it was associated with minimal diastolic BP increase [1.0 (95% CI: 0.5, 1.53) mmHg]. MRAs were not associated with systolic and diastolic BP reduction in heart failure patients. This finding suggests that MRAs should be used according to their indications in heart failure independently of initial BP levels.




Similar content being viewed by others


Abbreviations
- BP:
-
blood pressure
- MRA:
-
mineralocorticoid antagonists
References
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ et al (2016) 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)developed with the special contribution of the heart failure association (HFA) of the ESC. Eur Heart J 37:2129–2200
Zannad F (2007) Aldosterone antagonist therapy in resistant hypertension. J Hypertens 25:747–750
Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Bohm M et al (2013) 2013 ESH/ESC guidelines for the Management of Arterial Hypertension: The task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 34:2159–2219
Bazoukis G, Thomopoulos C, Tsioufis C (2017) Effect of mineralocorticoid antagonists on blood pressure lowering: overview andmeta-analysis of randomized controlled trials in hypertension journal of hypertension:35
Rossignol P, Claggett B, Liu J, Vardeny O, Pitt B, Zannad F, et al. (2017) Spironolactone and resistant hypertension in heart failure with preserved ejection fraction. American journal of hypertension.
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 339:b2535
Edelmann F, Wachter R, Schmidt AG, Kraigher-Krainer E, Colantonio C, Kamke W et al (2013) Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction: The Aldo-DHF randomized controlled trial. JAMA 309:781–791
Mottram PM, Haluska B, Leano R, Cowley D, Stowasser M, Marwick TH (2004) Effect of aldosterone antagonism on myocardial dysfunction in hypertensive patients with diastolic heart failure. Circulation 110:558–565
Deswal A, Richardson P, Bozkurt B, Mann DL (2011) Results of the randomized aldosterone antagonism in heart failure with preserved ejection fraction trial (RAAM-PEF). J Card Fail 17:634–642
Zannad F, McMurray JJ, Krum H, van Veldhuisen DJ, Swedberg K, Shi H et al (2011) Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med 364:11–21
Mak GJ, Ledwidge MT, Watson CJ, Phelan DM, Dawkins IR, Murphy NF et al (2009) Natural history of markers of collagen turnover in patients with early diastolic dysfunction and impact of eplerenone. J Am Coll Cardiol 54:1674–1682
Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B et al (2003) Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 348:1309–1321
Pitt B, Pfeffer MA, Assmann SF, Boineau R, Anand IS, Claggett B et al (2014) Spironolactone for heart failure with preserved ejection fraction. N Engl J Med 370:1383–1392
Jorde UP, Vittorio T, Katz SD, Colombo PC, Latif F, Le Jemtel TH (2002) Elevated plasma aldosterone levels despite complete inhibition of the vascular angiotensin-converting enzyme in chronic heart failure. Circulation 106:1055–1057
Thomopoulos C, Parati G, Zanchetti A (2016) Effects of blood pressure lowering treatment in hypertension: 8. Outcome reductions vs discontinuations because of adverse drug events - meta-analyses of randomized trials. J Hypertens 34:1451–1463
Berbenetz NM, Mrkobrada M (2016) Mineralocorticoid receptor antagonists for heart failure: Systematic review and meta-analysis. BMC Cardiovasc Disord 16:246
Pitt B, Kober L, Ponikowski P, Gheorghiade M, Filippatos G, Krum H et al (2013) Safety and tolerability of the novel non-steroidal mineralocorticoid receptor antagonist BAY 94-8862 in patients with chronic heart failure and mild or moderate chronic kidney disease: A randomized, double-blind trial. Eur Heart J 34:2453–2463
Filippatos G, Anker SD, Bohm M, Gheorghiade M, Kober L, Krum H et al (2016) A randomized controlled study of finerenone vs. eplerenone in patients with worsening chronic heart failure and diabetes mellitus and/or chronic kidney disease. Eur Heart J 37:2105–2114
Sato N, Ajioka M, Yamada T, Kato M, Myoishi M, Yamada T et al (2016) A randomized controlled study of Finerenone vs. Eplerenone in Japanese Patients With Worsening Chronic Heart Failure and Diabetes and/or Chronic Kidney Disease Circulation Journal. Official J Japanese Circulation Soc 80:1113–1122
Brown MJ (2007) Renin: friend or foe? Heart 93:1026–1033
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare no conflict of interest regarding the overview and meta-analyses, but C.Th. declares consultancy fees from Astra Zeneca, and lecture honoraria from Sanofi, MSD, and Servier.
Electronic supplementary material
ESM 1
(DOCX 412 kb)
Rights and permissions
About this article

Cite this article
Bazoukis, G., Thomopoulos, C., Tse, G. et al. Is there a blood pressure lowering effect of MRAs in heart failure? An overview and meta-analysis. Heart Fail Rev 23, 547–553 (2018). https://doi.org/10.1007/s10741-018-9689-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10741-018-9689-9