
Abstract
The 2030 Agenda for sustainable development was launched to achieve Sustainable Development Goals (SDGs) across the globe. This paper is based on the primary database to assess the nutritional status of 5–10 years children and the incidence of deprivation in their households of a backward district (Purulia), India in the context of the first two SDGs, e.g., no poverty and zero hunger. We conclude that around 74% of children are undernourished. The proportion of households multidimensionally deprived is 90%, and the majority of them live on less than $1.25 a day. Results reveal that the BMI of mother and the education of father are the two most statistically significant predictors of child malnutrition. Purulia has long been witnessing the persistent nature of deprivation, which is well reflected in the child’s health. The district is quite far from the national targets in achieving the SDGs. Government, private sector, and civil society must come together to accelerate the progress of SDGs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
The Global Hunger Index (GHI) of 2020 reveals that India ranks 94th (‘serious’ condition as per GHI score) out of 107 countries of the world based on the four indicators, such as undernourishment, wasting, stunting and mortality rate of under 5 years children; and India is much behind than Sri Lanka (64th), Nepal (73rd), Bangladesh (75th), Myanmar (78th) and Pakistan (88th), while the global average of hunger in terms of GHI is assessed as ‘moderate’ level. Globally, there are 690 million people are found to be undernourished (Global Hunger Index, 2020). In the case of under 5 years children, around 144 million (21.30%) and 47 million (6.90%) children suffer from stunting (prolonged malnutrition) and wasting (acute malnutrition), respectively, where India records the highest prevalence of wasted children in the world (Global Hunger Index, 2020; UNICEF et al., 2020). There were 149 million (21.90%) stunted and 49 million (7.30%) wasted children in 2018, and a declining global trend is observed for both cases. It was reported that Asia was the home to the highest number of wasted (68%) and stunted (55%) children under 5 years of age in the world in 2018 (UNICEF et al., 2019). Around 5.3 million children died in 2018 before completing their fifth birthday, in several cases as a result of severe undernutrition (Global Hunger Index, 2020). The Human Development Report (HDR), 2020 of the United Nations Development Programme (UNDP) unveils that the average Human Development Index (HDI) of the world is 0.737 and belongs to the ‘high human development’ category, while India slips two steps down from its earlier position and belongs to ‘medium human development’ category with the rank of 131st (0.645) out of 189 countries. These statistics indicate the incidence of poverty, hunger, and malnutrition mainly in developing countries of the world (UNDP, 2020a).
Several global, national, and regional organizations set up several goals at different times to eradicate different types of inequalities and deprivations from the world. The ‘Millennium Development Goals’ (MDGs) of the United Nations (UN) came into being in September 2000 with 8 goals for the world to be achieved by the year 2015. All the signed nations agreed and committed to fighting against poverty and hunger, illiteracy, gender inequality, child mortality, poor maternal health, diseases, environmental degradation, and developing global partnership for development (Binagwahoet al., 2011; Manyike et al., 2014; Pomati & Nandy, 2019). This initiative yielded success by rescuing millions of people from the paw of severe poverty and hunger, illiteracy, diseases, and other unpleasant situations, but the work was not completed within the time frame of 15 years. Thus, the 2030 Agenda came up with 17 ‘Sustainable Development Goals’ (SDGs) to be achieved by 2030. Among those goals of SDGs, no poverty and zero hunger are mainly common between MDGs and SDGs (Abbott & Bernstein, 2015; Blanc, 2015; Pomati & Nandy, 2019).
In the case of India, the National Family Health Survey (NFHS-4) of 2017 reveals that the proportion of stunted, wasted, and underweight children under 5 years was 38.40%, 21%, and 35.80%, respectively, while the child mortality rate was 50 per thousand live births. Only the percentage of wasted children increased in NFHS-4 (2021) compared to NFHS-3 (19.80%) of 2005-06. In the case of West Bengal (a state of India), under 5 stunted, wasted, and underweight children were 32.50%, 20.30%, and 31.60%, respectively. Here, also the percentage of wasted children is higher than the NFHS-3. The under 5 child mortality rate was found to be 32 for West Bengal, while it was 38 for rural Bengal (IIPS, 2017). It is quite clear from NFHS reports that the phenomenon of undernutrition is very much prevalent in India, and West Bengal is no exception (IIPS, 2017, 2021).
It is observed from NFHS-3 and NFHS-4 reports that the scenario of child malnutrition in West Bengal is lower than the national average, but the prevalence of malnutrition is not evenly distributed across the districts of the state (IIPS, 2017, 2021). Moreover, there are different studies done considering the role of bio-demographic factors in the prevalence of child malnutrition across the country (Kanjilal et al., 2010; Bisai et al., 2014; Panigrahi & Das, 2014; Amruth et al., 2015; Rengma et al., 2016; Ansuya et al., 2018; Roy et al., 2018; De & Chattopadhyay, 2019; Agarwal et al., 2021). In the present research work, Purulia, one of the poorest districts in terms of Gender Development Index (GDI) and HDI (Government of West Bengal, 2004), and Multidimensional Poverty Index (MPI) in West Bengal (National Institute for Transforming India [NITI] Aayog, 2021a), has been considered to study the prevalence of child malnutrition (Fig. 1). The proportion of rural populations in the district is 87.26%, which is quite high. The literacy rate of the district is 64.48%, whereas the female literacy rate is 50.52%. The majority of the working population (60.90%) is associated with agricultural activities (Government of West Bengal, 2014, 2015). Purulia has a long history of poverty and deprivation, and the majority of the people live a life of hand-to-mouth. The adverse geophysical conditions directly impact their socioeconomic status (Ghosh et al., 2021; Mandal & Ghosh, 2019; Mandal et al., 2017, 2018a; Roy & Jana, 2019). National and international organizations assess child malnutrition, mainly for under 5 years (UNICEF et al., 2016, 2018, 2019, 2020; IIPS, 2017, 2021). So, we can access the data and observe the status of this age group. But the condition of other age groups also needs to be discovered. There are several works conducted in the Purulia district to assess the nutritional level of children of a specific community or age group, and no such significant work was carried out on a large scale taking into account the bio-demographic and socio-economic perspectives of children and their households (Chowdhury et al., 2008; Dasgupta and Chattopadhyay 2008; Bose and Das, 2009; Chowdhury et al., 2010; De & Chattopadhyay, 2019; Mandal et al., 2017; Mandal & Ghosh, 2019; Ghosh et al., 2021; Mandal, 2021). It is already documented that Purulia is tangled with poverty for decades (Government of West Bengal, 2004; IIPS, 2017, 2021; NITI Aayog, 2021a), but the incidence of undernutrition is not studied well in the context of poverty in the district. The present study attempts to assess the incidence of child malnutrition of 5 to 10 years of the district in terms of bio-demographic and socio-economic perspectives. It will help out to document new data and information on child malnutrition and its possible responsible factors. This study also seeks to perceive the status of the first two goals of SDGs (1. End of poverty in all forms, and 2. Zero hunger). All the countries of the world are committed to achieving success in obtaining SDGs within the stipulated time frame, thus, monitoring and frequent assessment are required in this respect. The Government of India has consistently been trying to obtain SDGs (NITI Aayog, 2021b), but it is also important to know how far the SDGs are successful at the regional level. Based on the story of the success and impediment of SDGs in the context of Purulia, more suitable policies may be adopted to reduce the incidence of poverty and malnutrition in the district to achieve the 2030 Agenda.

Location map of the study area
2 Materials and methods
2.1 Purulia and its persistent nature of deprivation and undernutrition
The story of deprivation and misery of the people of Purulia can well be traced from the book entitled ‘A Statistical Account of Bengal’ long before the independence of India, written by W.W. Hunter and published in 1877. The poor peasants were deprived by the Zamindars, Mahajans, village rice-merchant, and money lenders. Thus, poverty was an integral part of their life (Hunter, 1877). During the British reign, the people of Purulia also experienced deprivation and not received the facility of basic needs (Bhattacharya, 1986). After the independence, the increasing rate of population growth and the constant pressure on agricultural lands, less chance of employability in other sectors, and low level of income keep the incidence of poverty almost constant. Ultimately the poor quality of life is experienced by the inhabitants, which is well reflected by the status of child malnutrition (Ghosh et al., 2021; Mandal, 2021; Mandal & Ghosh, 2019; Mandal et al., 2018a). Bagli and Tewari (2019) reveal that the incidence and extent of multidimensional poverty in the Purulia district are found to be much higher than the national average, whereas the breadth of poverty is seen as almost the same for the district in comparison with India. To date, Purulia is an agrarian society, and the majority of the people are associated with agricultural activities (Census of India, 2011). It is quite unfortunate that agriculture is still gambling on Monsoon in India (Ghosh et al., 2020a); and in the case of Purulia, poor soil quality, undulating hard rock terrain with a high degree of slope (Ghosh et al., 2020a, 2020b) and limited facility and access to irrigation (Government of West Bengal, 2015) impede the all-round the year agricultural production (Fig. 2). This situation clearly portrays the low-income status of the district, which ultimately impacts the livelihood pattern of people (Mandal, 2021; Mandal & Ghosh, 2019; Mandal et al., 2018a; Roy & Jana, 2019).

Land use and land cover map of Purulia
It is also reported by the NITI Aayog (2021a) that the Purulia district ranks first in MPI in the state of West Bengal. The report of NFHS-4 indicated the prevalence of stunting, wasting, and underweight was 45.50%, 34.60%, and 58.20%, respectively (IIPS, 2017). All these values, unfortunately, cross the critical value of public health significance of WHO, 1995 (WHO, 2010). The NFHS-4 report also indicated that around 47.50% of women in the district suffered from below-normal BMI. Pregnant and all women found to be anemic were 80.70% and 80%, respectively. Only 23.50% of mothers received full antenatal care in the district (IIPS, 2017). Only 3.60% of pregnant mothers took iron folic acid tablets for 180 days or more. The proportion of children, who were exclusively breastfed for six months after birth, was only 50.70%. It was revealed that 66.80% of children aged between 6 to 59 months were found to be anemic (IIPS, 2017). The distress condition of mothers and children is persistent and is related to place and its continuous journey through deprivation. A brief profile on malnutrition and socio-economic conditions of the district and the state of West Bengal is also presented in Table 1.
2.2 Data and anthropometric assessment
The study was carried out at 16 villages of Purulia district including 671 children aged 5 to 10 years from 504 households adopting a multi-stage sampling technique. Of the total sample size of children, the respective male and female children were 360 and 311. The study was conducted from January to April 2019. A pre-tested questionnaire was framed to collect data on socio-economic and bio-demographic parameters. Only the willing participants were included in the sample. Anthropometric techniques are the most widely popular and suitable instruments to determine the nutritional status of children (Government of India, 2013; UNICEF et al., 2016, 2018, 2019, 2020; Mandal & Ghosh, 2019; Ghosh et al., 2021). Measurements of height and weight and records of age were obtained for children and mothers to assess their nutritional status. In order to determine the type of undernutrition, stunting (Height-for-Age Z-Score/HAZ), wasting (Body Mass Index [BMI]-for-Age Z-Score/BAZ), and underweight (Weight-for-Age Z-Score/WAZ) were computed using ‘WHO Anthro-Plus Software’ following the ‘World Health Organization Child Growth Standards, 2006’ (de Onis et al., 2006; World Health Organization [WHO], 2010, 2018). Stunting is the short height of a child in terms of his/her age, and it negatively impacts physical and cognitive development. In contrast, wasting refers to the thinness of a child compared to his/her height. The risk of mortality is increased if the child is found to be moderately or severely wasted (UNICEF et al., 2020). When a child is unable to gain an expected weight at a particular age is called underweight. The risk of death gets increased for severely underweight children (Government of India, 2013). To compute overall undernutrition, a Composite Index of Anthropometric Failure (CIAF) is constructed, introduced by Peter Svedberg in 2000, for this study following the specified methodology (Nandy & Svedberg, 2012).
2.3 Multidimensional deprivation index
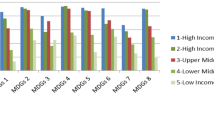
To reveal the socio-economic status of the studied households, the Multidimensional Deprivation Index (MDI) is computed based on the basic methodology of MPI of UNDP (UNDP, 2020b). To compute the MDI, a number of socio-economic variables are taken into consideration (Table 2). All the parameters are given the same weight to keep the result simpler. To compute the MDI, the following equations are adopted, where ‘H’ indicates headcount ratio, the proportion of households who are multidimensionally deprived; ‘q’ refers to the number of multidimensionally deprived households; ‘n’ depicts total sample households; ‘A’ is the intensity of multidimensional deprivation; ‘c’ denotes total deprivation of deprived households in respect to parameters; ‘d’ is the total adopted parameters.
2.4 Bio-demographic and socio-economic determinants of child malnutrition
The prevalence of malnutrition in children is closely associated with different bio-demographic and socio-economic factors. Specifically, the undernutrition scenario of children in underdeveloped and developing countries results from the vicious circle of poverty and disease (de Onis & Blossner, 1997; Mandal et al., 2017; Mandal & Ghosh, 2019; Ghosh et al., 2021). But in this globalized world of the twenty-first century, the incidence of undernutrition is experienced by a wide range of pockets across the globe (UNICEF et al., 2019). Several studies observed that the bio-demographic and socio-economic factors, such as BMI of mother, marriage age of mother, child birth weight, number of siblings, birth order, food intake, family income, education of parents, sanitation facility, source of drinking water, have a direct bearing in the prevalence of malnutrition of children (de Onis & Blossner, 1997; Cummins, 1998; Phillips, 2006; Kanjilal et al., 2010; Panigrahi & Das, 2014; Amruth et al., 2015; Rengma et al., 2016; Ansuya et al., 2018; De & Chattopadhyay, 2019; Islam & Biswas, 2020; Agarwal et al., 2021). In this present study, a total number of fifteen bio-demographic and socio-economic parameters are adopted as independent variables to find out the significant predictors of child malnutrition (Table 3). All these parameters are taken in view of the socio-economic and bio-demographic conditions of the district. The reports of NFHS & NITI Aayog (MPI) on socio-economic and bio-demographic conditions of Purulia clearly highlight the serious situation of the district, and most of the parameters of this study are taken from those reports to make the present study more fruitful. Testing these variables may bring out the association of different independent variables with child malnutrition.
3 Results
3.1 Prevalence of stunting (HAZ scenario)
The prevalence of stunting is observed to be 43.37% among the children at the district level, of which male and female children are 45.83% and 40.51%, respectively. The cut-off value of WHO, 1995, for public health significance indicates ‘very high prevalence (≥ 40%)’ of stunting among the children in the study area (WHO, 2010). Moderate stunting (26.23%) is more dominant than severe stunting (17.14%). Both the male (27.50%) and female (24.76%) children are more at risk of moderate stunting compared to severe stunting. The lowest incidence of stunting is noticed for the age group of 84 to 96 months (37.96%) followed by 60 to 72 months (41.67%) and 96 to 108 months (41.96%), while 72 to 84 and 108 to 120 months age groups experience stunting 46.83% and 50.96%, respectively (Table 4).
3.2 Prevalence of wasting (BAZ scenario)
The proportion of wasted children in the study area is 44.71%, of which male and female children are 43.33% and 46.30%, respectively. The share of wasted children is observed to be very high compared to the cut-off value for public health significance, i.e., ‘critical (≥ 15%)’ of WHO, 1995 (WHO, 2010). Severe wasting (18.33%) is less prevalent than moderate wasting (26.38%). Female children are more at risk of moderate wasting compared to severe wasting, while male children experience almost equally moderate and severe wasting. The proportion of wasted children is found to be lowest in 108 to 120 months (38.46%), and the remaining age groups endure wasting between 43 and 48% (Table 4).
3.3 Prevalence of underweight (WAZ scenario)
The underweight is more prevalent among the children of the study area compared to stunting and wasting. The total proportion of underweight children is 65.42%, of which male and female children are 65.55% and 65.27%, respectively. The prevalence of underweight children is found to be ‘very high prevalence (≥ 30%)’ as per the cut-off value of WHO, 1995 (WHO, 2010). Moderate underweight (35.17%) is more prevalent than severe underweight (30.25%) for both sexes. It is found that the prevalence of underweight is high among all age groups, and it ranges from 63 to 67% (Table 4).
3.4 Composite index of anthropometric failure
The overall undernutrition or CIAF of children is observed to be 73.77%. The proportion of male and female children is 74.72% and 72.67%, respectively. The category of wasting & underweight (22.80%); stunting & underweight (21.31%); and stunting, wasting & underweight (17.74%) mainly dominates the event of undernutrition among the children. The male children experience a high rate of stunting & underweight (23.33%) followed by wasting & underweight (21.39%); and stunting, wasting & underweight (17.78%). In the case of female children, the category of wasting & underweight (24.44%) is found to be more effective compared to stunting & underweight (18.97%); and stunting, wasting & underweight (17.68%). All the age groups experience a high rate of CIAF, which varies between 72 and 76% (Table 5).
4 Discussion
4.1 Prevalence of stunting and contemporary scenario
GHI (2020) reported that the global prevalence of under 5 children was 144 million (21.30%), while the national average of stunted children in India is 35.50% in 2019–21 (IIPS, 2021) and it was 38.40% in 2015–16 (IIPS, 2017). In the case of West Bengal, the figure is 33.80% in 2019–20 (IIPS, 2021). It is evident that the proportion of stunted children aged between 5 and 10 years in the Purulia district is higher (43.37%) than the global, national, and state averages. Moreover, it crosses the cut-off value of WHO, 1995 for public health significance (WHO, 2010). There are several studies conducted across India found different levels of stunting among several age groups of children, such as Arambag, West Bengal (2 to 6 years) 26.60% (Mandal et al., 2008); Paschim Medinipur, West Bengal (2 to 13 years) 49.60% (Bisai & Mallick, 2011); Paschim Medinipur, West Bengal (1 to 14 years) 26.10% (Bisai et al., 2008b); Bhubaneswar, Orissa (3 to 9 years) 57.40% (Panigrahi & Das, 2014); Bijapur, Karnataka (6 to 12 years) 25% (Shashank & Chethan, 2016); Sullia, Karnataka (5 to 11 years) 19.22% (Amruth et al., 2015); Odisha (1 to 6 years) 32.40% (Goswami, 2016). Several factors in reality influence the variation in the prevalence of stunting among children, namely: biological determinants, socio-economic and demographic characteristics of households, ethnic and cultural diversity, healthcare facilities, etc., (Alemayehu et al., 2015; Amruth et al., 2015; Bisai et al., 2008b, 2012; Islam & Biswas, 2020; Kanjilal et al., 2010; Panigrahi & Das, 2014; Rengma et al., 2016; Singh, 2020). Our study does not observe any statistically significant role of sex and age of children in the prevalence of stunting at the district level. The persistent nature of poverty (Government of West Bengal, 2004; IIPS, 2017; UNDP, 2020b; NITI Aayog, 2021a) and unemployment in the district is well imitated by the incidence of child undernutrition (Ghosh et al., 2021; Mandal, 2021; Mandal & Ghosh, 2019; Mandal et al., 2017, 2018a). Stunting among children is mainly the outcome of insufficient food intake, inappropriate food practices, frequent infections, and poverty (Government of India, 2013; Mandal et al., 2017; UNICEF et al., 2019). To overcome such a situation, much stress is required to encourage in a balanced diet and proper medical care (Mandal & Ghosh, 2019; UNICEF et al., 2019; Ghosh et al., 2021; Mandal, 2021).
4.2 Prevalence of wasting and contemporary scenario
There were 47 million (6.90%) under 5 wasted children in 2019 in the world (UNICEF et al., 2019), whereas the national average of India is 19.30% in 2019–21 (IIPS, 2021), which was 21% in 2015–16 (IIPS, 2017). The under 5 wasted children in West Bengal is 20.30% in 2019–20 (IIPS, 2021). This study records higher wasted children (44.17%) than the global, national, and state averages. Even the figure of wasted children exceeds the cut-off value of ‘critical (≥ 15%)’ for public health significance of WHO, 1995 (WHO, 2010). The prevalence of wasted children is observed in several works in different proportions across India, such as Arambag, West Bengal (2 to 6 years) 50% (Mandal et al., 2008); Paschim Medinipur, West Bengal (2 to 13 years) 22.70% (Bisai & Mallick, 2011); Paschim Medinipur, West Bengal (1 to 14 years) 19.40% (Bisai et al., 2008b); Darjeeling, West Bengal (5 to 12 years) 26.50% (Debnath et al., 2018); Odisha (1 to 6 years) 25% (Goswami, 2016); Assam (5 to 12 years) 17.15% (Mondal et al., 2016); Bhubaneswar, Orissa (3 to 9 years) 23.29% (Panigrahi & Das, 2014); Sullia, Karnataka (5 to 11 years) 26.50% (Amruth et al., 2015). It was documented in different studies that the variation in the prevalence of wasting mainly results from socio-economic-backgrounds and growth patterns of different age groups of children (Alemayehu et al., 2015; Amruth et al., 2015; Bisai et al., 2008a, 2008b; Das & Bose, 2009; Debnath et al., 2018; Islam & Biswas, 2020; Kanjilal et al., 2010; Panigrahi & Das, 2014; Rengma et al., 2016; Singh, 2020; Stiller et al., 2020). The study does not observe any statistically significant difference in sex and age groups of children in the prevalence of wasting; it may be due to the low socio-economic profile of the households (Ghosh et al., 2021; Mandal, 2021; Mandal & Ghosh, 2019; Mandal et al., 2017). The high incidence level of wasting is primarily associated with inadequate food intake, incorrect feeding practices, repeated infections, and diseases. Early interventions, in this case, may check the severity of wasting (Government of India, 2013; WHO, 2018).
4.3 Prevalence of underweight and contemporary scenario
The global estimation of underweight children was 113.40 million in 2015, which was 17.60% of total children aged below 5 years (de Onis et al., 2004). India records under 5 underweight children in 2019–21 as 32.10% (IIPS, 2021), while it was 35.80% in 2015–16 (IIPS, 2017). In 2019–20, the figure was 32.20% for West Bengal (IIPS, 2021). On the contrary, the share of underweight children in this district (65.42%) is not only high compared to the global, national, and state averages, rather it is almost double. The prevalence of underweight children even breaches the critical value of WHO, 1995 (WHO, 2010). Much literature on malnutrition documented that the proportion of undernourished children was found in Arambag, West Bengal (2 to 6 years) 63.30% (Mandal et al., 2008); Bhubaneswar, Orissa (3 to 9 years) 45.40% (Panigrahi & Das, 2014); Bijapur, Karnataka (6 to 12 years) 34.15% (Shashank & Chethan, 2016); Sullia, Karnataka (5 to 11 years) 26.50% (Amruth et al., 2015); Paschim Medinipur, West Bengal (2 to 13 years) 52.90% (Bisai & Mallick, 2011); Paschim Medinipur, West Bengal (1 to 14 years) 33.90% (Bisai et al., 2008b); Odisha (1 to 6 years) 42.60% (Goswami, 2016). It is often seen that factors like space and time, socio-economic, age groups, food habits, etc., determine the variations in the occurrence of child underweight (Bisai et al., 2008b; Das & Bose, 2009; Gupta et al., 2015; Nandy et al., 2005; Rengmaet al., 2016). In several cases, acute or chronic malnutrition results in underweight children, and the risk of mortality may be enhanced if a child is mildly underweight. This chance of mortality gets accelerated for severely underweight children (Government of India, 2013; WHO, 2018).
4.4 Prevalence of CIAF and contemporary scenario
Several studies mentioned that undernutrition is mainly the product of poverty and deprivation and is well reflected in child malnutrition (Ghosh et al., 2021; Government of India, 2013; Mandal & Ghosh, 2019; Mandal et al., 2017; Nandy et al., 2005). It is estimated that the proportion of undernourished children in India is 14% (Global Hunger Index, 2020), but few studies reported that 50% of children in West Bengal were undernourished (Biswas et al., 2018; Bose et al., 2008). Globally, 690 million (8.90%) people were undernourished in 2019, which was 10 million higher than in 2018 (Global Hunger Index, 2020). Our study finds the prevalence rate of undernourished children in Purulia based on CIAF is more than the global and national averages. Several studies carried out across India documented the proportion of undernourished children in different magnitudes. The risk of child morbidity and mortality is high among undernourished children (Nandy et al., 2005; Rice et al., 2000; Schroeder & Brown, 1994) than the well-off children (Tomkins & Watson, 1989; Pelletier et al., 1995; Latham, 1997; WHO, 1997; Cunha, 2000; Gillespie & Haddad, 2003; Nandy et al., 2005). The high prevalence of undernourished children is the result of poor socio-economic conditions, which in turn are responsible for diseases and further undernutrition (WHO, 1997; Wagstaff & Watanabe, 2000; Nandy et al., 2005). It is worth mentioning that there is no role of age and sex in the prevalence of CIAF or undernutrition of children in the study area. This situation emerges due to the low level of the socio-economic background of the district resulting from unfavorable geophysical settings, which impede agricultural activities, and ultimately extend the path of unemployment and misery (Bhattacharya, 1986; Ghosh et al., 2021; Mandal, 2021; Mandal & Ghosh, 2019; Mandal et al., 2017, 2018b).
4.5 Association of significant independent parameters in the prevalence of undernourishment
To determine the impact of bio-demographic and socio-economic variables on the nutritional status of children, multiple regression analysis is undertaken using IBM SPSS Statistics 26 software (Table 6). Results reveal that the education of father is the most statistically significant predictor (p< 0.000) of stunting in model 1 followed by family income (p< 0.002) in model 2. Several past studies found the education of father a significant predictor of child malnutrition (Kamiya, 2011; Meshram et al., 2012b; Alemayehu et al., 2015), while family income also plays a vital role to combat poverty and malnutrition (Kanjilal et al., 2010; Meshram et al., 2012b; Agu et al., 2019; Ahmad et al., 2020). In the case of child wasting, the BMI of mother is the most significant parameter (p< 0.001) of child malnutrition in model 1. Many research works documented the BMI of mother is an important reflector of child undernourishment (Cesare et al., 2015; Kang & Kim, 2019; Rahman et al., 2019). The incidence of underweight is also observed to be associated with the BMI of mother (p< 0.000) and the education of father (p< 0.002). Both the predictors have a direct bearing on underweight children (Nahar et al., 2010; Biswas & Bose, 2011; Meshram et al., 2012b; Cesare et al., 2015; Agu et al., 2019; Farooq et al., 2020). There are two important predictors observed to be statistically significant in models 1 and 2 for CIAF of children as it is highly determined by the BMI of mother (p< 0.000), which is well recorded by earlier research works (Ansuya et al., 2018; Wong et al., 2014). Education of father also plays a statistically significant (p< 0.002) role in the prevalence of CIAF among children. The relevance of paternal education is seen as statistically significant in the works of Ansuya et al. (2018) in rural Karnataka, Sabu et al., (2020) in Kerala, and Khanra et al. (2020) in Purba Medinipur, India. Thus, more importance must be given to bio-demographic and socio-economic parameters to reduce the prevalence of child undernutrition.
5 Computation of multidimensional deprivation index of households
The MDI is an important instrument to assess the different forms of deprivation at an individual level as it employs microdata obtained from household surveys (UNDP, 2018). This study attempts here to compute the MDI of the studied households of the district. It is found that 92% of households are multidimensionally deprived based on the selected socio-economic indicators. In the case of India, the calculated MPI in 2018 value was 27% (UNDP, 2018), while it was 27.90% in 2020 (UNDP, 2020b). The differences in results between the present study and others are due to selected parameters and their outcomes. The reports of HDR (Government of West Bengal, 2004) and NFHS-4 (IIPS, 2017) have already mentioned the very poor socio-economic status of the district Purulia in West Bengal. In contrast, the value of the intensity of multidimensionally deprivation of deprived households of the district is found to be 0.68. The intensity of deprivation in India in 2020 was around 0.44 (UNDP, 2020b). The estimated value of MDI of Purulia district is calculated to be 0.62, i.e., deprived conditions of households (Table 7), while the multidimensional poverty index of the district is computed as 0.21 by Bagli and Tewari (2019). The national average of multidimensional poverty index of India was 0.123 in 2020 (UNDP, 2020b). It is worth mentioning here Purulia, undoubtedly, is one of the deprived districts in India depending upon the findings of the present study and different other studies. It is to be noted that there is a close relation between MDI of households and the proportion of undernourished children.
6 Achievements and impediments of SDGs
6.1 Global level
The main aim of SDGs is to bring sustainable development in the economy, society, and environment. The 17 global goals with 169 targets of UN build on MDGs focus on completing the unfinished works of MDGs by 2030 (UN, 2020). Smith (2020) mentions the crucial role of SDGs in achieving global equality and their implementation achieved significant success in eradicating poverty and hunger. The global number of people living in extreme poverty came down to 10% in 2015 from 16% in 2010 (UN, 2019). In 2019, the global poverty estimation was 8.20%, and 6% of the world’s population will be living in extreme poverty in 2030 (UN, 2020). The incidence of poverty is high among low-income countries and around 736 million people in the world lived on less than $1.90 a day in 2015. In rural areas, the poverty was 17.20% and there lived about 79% of poor people in the world. Surprisingly, 46% extremely poor were children aged less than 14 years (UN, 2019). Undernourishment and food security remain global challenges. In 2014, around 630 million people were found to be undernourished, which rose to about 690 million in 2019. Estimation indicated moderate or severe food insecurity was experienced by 2 billion people (25.90%) in 2019, which was 22.40% in 2014. Eradicating hunger does not ensure that everyone has the access to sufficient nutritious food. Prior to the coronavirus outbreak, the progress rate in achieving SDGs started to slow down due to economic fallout, violent conflicts, climate change, socio-economic and political complexities in different areas (UN, 2020). The incidence of poverty and hunger may be tackled by the government adopting policies and social protection schemes (UN, 2019).
6.2 National and state level
In India, NITI Aayog, a nodal body overseeing the progress of SDGs, in partnership with UN and other stakeholders of the society strives to achieve the global goals of 2030. The SDG India Index 3.0, based on the SDGs goals and targets, is constructed by adopting 115 indicators (directly from the national indicator framework) to cover 70 targets of 16 SDGs. A composite score, ranging from 0 to 100 (0 to 49- aspirant; 50 to 64- performer; 65 to 99- front runner; 100- achiever), explains the overall performance in achieving targets of different SDGs by states and union territories. India itself scores 66 (front runner), while West Bengal ranks 18th (score- 62, performer) out of 28 states of India in 2020–21. Performance in the case of individual goal, West Bengal scores 59 (performer) in SDG-1 and 46 (aspirant) in SDG-2 and ranks 20th and 18th, respectively, among the states (NITI Aayog, 2021b). If we try to understand the performance of West Bengal in terms of selected indicators of SDGs 1 and 2, it shows around 20% of the population of the state lives below the national poverty line, the headcount ratio as per MPI is 26.30% (NITI Aayog, 2021b), and only 29.30% households with any usual member are covered under any health insurance. In contrast, the proportion of under 5 underweight and stunted children is 32.20% and 33.80%, respectively, while anemic pregnant women aged 15 to 49 years are 62.30% (IIPS, 2021). Moreover, 45.50% of adolescents (10 to 19 years) are also found anemic (NITI Aayog, 2021b). Unfortunately, any of these indicators do not meet their targets by 2020.
6.3 Regional level: Purulia
Though the SDG India Index 3.0 is not available at the district level, the situation remains unchanged for Purulia district. In order to assess the success rate of SDG-1 for Purulia, three indicators are mentioned here. The proportion of people who are multidimensionally poor in the district is 49.69% (headcount ratio) with MPI value of 0.236 (global SDG target- 1.2), and Purulia records itself as the poorest district in the state (NITI Aayog, 2021a). The national target in this regard is to bring down the value to 13.95%, but the goal is far away. Households with any usual member covered under any health insurance are only 35.60% (global SDG target- 1.3) in the district (IIPS, 2021). It is targeted as to attain the global SDG target- 1.4 that no household should live in a katcha (non-concrete) house. The national and state averages in this regard are 4.20% and 6%, respectively (NITI Aayog, 2021b), while 70.83% of people live in katcha houses in the district (Mandal, 2021), and it was also documented by Bagli and Tiwari (2019) around the same proportion. In contrast, the performance of Purulia in SDG-2 is not found satisfactory. The proportion of under 5 underweight and stunted children in the district was 46.30% and 36.90%, respectively (IIPS, 2021), while the national target has been set to reduce the share of underweight and stunted to 1.90% and 6%, respectively (NITI Aayog, 2021b). The anemic pregnant women aged 15–49 years were recorded at 72.20% (IIPS, 2021), where the national target is 25.20% (NITI Aayog, 2021b).
7 Conclusion
It is to be noted that the per capita monthly average income of the studied households is ₹1455, which is just above the estimated poverty line (₹1118.12) for rural West Bengal for the year 2018–19 (Mandal, 2021). The end of extreme poverty (SDG-1), the value measured for those people living a day on less than $1.25 (Leal Filho et al., 2019; UN, 2019), is quite hard to achieve for the district. This proportion of average earnings cannot assure a good livelihood for an individual. Moreover, the majority of the people are associated with low-profile economic activities in unorganized sectors, like daily wage occupations in agricultural and non-agricultural sectors, and disguised unemployment is also another serious issue in the district. The majority of the households still use smoking fuel for cooking, go for open defecation, and live in katcha houses. The education level of parents is not up to the mark, and food they take is not well balanced in terms of required amount of calorie. In a nutshell, it may be said that the poor nutritional status mainly of children is highly associated with poor socio-economic characteristics of households, and BMI of mother are education of father are the two most statistically significant predictors of child malnutrition. Thus, the success rate of SDG-1 & 2 is not so profound and not reflected through the livelihood pattern of households. More emphasis needs to be given at local level to enhance the purchasing capacity of poor to enjoy a decent life. In order to overcome this situation, employment generation both for skilled and unskilled labourer must be given highest priority. Locally available potential employment generating resources, such as sericulture, shellac, handicraft, tourism based on geo-morphosites need to encouraged and supported. Rainwater harvesting in large scale will definitely reduce the water scarcity of the district during the lean season, and such water may be used in domestic and agriculture purposes. Policies like these framed on ground reality may be proved more effective for Purulia district in a long run.
Data availability
Available on request.
References
Aayog, N. I. T. I. (2021a). National Multidimensional Poverty Index: Baseline Report Based on NFHS-4 (2015–16). Government of India.
Aayog, N. I. T. I. (2021b). SDG India Index & Dashboard 2020–21. Government of India.
Abbott, K. W., & Bernstein, S. (2015). The high-level political forum on sustainable development: Orchestration by default and design (SSRN scholarly paper ID 2443973). Social Science Research Network. https://papers.ssrn.com/abstract=2443973
Agarwal, A. K., Sarswat, S., Mahore, R., Saraswat, S., Kuity, P., & Tripathi, A. (2021). Malnutrition prevailing trend study among under five children of urban slum area of Gwalior city Madhya Pradesh. International Journal of Community Medicine and Public Health, 8(2), 623.
Agu, N., Emechebe, N., Yusuf, K., Falope, O., & Kirby, R. S. (2019). Predictors of early childhood undernutrition in Nigeria: The role of maternal autonomy. Public Health Nutrition, 22(12), 2279–2289. https://doi.org/10.1017/S1368980019000818
Ahmad, D., Afzal, M., & Imtiaz, A. (2020). Effect of socioeconomic factors on malnutrition among children in Pakistan. Future Business Journal, 6(1), 30. https://doi.org/10.1186/s43093-020-00032-x
Alemayehu, M., Tinsae, F., Haileslassie, K., Seid, O., Gebregziabher, G., & Yebyo, H. (2015). Undernutrition status and associated factors in under-5 children, in Tigray Northern Ethiopia. Nutrition, 31(7–8), 964–970. https://doi.org/10.1016/j.nut.2015.01.013
Amruth, M., Kumar, S., Kulkarni, A., Kamble, S., & Ismail, I. (2015). A study on nutritional status and morbidity pattern among primary school children in Sullia town, South India. Indian Journal of Basic and Applied Medical Research, 4(4), 100–112.
Ansuya, B. S., Nayak, B. U., George, A., Shashidhara, Y. N., Mundkur, S. C., & Guddattu, V. (2018). Risk factors for malnutrition among preschool children in rural Karnataka: A case-control study. BMC Public Health. https://doi.org/10.1186/s12889-018-5124-3
Bagli, S., & Tewari, G. (2019). Multidimensional poverty: An exploratory study in Purulia district West Bengal. Economic Affairs. https://doi.org/10.30954/0424-2513.3.2019.7
Bhattacharya, T. (1986). Purulia. Pharma K L M Private Limited.
Binagwaho, A., Agbonyitor, M., Rukundo, A., Ratnayake, N., Ngabo, F., Kayumba, J., Dowdle, B., Chopyak, E., & Smith Fawzi, M. C. (2011). Underdiagnosis of malnutrition in infants and young children in Rwanda: Implications for attainment of the millennium development goal to end poverty and hunger. International Journal for Equity in Health, 10(1), 61. https://doi.org/10.1186/1475-9276-10-61
Bisai, S. (2014). Prevalence of undernutrition among Santal tribal preschool children of Paschim Medinipur district, West Bengal India. International Journal of Pediatrics.
Bisai, S., Bose, K., & Ghosh, A. (2008a). Nutritional status of Lodha children in a village of Paschim Medinipur district, West Bengal. Indian Journal of Public Health, 52(4), 203–206.
Bisai, S., Bose, K., & Ghosh, A. (2008b). Prevalence of undernutrition of Lodha children aged 1–14 years of Paschim Medinipur district, West Bengal, India. Iranian Journal of Pediatrics, 18, 323–329.
Bisai, S., Bose, K., Ghosh, T., De, G. K., Khongsdier, R., Koziel, S., Mahalanabis, D., & Mallick, P. (2012). Nutritional status based on anthropometry of tribal preschool children in Paschim Medinipur district of West Bengal, India. International Journal of Innovative Research and Development, 1, 61–79.
Bisai, S., & Mallick, C. (2011). Prevalence of undernutrition among Kora-Mudi children aged 2–13 years in Paschim Medinipur district, West Bengal. India. World Journal of Pediatrics, 7(1), 31–36. https://doi.org/10.1007/s12519-010-0239-3
Biswas, S., Giri, S. P., & Bose, K. (2018). Assessment of nutritional status by composite index of anthropometric failure (CIAF): A study among preschool children of Sagar Block, South 24 Parganas district, West Bengal. India. Anthropological Review, 81(3), 269–277. https://doi.org/10.2478/anre-2018-0022
Blanc, D. le. (2015). Towards integration at last? The sustainable development goals as a network of targets (DESA working paper no. 141). Department of Economic & Social Affairs. https://www.un.org/esa/desa/papers/2015/wp141_2015.pdf
Biswas, S., & Bose, K. (2011). Effect of number of rooms and sibs on nutritional status among rural Bengalee preschool children from eastern India. Collegium Antropologicum, 35(4), 1017–1022.
Bose, K., & Bisai, S. (2008). Prevalence of undernutrition among rural adolescents of West Bengal. India. Journal of Tropical Pediatrics, 54(6), 422–423. https://doi.org/10.1093/tropej/fmn044
Bose, K., Bisai, S., Chakraborty, J., Datta, N., & Banerjee, P. (2008). Extreme levels of underweight and stunting among pre-adolescent children of low socioeconomic class from Madhyamgram and Barasat, West Bengal India. Collegium Antropologicum, 32(1), 73–77.
Census of India. (2011). C.D. Block wise primary census abstract data (PCA)—West Bengal. Ministry of Home Affairs, Government of India.
Cesare, M. D., Bhatti, Z., Soofi, S. B., Fortunato, L., Ezzati, M., & Bhutta, Z. A. (2015). Geographical and socioeconomic inequalities in women and children’s nutritional status in Pakistan in 2011: An analysis of data from a nationally representative survey. The Lancet Global Health, 3(4), e229–e239. https://doi.org/10.1016/S2214-109X(15)70001-X
Chowdhury, S. D., Brian, H. W., & Ghosh, T.(2010) Nutritional and socioeconomic factors in motor development of Santal children of the Purulia district India. Early Human Development 86(12) 779–784 S0378378210002446. https://doi.org/10.1016/j.earlhumdev.2010.08.029
Cummins, R. A. (1998). Quality of life definition and terminology: A discussion document from the international society for quality of life studies. International Society for Quality-of-Life Studies.
Cunha, A. L. (2000). Relationship between acute respiratory infection and malnutrition in children under 5 years of age. Acta Paediatrica, 89(5), 608–609. https://doi.org/10.1111/j.1651-2227.2000.tb00347.x
Das, S., & Bose, K. (2009). Undernutrition among Bauri pre-school children of Nituria block, Purulia district, West Bengal, India. Journal of Life Sciences, 1(2), 85–89. https://doi.org/10.1080/09751270.2009.11885137
Dasgupta, T., & Chattopadhyay, R. N. (2008). Poverty portrayal in the context of rural bengal: A case-study of Purulia District of West Bengal’. Studies of Tribes and Tribals, 6(1), 1–11. https://doi.org/10.1080/0972639X.2008.11886569
de Onis, M., Blössner, M., Borghi, E., Frongillo, E. A., & Morris, R. (2004) Estimates of Global Prevalence of Childhood Underweight in 1990 and 2015. JAMA 291(21) 2600–2606. https://doi.org/10.1001/jama.291.21.2600
de Onis, M., Onyango, A. W., Borghi, E., Garza, C., & Yang, H. (2006). Comparison of the world health organization (WHO) child growth standards and the national center for health statistics/WHO international growth reference: Implications for child health programmes. Public Health Nutrition, 9(7), 942–947. https://doi.org/10.1017/PHN20062005
De, P., & Chattopadhyay, N. (2019). Effects of malnutrition on child development: Evidence from a backward district of India. Clinical Epidemiology and Global Health, 7(3), 439–445. https://doi.org/10.1016/j.cegh.2019.01.014
Debnath, S., Mondal, N., & Sen, J. (2018). Socio-economic and demographic correlates of stunting and thinness among rural school-going children Aged 5–12 Years of North Bengal Eastern, India. Journal of Life Sciences. https://doi.org/10.31901/24566306.2018/10.01.207
Dutta Chowdhury, S., Chakraborty, T., & Ghosh, T. (2008). Prevalence of Undernutrition in Santal Children of Puruliya District, West Bengal. Indian Pediatrics, 45(1), 43–46.
Farooq, R., Khan, H., Khan, M. A., & Aslam, M. (2020). Socioeconomic and demographic factors determining the underweight prevalence among children under-five in Punjab. BMC Public Health, 20(1), 1817. https://doi.org/10.1186/s12889-020-09675-5
Ghosh, D., Mandal, M., Banerjee, M., & Karmakar, M. (2020a). Impact of hydro-geological environment on availability of groundwater using analytical hierarchy process (AHP) and geospatial techniques: A study from the upper Kangsabati river basin. Groundwater for Sustainable Development, 11, 100419.
Ghosh, D., Mandal, M., Karmakar, M., Banerjee, M., & Mandal, D. (2020b). Application of geospatial technology for delineating groundwater potential zones in the Gandheswari watershed. West Bengal. Sustainable Water Resources Management, 6(1), 14. https://doi.org/10.1007/s40899-020-00372-0
Ghosh, D., Mandal, M., Karmakar, M., Mandal, D., Modak, P., Ghosh, B., Mandi, S., & Haque, Sk. (2021). The prevalence of undernutrition among the Santal children and quality of life of their households: A study from hilly region of West Bengal. Spatial Information Research. https://doi.org/10.1007/s41324-021-00391-9
Gillespie, S., & Haddad, L. (2003). The double burden of malnutrition in Asia: Causes, consequences, and solutions (FIRST). SAGE Publications Pvt.
Global Hunger Index (2020). 2020 synopsis global hunger index: One decade to zero hunger linking health and sustainable food systems. Deutsche Welthungerhilfe; Concern Worldwide. https://reliefweb.int/sites/reliefweb.int/files/resources/synopsis.pdf
Goswami, M. (2016). Prevalence of under-nutrition measured by composite index of anthropometric failure (CIAF) among the Bhumij children of Northern Odisha, India. Journal of Nepal Paediatric Society, 36(1), 61–67. https://doi.org/10.3126/jnps.v36i1.14390
Government of West Bengal (India) (Ed.) (2004). West Bengal human development report, 2004. Development and Planning Department, Government of West Bengal.
Government of India (2013). Participant Manual for Facility Based Care for Severe Acute Malnutrition. Ministry of Health and Family Welfare Government of India.
Government of West Bengal (2014). District statistical handbook Purulia 2014. Department of Planning & Statistics.
Government of West Bengal (2015). Statistical abstract of West Bengal 2015. Bureau of Applied Economics and Statistics, Government of West Bengal.
Gupta, V., Mohapatra, D., & Kumar, V. (2015). Nutritional assessment among children (Under five years of age) using various anthropometric indices in an urban area of district Rohtak, Haryana. India. International Journal of Biomedical Research, 6(9), 629. https://doi.org/10.7439/ijbr.v6i9.2424
Hunter, W. W. (1877). A statistical account of Bengal (Vol. 17). Tubner & Co.
International Institute for Population Sciences (IIPS) (2017). National family health survey (NFHS-4), 2015–16 India. International Institute for Population Sciences.
Islam, Md. S., & Biswas, T. (2020). Prevalence and correlates of the composite index of anthropometric failure among children under 5 years old in Bangladesh. Maternal & Child Nutrition. https://doi.org/10.1111/mcn.12930
Kamiya, Y. (2011). Socioeconomic determinants of nutritional status of children in Lao PDR: Effects of household and community factors. Journal of Health, Population, and Nutrition, 29(4), 339–348. https://doi.org/10.3329/jhpn.v29i4.8449
Kang, Y., & Kim, J. (2019). Risk factors for undernutrition among children 0–59 months of age in Myanmar. Maternal & Child Nutrition. https://doi.org/10.1111/mcn.12821
Kanjilal, B., Mazumdar, P., Mukherjee, M., & Rahman, M. H. (2010). Nutritional status of children in India: Household socio-economic condition as the contextual determinant. International Journal for Equity in Health, 9(1), 19. https://doi.org/10.1186/1475-9276-9-19
Khanra, P., Bose, K., & Chakraborty, R. (2020). Mother’s education level is associated with anthropometric failure among 3 to 12 year old rural children in Purba Medinipur, West Bengal, India. Journal of Biosocial Science. https://doi.org/10.1017/S0021932020000577
Latham, M. C. (1997). Human nutrition in the developing world. Food and Agriculture Organization of the United Nations.
Leal Filho, W., Tripathi, S. K., Andrade Guerra, J. B. S. O. D., Giné-Garriga, R., OrlovicLovren, V., & Willats, J. (2019). Using the sustainable development goals towards a better understanding of sustainability challenges. International Journal of Sustainable Development & World Ecology, 26(2), 179–190. https://doi.org/10.1080/13504509.2018.1505674
Mandal, M., Karmakar, M., Modak, P., & Ghosh, D. (2017). Nutrition and child health: Peeping at the hilly tract of Jangalmahal area of Purulia district. In Food Security & Urbanization Equilibrium: A Sustainable Man-system Approach (1st ed.). Ashadeep
Mandal, M. (2021). A Geographical analysis of child malnutrition in Purulia district, West Bengal, (Unpublished PhD Thesis). University of Calcutta, India.
Mandal, G. C., Bose, K., Bisai, S., & Ganguli, S. (2008). Undernutrition among integrated child development services (ICDS) scheme children aged 2–6 years of Arambag, Hooghly district, West Bengal, India: A serious public health problem. Italian Journal of Public Health. https://doi.org/10.2427/5852
Mandal, M., & Ghosh, D. (2019). Undernutrition level among the children under 5 years age in Arsha community development block of Purulia district, West Bengal. Indian Journal of Landscape Systems and Ecological Studies, 42(2), 49–63.
Mandal, M., Modak, P., Karmakar, M., & Ghosh, D. (2018a). Tribal people of Purulia and their quality of life. Eastern Geographer, 24(1), 126–135.
Mandal, M., Modak, P., Karmakar, M., Mandal, D., Mandi, S., & Ghosh, D. (2018b). Educational attainment of tribal people: A case study in Ajodhya gram panchayat of Baghmundi C.D. Block in Purulia district. ILEE, 42(2), 105–111.
Manyike, P. C., Chinawa, J. M., Ubesie, A., Obu, H. A., Odetunde, O. I., & Chinawa, A. T. (2014). Prevalence of malnutrition among pre-school children in South-East Nigeria. Italian Journal of Pediatrics, 40(1), 75. https://doi.org/10.1186/s13052-014-0075-5
Mondal, N., Ronchehon, R., &Bharali, N. (2016). Prevalence of thinness, overweight and obesity among Karbi tribal children aged 5–12 years of Karbi Anglong, Assam northeast India. In Human Growth and Nutrition: A Biocultural Synthesis (1st ed.). Kalpaz.
Meshram, I. I., Arlappa, N., Balakrishna, N. Rao, K. M., Laxmaiah, A., &Brahmam, G. N. V. (2012b). Trends in the prevalence of undernutrition, nutrient and food intake and predictors of undernutrition among under five year tribal children in India. Asia Pacific Journal of Clinical Nutrition, 21(4), 568–576.
Nahar, B., Ahmed, T., Brown, K. H., & Hossain, M. I. (2010). Risk factors associated with severe underweight among young children reporting to a diarrhoea treatment facility in Bangladesh. Journal of Health, Population and Nutrition, 28(5), 476–483. https://doi.org/10.3329/jhpn.v28i5.6156
Nandy, S., Irving, M., Gordon, D., Subramanian, S. V., & Smith, G. D. (2005). Poverty, child undernutrition and morbidity: New evidence from India. Bulletin of the World Health Organization, 83(3), 210–216.
Nandy, S., & Svedberg, P. (2012). The composite index of anthropometric failure (CIAF): An alternative indicator for malnutrition in young children. In V. R. Preedy (Ed.), Handbook of Anthropometry (pp. 127–137). Springer.
World Health Organization (1997). Nutrition and poverty (Discussion paper nutrition policy paper #16). United Nations Administrative Committee on Coordination (ACC), Sub-Committee on Nutrition (SCN).
de Onis, M., & Blössner, M. (1997). WHO global database on child growth and malnutrition. https://apps.who.int/iris/handle/10665/63750
Panigrahi, A., & Das, S. C. (2014). Undernutrition and its correlates among children of 3–9 years of age residing in slum areas of Bhubaneswar, India. The Scientific World Journal, 2014, 1–9. https://doi.org/10.1155/2014/719673
Pelletier, D. L., Frongillo, E. A., Schroeder, D. G., & Habicht, J. P. (1995). The effects of malnutrition on child mortality in developing countries. Bulletin of the World Health Organization, 73(4), 443–448.
Phillips, D. (2006). Quality of life: Concept, policy and practice. Routledge.
Pomati, M., & Nandy, S. (2019). Assessing progress towards SDG2: Trends and patterns of multiple malnutrition in young children under 5 in West and Central Africa. Child Indicators Research, 13(5), 1847–1873. https://doi.org/10.1007/s12187-019-09671-1
Rahaman, S. N., Das, S., Dash, S. K., Giri, B., & Ali, K. M. (2019). Nutritional status of primary school children in different parts of India: A review. International Journal of Current Research and Review, 11(07), 01–04.
Rengma, M., Bose, K., & Mondal, N. (2016). Socio-economic and demographic correlates of stunting among adolescents of Assam North- East India. Anthropological Review, 79(4), 409–425. https://doi.org/10.1515/anre-2016-0030
Rice, A. L., Sacco, L., Hyder, A., & Black, R. E. (2000). Malnutrition as an underlying cause of childhood deaths associated with infectious diseases in developing countries. Bulletin of the World Health Organization, 78(10), 1207–1221.
Roy, K., Dasgupta, A., Roychoudhury, N., Bandyopadhyay, L., Mandal, S., & Paul, B. (2018). Assessment of under nutrition with composite index of anthropometric failure (CIAF) among under-five children in a rural area of West Bengal, India. International Journal of Contemporary Pediatrics, 5(4), 1651–1656. https://doi.org/10.18203/2349-3291.ijcp20182583
Roy, S. S., & Jana, N. C. (2019). Agricultural productivity and efficiency in Purulia district, West Bengal. International Journal of Reviews and Research in Social Sciences, 7(2), 179–190. https://doi.org/10.5958/2454-2687.2019.00016.9
Sabu, K., Ravindran, T. S., & Srinivas, P. (2020). Factors associated with inequality in composite index of anthropometric failure between the Paniya and Kurichiya tribal communities in Wayanad district of Kerala. Indian Journal of Public Health, 64(3), 258. https://doi.org/10.4103/ijph.IJPH_340_19
Schroeder, D. G., & Brown, K. H. (1994). Nutritional status as a predictor of child survival: Summarizing the association and quantifying its global impact. Bulletin of the World Health Organization, 72(4), 569–579.
Shashank, K. J., & Chethan, T. K. (2016). Nutritional status of school going children between the age group of 6–12 yrs in rural area of Bijpaur district. National Journal of Community Medicine, 7(5), 409–412.
Singh, A. (2020). Childhood malnutrition in india. IntechOpen. https://doi.org/10.5772/intechopen.89701
Smith, M. J. (2020). Sustainable development goals: Genuine global change requires genuine measures of efficacy. Journal of Maps. https://doi.org/10.1080/17445647.2020.1749386
Stiller, C. K., Golembiewski, S. K. E., Golembiewski, M., Mondal, S., Biesalski, H.-K., & Scherbaum, V. (2020). Prevalence of undernutrition and anemia among Santal Adivasi children, Birbhum district, West Bengal, India. International Journal of Environmental Research and Public Health, 17(1), 342. https://doi.org/10.3390/ijerph17010342
International Institute for Population Sciences (IIPS) (2021). National Family Health Survey 2019–20 (NFHS-5) India. International Institute for Population Sciences.
Tomkins, A., & Watson, F. (1989). Malnutrition and infection−A review (Nutrition policy discussion paper no. 5). World Health Organization.
United Nations Children’s Fund (UNICEF), World Health Organization (WHO), & International Bank for Reconstruction and Development/The World Bank (2016). Levels and trends in child malnutrition: Key findings of the 2016 edition of the joint child malnutrition estimates. World Health Organization. https://www.who.int/nutgrowthdb/jme_brochure2016.pdf
United Nations Children’s Fund (UNICEF), World Health Organization (WHO), & International Bank for Reconstruction and Development/The World Bank (2018). Levels and trends in child malnutrition: Key findings of the 2018 edition of the joint child malnutrition estimates. World Health Organization. https://www.who.int/nutgrowthdb/jme_brochure2018.pdf
United Nations Development Programme (UNDP) (2018). Human development indices and indicators: 2018 statistical update. United Nations Development Programme (UNDP).
United Nations Children’s Fund (UNICEF), World Health Organization (WHO), & International Bank for Reconstruction and Development/The World Bank (2019). Levels and trends in child malnutrition: Key findings of the 2019 edition of the joint child malnutrition estimates. World Health Organization. https://www.who.int/nutgrowthdb/jme-2019-key-findings.pdf
United Nations (2019). The sustainable development goals report 2019
United Nations Development Programme (UNDP) (2020b). The 2019 global multidimensional poverty index (MPI). United Nations Development Programme (UNDP).
United Nations Children’s Fund (UNICEF), World Health Organization (WHO), & International Bank for Reconstruction and Development/The World Bank (2020). Levels and trends in child malnutrition: Key findings of the 2020 edition of the joint child malnutrition estimates. World Health Organization. https://www.who.int/nutgrowthdb/jme_2020-key-findings.pdf
United Nations (UN) (2020). The sustainable development goals report 2020.
United Nations Development Programme (2020a). Human development report 2020a: The next frontier human development and the anthropocene. Human Development Report Office (HDRO) of the United Nations Development Programme (UNDP).
United Nations Development Programme (UNDP). (2020b). The 2019 global multidimensional poverty index (MPI). United Nations Development Programme (UNDP).
Wagstaff, A., & Watanabe, N. (2000). Socio-economic inequalities in child malnutrition in the developing world (Policy research working paper no. 2434). World Bank.
Wong, H. J., Moy, F. M., & Nair, S. (2014). Risk factors of malnutrition among preschool children in Terengganu, Malaysia: A case control study. BMC Public Health, 14, 785. https://doi.org/10.1186/1471-2458-14-785
World Health Organization (2010). WHO | nutrition landscape information system (NLIS). WHO. http://www.who.int/nutrition/nlis/en/
World Health Organization (2018). The WHO anthro survey analyser. World Health Organization. http://www.who.int/nutgrowthdb/software/en/
World Health Organization (WHO). (2010). WHO | nutrition landscape information system (NLIS). WHO. http://www.who.int/nutrition/nlis/en/
Acknowledgements
The authors are thankful to Mr. Pradip Kumar Mandal, M.A. in Geography, for his constant support and help during the collection of database from the field. They are also grateful to the research participants, who voluntarily expressed their willingness to be a part of this study. Authors are indebted to Dr. Samiran Bisai, Associate Professor of Anthropology and Tribal Studies and Dr. Sadaruddin Biswas, Assistant Professor of Anthropology and Tribal Studies, Sidho-Kanho-Birsha University, Purulia, India, for their kind help in data analysis and interpretation. They are also beholden to Dr. Supravat Bagli, Professor of Economics, Presidency University, Kolkata, India, for his constructive suggestion in framing the study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
MM contributed to conceptualization, planning, methodology, investigation, supervision, formal analysis, writing—original draft, writing—review and editing. DG contributed to supervision, writing—review and editing. MK contributed to conceptualization, methodology, investigation, data curation, software. SM contributed to investigation, formal analysis, data curation. PM contributed to investigation, formal analysis, software, data curation. BG contributed to investigation, formal analysis, software, data curation. DM contributed to investigation, formal analysis, data curation.
Corresponding author
Ethics declarations
Conflict of interest
Authors declare that they do not have any conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mandal, M., Ghosh, D., Karmakar, M. et al. Rural child health in India: the persistent nature of deprivation, undernutrition and the 2030 Agenda. Environ Dev Sustain 26, 4837–4860 (2024). https://doi.org/10.1007/s10668-023-02912-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10668-023-02912-y