
Abstract
Petrol stations emit benzene and other contaminants that have been associated with an increased risk of childhood leukemia. We carried out a population-based case-control study in two provinces in Northern Italy. We enrolled 182 cases of childhood leukemia diagnosed during 1998–2019 and 726 age- and sex-matched population controls. We geocoded the addresses of child residences and 790 petrol stations located in the study area. We estimated leukemia risk according to distance from petrol stations within a 1000 m buffer and amount of supplied fuel within a buffer of 250 m from the child’s residence. We used conditional logistic regression models to approximate risk ratios (RRs) and 95% confidence intervals (CIs) for associations of interest, adjusted for potential confounders. We also modeled non-linear associations using restricted cubic splines. In secondary analyses, we restricted to acute lymphoblastic leukemia (ALL) cases and stratifed by age (<5 and ≥5 years). Compared with children who lived≥1000 m from a petrol station, the RR was 2.2 (95% CI 0.5–9.4) for children living<50 m from nearest petrol station. Associations were stronger for the ALL subtype (RR=2.9, 95% CI 0.6–13.4) and among older children (age≥5 years: RR=4.4, 95% CI 0.6–34.1; age<5 years: RR=1.6, 95% CI 0.1–19.4). Risk of leukemia was also greater (RR=1.6, 95% CI 0.7–3.3) among the most exposed participants when assigning exposure categories based on petrol stations located within 250 m of the child’s residence and total amount of gasoline delivered by the stations. Overall, residence within close proximity to a petrol station, especially one with more intense refueling activity, was associated with an increased risk of childhood leukemia, though associations were imprecise.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Leukemia is the most common cancer among children. Childhood leukemia accounts for approximately 27% of all childhood cancers in the United States and 30-35% in Europe and Asia (e.g., Ireland, France, Germany, China) [1]. Acute lymphoblastic leukemia (ALL) is the most commonly diagnosed childhood cancer worldwide [2] and is more frequent in European and Hispanic populations [3]. According to data from populations covered by high-quality cancer registries, the incidence of ALL has been estimated at 46.4 per 1 million children (i.e., one third of all new diagnoses) [3].
Though epidemiological studies have identified several potential genetic and environmental risk factors for childhood leukemia, uncertainties still surround their causes, the presence of dose-response relations, and the presence of thresholds for environmental contaminants to increase disease risk [4,5,6,7,8,9,10,11,12,13,14,15,16]. Air pollution generated by motorized traffic and industrial sources is one of these putative risk factors [17]. The International Agency for Research on Cancer (IARC) classified outdoor air pollution and particulate matter from outdoor air pollution as carcinogenic to humans (IARC Group 1), based on sufficient evidence of carcinogenicity in humans and experimental animals and strong mechanistic evidence. Among traffic pollutants, there is benzene, a designated Group I carcinogen by the IARC that is associated with adult leukemia and lymphomas [18,19,20], and there is consistent evidence indicating that benzene exposure increases the risk of childhood leukemia [21]. A harmful effect of benzene is still conceivable even at the much lower air pollution levels documented in western countries during the last decades [22].
In urban areas, the highest concentrations of atmospheric pollutants have been found near high-traffic roads. However, since pollutants are emitted during fuel refueling activities and petrol leaks, petrol stations are also considered potential sources of exposure to air pollutants, such as 1,3-butadiene and in particular benzene [23, 24]. Primary petrol compounds enter the air of gas stations due to high evaporation of gasoline. A recent study evaluated the concentration of these compounds in the ambient air of gas stations [23] and found benzene concentrations ranged from about 1 to more than 5 ppm, higher than the recommended exposure limit, 0.1 ppm time weighted average, by The National Institute for Occupational Safety and Health [25, 26].
Some studies have assessed the contribution of petrol refueling stations to the pollutants concentrations in their wider vicinity, finding higher levels of pollutants not only close to the pumps, but also throughout the whole service station area and some distance beyond (50–100 m) [24, 27,28,29,30], depending on station fueling activity and meteorological conditions [29, 31]. To our knowledge, however, no studies have considered the station’s activity when estimating effects of exposure on disease risk, despite the levels of pollutant concentrations around stations being strongly dependent on the amount of fuel delivered [31, 32].
We assessed the extent to which residential exposure to gasoline service stations was associated with risk of childhood leukemia in Northern Italy, by considering both distance from the stations located within proximity of the residence and gas station activity. We also critically summarized existing epidemiologic evidence on the risk of childhood leukemia following long-term exposure to gasoline service stations, updating a previous meta-analysis on this topic [33].
Methods
Case and control selection
Following the Ethics Committee approval [14, 16, 34], we have identified all newly-diagnosed cases of childhood leukemia (ICD-9 codes 204–208) in the 0–14 aged population of Modena and Reggio Emilia, two provinces in Northern Italy (population around 1,200,000), from 1998 to 2019. Details for case and control identification have been described elsewhere in detail [35]. Briefly, we identified the cases through the Italian hospital-based registry of childhood malignancies, available from the Italian Association of Pediatric Emato-Oncology (AIEOP) and capturing all cancer cases arising in Italy [36]. The referent population included four children for each case, matched on sex, year of birth, and province of residence during the year of diagnosis, randomly selected among those enrolled in the National Health Service directory of the Modena and Reggio Emilia provinces, where all residents are compulsorily registered.
We collected data on residential address at time of diagnosis for cases from the AIEOP databased, and in the corresponding year for their matched controls using the historical population database of the National Health Service. We geocoded the home buildings within a Geographical Information System (GIS) using Arc-GIS software (version 9.2, ESRI, Redlands, CA 2006). The satellite coordinates of the residences were retrieved using methodology based on an official geocoding database made available by the Modena and Reggio Emilia Province and, for addresses not included in the database, through the Google Earth App or direct in loco measurement using a portable GPS device (GPSmap 60CSx, Garmin Int. Corp., Olathe, KS) [16, 34, 35]. To identify petrol stations, we obtained information from the Trade Observatory of the Emilia-Romagna Region about all the 859 facilities located in the territory of Modena and Reggio Emilia provinces. All stations were georeferenced in the GIS through Google Earth or in loco measurements, focusing on the exact position of the pumps whenever possible, or to the geometric center of the station area.
Exposure to petrol station
We assessed exposure to petrol stations in two ways. First, petrol station exposure was expressed as distance from home to the nearest petrol station divided into categories with the following cut points: 50, 200, 500, 1000 and over 1000 m.
Secondly, we estimated the activity of each station in terms of fuel sold over an entire year, and we assessed child exposure to all stations located up to 1000 m around the residences. For this purpose, through record-linkage with the database provided by the Trade Observatory of the Emilia-Romagna Region, we retrieved the average daily quantity (L/day) of fuel sold in each petrol station in the year of leukemia diagnosis for cases and their matched controls. The total average daily quantity of fuel supplied by all the petrol stations located within 250 m buffer around residence was computed for each study participant. For this analysis, we then categorized petrol station exposure based on the amount of supplied fuel as follows: 0 = no petrol stations within the 250 m-buffer; 1 = fuel supply until 149 L/day within the 250 m-buffer; 2 = fuel supply ≥ 150 until 999 L/day within the 250 m-buffer; and 3 = fuel supply ≥ 1000 L/day within the 250 m-buffer.
Confounders
We considered several potential confounders in multivariable analysis. We modeled outdoor air concentration of PM10 at the residence of each child, using the CAlifornia LINE Source Dispersion Model, version 4 (CALINE4 - Sacramento CA, Dept. of transportation, Division of New Technology and Research, 1989), a line source air quality model, based on vehicular traffic flow parameters and meteorological data [34]. We also modeled the magnetic fields generated by the 132 + kV power lines possibly located close to the child’s residence in the study territory using a methodology previously validated and explained in detail [16, 37]. We also included as adjustment factor to the multivariable analysis the presence of indoor transformer stations in the building of residence, using information about high-voltage power line net and transformer stations in the two study provinces made available by the Emilia-Romagna Regional Agency for Environmental Prevention and Energy (ARPAE). We then determined the urban and arable crop by calculating the percentage of the land use type in proximity to each geocoded home, based on a circular area with a radius of 100 m around the residence of each child according to the Land Use Map 2014 for both Modena and Reggio Emilia provinces [14, 38, 39].
We also collected information on socio-demographic variables maternal age and ethnicity using birth certificate data provided by the Local Health Authorities of Modena and Reggio Emilia, and parental annual income for the index year by the Italian Revenue Agency of the Ministry of Finance.
Data analysis
We estimated the risk ratio (RR) of childhood leukemia in relation to categorical distance (categorized as < 20, 50 - <200, 200 - <500, 500 - <1000 and ≥ 1000 m) to the nearest petrol station by computing the disease odds ratio and its 95% confidence interval (CI) using conditional logistic regression models, with matching for age, sex and province of residence. In the multivariable models, we included as potential confounders the following variables: modeled PM10 concentrations, calculated ELF-MF (categorized as < 0.1, 0.1 - <0.2, 0.2 - <0.4 and ≥ 0.4 µT) [16], presence of electric transformer rooms near the building of residence (categorized as < 5 m, ≥ 5 - <10 m, ≥ 10 - <20 m, - ≥20 m), percentage of urban area providing information related to the type of neighborhood within the 100 m-buffer around the residence [35], and percentage of arable crops within the 100 m-buffer around the residence (continuous) as related to pesticide exposure [14]. In addition, in a subgroup analysis for participants having additional information available, we added maternal ethnicity (categorized as white, Black or Asian), father income, and maternal age at delivery (continuous). We also conducted subgroup analyses by child’s age of diagnosis (< 5 and ≥ 5 years), and restricted to ALL, the only cancer subtype with sufficient numbers for meaningful analyses. We used restricted cubic splines to model the shape of the association. We selected the number of knots using the Akaike Information Criterion (AIC) and the knot-placement method [40] to assess the association between residential distance from the nearest petrol station and RR of leukemia through a nonlinear model based on restricted cubic splines, using three knots at fixed distances (50, 200, and 500 m) and ≥ 1000 m as the reference.
Updated systematic review and meta-analysis
We performed a systematic literature search (PROSPERO registration no. CRD42023402919) using online databases PubMed/MEDLINE, Web of Science and EMBASE from inception up to April 3, 2023 according the PRISMA guidelines [41]. We also used citation chasing methods namely backward and forward reference list scanning to retrieve additional eligible papers. Two authors (TF and MV) performed the screening of title/abstract and then of the full-text with the help of a third author (MM) to solve disagreement. According PECOS (population, exposure, comparison, outcome and study design) statement, we searched all observational studies that have investigated the risk of childhood leukemia in relation to exposure to petrol station using either proximity of children residence or modelled exposure. We used keywords related to ‘petrol’ or ‘gasoline station’ and ‘childhood’ or ‘infant leukemia’. Details of literature search are reported in Supplemental Table S1. We assessed the risk of bias (RoB) of included studies using the Newcastle - Ottawa quality assessment scale (NOS). Details of criteria for study evaluation are reported in Supplemental Table S2. Two authors independently performed the RoB assessment (MM and TF), with discrepancies solved based on the review of a third author (MV). We carried out a highest versus lowest exposure meta-analysis of all eligible studies using a random-effects model, and we performed stratified analysis according exposure assessment method (i.e., using questionnaires or georeferencing data). Finally, we assessed potential for publication bias using a funnel plot and Egger’s test.
Results
The study enrolled 183 incident cases of childhood leukemia, of which 148 were cases of lymphoblastic leukemia ALL, and 732 matched controls. We excluded one case (alongside the respective controls) and two additional eligible controls due to missing residential information. The final analysis included 182 cases (98 males and 84 females) and 726 age-and sex-matched population controls. The average age at diagnosis was 6.2 years (standard deviation: 3.9), with corresponding median value of 5.7 years (interquartile range-IQR: 3.0–9.0). The median values (IQR) for cases and controls of the adjustment variables were: fuel supply (L/day) within the 1000 m-buffer = 804 (0-2454) and 868 (0-2255); PM10 (µg/m3) = 4.9 (2.4–8.3) and 4.6 (2.0-7.8); urban area within the 100 m-buffer around the residence = 0.6 (0.4–0.8) and 0.6 (0.4–0.8); arable crops within the 100 m-buffer around the residence = 0.0 (0.0-0.1) and 0.0 (0.0-0.1), respectively. Distribution for ELF-MF was categorized as follows: <0.1 µT for 180 cases and 725 controls; 0.1 - <0.2 µT for 0 cases and 1 control; 0.2 - <0.4 µT for 1 case and 0 controls and ≥ 0.4 µT 1 case and 0 controls. Electric transformer rooms near the building of residence were categorized for cases and controls as follows: ≥20 m for 178 cases and 709 controls; ≥10 and < 20 m for 2 cases and 10 controls; ≥5 and < 10 m for 1 case and 4 controls; <5 m for 1 case and 3 controls. Data on the distribution of cases and controls by residential proximity to the nearest petrol station and by exposure category are reported in Table 1.
RRs for leukemia risk according to residential proximity to the nearest petrol station are shown in Table 2. Compared to those living ≥ 1000 m, RRs for children living < 50 m were 2.3 (95% CI 0.5–10.0) and 2.2 (95% CI 0.5–9.4) in crude and adjusted analyses, respectively. Corresponding RRs were stronger in analyses confined to ALL cases: 2.8 (95% CI 0.6–13.2) and 2.9 (95% CI 0.6–13.4), respectively.
The age-stratified results are presented in Table 2. Focusing on children whose residence was extremely close to petrol station (< 50 m), we found an increased risk among older children (age ≥ 5 years) of 4.3 (95% CI 0.6–32.4) compared with 1.2 (95% CI 0.1–12.2) among younger children (age < 5 years) in the bivariate model. When limiting the analysis to ALL cases in the bivariate model, RRs were 1.6 (95% CI 0.1–18.8) among younger children and 4.7 (95% CI 0.6–36.0) among older children. In multivariable analysis, we found relatively similar RRs for all leukemia cases and as well as ALL cases (Table 2).
In spline regression analyses for overall leukemia (Fig. 1) and ALL (Fig. 2), residential proximity to a petrol station was positively associated with leukemia risk only within close proximity of the station (< 50 m): RR = 1.4 (95% CI 0.6–2.9).

Spline regression analysis assessing the risk ratio of childhood leukemia according to distance of child’s residence from the closest petrol station. Restricted cubic spline with three knots at fixed distances (50, 200, and 500 m). A Bivariate model; B Multivariable model

Spline regression analysis assessing the risk ratio of childhood acute lymphoblastic leukemia (ALL) according to distance of child’s residence from petrol station. Restricted cubic spline with three knots at fixed distances (50, 200, and 500 m). A Bivariate model; B Multivariable model
When we considered all the petrol stations located within 250 m of the child’s residence, as well as the total amount of gasoline sold by the station the year before the index year, RRs for leukemia were 1.6 (95% CI 0.8–3.2) and 1.6 (95% CI 0.7–3.3) in bivariate and multivariable analyses, respectively, for the highest category of exposure (Table 3), with no indication of monotonic relation across the exposure categories. Corresponding RR estimates for ALL were 1.5 (0.6–3.5) and 1.5 (0.6–3.8). Older children (age ≥ 5 years) living inside buffer of 250 m with petrol stations that have sold more than 1000 L/day had a higher risk of leukemia overall (bivariate and multivariable models: RR = 2.1, 95% CI 0.8–5.1 and RR = 2.4, 95% CI 0.9–6.1, respectively), and of ALL (RR = 2.4, 95% CI 0.8–7.2 in the bivariate model and RR = 3.4, 95% CI 1.0-11.1 in the multivariable model). In the remaining categories of exposure, there was no clear association, neither evidence of dose-response trends. Sensitivity analyses among subjects with complete data on demographic variables, specifically maternal ethnicity and paternal income, showed similar though less precise results (Supplemental Table S3) when compared with the overall analysis and the analysis among the same subgroup without adjusting for these additional variables.
In the systematic review and meta-analysis, our literature search retrieved 31 records after removal of duplicates. We then excluded 20 studies after title/abstract screening and an additional six studies after full-text evaluation as they assessed benzene exposure during parental occupation only (n = 1), petrol station exposure was not evaluated (n = 2), or were conference abstract (n = 1) or commentaries (n = 2) (Supplemental Figure S2). We retrieved one additional study [42] through citation chasing, leading to a total of six studies for analysis not including the present study. Characteristics of retrieved studies are reported in Table 4. The ages of the study populations for all in the range 0–14 years, with dates of diagnosis ranging from 1985 to 2019. All studies had a case-control design, including a case-cohort study [33]. Three studies investigated exposure to petrol station using questionnaire [42,43,44], although one study assessed exposure to both petrol station and car repair garage [43]. One study validated questionnaire-based exposure using georeferencing data [44]. The three remaining studies used georeferencing data for exposure assessment [33, 45, 46], one in particular through evaluation of petrol station density (number of stations per km2). Results of the bias assessment are reported in Supplemental Table S4.
Meta-analysis of the results of the aforementioned six studies plus those generated by the present study are reported in Fig. 3, showing a summary RR of 1.66 (95% CI 1.14–2.41). Analyses stratified by modality of exposure assessment yielded similar results, with lower precision for studies based on questionnaire data (Supplemental Figure S3). Sensitivity analysis excluding the study assessing also proximity of car repair garages showed consistent results, yielding a summary RR of 1.50 (95% CI 1.05–2.15) (Supplemental Figure S4). The sensitivity analysis restricted to four “high-quality” studies (NOS score ≥ 8) still showed an elevated disease risk with RR = 1.80 (95% CI 1.37–2.38) (Supplemental Figure S5). The funnel plot showed some evidence of publication bias (Supplemental Figure S6).

Forest-plot of the meta-analysis of the association between petrol station exposure and childhood leukemia risk. The area of each grey square is proportional to the inverse of the variance of the estimated log risk ratio (RR) and horizontal lines represent their 95% confidence intervals (Cis). The black diamond represents the combined RR using the random-effects restricted maximum likelihood (REML) model. The solid vertical line represents RR = 1
Discussion
In this study, we examined childhood leukemia risk in relation to proximity to petrol stations. We observed an increased leukemia risk, though imprecise, when assessing exposure as distance from residence (< 50 m) to the nearest petrol station, while the excess risk associated with the intensity of activity of all stations located < 250 m from the residence was not as large. In both analyses no dose-response relation emerged, since a clear excess risk occurred only in the highest exposure category, suggesting the occurrence of a threshold of exposure to the fugitive chemical emissions from fuel pumps, heightening disease risk, mainly based on the distance from the station. This suggests a far higher relevance of close residential proximity to the gas station when compared with ‘moderate’ proximity and with the overall station refueling activity, in terms of increasing childhood leukemia risk.
While there are no previous studies based on the station activity, to the best of our knowledge, our results on residential distance from petrol station are consistent with three of the four studies carried out on the same topic. In a UK study [46] that estimated childhood cancer risks in relation to proximity to main roads and petrol stations, a slight increase in leukemia risk was found within 100 m from a petrol station (OR = 1.5, 95% CI 0.6–2.9). In a hospital-based case-control study in France [43], residence close to a petrol station or a repair garage during childhood was strongly associated with excess risk of childhood leukemia (OR = 4.0, 95% CI 1.5 to 10.3). This association was even stronger for acute non-lymphocytic leukemia (OR = 7.7, 95% CI 1.7 to 34.3), and was not altered by adjustment for potential confounding factors. In 2009, Brosselin et al. [44] reported results of a large national registry-based case-control study ESCALE in France (2003–2004) indicating a strong positive association between living in a residence adjoining of a garage or petrol station and acute childhood leukemia. However, these studies differed from ours regarding exposure definitions and assessment: while we classified children living within 50 m of a petrol station in the highest exposure category, the English study used a 100 m threshold and the French studies considered only children living close to a gas station, without specifying the exact distance, also assessing exposure through interviews with the children’s mothers and thus potentially affected by recall bias [43, 44]. In a case-control study carried out in Malaysia [42], and based on data collected through questionnaires, no association emerged, though the cut point used to refine residential exposure was quite large, not comparable to that used in the other studies including our one and likely inadequate to detect any association (≤ 1 km vs. >1 km from a petrol station).
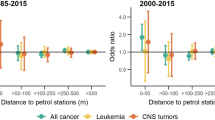
An additional case-control study [45] revealed an exposure-response relation between petrol station density (per square kilometer), as a marker of traffic-related air pollution, and the risk of leukemia in young children. A nationwide case-control study carried out in Switzerland (during 1985–2015) found evidence of an increased risk of childhood cancer (all diagnoses combined) among children living in close vicinity (< 50 m vs. ≥500 m) of petrol stations [33].
A relevant distinct feature of the present analysis is the integration of data on petrol station activity along with its distance from the child’s residence. There is clear evidence from studies of gas station workers that their exposure to air pollutants is positively related to the volume of refueling in petrol stations, as well as the confinement of pollutants in semi-closed spaces of the work place [25, 47,48,49].
Our results showed a direct relation between residing in close proximity to a petrol station and risk of leukemia, both based on fixed cut points of distance from the stations and modeling exposure through a combination of distance and gas station activity. Associations were strongest for ALL cases in older children (age ≥ 5 years), with a two-fold increased risk for children in the category of major exposure (< 50 m) and a four-fold increased risk among children diagnosed after 5 years. The latter finding might be ascribed to a higher cumulative exposure among older children, due to both their age and to their tendency to spend more time outside. Such excess risk may persist up to 250 m from the gas station also depending on their activity, a plausible finding given the results of air monitoring studies [31, 50].
In this study, we assessed exposure without requiring any active participation by study participants and their families, nor by petrol station personnel, thus avoiding selection and information bias, as individual participation was not needed. We also carried out the exposure assessment in a blinded manner with reference to the case and control status of the participants. A potential limitation of our study is that information on the activity of each petrol station was available during 1998–2017 only. Since our study includes children with diagnoses that occurred from 1998 to 2019, we decided to consider, for the last two years 2018-19 and for each station, the fuel supply corresponding to the most recent year available: 2017. Residual or unmeasured confounding could have also been possible, and some demographic characteristics were unavailable for many study participants as well as complete information about medical imaging procedures [4]. A sensitivity analysis limited to study participants accounting for all potential confounders measured yielded similar results to the analysis carried out without such more comprehensive adjustment, both in this subgroup and in the entire study population, suggesting that the demographic factors for which we lacked complete information were not a major source of confounding. However, we may not have collected and controlled for all relevant confounders of the associations (e.g., using paternal income as a proxy for household income, or lacking information about exposure to ionizing radiation for diagnostic purposes), and therefore some effect of residual confounding in biasing our results could not be entirely ruled out [51]. We also acknowledge the statistical instability of our risk estimates, due to the very limited number of exposed children, a limitation suggesting caution in interpreting our results, though being consistent with the results from the other comparable studies as reflected by the pooled estimates of the meta-analysis. Finally, we acknowledge the potential for exposure misclassification associated with lack of historical residential stability or time spent at home (e.g., a substantial part of the daytime hours may have spent at a different residence (e.g., grandparents’ home, school, or day care). However, while we could not comprehensively assess residential mobility or time spent at one’s residence since the study design did not include a direct contact with children’s families, residential stability of the study participants was likely to be high (> 70% for all children and > 82% for children less than 5 years) based on data previously ascertained in subgroup of the study population [14, 16, 34].
Abbreviations
- AIC:
-
Akaike Information Criterion
- AIEOP:
-
Associazione Italiana Ematologia Oncologia Pediatrica
- ARPAE:
-
Regional Agency for Environmental Protection and Energy
- CI:
-
Confidence interval
- GIS:
-
Geographical Information System
- ICD-9:
-
International Classification of Diseases, 9th Edition
- µT:
-
MicroTesla
- RR:
-
Relative risk
References
Namayandeh SM, Khazaei Z, Lari Najafi M, Goodarzi E, Moslem A. GLOBAL leukemia in children 0–14 statistics 2018, incidence and mortality and human development index (HDI): GLOBOCAN sources and methods. Asian Pac J Cancer Prev. 2020;21(5):1487–94. https://doi.org/10.31557/APJCP.2020.21.5.1487.
Sun Y, Long S, Liu W. Observation of the molecular genetics among children with acute lymphoblastic leukemia: a retrospective study based on the SEER database. Med (Baltim). 2020;99(21):e20009. https://doi.org/10.1097/MD.0000000000020009.
Steliarova-Foucher E, Colombet M, Ries LAG, et al. International incidence of childhood cancer, 2001-10: a population-based registry study. Lancet Oncol. 2017;18(6):719–31. https://doi.org/10.1016/S1470-2045(17)30186-9.
Onyije FM, Olsson A, Baaken D, et al. Environmental risk factors for childhood acute lymphoblastic leukemia: an umbrella review. Cancers (Basel). 2022;14(2):382. https://doi.org/10.3390/cancers14020382.
Karalexi MA, Tagkas CF, Markozannes G, et al. Exposure to pesticides and childhood leukemia risk: a systematic review and meta-analysis. Environ Pollut. 2021;285:117376. https://doi.org/10.1016/j.envpol.2021.117376.
Mazzei-Abba A, Folly CL, Kreis C, et al. External background ionizing radiation and childhood cancer: update of a nationwide cohort analysis. J Environ Radioact. 2021;238–239:106734. https://doi.org/10.1016/j.jenvrad.2021.106734.
Lupatsch JE, Kreis C, Konstantinoudis G, Ansari M, Kuehni CE, Spycher BD. Birth characteristics and childhood leukemia in Switzerland: a register-based case-control study. Cancer Causes Control. 2021;32(7):713–23. https://doi.org/10.1007/s10552-021-01423-3.
Van Maele-Fabry G, Gamet-Payrastre L, Lison D. Household exposure to pesticides and risk of leukemia in children and adolescents: updated systematic review and meta-analysis. Int J Hyg Environ Health. 2019;222(1):49–67. https://doi.org/10.1016/j.ijheh.2018.08.004.
Kreis C, Doessegger E, Lupatsch JE, Spycher BD. Space-time clustering of childhood cancers: a systematic review and pooled analysis. Eur J Epidemiol. 2019;34(1):9–21. https://doi.org/10.1007/s10654-018-0456-y.
Amoon AT, Crespi CM, Ahlbom A, et al. Proximity to overhead power lines and childhood leukaemia: an international pooled analysis. Br J Cancer. 2018;119(3):364–73. https://doi.org/10.1038/s41416-018-0097-7.
Schuz J, Erdmann F. Environmental exposure and risk of childhood leukemia: an overview. Arch Med Res. 2016;47(8):607–14. https://doi.org/10.1016/j.arcmed.2016.11.017.
Metayer C, Petridou E, Arangure JM, et al. Parental tobacco smoking and acute myeloid leukemia: the Childhood Leukemia International Consortium. Am J Epidemiol. 2016;184(4):261–73. https://doi.org/10.1093/aje/kww018.
Wiemels J. Perspectives on the causes of childhood leukemia. Chem Biol Interact. 2012;196(3):59–67. https://doi.org/10.1016/j.cbi.2012.01.007.
Malagoli C, Costanzini S, Heck JE, et al. Passive exposure to agricultural pesticides and risk of childhood leukemia in an italian community. Int J Hyg Environ Health. 2016;219(8):742–8. https://doi.org/10.1016/j.ijheh.2016.09.015.
Pedersen C, Johansen C, Schuz J, Olsen JH, Raaschou-Nielsen O. Residential exposure to extremely low-frequency magnetic fields and risk of childhood leukaemia, CNS tumour and lymphoma in Denmark. Br J Cancer. 2015;113(9):1370–4. https://doi.org/10.1038/bjc.2015.365.
Malagoli C, Fabbi S, Teggi S, et al. Risk of hematological malignancies associated with magnetic fields exposure from power lines: a case-control study in two municipalities of northern Italy. Environ Health. 2010;9:16. https://doi.org/10.1186/1476-069X-9-16.
Kreis C, Heritier H, Scheinemann K, et al. Childhood cancer and traffic-related air pollution in Switzerland: a nationwide census-based cohort study. Environ Int. 2022;166:107380. https://doi.org/10.1016/j.envint.2022.107380.
IARC, Benzene. IARC Monographs on the evaluation of carcinogenic risks to humans. Volume 120. France: Lion; 2018.
Talbott EO, Xu X, Youk AO, Rager JR, Stragand JA, Malek AM. Risk of leukemia as a result of community exposure to gasoline vapors: a follow-up study. Environ Res. 2011;111(4):597–602. https://doi.org/10.1016/j.envres.2011.03.009.
Goldstein BD. Benzene as a cause of lymphoproliferative disorders. Chem Biol Interact. 2010;184(1–2):147–50. https://doi.org/10.1016/j.cbi.2009.12.021.
Filippini T, Hatch EE, Rothman KJ, et al. Association between outdoor air pollution and childhood leukemia: a systematic review and dose-response meta-analysis. Environ Health Perspect. 2019;127(4):46002. https://doi.org/10.1289/EHP4381.
Ghahremanloo M, Lops Y, Choi Y, Mousavinezhad S. Impact of the COVID-19 outbreak on air pollution levels in East Asia. Sci Total Environ. 2021;754:142226. https://doi.org/10.1016/j.scitotenv.2020.142226.
Allahabady A, Yousefi Z, Tahamtan RAM, Sharif ZP. Measurement of BTEX (benzene, toluene, ethylbenzene and xylene) concentration at gas stations. Environ Health Eng Manag. 2022;9(1):23–31. https://doi.org/10.34172/Ehem.2022.04.
Jo WK, Oh JW. Exposure to methyl tertiary butyl ether and benzene in close proximity to service stations. J Air Waste Manag Assoc. 2001;51(8):1122–8. https://doi.org/10.1080/10473289.2001.10464339.
Chaiklieng S, Suggaravetsiri P, Autrup H. Risk Assessment on benzene exposure among gasoline station workers. Int J Environ Res Public Health. 2019;16(14):2545. https://doi.org/10.3390/ijerph16142545.
The National Institute for Occupational Safety and Health (NIOSH). Immediately Dangerous to Life or Health concentrations (IDLH), Benzene. 1994.
Duarte-Davidson R, Courage C, Rushton L, Levy L. Benzene in the environment: an assessment of the potential risks to the health of the population. Occup Environ Med. 2001;58(1):2–13. https://doi.org/10.1136/oem.58.1.2.
Gonzalez-Flesca N, Vardoulakis S, Cicolella A. BTX concentrations near a stage II implemented petrol station. Environ Sci Pollut Res Int. 2002;9(3):169–74. https://doi.org/10.1007/BF02987484.
Sairat T, Homwuttiwong S, Homwutthiwong K, Ongwandee M. Investigation of gasoline distributions within petrol stations: spatial and seasonal concentrations, sources, mitigation measures, and occupationally exposed symptoms. Environ Sci Pollut Res Int. 2015;22(18):13870–80. https://doi.org/10.1007/s11356-015-4615-3.
Uren S, Report. SSE/AQ/1085: a pilot study to assess benzene concentration in the vicinity of petrol stations: Department for Environmental Food & Rural Affairs - Air Quality Division. London, UK Division DotE-AQ;1996. Report No.: SSE/AQ/1085.
Karakitsios SPD, Kassomenos VK, Pilidis PA. Contribution to ambient benzene concentrations in the vicinity of petrol stations: estimation of the associated health risk. Atmos Environ. 2007;41:1889–902. https://doi.org/10.1016/j.atmosenv.2006.10.052.
Sarigiannis DA, Karakitsios SP, Gotti A, Papaloukas CL, Kassomenos PA, Pilidis GA. Bayesian algorithm implementation in a real time exposure assessment model on benzene with calculation of associated cancer risks. Sens (Basel). 2009;9(2):731–55. https://doi.org/10.3390/s90200731.
Mazzei A, Konstantinoudis G, Kreis C, et al. Childhood cancer and residential proximity to petrol stations: a nationwide registry-based case-control study in Switzerland and an updated meta-analysis. Int Arch Occup Environ Health. 2022;95(5):927–38. https://doi.org/10.1007/s00420-021-01767-y.
Vinceti M, Rothman KJ, Crespi CM, et al. Leukemia risk in children exposed to benzene and PM(10) from vehicular traffic: a case-control study in an italian population. Eur J Epidemiol. 2012. https://doi.org/10.1007/s10654-012-9727-1.
Malagoli C, Malavolti M, Costanzini S, et al. Increased incidence of childhood leukemia in urban areas: a population-based case-control study. Epidemiol Prev. 2015;39(4 Suppl 1):102–7.
Ferrari A, Dama E, Pession A, et al. Adolescents with cancer in Italy: entry into the national cooperative paediatric oncology group AIEOP trials. Eur J Cancer. 2009;45(3):328–34. https://doi.org/10.1016/j.ejca.2008.12.003.
Andreuccetti D. Manuale programma CAMPI version 4.1. Firenze: Consiglio Nazionale delle Ricerche; 2002.
Vinceti M, Filippini T, Violi F, et al. Pesticide exposure assessed through agricultural crop proximity and risk of amyotrophic lateral sclerosis. Environ Health. 2017;16(1):91. https://doi.org/10.1186/s12940-017-0297-2.
Costanzini S, Teggi S, Bigi A, et al. Atmospheric dispersion modelling and spatial analysis to evaluate population exposure to pesticides from farming processes. Atmosphere. 2018;9(2):38. https://doi.org/10.3390/atmos9020038.
Harrell FE. Regression modeling strategies with applications to linear models, logistic regression, and survival analysis. 1 edition ed: Springer Cham; 2001.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–89. https://doi.org/10.1016/j.jclinepi.2021.03.001.
Abdul Rahman HI, Shah SA, Alias H, Ibrahim HM. A case-control study on the association between environmental factors and the occurrence of acute leukemia among children in Klang Valley, Malaysia. Asian Pac J Cancer Prev. 2008;9(4):649–52.
Steffen C, Auclerc MF, Auvrignon A, et al. Acute childhood leukaemia and environmental exposure to potential sources of benzene and other hydrocarbons; a case-control study. Occup Environ Med. 2004;61(9):773–8. https://doi.org/10.1136/oem.2003.010868.
Brosselin P, Rudant J, Orsi L, et al. Acute childhood leukaemia and residence next to petrol stations and automotive repair garages: the ESCALE study (SFCE). Occup Environ Med. 2009;66(9):598–606. https://doi.org/10.1136/oem.2008.042432.
Weng HH, Tsai SS, Chiu HF, Wu TN, Yang CY. Childhood leukemia and traffic air pollution in Taiwan: petrol station density as an indicator. J Toxicol Environ Health A. 2009;72(2):83–7. https://doi.org/10.1080/15287390802477338.
Harrison RM, Leung PL, Somervaille L, Smith R, Gilman E. Analysis of incidence of childhood cancer in the West Midlands of the United Kingdom in relation to proximity to main roads and petrol stations. Occup Environ Med. 1999;56(11):774–80. https://doi.org/10.1136/oem.56.11.774.
Dehghani M, Fazlzadeh M, Sorooshian A, et al. Characteristics and health effects of BTEX in a hot spot for urban pollution. Ecotoxicol Environ Saf. 2018;155:133–43. https://doi.org/10.1016/j.ecoenv.2018.02.065.
Geraldino BR, Nunes RFN, Gomes JB, et al. Evaluation of exposure to toluene and xylene in gasoline station workers. Adv Prev Med. 2021;2021:5553633. https://doi.org/10.1155/2021/5553633.
Tongsantia U, Chaiklieng S, Suggaravetsiri P, Andajani S, Autrup H. Factors affecting adverse health effects of gasoline station workers. Int J Environ Res Public Health. 2021;18(19):10014. https://doi.org/10.3390/ijerph181910014.
Kwon J, Weisel CP, Turpin BJ, et al. Source proximity and outdoor-residential VOC concentrations: results from the RIOPA study. Environ Sci Technol. 2006;40(13):4074–82. https://doi.org/10.1021/es051828u.
Marinacci C, Spadea T, Biggeri A, Demaria M, Caiazzo A, Costa G. The role of individual and contextual socioeconomic circumstances on mortality: analysis of time variations in a city of north west Italy. J Epidemiol Community Health. 2004;58(3):199–207. https://doi.org/10.1136/jech.2003.014928.
Funding
This study was supported by Modena Charity Associazione Sostegno Ematologia Oncologia Pediatrica – ASEOP and by the grant FAR (Fondo di Ateneo per la Ricerca) 2022 from the University of Modena and Reggio Emilia.
Author information
Authors and Affiliations
Contributions
MV and CM conceived the study. Material preparation and data collection were performed by MM, CM, TF, AB, GP, MC and SC. Data analyses were performed by MM, CM, TF and MV. The first draft of the manuscript was written by MM and CM; and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
LAW is a consultant for AbbVie Inc. and the Gates Foundation, and has received in-kind donations for primary data collection in PRESTO from Swiss Precision Diagnostics and Kindara.com. All other authors declare that they have no competing interests.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Modena Ethics Committee (approval number 1103/2020/OSS/AUO/MO).
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Malavolti, M., Malagoli, C., Filippini, T. et al. Residential proximity to petrol stations and risk of childhood leukemia. Eur J Epidemiol 38, 771–782 (2023). https://doi.org/10.1007/s10654-023-01009-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10654-023-01009-0