
Abstract
Background
Biologic therapies are effective at inducing and maintaining remission in people with inflammatory bowel disease (IBD). Previous studies have associated TNF-a inhibitors with weight gain, however, it is unclear if this is a class-specific effect or a manifestation of good disease control. To clarify this issue, a retrospective study was undertaken to examine weight changes over time during therapy with different biologic agents.
Methods
Adult patients with IBD who received any biological therapy for at least 12 months, between 2008 and 2020, were identified at two specialised IBD services. Demographic, disease, and therapy-related data were examined.
Weight change and patterns thereof were examined for each specific therapy and relationships amongst weight outcomes and various predictive factors explored.
Results
Of 294 patients (156 females), 165 received Infliximab (IFX), 68 Adalimumab (ADA), 36 Vedolizumab (VDZ) and 25 Ustekinumab (UST). There was a statistically significant weight gain over time in the IFX and VDZ groups and more weight gain in the IFX vs ADA and VDZ vs ADA at most time points.
Three weight trajectories were identified: around 95% of patients had small weight loss or a modest weight gain but 5% of patients, most of whom were on IFX had marked weight gain (24.3 kg). Having a baseline high BMI, being female, having an initiation CRP ≤ 5 or albumin > 35 reduced the odds of major weight gain.
Conclusion
Weight gain in biologic treated IBD patients appears to be associated with clinical factors (male gender, high CRP, low albumin) and therapy-specific factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Inflammatory bowel disease (IBD) is a group of chronic immune-mediated intestinal disorders predominantly recognised as Crohn’s Disease (CD) and ulcerative colitis (UC). The pathophysiology of IBD involves complex genetic, environmental, microbial, and immune-related factors. Inadequately treated IBD can lead to serious potentially preventable complications [1. The current standard medical treatment approaches involve single agent or combination therapy with both targeted and older untargeted therapies. Commonly used targeted biological therapies include monoclonal antibodies such as anti-tumour necrosis factor-alpha (TNF-α), anti-α4β7, and anti-Interleukin-12/Interleukin-23 (IL12/23) antibodies.
TNF-α inhibitors such as Infliximab (IFX) and Adalimumab (ADA), are monoclonal antibodies that neutralize pro-inflammatory cytokines. There is an association suggested between this class (particularly IFX) and weight gain [2,3,4,5], with multiple proposed mechanisms such as improved disease activity and subsequent increase in muscle mass and reduced visceral sensitivity and hence fullness sensation [2, 6,7,8].However, it remains generally unclear if this is a true causal relationship or whether weight gain is simply a “desired” consequence of good disease control.
Assessment of this phenomenon can be challenging, as patients with IBD treated with IFX usually have a high baseline inflammatory burden and poor nutritional status, meaning that weight gain might simply be related to the reversal of gut inflammation and improved nutrition. However, it is important to note that many of the published studies [4, 5], included patients with rheumatological conditions, thus weight gain in anti-TNF-α treated patients may not be exclusively the result of improvement in gut function.
One of the largest analyses [2] of weight gain in IBD patients treated with anti-TNF-α, reported weight changes in kilograms, without including Body Mass Index (BMI). Despite its well-described limitations notably as a determinant of body fat mass and distribution and of nutritional status [9], BMI has valid national reference data and a reported relationship with levels of adiposity, hence, measuring BMIs throughout the treatment period, is an acceptable primary tool [10] to indicate whether weight change goes in an appropriate or inappropriate direction.
Obesity is associated with an increased risk of complications in IBD and loss of response to therapy [11]. Contrary to conventional belief, up to one-third of patients with IBD are obese, which parallels rates in the general population [11]. More interestingly, the increasing incidence of CD over the last two decades parallels the obesity epidemic [12]. It has been postulated that visceral adiposity might increase the risk of developing CD, progressing to penetrating disease, and requiring surgery [13, 14]; hence, it is important for IBD clinicians to consider obesity treatment as an important element of their patient care.
We, therefore, conducted this study to:
-
Compare weight and BMI changes from baseline during therapy with different biologic agents.
-
Examine different weight patterns over time and assess for possible clinical characteristics associating with each subgroup.
-
Determine whether weight change reflects the extent of suppression of systemic indices of inflammation (CRP) and remission state.
Methods
Patient Cohort and Characteristics
Adult patients who received any biologic therapy for IBD for at least 12 months between 2008 and 2020, were identified from prospectively maintained medical records at two hospital-based IBD centers.
Extracted data included: demographics; weight and BMI at baseline, 6, 12, 24, and 48 months; IBD type and phenotype; IBD treatment site (Royal Adelaide Hospital/Logan Hospital); disease duration, baseline endoscopy, follow up endoscopy (if available), hemoglobin (Hb), C-reactive protein (CRP), albumin (alb); monotherapy or combination therapy; initial steroid therapy and biologic dosing schedule.
Treatment Schedules and Assessment Times
Common causes for primary and secondary non-response include inadequate dosing that can be identified through assessment of drug and anti-drug antibody levels. Both dose intensification from 5 mg/kg [15] to 7.5 mg/kg or 10 mg/kg 8 weekly and increased infusion frequency to 4 weekly or 6 weekly are widely accepted strategies to optimize IFX levels [15].
Standard ADA maintenance therapy is given in 40 mg subcutaneous (SC) injections every other week [16]; if escalation is needed, the dose can be increased to 60 or 80 mg or the frequency can be increased to weekly.
The recommended standard maintenance dose of VDZ is 300 mg IV every 8 weeks that can be escalated to 300 mg 6 or 4 weekly in case of inadequate response [17, 18].
For Ustekinumab, after weight-based IV induction therapy, maintenance is usually with 90 mg SC injections every 8 weeks, [19] frequency can be increased to 4 or 6 weekly if escalation is needed.
We note that in Australia, clinical remission is a pre-requisite for ongoing pharmaceutical benefit scheme (PBS) subsidy of any of the biologic therapies.
Data and Sources
Data was collected from prospectively made entries into hospitals’ electronic medical records and specific IBD databases. Endoscopy data prior to initiation of biological therapy was collected from “Provation” endoscopy electronic record system. Due to the lack of standardized IBD reporting among endoscopists and for the simplicity of analysis, endoscopic disease activity for both CD and UC was recorded as in remission, mild, moderate, or severe. For CD, when the Simple endoscopic score for Crohn’s Disease (SES-CD) was reported by the endoscopist [20], the following decoding applied: 0–2 (remission), 3–6 (mild disease), 7–15 (moderate disease), > 15 severe disease; otherwise, the description reported by the endoscopist was recorded. For UC, when the Mayo score was reported by the endoscopist [21], the following decoding applied: 0 (remission), 1 (mild disease), 2 (moderate disease), 3 (severe disease); otherwise, we recorded the description used by the endoscopist.
Patients with any missing data but follow up endoscopy were excluded from the study.
Statistical Analysis
Weight change from baseline was examined with a linear mixed-effects model, including the interaction of treatment group and time period. Covariates of baseline weight, IBD treatment site, Hb, alb, and CRP were included in an adjusted model. To control for repeated measurements over time, a compound symmetry covariance structure was used. The “IBD treatment site” covariate was included as a fixed effect to adjust for clustering on hospital.
For the subset of patients who had a follow-up colonoscopy, a linear mixed-effect model, adjusted for repeated measures, was applied to examine weight change from baseline, predictors being presence or absence of endoscopic remission, treatment group, time period, baseline weight, and IBD treatment site. Assumptions of a linear model were found to be upheld by inspection of scatter plots and histograms of residuals and predicted values (Supp Fig. 1).

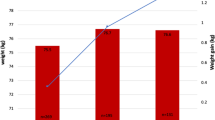
Mean weight change over a period of 48 months in the 4 different biological groups
To describe the course of weight change over the first 48 months of biologic therapy, a latent class analysis was applied. The best-fitting model was identified on the basis of the Bayesian Information Criterion (BIC) and its interpretability. Patients were assigned to trajectory groups using the maximum probability rule. Univariate and multivariable ordinal logistic regressions were used to assess factors associated with membership of each group.
An initial multivariable logistic model was performed by including all predictors with P value < 0.2 on univariate regression. Backward elimination was performed, removing one covariate with the highest P-value, one model at a time until all covariates had a P value < 0.2 [22].
The statistical software used was SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics Approval
The Central Adelaide local health Network (CALHN) Research services (South Australia) and Metro South Health (MSH) Manager, Research Integrity and compliance (Queensland) reviewed the project and confirmed that the project meets criteria for audit and none of the triggers for consideration of ethical review are present and therefore formal ethics approval was not required. Publication approval was provided by the CALHN and MSH research committees.
Results
General Cohort Description
A total of 807 patients on biological therapy were initially screened for inclusion in the study, 513 patients were excluded due to short duration of therapy and any missing data (height, weight at a certain time point, inflammatory markers), leaving 294 patients for analysis (Supp Fig. 2). Follow-up colonoscopy data were available for 116 patients within 18 months of induction therapy.

Three different trajectories of weight gain over time in our cohort of patient
Of the 294 patients included, 165 were on IFX, 68 on ADA, 36 on VDZ, and 25 on UST. In total, 179 patients remained on biological therapy at 48 months (Supp Fig. 3).
Patient characteristics are summarized in Table 1.
There was a trend for weight gain in the whole cohort with mean weight of 77.4 kg (SD19.10) at induction and 80.0 kg (18.72) at 48 months (P = 0.14).
The mean BMI at induction was 26.58 kg/m2(SD 6.01) classifying our cohort as overweight on average and was 27.08 kg/m2 (SD 5.37) at 48 months(P = 0.36).
At induction of therapy; 27.5% of patients were obese (BMI ≥ 30 kg/m2), 23.5% were overweight (BMI ≥ 25–29.9 kg/m2), 38.1% had a normal weight (BMI ≥ 18.5–24.9 kg/m2) and 10.9% of patients were underweight (BMI < 18.5 kg/m2).
Weight and BMI Patterns in Different Biological Groups
Adjusting for baseline weight, treatment site, CRP, Alb, and Hb and controlling for repeated measurements over time (interaction P value = 0.026), the weight pattern differed over time between the 4 biological classes included in the study (Fig. 1).
The BMI change over time is significantly different between treatment groups only when we don’t adjust for markers of inflammation.
Applying the same adjustments, there was a statistically significant weight gain in the IFX group and the VDZ subgroups and a significant BMI increment in the IFX group.
Over a period of 48 months, the mean weight and BMI gain in the IFX treated groups were respectively 2.4 kg (95% CI: 1.4 kg, 3.4 kg) and 0.77 kg/ m2 (95% CI: 0.43 kg/ m2, 1.1 kg/ m2).
There was found to be a significantly greater weight and BMI gains over time in the IFX group compared with the ADA group (mean difference = 0.06, 95% CI: 0.002, 0.11, P value = 0.0437). (Table 2).
Weight Patterns and Associated Clinical Characteristics
An inverse association between baseline weight and weight change was found. This held true whilst adjusting for the interaction between treatment group and time period, Hb, CRP, albumin, and IBD unit, and controlling for repeated measurements over time (global P value = 0.0164). For every 10 kg increase in baseline weight, the weight change from baseline decreases by half a kilogram (estimate = – 0.05, 95% CI: – 0.09, – 0.01). Thus heavier patients, on average, gain less weight than lighter patients. (Table 2).
In the subgroup with follow-up colonoscopy data, endoscopic remission did not appear to have a statistically significant impact on weight change, adjusting for time period, treatment group, baseline weight, and hospital, and controlling for repeated measurements over time (global P value = 0.755).
A latent class analysis was performed aiming to assign each of the 294 patients to one of three weight trajectory groups: weight loss (57.4%), modest weight gain (37.8%), and marked weight gain (4.8%) (Fig. 2).
Out of the 14 patients with marked weight gain, 11 were on IFX.
The respective mean weight changes from baseline to 48 months per group, were – 2.41 kg (SD ± 4.47), + 7.09 kg (4.64), and + 25.8 kg (5.41).
The respective mean BMIs from baseline to 48 months were: 27.49 (SD 6.27) to 26.53 (SD 5.4); 25.68 (SD 4.95) to 27.65 (SD 5.16) and 21.1 (SD 4.79) to 29.8 (SD 5.16).
There was a statistically significant association between Group affiliation and the following predictors on univariate logistic regression analysis (Table 3):
-
(i)
Gender (global P value = 0.0031): Females had a lesser probability of being in the ‘marked weight gain’ group than males (OR = 0.50, 95% CI: 0.31, 0.79).
-
(ii)
CRP (global P value = 0.0187): Patients with a CRP \(\le\) 5 were 43% less likely to be in the ‘marked weight gain’ group than patients with a CRP > 5 (OR = 0.57, 95% CI: 0.36, 0.91).
-
(iii)
Albumin (global P value = 0.0053): Patients with an albumin > 35 were 50% less likely to be in the ‘marked weight gain’ group than patients with an albumin \(\le 35\)(OR = 0.50, 95% CI: 0.31, 0.82)
-
(iv)
Baseline BMI (global P value = 0.0001): For every one unit increase in BMI, the odds of being in the ‘marked weight gain’ group decreased by 8% (OR = 0.92, 95% CI: 0.88, 0.96).
There was no statistically significant association between various weight trajectories and: age (global P = 0.13), disease type (CD Vs UC; global P = 0.63), disease duration (global P = 0.16), steroid therapy at baseline (global P = 0.74), dose-escalated therapy (global P = 0.95) or combination versus monotherapy (global P = 0.80). Nor was small bowel involvement in CD associated with a specific weight trajectory. (L1/L3 vs L2 only; global P = 0.33).
In a multivariable model (Table 4) after adjusting for all other variables, a statistically significant inverse association remained between weight trajectory group and: Alb (global P value = 0.023), initial BMI (global P value = 0.0005) and female gender (global P value = 0.0045).
Patients with an initial albumin \(\le\) 35 were 1.9 times more likely to be in the ‘major weight gain’ group than patients with an albumin > 35 (adjusted OR = 1.9, 95% CI:1.1, 3.2).
For every unit increase in initial BMI, the odds of being in the ‘major weight gain’ group decrease by 8% (adjusted OR = 0.92, 95% CI: 0.88, 0.97).
Males were twice as likely to be in the ‘major weight gain’ group than females (adjusted OR = 2.0, 0.95% CI: 1.3, 3.3).
Discussion
Despite an anecdotal trend of weight gain in our cohort of patients, a more detailed observation shows that more than half of our patients were overweight or obese at induction of therapy; subsequently more than half of the cohort lost weight over time.
That might reflect a weight change towards their ideal body weight due to reversal of inflammation and catabolic burden leading to an improved quality of life and physical activity. It is an interesting observation given that a recent prospective cohort study (23)concluded that all biologicals are associated with some degree of weight gain.
In patients who gained weight, a modest weight gain (7.09 kg) occurred in 38% of cases and significant gain (25.8 kg) occurred only in 14 patients (4.8%) of which 11 were on IFX and 2 on VDZ, upgrading the mean BMI of this subgroup from "normal” to significantly “overweight”.
Weight gain appears to be a combination of class and disease effects as we found that both active disease at baseline and specific therapies such as IFX and VDZ were associated with greater weight gain than other therapies.
Patient characteristics including male gender, a lower baseline weight, and disease characteristics such as indices of active systemic inflammation (high CRP and Low albumin) at initiation of therapy were associated with more weight gain.
Those results, notably active disease and patient characteristics are consistent with previous research [2, 3] looking at weight gain in patients with IBD treated with IFX.
In patients with other immune-mediated inflammatory diseases (IMID) such as psoriasis and psoriatic arthritis, anti-TNF-α treatment was associated with an increase in fat and lean mass as demonstrated by Di Renzo et al. and Briot et al. [4, 5]. They suggest that weight gain is induced by a reversal of the systemic TNF- α effect on body weight hemostasis such as increased lipolysis, increased muscle cell catabolism, and general proteolysis. Other studies have suggested that TNF-α blockers might increase visceral adiposity [7], have a central orexigenic effect [6], and suppress inflammatory myopenia [13].
In our study, the magnitude of weight gain achieved in IFX-treated patients appears to be beyond what might be expected with control of inflammation and raises the hypothesis of a class-dominant effect, however, this is difficult to confirm due to the retrospective nature of our work.
Interestingly, patients treated with ADA showed a trend towards weight gain from induction to 24 months but not further. This might be explained by drug-specific characteristics such as gastrointestinal side effects (nausea, vomiting, and abdominal pain), pharmacokinetics, patients-specific factors, or simply by the smaller ADA subgroup size.
Similarly, UST-treated patients showed a trend for weight gain that did not reach significance.
Vedolizumab treated patients acquired significant weight gain. It was noted that the mean age of this subgroup (51, SD13.9) is the highest in the cohort. Being a gut-specific biological, we suggest that the significant weight gain seen in the VDZ treated patients, is due to improved intestinal mucosal health, nutritional status, and decreased protein wasting. Age might be an important factor in this subgroup.
This aligns with the results of Borren et al.’s study [23] showing that all patients with IBD treated with biologicals acquire a degree of weight gain, however, in their study, none of the disease activity parameters showed any statistical association with weight gain and no significant differences between any of the biologic therapies for weight gain was seen.
Disease activity as assessed by endoscopic remission did not seem to affect weight gain. This might reflect a lack of precision in the available data, a smaller size of cohort with follow-up colonoscopy at 18 months, or a potential systemic, rather than gut-specific mechanism of weight gain in patients treated with those drugs. This has been previously suggested for IFX in other studies [2, 6,7,8].
To date, the largest analysis of weight gain on TNF-α inhibitors for IBD patients is a post-hoc analysis where a total of 1273 patients from ACCENT I, ACCENT II, ACT 1, and SONIC trials were compared to a subgroup of 170 patients on Azathioprine monotherapy from the sonic trial [2]. The study concluded that patients on AZA gained less weight than IFX treated patients and within the latter group, patients with markers of severe disease, CD patients, and male patients were likely to gain more weight.
Our findings are similar; however, we did not have an adequate sample size ratio to examine differences in weight patterns between CD and UC. The authors did not consider CD distribution in their calculations and did not comment on changes in BMI. Additionally, it is potentially more valid to compare patients on a certain biologic therapy to patients on another biologic, as patients who qualify for this treatment are likely to have a more severe disease phenotype.
IBD as most of the immune-mediated inflammatory diseases is a systemic disease associated with cardiovascular and metabolic comorbidities, hence it is important to determine whether weight gain was due to an increase in fat or muscle mass; this can only be done with prospective assessment of body composition, nutritional status, and basal metabolic rate.
Due to the limitations of our study, it is hard to confidently comment on whether where it occurred, weight gain reflects a desirable increase in lean body mass due to reduced systemic inflammation, or an undesirable drug-specific side effect.
The lower baseline weight and high indices of systemic inflammation in the weight gain subgroups suggest it may be the former. Significant weight gain was observed in only 14 patients (< 5% of the whole cohort), 6 of whom were initially underweight which suggests that, unlike steroids, weight gain on biologics is likely to represent a desired drug-related effect.
Another interesting observation in this study is that around half of our biological treated patients with IBD are obese or overweight with only 10% being underweight.
This is likely a reflection of the international “obesity pandemic”. “Obesity prophylaxis” with appropriate diet and physical activity should be addressed at every clinical consultation, given the proven IBD and non-IBD-related complications of obesity.
Our study has multiple limitations, particularly its retrospective nature, hence nutrition and calorie intake, physical activity, accurate remission status, and body composition were not well examined. Trough levels of biological at regular treatment intervals would have been helpful to accurately measure the effect of the drug on weight gain.
Conclusion
Just over half of our biological-treated IBD patients lost a small amount of weight during treatment. That said, around 50% of patients were overweight/obese at induction of therapy.
Weight gain, when acquired was associated with therapy-specific factors (IFX and VDZ), patient’s clinical characteristics (male gender, low baseline BMI), and disease-specific factors (active systemic inflammation).
References
Chang JT. Pathophysiology of inflammatory bowel diseases. N Engl J Med. 2020;383:2652–2664.
Christian KE, Russman KM, Rajan DP, Barr EA, Cross RK. Gender differences and other factors associated with weight gain following initiation of infliximab: a post hoc analysis of clinical trials. Inflamm Bowel Dis. 2020;26:125–131.
Kaazan P, Tan Z, Bednarz J, Hughes J, Grafton R, Andrews JM. Infliximab-related weight gain in inflammatory bowel disease: associations and financial impacts. Intern Med J. 2020;50:1134–1138.
Renzo LD, Saraceno R, Schipani C et al. Prospective assessment of body weight and body composition changes in patients with psoriasis receiving anti-TNF-alpha treatment. Dermatol Ther. 2011;24:446–451.
Briot K, Gossec L, Kolta S, Dougados M, Roux C. Prospective assessment of body weight, body composition, and bone density changes in patients with spondyloarthropathy receiving anti-tumor necrosis factor-alpha treatment. J Rheumatol. 2008;35:855–861.
Gray MA, Chao CY, Staudacher HM et al. Anti-TNFalpha therapy in IBD alters brain activity reflecting visceral sensory function and cognitive-affective biases. PLoS One. 2018;13:e0193542.
Parmentier-Decrucq E, Duhamel A, Ernst O et al. Effects of infliximab therapy on abdominal fat and metabolic profile in patients with Crohn’s disease. Inflamm Bowel Dis. 2009;15:1476–1484.
Ding NS, Malietzis G, Lung PFC et al. The body composition profile is associated with response to anti-TNF therapy in Crohn’s disease and may offer an alternative dosing paradigm. Aliment Pharmacol Ther. 2017;46:883–891.
Nuttall FQ. Body mass index: obesity, bmi, and health: a critical review. Nutr. Today. 2015;50:117–128.
Cornier MA, Despres JP, Davis N et al. Assessing adiposity: a scientific statement from the American heart association. Circulation. 2011;124:1996–2019.
Singh S, Dulai PS, Zarrinpar A, Ramamoorthy S, Sandborn WJ. Obesity in IBD: epidemiology, pathogenesis, disease course and treatment outcomes. Nat Rev Gastroenterol Hepatol. 2017;14:110–121.
Long MD, Crandall WV, Leibowitz IH et al. Prevalence and epidemiology of overweight and obesity in children with inflammatory bowel disease. Inflamm Bowel Dis. 2011;17:2162–2168.
Bryant RV, Schultz CG, Ooi S et al. Visceral adipose tissue is associated with stricturing crohn’s disease behavior, fecal calprotectin, and quality of life. Inflamm Bowel Dis. 2019;25:592–600.
Van Der Sloot KW, Joshi AD, Bellavance DR et al. Visceral adiposity, genetic susceptibility, and risk of complications among individuals with Crohn’s disease. Inflamm Bowel Dis. 2017;23:82–88.
Sandborn WJ, Hanauer SB. Infliximab in the treatment of Crohn’s disease: a user’s guide for clinicians. Am J Gastroenterol. 2002;97:2962–2972.
Sandborn WJ, Hanauer SB, Rutgeerts P et al. Adalimumab for maintenance treatment of Crohn’s disease: results of the CLASSIC II trial. Gut. 2007;56:1232–1239.
Feagan BG, Rutgeerts P, Sands BE et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369:699–710.
Peyrin-Biroulet L, Danese S, Argollo M et al. Loss of response to vedolizumab and ability of dose intensification to restore response in patients with crohn’s disease or ulcerative colitis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2019;17:838–486.
Feagan BG, Sandborn WJ, Gasink C et al. Ustekinumab as induction and maintenance therapy for Crohn’s Disease. N Engl J Med. 2016;375:1946–1960.
Mary JYMR. Development and validation of an endoscopic index of the severity for Crohn’s disease: A prospective multicentre study. Gut. 1989;30:983–989.
Paine ER. Colonoscopic evaluation in ulcerative colitis. Gastroenterol Rep. 2014;2:161–168.
Heinze G, Dunkler D. Five myths about variable selection. Transpl Int. 2017;30:6–10.
Borren NZ, Tan W, Jess AT et al. Assessment of body weight changes in patients with inflammatory bowel diseases initiating biologic therapy: a prospective cohort study. Digestive Dis Sci. 2020;65:3672–3678.
Acknowledgments
The inflammatory bowel disease nurses at both the Royal Adelaide and Logan Hospitals.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Contributions
PK: study design, data collection sheets design, coordinating the work between team members, data collection at two sites, data analysis, manuscript writing (first and last drafts). ZT—Data collection at one site. M and M: data collection at one site. SE: statistical analysis and review. M: Draft review and help with study design. A: Multiple study draft reviews and senior study design. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interests
Pkaazan, Z Tan, P Maiyani, M Mickenbecker, S Edwards & C McIvor: None. JM Andrews – Speaker’s fees, research support &/or Advisory Boards for Abbott, AbbVie, Allergan, Anatara, AstraZeneca, Bayer, BMS 2020, Celgene, Celltrion, Falk, Ferring, Gilead, Hospira, Immuninc, ImmunsanT, Janssen, MSD, Nestle, Novartis, Progenity, Pfizer, Sandoz, Shire, Takeda, Vifor, RAH research Fund, The Hospital Research Fund 2020–2022, The Helmsley Trust 2020–2023.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Kaazan, P., Tan, Z., Maiyani, P. et al. Weight and BMI Patterns in a Biologicals-Treated IBD Cohort. Dig Dis Sci 67, 5628–5636 (2022). https://doi.org/10.1007/s10620-022-07488-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-022-07488-7