
Abstract
Background and Aims
In rare cases, the diagnosis of Crohn’s disease (CD) can only be achieved using small bowel capsule endoscopy (SBCE). We investigate the characteristics of patients with CD only visible on SBCE and assess their disease course.
Methods
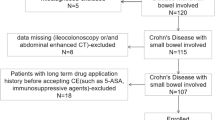
Data of all adult patients with confirmed CD diagnosis based on SBCE with normal endoscopic and cross-sectional imaging findings were retrospectively collected in three tertiary-level hospitals from January 2014 to March 2020.
Results
Thirteen patients were included. Ten patients were females, and the mean age at diagnosis was 36 years. Ileum was mostly involved (85%), while duodenum and jejunum were affected in 23% and 38% of the cases, respectively. Nine patients had one segment involved, while four subjects had two or three segments affected. All patients had inflammatory behavior. First treatment consisted of steroids in all cases, and six patients were later treated with immunosuppressant or biologics. After a mean follow-up of 27.5 months, no change in disease behavior, hospitalization, or CD-related surgery was observed.
Conclusions
CD only visible at SBCE is a rare condition with a more favorable disease course compared to general CD with a lower rate of complicated behavior, hospitalization, and surgery, despite a similar use of immunosuppressant or biologics.
Similar content being viewed by others


Change history
25 September 2020
A Correction to this paper has been published: https://doi.org/10.1007/s10620-020-06613-8
Abbreviations
- CD:
-
Crohn’s disease
- IBD:
-
Inflammatory bowel disease
- CTE:
-
Computed tomography enterography
- MRE:
-
Magnetic resonance enterography
- US:
-
Ultrasonography
- SBCE:
-
Small bowel capsule endoscopy
- EIMs:
-
Extra-intestinal manifestations
- CECDAI:
-
Capsule Endoscopy Crohn’s Disease Activity Index
- CRP:
-
C-reactive protein
- FC:
-
Fecal calprotectin
- TNF:
-
Tumor necrosis factor
- IMIDS:
-
Immune-mediated inflammatory disease
References
Torres J, Mehandru S, Colombel JF, et al. Crohn’s disease. Lancet. 2017;389:1741–1755.
Gomollón F, Dignass A, Annese V, et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: part 1: diagnosis and medical management. J Crohn Colitis. 2017;11:3–25.
Peyrin-Biroulet L, Loftus EV Jr, Colombel JF, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105:289–297.
Maaser C, Sturm A, Vavricka SR, et al. ECCO-ESGAR guideline for diagnostic assessment in IBD part 1: initial diagnosis, monitoring of known IBD, detection of complications. J Crohns Colitis. 2019;13:144–164.
Manes G, Imbesi V, Ardizzone S, et al. Use of double-balloon enteroscopy in the management of patients with Crohn’s disease: feasibility and diagnostic yield in a high-volume centre for inflammatory bowel disease. Surg Endosc. 2009;23:2790–2795.
Iddan G, Meron G, Glukhovsky A, Swain P. Wireless capsule endoscopy. Nature. 2000;405:417.
Enns RA, Hookey L, Armstrong D, et al. Clinical practice guidelines for the use of video capsule endoscopy. Gastroenterology. 2017;152:497–514.
Hosoe N, Takabayashi K, Ogata H, Kanai T. Capsule endoscopy for small-intestinal disorders: current status. Dig Endosc. 2019;31:498–507.
Long MD, Barnes E, Isaacs K, et al. Impact of capsule endoscopy on management of inflammatory bowel disease: a single tertiary care center experience. Inflamm Bowel Dis. 2011;17:1855–1862.
Sorrentino D, Nguyen V. Clinically significant small bowel Crohn’s disease might only be detected by capsule endoscopy. Inflamm Bowel Dis. 2018;24:1566–1574.
Dionisio PM, Gurudu SR, Leighton JA, et al. Capsule endoscopy has a significantly higher diagnostic yield in patients with suspected and established small bowel Crohn’s disease: a meta-analysis. Am J Gastroenterol. 2010;105:1240–1248.
González-Suárez B, Rodriguez S, Ricart E, et al. Comparison of capsule endoscopy and magnetic resonance enterography for the assessment of small bowel lesions in Crohn’s disease. Inflamm Bowel Dis. 2018;24:775–780.
Beaugerie L, Seksik P, Nion-Larmurier I, et al. Predictors of Crohn’s disease. Gastroenterology. 2006;130:650–656.
Cosnes J, Bourrier A, Nion-Larmurier I, Sokol H, Beaugerie L, Seksik P. Factors affecting outcomes in Crohn’s disease over 15 years. Gut. 2012;61:1140–1145.
Eglinton TW, Barclay ML, Gearry RB, Frizelle FA. The spectrum of perianal Crohn’s disease in a population-based cohort. Dis Colon Rectum. 2012;55:773–777.
Panes J, Bouzas R, Chaparro M, et al. Systematic review: the use of ultrasonography, computed tomography and magnetic resonance imaging for the diagnosis, assessment of activity and abdominal complications of Crohn’s disease. Aliment Pharmacol Ther. 2011;34:125–145.
Thia KT, Sandborn WJ, Harmsen WS, et al. Risk factors associated with progression to intestinal complications of Crohn’s disease in a population-based cohort. Gastroenterology. 2010;139:1147–1155.
Guizzetti L, Zou G, Khanna R, et al. Development of clinical prediction models for surgery and complications in Crohn’s disease. J Crohns Colitis. 2018;12:167–177.
Chow DK, Sung JJ, Wu JC, et al. Upper gastrointestinal tract phenotype of Crohn’s disease is associated with early surgery and further hospitalization. Inflamm Bowel Dis. 2009;15:551–557.
Lazarev M, Huang C, Bitton A, et al. Relationship between proximal Crohn’s disease location and disease behavior and surgery: a cross-sectional study of the IBD Genetics Consortium. Am J Gastroenterol. 2013;108:106–112.
Cosnes J, Cattan S, Blain A, et al. Long-term evolution of disease behavior of Crohn’s disease. Inflamm Bowel Dis. 2002;8:244–250.
Girelli CM, Porta P, Malacrida V, Barzaghi F, Rocca F. Clinical outcome of patients examined by capsule endoscopy for suspected small bowel Crohn’s disease. Dig Liver Dis. 2007;39:148–154.
Egea-Valenzuela J, Carrilero-Zaragoza G, Iglesias-Jorquera E, et al. Historical analysis of experience with small bowel capsule endoscopy in a Spanish tertiary hospital. Gastroenterol Hepatol. 2017;40:70–79.
Katsinelos P, Fasoulas K, Beltsis A, et al. Diagnostic yield and clinical impact of wireless capsule endoscopy in patients with chronic abdominal pain with or without diarrhea: a Greek multicenter study. Eur J Intern Med. 2011;22:63–66.
Carretero C, Prieto-Frías C, Muñoz-Navas M. Capsule reading is resources consuming. How can we make the best of it. Rev Esp Enferm Dig. 2015;107:331–333.
Egea-Valenzuela J, Suárez B, Bernald C, et al. Development and validation of a scoring index to predict the presence of lesions in capsule endoscopy in patients with suspected Crohn’s disease of the small bowel: a Spanish multicenter study. Eur J Gastroenterol Hepatol. 2018;30:499–505.
Koulaouzidis A, Douglas S, Plevris JN. Lewis score correlates more closely with fecal calprotectin than Capsule Endoscopy Crohn’s Disease Activity Index. Dig Dis Sci. 2012;57:987–993. https://doi.org/10.1007/s10620-011-1956-8.
Ponte A, Pinho R, Rodrigues A, et al. Evaluation and comparison of capsule endoscopy scores for assessment of inflammatory activity of small-bowel in Crohn’s disease. Gastroenterol Hepatol. 2018;41:245–250.
Yablecovitch D, Lahat A, Neuman S, et al. The Lewis score or the capsule endoscopy Crohn’s disease activity index: which one is better for the assessment of small bowel inflammation in established Crohn’s disease? Ther Adv Gastroenterol. 2018;14:11.
Omori T, Kambayashi H, Murasugi S, et al. Comparison of Lewis score and capsule endoscopy Crohn’s disease activity index in patients with Crohn’s disease. Dig Dis Sci. 2020;65:1180–1188. https://doi.org/10.1007/s10620-019-05837-7.
Funding
No funding was received for the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
TC collected the data, wrote the first draft of the article, created tables and figures, and contributed to the editing. FD collected the data and contributed to the editing. CZ and NM contributed to the editing and revised the article for important intellectual content. LPB contributed to editing of the manuscript and supervised the work.
Corresponding author
Ethics declarations
Conflict of interest
TC, FD, CZ, and NM have no conflict of interest to disclose. LPB reports personal fees from AbbVie, Janssen, Genentech, Ferring, Tillots, Pharmacosmos, Celltrion, Takeda, Boerhinger Ingelheim, Pfizer, Index Pharmaceuticals, Sandoz, Celgene, Biogen, Samsung Bioepis, Alma, Sterna, Nestle, Enterome, Allergan, MSD, Roche, Arena, Gilead, Hikma, Amgen, BMS, Vifor, Norgine; Mylan, Lilly, Fresenius Kabi, Oppilan Pharma, Sublimity Therapeutics, Applied Molecular Transport, OSE Immunotherapeutics, Enthera, Theravance; grants from AbbVie, MSD, Takeda; stock options: CTMA.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chateau, T., Damico, F., Zallot, C. et al. Crohn’s Disease Only Visible on Small Bowel Capsule Endoscopy: A New Entity. Dig Dis Sci 66, 2712–2716 (2021). https://doi.org/10.1007/s10620-020-06553-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-020-06553-3